Descargar la presentación
La descarga está en progreso. Por favor, espere

1
UPDATE 2008 Prevención y dislipemia.
Hotel Beatriz Fuengirola 2008 UPDATE 2008 Prevención y dislipemia. JJGD

2
INDICE ESTATINAS. LO NUEVO EN PREVENCION PRIMARIA Y SECUNDARIA
HDL Y LA HISTORIA DEL TORCETRAPIB. OBESIDAD. CULEBRON GLITAZONAS.

3
OBESIDAD

4
Se investigo la asociación entre el BMI en niños (7 a 13 años) y la aparicion de cardiopatía isquémica en edad adulta (> 25 años), con y sin ajuste por el peso al nacer. Se trata de una cohorte de 276,835 escolares daneses cuyo peso y talla fue medida nacidos entre 1930 y 1976 Los eventos fueron evaluados a través de registros nacionales.

5
he graphs depict the association between childhood BMI and the risk of having a CHD event (nonfatal or fatal) in adulthood. Hazard ratios and 95% confidence intervals are given for a 1-unit increase in BMI z score at each age from 7 to 13 years. The data are from 139,857 boys (Panel A) and 136,978 girls (Panel B) in the Copenhagen School Health Records Cohort. The associations were linear within each age, since trend tests resulted in the rejection of the alternative of nonlinearity modeled as a restricted cubic spline with five knots (all P values >0.15).
 and 136,978 girls (Panel B) in the Copenhagen School Health Records Cohort. The associations were linear within each age, since trend tests resulted in the rejection of the alternative of nonlinearity modeled as a restricted cubic spline with five knots (all P values >0.15)..")
6
Adjusted Hazard Ratio for the Risk of a Fatal or a Nonfatal CHD Event in Adulthood in Relation to a 1-Unit Increase in BMI z Score in a Cohort of 276,835 Children Table 2. Adjusted Hazard Ratio for the Risk of a Fatal or a Nonfatal CHD Event in Adulthood in Relation to a 1-Unit Increase in BMI z Score in a Cohort of 276,835 Children. Conclusion In this study, we determined that higher BMI values in childhood are associated with a greater risk of CHD in adulthood. Furthermore, these risks increase with increasing age of the children. Cutoff points at which the risk dramatically increased were not identified; the risk increased across the spectrum of BMI values. Because more children are becoming heavier at progressively younger ages, our results suggest that a focus should be placed on helping children to attain and maintain appropriate weight to prevent future adverse health consequences. Baker J et al. N Engl J Med 2007;357:

7
Annual Excess Coronary Heart Disease (CHD) Events from 2020 to 2035 Associated with Three Projections of Future Adult Obesity Figure 1. Annual Excess Coronary Heart Disease (CHD) Events from 2020 to 2035 Associated with Three Projections of Future Adult Obesity. High rates of current adolescent overweight are expected to increase the excess incidence of CHD, including new angina, first myocardial infarction, and death from CHD (Panel A); of the total number of CHD events, including myocardial infarction, cardiac arrest, coronary revascularization procedure, and death from CHD (Panel B); and of death from CHD (Panel C) and from other causes (Panel D). Curves are shown for average projections, low projections, and high projections. Bibbins-Domingo K et al. N Engl J Med 2007;357:
 Events from 2020 to 2035 Associated with Three Projections of Future Adult Obesity. High rates of current adolescent overweight are expected to increase the excess incidence of CHD, including new angina, first myocardial infarction, and death from CHD (Panel A); of the total number of CHD events, including myocardial infarction, cardiac arrest, coronary revascularization procedure, and death from CHD (Panel B); and of death from CHD (Panel C) and from other causes (Panel D). Curves are shown for average projections, low projections, and high projections. Bibbins-Domingo K et al. N Engl J Med 2007;357:")
8
Reducción del 24 % Background
Obesity is associated with increased mortality. Weight loss improves cardiovascular risk factors, but no prospective interventional studies have reported whether weight loss decreases overall mortality. In fact, many observational studies suggest that weight reduction is associated with increased mortality. Methods The prospective, controlled Swedish Obese Subjects study involved 4047 obese subjects. Of these subjects, 2010 underwent bariatric surgery (surgery group) and 2037 received conventional treatment (matched control group). We report on overall mortality during an average of 10.9 years of follow-up. At the time of the analysis (November 1, 2005), vital status was known for all but three subjects (follow-up rate, 99.9%). Results The average weight change in control subjects was less than ±2% during the period of up to 15 years during which weights were recorded. Maximum weight losses in the surgical subgroups were observed after 1 to 2 years: gastric bypass, 32%; verticalbanded gastroplasty, 25%; and banding, 20%. After 10 years, the weight losses from baseline were stabilized at 25%, 16%, and 14%, respectively. There were 129 deaths in the control group and 101 deaths in the surgery group. The unadjusted overall hazard ratio was 0.76 in the surgery group (P = 0.04), as compared with the control group, and the hazard ratio adjusted for sex, age, and risk factors was 0.71 (P = 0.01). The most common causes of death were myocardial infarction (control group, 25 subjects; surgery group, 13 subjects) and cancer (control group, 47; surgery group, 29). Conclusions Bariatric surgery for severe obesity is associated with long-term weight loss and decreased overall mortality. Copyright © 2007 Massachusetts Medical Society. All rights reserved. Downloaded from by MANUEL JIMENEZ NAVARRO on December 23, Reducción del 24 %
 and received conventional treatment (matched control group). We report on overall. mortality during an average of 10.9 years of follow-up. At the time of the analysis. (November 1, 2005), vital status was known for all but three subjects (follow-up. rate, 99.9%). Results. The average weight change in control subjects was less than ±2% during the period. of up to 15 years during which weights were recorded. Maximum weight losses in the. surgical subgroups were observed after 1 to 2 years: gastric bypass, 32%; verticalbanded. gastroplasty, 25%; and banding, 20%. After 10 years, the weight losses. from baseline were stabilized at 25%, 16%, and 14%, respectively. There were 129. deaths in the control group and 101 deaths in the surgery group. The unadjusted. overall hazard ratio was 0.76 in the surgery group (P = 0.04), as compared with the. control group, and the hazard ratio adjusted for sex, age, and risk factors was (P = 0.01). The most common causes of death were myocardial infarction (control. group, 25 subjects; surgery group, 13 subjects) and cancer (control group, 47; surgery. group, 29). Conclusions. Bariatric surgery for severe obesity is associated with long-term weight loss and. decreased overall mortality. Copyright © 2007 Massachusetts Medical Society. All rights reserved. Downloaded from by MANUEL JIMENEZ NAVARRO on December 23, Reducción del 24 %")
9
Fig 1 Results of search for relevant studies
Rucker, D. et al. BMJ 2007;335: Copyright ©2007 BMJ Publishing Group Ltd.

10
REDUCCION PESO CON ORLISTAT (kg)
Rucker, D. et al. BMJ 2007;335: Copyright ©2007 BMJ Publishing Group Ltd.

11
REDUCCION PESO CON SIBUTRAMINA
Rucker, D. et al. BMJ 2007;335: Copyright ©2007 BMJ Publishing Group Ltd.

12
REDUCCION PESO CON RIMONABANT (KG)
Rucker, D. et al. BMJ 2007;335: Copyright ©2007 BMJ Publishing Group Ltd.

13
Rimonabant, sibutramina y orlistat reducen de forma modesta el peso (menos de 5kg)
con efectos diferentes sobre los factores de riesgo cardiovascular y diferentes perfiles de efectos adversos. No existen en la actualidad datos sobre su efecto en endpoints clinicos aunque existen estudios en marcha

15
GLITAZONAS

16
14-JUNIO2007

17
5-julio-2007

19
12-SEPTIEMBRE-2007

20
12-SEPTIEMBRE-2007

22
12-diciembre-2007

24
conclusiones No hay por tanto dudas con la información actual que el uso de glitazonas suponen un aumento del riesgo de IC, tanto con pioglitazona como rosiglitazona Existe una duda mas que razonable sobre los efectos de la rosiglitazona pero no de la pioglitazona sobre la incidencia de IAM y un posible aumento de la mortalidad cardiovascular.

25
ESTATINAS. PREVENCION PRIMARIA PREVENCION SECUNDARIA

26
WOSCOPS 7,9 % p < 0,001 5,5 % The west of scotland coronary prevention Study (WOSCOPS) was a randomized, double-blind, placebo-controlled clinical trial of the 3-hydroxy-3-methylglutaryl coenzyme A reductase inhibitor pravastatin (Pravachol, Bristol- Myers Squibb) in middle-aged men without a history of myocardial infarction.1-3 After an average of approximately 5 years, the combined outcome of death from definite coronary heart disease or definite nonfatal myocardial infarction was reduced from 7.9% in the placebo group to 5.5% in the pravastatin group (P<0.001), and the risk of death from definite or suspected coronary heart disease was reduced from 1.9% to 1.3% (P = 0.04). There was a trend toward a reduction in the risk of stroke, and there was no evidence of an increased risk of death from noncardiovascular causes or of an increased risk of incident cancer. Mortality from any cause was 4.1% in the placebo group and 3.2% in the pravastatin group (P = 0.051, unadjusted for covariants).
 in middle-aged men without a. history of myocardial infarction.1-3 After an average. of approximately 5 years, the combined outcome. of death from definite coronary heart disease. or definite nonfatal myocardial infarction. was reduced from 7.9% in the placebo group to. 5.5% in the pravastatin group (P<0.001), and the. risk of death from definite or suspected coronary. heart disease was reduced from 1.9% to 1.3% (P = 0.04). There was a trend toward a reduction. in the risk of stroke, and there was no evidence. of an increased risk of death from noncardiovascular. causes or of an increased risk of incident. cancer. Mortality from any cause was 4.1% in the. placebo group and 3.2% in the pravastatin group. (P = 0.051, unadjusted for covariants).")
27
5778 (91.1%) aceptaron el seguimiento a 10 años.
El % de pacientes tratados con estatinas según los grupos iniciales son respectivamente : % y 24.3% a 1 año, % y 29.4% a 3 años, y % y 35.2% a 5 años. (p<0.001 para todas las comparaciones). The three major cholesterollowering trials carried out in people without a history of coronary events (primary prevention trials) include the West of Scotland Coronary Prevention Study (WOSCOPS),1 the Air Force/Texas Coronary Atherosclerosis Prevention Study,2 and the Anglo-Scandinavian Cardiac Outcomes Trial — Lipid Lowering Arm.3 Of these trials, WOSCOPS entered people with the highest levels of LDL cholesterol. A total of 6595 men, aged 45 to 64 years, without a prior myocardial infarction, who had a mean plasma LDL cholesterol level of 192 mg per deciliter (5.0 mmol per liter), were randomly assigned to receive 40 mg of pravastatin daily or placebo. Pravastatin lowered serum LDL cholesterol by 26% as compared with no lowering with placebo. After an average follow-up of 4.9 years, there was a statistically significant difference in the rate of the primary end point, nonfatal myocardial infarction or death from coronary heart disease, between the pravastatin group and the placebo group (5.5% vs. 7.9%, P<0.001).
. The three major cholesterollowering. trials carried out in people without a history. of coronary events (primary prevention trials) include the West of Scotland Coronary Prevention. Study (WOSCOPS),1 the Air Force/Texas Coronary. Atherosclerosis Prevention Study,2 and the. Anglo-Scandinavian Cardiac Outcomes Trial — Lipid Lowering Arm.3 Of these trials, WOSCOPS. entered people with the highest levels of LDL cholesterol. A total of 6595 men, aged 45 to 64 years, without a prior myocardial infarction, who had. a mean plasma LDL cholesterol level of 192 mg. per deciliter (5.0 mmol per liter), were randomly. assigned to receive 40 mg of pravastatin daily or. placebo. Pravastatin lowered serum LDL cholesterol. by 26% as compared with no lowering with. placebo. After an average follow-up of 4.9 years, there was a statistically significant difference in. the rate of the primary end point, nonfatal myocardial. infarction or death from coronary heart. disease, between the pravastatin group and the. placebo group (5.5% vs. 7.9%, P<0.001).")
28
MORTALIDAD TOTAL Y CV Death from any cause was 18.7% for patients originally assigned to pravastatin as compared with 20.5% for patients originally assigned to placebo (hazard ratio, 0.88; 95% confidence interval [CI], 0.79 to 0.99; P = 0.03). When examined by period, the risk reduction in the pravastatin group was 24% during the trial (P = 0.04), 9% in the post-trial period (P = 0.15), and 12% for the overall follow-up period (P = 0.03)
. When examined by period, the risk. reduction in the pravastatin group was 24% during. the trial (P = 0.04), 9% in the post-trial period. (P = 0.15), and 12% for the overall follow-up period. (P = 0.03)")
29
Estos resultados beneficiosos a los 10 años de finalizado el estudio no pueden extrapolarse al campo de la prevención secundaria. A destacar la ausencia a los 15 años de un aumento de la mortalidad por causas no cardiovasculares ni por cáncer excepto en el cáncer de próstata. 1.8% a 2.7% (P = 0.03). The results for mortality from noncardiovascular causes, mortality from cancer, and all incident cancers suggest no evidence of long-term harm for the patients taking pravastatin. The only cancer outcome that occurred with significantly greater frequency in the pravastatin group than in the placebo group was prostate cancer. Taking into account the multiple statistical tests performed, it is arguable that this result was due to chance rather than to a causal relationship. In the meta-analysis of statin trials,17 data were not reported for prostate cancer as a separate site of cancer. However, there was no excess in the number of genitourinary cancers in that analysis, and the results of an observational case–control study suggest a possible reduction in prostate cancer with statin use.18 A meta-analysis of the incidence of cancer in statin trials19 showed no significant difference in the incidence of prostate cancer between the statin and control groups in trials involving a total of 20,063 participants. However, reports on these other studies did not include data on long-term follow-up, and some cancers may have a long latency period. there was a statistically significant reduction in death from coronary heart disease or nonfatal myocardial infarction, from 10.3% in the group originally assigned to placebo to 8.6% in the group originally assigned to pravastatin. Rates of death from cardiovascular causes and mortality from any cause were not significantly lower in the patients assigned to pravastatin during posttrial follow-up; however, significant reductions were maintained for the entire study interval (including both the trial and the post-trial periods). There was no excess of cancer deaths associated with pravastatin. the main explanations for the ongoing benefit are stabilization of existing plaque, slowing of the progression of coronary artery disease, and possibly regression of atherosclerosis.
. There was no excess of cancer deaths associated. with pravastatin. the main explanations for the ongoing benefit are stabilization of existing plaque, slowing of the progression of coronary artery disease, and possibly regression of atherosclerosis.")
30
Prospective Studies Collaboration
Datos obtenidos de 61 estudios prospectivos observacionales, consistente en casi adultos sin enfermedad previa y con medidas basales de colesterol total y tension arterial. Durante cerca de 12 millones persona-año en riesgo entre edades de 40 a 89 años se produjeron muertes vasculares( Card. isquémica, ACV, otros). Se dispuso de información sobre su HDL c en participantes entre los que se produjeron 5000 muertes vasculares (3000 Card. Isquémica, 1000 ACV, 1000 otros). The eff ects of other vascular risk factors—–particularly blood pressure—on the epidemiological associations of cholesterol with ischaemic heart disease (IHD) and stroke remain uncertain. Although blood levels of total cholesterol are used widely to predict IHD, the relative risk per unit change in cholesterol decreases with age1,2 and, perhaps, blood pressure,3,4 and it is unclear whether an importantly positive association persists into old age. Furthermore, total cholesterol consists largely of the cholesterol in low-density lipoprotein particles (LDL cholesterol) plus the cholesterol in high-density lipoprotein particles (HDL cholesterol), which have opposite associations with IHD risk. Results from randomised trials have shown that treatment with a statin, which lowers LDL cholesterol, substantially reduces the incidence of IHD.5 These trials have also shown a substantial reduction in the incidence of ischaemic stroke (without any apparent increase in haemorrhagic stroke).5 The defi nite reduction in total stroke in the statin trials contrasts strongly with the weakness of the epidemiological association between blood cholesterol and stroke,1,6–13 and that epidemiological association needs further exploration.
. Se dispuso de información sobre su HDL c en participantes entre los que se produjeron 5000 muertes vasculares (3000 Card. Isquémica, 1000 ACV, 1000 otros). The eff ects of other vascular risk factors—–particularly. blood pressure—on the epidemiological associations of. cholesterol with ischaemic heart disease (IHD) and. stroke remain uncertain. Although blood levels of total. cholesterol are used widely to predict IHD, the relative. risk per unit change in cholesterol decreases with age1,2. and, perhaps, blood pressure,3,4 and it is unclear whether. an importantly positive association persists into old age. Furthermore, total cholesterol consists largely of the. cholesterol in low-density lipoprotein particles (LDL. cholesterol) plus the cholesterol in high-density. lipoprotein particles (HDL cholesterol), which have. opposite associations with IHD risk. Results from. randomised trials have shown that treatment with a. statin, which lowers LDL cholesterol, substantially. reduces the incidence of IHD.5 These trials have also. shown a substantial reduction in the incidence of. ischaemic stroke (without any apparent increase in. haemorrhagic stroke).5 The defi nite reduction in total. stroke in the statin trials contrasts strongly with the. weakness of the epidemiological association between. blood cholesterol and stroke,1,6–13 and that epidemiological. association needs further exploration.")
31
MORTALIDAD POR CARDIOPATIA ISQUEMICA AJUSTADO POR EDAD
Figure 1 shows the age-specifi c relation between usual total cholesterol and IHD mortality, plotted on a doubling (ie, logarithmic) scale. On this scale, relations were approximately linear (ie, log-linear) within each decade of age at risk. In both men and women, a prolonged diff erence of 1 mmol/L lower total cholesterol was associated with an IHD mortality that was about a half lower in early middle age (40–49 years), about a third lower in later middle age (50–69 years), and about a sixth lower in old age (70–89 years) (fi gure 1). These fi ndings were only slightly attenuated by adjustment for systolic blood pressure and were unaltered by adjustment for smoking (webtable 6).
 scale. On this scale, relations were. approximately linear (ie, log-linear) within each decade. of age at risk. In both men and women, a prolonged. diff erence of 1 mmol/L lower total cholesterol was. associated with an IHD mortality that was about a half. lower in early middle age (40–49 years), about a third. lower in later middle age (50–69 years), and about a sixth. lower in old age (70–89 years) (fi gure 1). These fi ndings. were only slightly attenuated by adjustment for systolic. blood pressure and were unaltered by adjustment for. smoking (webtable 6).")
32
¿Que ocurre tras ajustar por otros factores de riesgo?

33
Mortalidad por ACV Ajustando por edad Ajustando por tensión arterial
For IHD mortality, age and blood pressure substantially aff ected the strength of the proportional diff erence in risk associated with a specifi c diff erence in cholesterol, but did not aff ect its direction. For stroke mortality, however, age and blood pressure aff ected not only the strength but also the direction of the association. Randomised trials of cholesterol-lowering statin therapy in a wide range of patient populations have shown substantial reductions in the incidence of IHD and of stroke.5,24 In the PSC, the continuous positive relations observed at all ages between total cholesterol and IHD mortality, irrespective of the level of blood pressure, are in keeping with these randomised trial results, and with strategies to lower population levels of LDL cholesterol in all age groups.

34
Prospective Sudies Collaboration: Conclusiones
En el PSC la relación continua observada entre los niveles de colesterol total y mortalidad por cardiopatía isquémica entre todos los rangos de edad es acorde con los resultados de los estudios randomizados y con la estrategia de reducir los niveles de colesterol en todos los grupos de edad. La ausencia de una asociación independiente positiva entre colesterol total y mortalidad por ACV en edad media o en aquellos con TA >145 mm Hg e incluso su relación negativa con la mortalidad por ACV a edades avanzadas o mayor tensión arterial, es inexplicada y necesita mas valoración.

35
Prevención secundaria. No hay dudas. Prevención primaria.
Mortalidad total. RR 0,95(0, ) No se ve reducida por estatinas. Eventos CV. RR 0,82 (0,77-0,87).RR absoluto 1,5 %. 67 personas tratadas 5 años para prevenir 1 ECV. No hay reducción de eventos CV ni en mujeres ni en > 69 años independientemente del sexo. Abramson J, Wright JM. Are lipid-lowering guidelines evidence-based? Lancet Jan 20;369(9557):168-9.
 No se ve reducida por estatinas. Eventos CV. RR 0,82 (0,77-0,87).RR absoluto 1,5 %. 67 personas tratadas 5 años para prevenir 1 ECV. No hay reducción de eventos CV ni en mujeres ni en > 69 años independientemente del sexo. Abramson J, Wright JM. Are lipid-lowering guidelines evidence-based Lancet Jan 20;369(9557):")
36
CRITERIOS DE INCLUSION Randomizacion a estatinas o placebo
Cardiopatía isquémica documentada en el momento de la randomizacion Al menos incluir 50 pacientes ancianos por estudio (definido como >65años) Al menos 6 meses de seguimiento Datos de mortalidad global, por Card. Isquémica, IAM no fatal, necesidad de revascularización o ACV. J Am Coll Cardiol 2008;51:37–45
 Al menos 6 meses de seguimiento. Datos de mortalidad global, por Card. Isquémica, IAM no fatal, necesidad de revascularización o ACV. J Am Coll Cardiol 2008;51:37–45.")
37
Mortalidad Total El uso de estatinas reduce el 22 % el riesgo de muerte a los 5 años en pacientes >65 años con Cardiopatía isquémica comparado con placebo. El numero de pacientes a tratar para salvar una vida es de 28 J Am Coll Cardiol 2008;51:37–45

38
Mortalidad por Cardiopatía Isquémica
El uso de estatinas reduce un 30 % el riesgo de muerte por cardiopatia isquemica a los 5 años en pacientes > 65 años con Cardiopatía isquémica comparado con placebo. El numero de pacientes a tratar para salvar una vida es de 34 J Am Coll Cardiol 2008;51:37–45

39
Incidencia de ACV El uso de estatinas reduce el 25 % el riesgo de ACV a los 5 años en pacientes > 65 años con Cardiopatía isquémica comparado con placebo. J Am Coll Cardiol 2008;51:37–45

41
Primary combined end point: CK-MB, troponin-I, myoglobin, CRP
ARMYDA-ACS : Diseño 580 pts excluded for: statin therapy emergency angiography LVEF <30% contraindications to statins severe renal failure 20 pts excluded for indication to: - medical therapy (N=8) - bypass surgery (N=12) 30 days Atorvastatin 80 mg 12 hrs pre-angio; further 40 mg 2 hrs before N=96 771 pts with NSTE-ACS sent to early coronary angiography (<48 hours) Jan ’05 - Dec ‘06 Randomization (N=191) PCI atorvastatin N=86 Primary combined end point: 30-day death, MI, TVR Coronary angiography atorvast PCI placebo N=85 Placebo 12 hrs pre-angio; further dose 2 hrs before N=95 1st blood sample (pre-PCI) 2nd and 3rd blood samples (8 and 24 hrs post-PCI) . Patti et al. J Am Coll Cardiol.2007; 49: CK-MB, troponin-I, myoglobin, CRP
 - bypass surgery (N=12) 30 days. Atorvastatin 80 mg. 12 hrs pre-angio; further 40 mg. 2 hrs before. N= pts with. NSTE-ACS. sent to. early coronary. angiography. (<48 hours) Jan ’05 - Dec ‘06. Randomization (N=191) PCI. atorvastatin. N=86. Primary combined end point: 30-day death, MI, TVR. Coronary. angiography. atorvast. PCI. placebo. N=85. Placebo. 12 hrs pre-angio; further. dose 2 hrs. before. N=95. 1st blood sample. (pre-PCI) 2nd and 3rd. blood samples. (8 and 24 hrs. post-PCI) . Patti et al. J Am Coll Cardiol.2007; 49: CK-MB, troponin-I, myoglobin, CRP.")
42
ARMYDA-ACS Individual and Combined Outcome Measures
of the Primary End Point at 30 days 14/85 (17%) % 13/85 (15%) P=0.01 P=0.04 4/86 (5%) 4/86 (5%) 1/85 (2%) Endpoint primario combinado Patti et al. J Am Coll Cardiol.2007; 49:
 % 13/85. (15%) P=0.01. P= /86. (5%) 4/86. (5%) 1/85. (2%) Endpoint primario combinado. Patti et al. J Am Coll Cardiol.2007; 49:")
43
ARMYDA-ACS: CONCLUSIONES
ARMYDA-ACS indica que incluso un tratamiento de corta duración con atorvastatina previo a ICP puede mejorar la evolución en pacientes con SCASET. Este beneficio ocurre a expensas fundamentalmente de la reducción de IAM periprocedimiento (reduccion de riesgo relativo del 70 %) Los efectos pleiotropicos de las estatinas pueden ser las responsables de este efecto. In the ARMYDA–ACS randomized trial of 171 patients with non-ST segment elevation ACS [5], they were randomly assigned to pretreatment with atorvastatin (80mg 12 h before percutaneous coronary intervention and a 40mg preprocedure dose) or placebo. All patients received long-term atorvastatin treatment thereafter (40 mg/day). The 30-day incidence of major adverse cardiac events was 5% in the atorvastatin arm and 17% in the placebo arm (P¼0.01). That trial indicated that even short-term pretreatment with a statin may improve outcomes in ACS patients undergoing early invasive strategies. What is unknown from the study, because patients on current therapy with statins were excluded, was whether the chronic administration of statins would have similar benefits to such acute administration.
 Los efectos pleiotropicos de las estatinas pueden ser las responsables de este efecto. In the ARMYDA–ACS randomized trial of 171 patients. with non-ST segment elevation ACS [5], they were. randomly assigned to pretreatment with atorvastatin. (80mg 12 h before percutaneous coronary intervention. and a 40mg preprocedure dose) or placebo. All patients. received long-term atorvastatin treatment thereafter. (40 mg/day). The 30-day incidence of major adverse. cardiac events was 5% in the atorvastatin arm and 17% in the placebo arm (P¼0.01). That trial indicated that. even short-term pretreatment with a statin may improve. outcomes in ACS patients undergoing early invasive strategies. What is unknown from the study, because patients. on current therapy with statins were excluded, was. whether the chronic administration of statins would have. similar benefits to such acute administration.")
44
HDL

45
En el Treating to New Targets (TNT) trial 2661 pacientes alcanzaron un LDLc < 70 mg/dl.
El objetivo de este estudio era comprobar si la asociacion inversa entre HDLc y eventos CV se mantiene a bajos niveles de LDL. BACKGROUND High-density lipoprotein (HDL) cholesterol levels are a strong inverse predictor of cardiovascular events. However, it is not clear whether this association is maintained at very low levels of low-density lipoprotein (LDL) cholesterol. METHODS A post hoc analysis of the recently completed Treating to New Targets (TNT) study assessed the predictive value of HDL cholesterol levels in 9770 patients. The primary outcome measure was the time to a first major cardiovascular event, defined as death from coronary heart disease, nonfatal non–procedure-related myocardial infarction, resuscitation after cardiac arrest, or fatal or nonfatal stroke. The predictive relationship between HDL cholesterol levels at the third month of treatment with statins and the time to the first major cardiovascular event was assessed in univariate and multivariate analyses and was also assessed for specific LDL cholesterol strata, including subjects with LDL cholesterol levels below 70 mg per deciliter (1.8 mmol per liter). RESULTS The HDL cholesterol level in patients receiving statins was predictive of major cardiovascular events across the TNT study cohort, both when HDL cholesterol was considered as a continuous variable and when subjects were stratified according to quintiles of HDL cholesterol level. When the analysis was stratified according to LDL cholesterol level in patients receiving statins, the relationship between HDL cholesterol level and major cardiovascular events was of borderline significance (P = 0.05). Even among study subjects with LDL cholesterol levels below 70 mg per deciliter, those in the highest quintile of HDL cholesterol level were at less risk for major cardiovascular events than those in the lowest quintile (P = 0.03). CONCLUSIONS In this post hoc analysis, HDL cholesterol levels were predictive of major cardiovascular events in patients treated with statins. This relationship was also observed among patients with LDL cholesterol levels below 70 mg per deciliter. (ClinicalTrials.gov number, NCT ) Copyright © 2007 Massachusetts Medical Society. All rights reserved. Downloaded from by MANUEL JIMENEZ NAVARRO on December 23, N Engl J Med 357:1301, September 27, 2007
 cholesterol levels are a strong inverse predictor of. cardiovascular events. However, it is not clear whether this association is maintained. at very low levels of low-density lipoprotein (LDL) cholesterol. METHODS. A post hoc analysis of the recently completed Treating to New Targets (TNT) study. assessed the predictive value of HDL cholesterol levels in 9770 patients. The primary. outcome measure was the time to a first major cardiovascular event, defined as. death from coronary heart disease, nonfatal non–procedure-related myocardial infarction, resuscitation after cardiac arrest, or fatal or nonfatal stroke. The predictive. relationship between HDL cholesterol levels at the third month of treatment with. statins and the time to the first major cardiovascular event was assessed in univariate. and multivariate analyses and was also assessed for specific LDL cholesterol strata, including subjects with LDL cholesterol levels below 70 mg per deciliter (1.8 mmol. per liter). RESULTS. The HDL cholesterol level in patients receiving statins was predictive of major cardiovascular. events across the TNT study cohort, both when HDL cholesterol was considered. as a continuous variable and when subjects were stratified according to. quintiles of HDL cholesterol level. When the analysis was stratified according to LDL. cholesterol level in patients receiving statins, the relationship between HDL cholesterol. level and major cardiovascular events was of borderline significance (P = 0.05). Even among study subjects with LDL cholesterol levels below 70 mg per deciliter, those in the highest quintile of HDL cholesterol level were at less risk for major cardiovascular. events than those in the lowest quintile (P = 0.03). CONCLUSIONS. In this post hoc analysis, HDL cholesterol levels were predictive of major cardiovascular. events in patients treated with statins. This relationship was also observed among. patients with LDL cholesterol levels below 70 mg per deciliter. (ClinicalTrials.gov. number, NCT ) Copyright © 2007 Massachusetts Medical Society. All rights reserved. Downloaded from by MANUEL JIMENEZ NAVARRO on December 23, N Engl J Med 357:1301, September 27,")
46
Todos pacientes Pacientes LDL <70
El TNT fue uno de los estudios que demostraron que los niveles muy bajos de LDLc (por debajo de los recomendados en las guías de práctica clínica) reducían todavía mas los eventos cardiovasculares. Atorvastatina 80 mg/día funcionaba mejor que atorvastatina 10 mg/día. En este análisis post hoc se analizó el valor predictivo de eventos del HDLc en 9770 pacientes estratificados según sus quintiles de HDLc. La tasa de eventos cardiovasculares mayores a los 5 años se reducía en un 40% en el quintil mas alto de HDLc comparado con el quintil mas bajo de HDLc. Tras el ajuste para covariables, el HDLc seguía siendo un predictor significativo de eventos cardiovasculares mayores detectandose una reducción del 25% de eventos en el quintil mas alto de HDLc con respecto al quintil mas bajo. Cuando se examinó el subgrupo con LDLc menor de 70 mg%, los pacientes con niveles de HDLc superiores a 55 mg% tenían menor riesgo de eventos que los pacientes en el quintil mas bajo de HDLc. Este estudio indica que con independencia del nivel de LDLc que se consiga con las estatinas, es conveniente tratar el HDLc bajo para minimizar el riesgo de eventos. N Engl J Med 357:1301, September 27, 2007
 reducían todavía mas los eventos cardiovasculares. Atorvastatina 80 mg/día funcionaba mejor que atorvastatina 10 mg/día. En este análisis post hoc se analizó el valor predictivo de eventos del HDLc en 9770 pacientes estratificados según sus quintiles de HDLc. La tasa de eventos cardiovasculares mayores a los 5 años se reducía en un 40% en el quintil mas alto de HDLc comparado con el quintil mas bajo de HDLc. Tras el ajuste para covariables, el HDLc seguía siendo un predictor significativo de eventos cardiovasculares mayores detectandose una reducción del 25% de eventos en el quintil mas alto de HDLc con respecto al quintil mas bajo. Cuando se examinó el subgrupo con LDLc menor de 70 mg%, los pacientes con niveles de HDLc superiores a 55 mg% tenían menor riesgo de eventos que los pacientes en el quintil mas bajo de HDLc. Este estudio indica que con independencia del nivel de LDLc que se consiga con las estatinas, es conveniente tratar el HDLc bajo para minimizar el riesgo de eventos. N Engl J Med 357:1301, September 27,")
47
Las estatinas reducen los niveles de LDLc y enlentecen la progresión de la arteriosclerosis coronaria. Las estatinas aumentan los niveles de HDLc entre un 5 a un 15 % pero no se ha establecido si este aumento se traduce en un beneficio clínico significativo. El objetivo de este estudio es determinar la contribución relativa del aumento de HDLc por las estatinas en la progresion de la arteriosclerosis coronaria. Nicholls SJ, et al. JAMA Feb; 297(5):
:")
48
Statins, High-Density Lipoprotein Cholesterol, and Regression of Coronary Atherosclerosis: Study Design 1455 pacientes de4 estudios (REVERSAL, CAMELOT, ACTIVATE, ASTEROID) con CI bajo IVUS seriado que reciben tratamiento con estatinas REVERSAL n=502 CAMELOT n=240 ACTIVATE n=364 ASTEROID n=349 18 o 24 meses de seguimiento Endpoint primario: Relacion entre cambios en LDLc y HDL c y volumen de ateroma. Nicholls SJ, et al. JAMA Feb; 297(5):
 con CI bajo IVUS seriado que reciben tratamiento con estatinas. REVERSAL. n=502. CAMELOT. n=240. ACTIVATE. n=364. ASTEROID. n= o 24 meses de seguimiento. Endpoint primario: Relacion entre cambios en LDLc y HDL c y volumen de ateroma. Nicholls SJ, et al. JAMA Feb; 297(5):")
49
fueron predictores independientes de la regresión de ateroma.
In univariate analysis, mean levels and treatment-mediated changes in LDL-C, total cholesterol, non-HDL-cholesterol, apolipoprotein B, and ratio of apolipoprotein B to apolipoprotein A-I were significantly correlated with the rate of atherosclerotic progression, whereas treatment-mediated changes in HDL-C were inversely correlated with atheroma progression. In multivariate analysis, mean levels of LDL-C (β coefficient, 0.11 [95% confidence interval, ]) and increases in HDL-C (β coefficient, [95% confidence interval, ]) remained independent predictors of atheroma regression. Substantial atheroma regression (≥5% reduction in atheroma volume) was observed in patients with levels of LDL-C less than the mean (87.5 mg/dL) during treatment and percentage increases of HDL-C greater than the mean (7.5%; P<0.001). No significant differences were found with regard to clinical events. En el análisis multivariable los niveles medios de LDLc y de aumento de HDLc fueron predictores independientes de la regresión de ateroma. La regresión de ateroma significativa (> 5% reducción de volumen de ateroma) se observo en pacientes con reducciones de LDL c por debajo de la media con tratamiento e incrementos de HDLc por encima de la media(7,5 %)
 and increases in HDL-C (β coefficient, [95% confidence interval, ]) remained independent predictors of atheroma regression. Substantial atheroma regression (≥5% reduction in atheroma volume) was observed in patients with levels of LDL-C less than the mean (87.5 mg/dL) during treatment and percentage increases of HDL-C greater than the mean (7.5%; P<0.001). No significant differences were found with regard to clinical events. En el análisis multivariable los niveles medios de LDLc y de aumento de HDLc. fueron predictores independientes de la regresión de ateroma. La regresión de ateroma significativa (> 5% reducción de volumen de ateroma) se observo en pacientes con reducciones de LDL c por debajo de la media con tratamiento e incrementos de HDLc por encima de la media(7,5 %)")
50
El tratamiento con estatinas se asocia con regresión de la arteriosclerosis coronaria cuando LDLc es reducido sustancialmente y HDL c aumenta mas de un 7,5% Estos hallazgos sugieren que el beneficio de las estatinas son derivados de reducción en los niveles de lipoproteínas aterogénicas y aumentos en HDL c However, it remains to be determined whether the atherosclerotic regression associated with these changes in lipid levels will translate to meaningful reductions in clinical events and improved clinical outcomes. Nicholls SJ, et al. JAMA Feb; 297(5):
:")
51
Description The goal of the trial was to evaluate the effect of treatment with torcetrapib, a cholesteryl ester transfer protein (CETP) inhibitor, in addition to atorvastatin compared with atorvastatin alone on disease progression among patients with coronary disease. Drugs/Procedures Used Following a 4- to 10-week run-in phase in which all patients were treated with atorvastatin titrated to achieve a low-density lipoprotein (LDL) level of mg/dl, patients were randomized in a double-blind manner to treatment with torcetrapib (60 mg; n = 591) in addition to atorvastatin compared with atorvastatin alone with matching placebo (n = 597). Intravascular ultrasonography was performed at baseline and at 24 months. Principal Findings Mean atorvastatin dose was 23 mg in both groups. High-density lipoprotein (HDL) cholesterol at follow-up was higher in the torcetrapib group than the atorvastatin alone group (72.1 mg/dl vs mg/dl, p < 0.001); LDL levels were lower in the torcetrapib group (70.1 mg/dl vs mg/dl, p < 0.001). Median C-reactive protein levels at follow-up were higher in the torcetrapib group than the atorvastatin alone group (1.8 mg/l vs. 1.5 mg/l, p = 0.02). Systolic blood pressure was higher at follow-up in the torcetrapib group (126.4 mm Hg vs mm Hg, p < 0.001), as was diastolic blood pressure (76.0 mm Hg vs mm Hg, p < 0.001), representing an increase in blood pressure in the torcetrapib group of 6.5/2.8 mm Hg. The primary endpoint of change from baseline in percent atheroma volume did not differ between treatment groups (0.12% for torcetrapib vs. 0.19% for atorvastatin alone, p = 0.72), nor did change in atheroma volume of the most diseased 10 mm segment (-4.1 mm3 for torcetrapib vs mm3 for atorvastatin alone, p = 0.12). Reduction in normalized total atheroma volume was greater in the torcetrapib group compared with atorvastatin alone (-9.4 mm3 vs mm3, p = 0.02). All-cause death occurred in 1.4% of the torcetrapib group and 1.0% of the atorvastatin alone group. The composite of death from coronary heart disease, nonfatal myocardial infarction (MI), nonfatal stroke, hospitalization for unstable angina, or coronary revascularization did not differ between groups (21.0% for torcetrapib vs. 19.6% for atorvastatin alone). Blood pressure-related adverse events occurred more frequently in the torcetrapib group (23.7% vs. 10.6%), as did an increase in blood pressure of >15 mm Hg (9.0% vs. 3.2%). Interpretation Among patients with coronary disease, treatment with the CETP inhibitor torcetrapib in addition to atorvastatin therapy was not associated with a difference in change in percent atheroma volume compared with atorvastatin alone at 24-month follow-up. Torcetrapib was effective in raising HDL in the present study. However, there was no effect on atherosclerosis progression, despite having the expected impact on increasing HDL and lowering LDL. Commercial development of torcetrapib was recently stopped after a large trial showed an increase in mortality with torcetrapib, along with an increase in blood pressure. The present study, while much smaller than the other trial, did not show a difference in mortality with torcetrapib, but there were only 14 deaths in the trial. The study did show an increase in blood pressure with torcetrapib. The cause for the increase in mortality is not known at this time, as full results of the safety trial have not yet been presented or published. It is also not known if the increase in blood pressure and mortality is a class effect of the CETP inhibitors or if it is specific to torcetrapib. Conditions • Coronary heart disease Therapies • Lipid-lowering agent • Lipid-lowering agent / HMG CoA Reductase Inhibitor / Atorvastatin Study Design Randomized. Blinded. Patients Enrolled: 1,188 Mean Follow-Up: 24 months Mean Patient Age: Mean age, 57 years % Female: 30 Primary Endpoints Change in percent atheroma volume Secondary Endpoints Normalized total atheroma volume, and change in atheroma volume in the most diseased 10 mm segment Patient Population Age years, clinically indicated cardiac catheterization showing ≥1 stenosis on angiography with ≥20% narrowing, and if the target vessel had less than 50% obstruction throughout a segment of 40 mm or longer Exclusions: Left main coronary artery with >50% obstruction, blood pressure >140/90 mm Hg despite treatment, triglyceride >500 mg/dl, or creatinine >1.7 times the upper limit of normal References: Nissen SE, Tardif JC, Nicholls SJ, et al. Effect of torcetrapib on the progression of coronary atherosclerosis. N Engl J Med 2007;356: Presented by Dr. Steven E. Nissen at the American College of Cardiology Annual Scientific Session, New Orleans, LA, March 2007. N Engl J Med 2007;356:
 level of mg/dl, patients were randomized in a double-blind manner to treatment with torcetrapib (60 mg; n = 591) in addition to atorvastatin compared with atorvastatin alone with matching placebo (n = 597). Intravascular ultrasonography was performed at baseline and at 24 months. Principal Findings Mean atorvastatin dose was 23 mg in both groups. High-density lipoprotein (HDL) cholesterol at follow-up was higher in the torcetrapib group than the atorvastatin alone group (72.1 mg/dl vs mg/dl, p < 0.001); LDL levels were lower in the torcetrapib group (70.1 mg/dl vs mg/dl, p < 0.001). Median C-reactive protein levels at follow-up were higher in the torcetrapib group than the atorvastatin alone group (1.8 mg/l vs. 1.5 mg/l, p = 0.02). Systolic blood pressure was higher at follow-up in the torcetrapib group (126.4 mm Hg vs mm Hg, p < 0.001), as was diastolic blood pressure (76.0 mm Hg vs mm Hg, p < 0.001), representing an increase in blood pressure in the torcetrapib group of 6.5/2.8 mm Hg. The primary endpoint of change from baseline in percent atheroma volume did not differ between treatment groups (0.12% for torcetrapib vs. 0.19% for atorvastatin alone, p = 0.72), nor did change in atheroma volume of the most diseased 10 mm segment (-4.1 mm3 for torcetrapib vs mm3 for atorvastatin alone, p = 0.12). Reduction in normalized total atheroma volume was greater in the torcetrapib group compared with atorvastatin alone (-9.4 mm3 vs mm3, p = 0.02). All-cause death occurred in 1.4% of the torcetrapib group and 1.0% of the atorvastatin alone group. The composite of death from coronary heart disease, nonfatal myocardial infarction (MI), nonfatal stroke, hospitalization for unstable angina, or coronary revascularization did not differ between groups (21.0% for torcetrapib vs. 19.6% for atorvastatin alone). Blood pressure-related adverse events occurred more frequently in the torcetrapib group (23.7% vs. 10.6%), as did an increase in blood pressure of >15 mm Hg (9.0% vs. 3.2%). Interpretation Among patients with coronary disease, treatment with the CETP inhibitor torcetrapib in addition to atorvastatin therapy was not associated with a difference in change in percent atheroma volume compared with atorvastatin alone at 24-month follow-up. Torcetrapib was effective in raising HDL in the present study. However, there was no effect on atherosclerosis progression, despite having the expected impact on increasing HDL and lowering LDL. Commercial development of torcetrapib was recently stopped after a large trial showed an increase in mortality with torcetrapib, along with an increase in blood pressure. The present study, while much smaller than the other trial, did not show a difference in mortality with torcetrapib, but there were only 14 deaths in the trial. The study did show an increase in blood pressure with torcetrapib. The cause for the increase in mortality is not known at this time, as full results of the safety trial have not yet been presented or published. It is also not known if the increase in blood pressure and mortality is a class effect of the CETP inhibitors or if it is specific to torcetrapib. Conditions • Coronary heart disease. Therapies • Lipid-lowering agent • Lipid-lowering agent / HMG CoA Reductase Inhibitor / Atorvastatin. Study Design. Randomized. Blinded. Patients Enrolled: 1,188. Mean Follow-Up: 24 months. Mean Patient Age: Mean age, 57 years. % Female: 30. Primary Endpoints Change in percent atheroma volume. Secondary Endpoints Normalized total atheroma volume, and change in atheroma volume in the most diseased 10 mm segment. Patient Population Age years, clinically indicated cardiac catheterization showing ≥1 stenosis on angiography with ≥20% narrowing, and if the target vessel had less than 50% obstruction throughout a segment of 40 mm or longer. Exclusions: Left main coronary artery with >50% obstruction, blood pressure >140/90 mm Hg despite treatment, triglyceride >500 mg/dl, or creatinine >1.7 times the upper limit of normal. References: Nissen SE, Tardif JC, Nicholls SJ, et al. Effect of torcetrapib on the progression of coronary atherosclerosis. N Engl J Med 2007;356: Presented by Dr. Steven E. Nissen at the American College of Cardiology Annual Scientific Session, New Orleans, LA, March N Engl J Med 2007;356:")
52
ILLUSTRATE : Diseño del Estudio
1188 pacientes entre los años, con cateterismo cardiaco clínicamente indicado, mostrando > 1 estenosis en la coronariografía con > 20% y vaso diana con una obstrucción ≤ 50% en segmentos > 40mm. Aleatorizado . Doble ciego . Edad media= 57 years. 30% Mujeres R 4-10 semanas de tratamiento continuo con atorvastatina dirigido a alcanzar niveles de LDL de mg/dl Atorvastatina + Torcetrapib 60 mg n=591 Atorvastatina + Placebo 60 mg n=597 Description The goal of the trial was to evaluate the effect of treatment with torcetrapib, a cholesteryl ester transfer protein (CETP) inhibitor, in addition to atorvastatin compared with atorvastatin alone on disease progression among patients with coronary disease. Drugs/Procedures Used Following a 4- to 10-week run-in phase in which all patients were treated with atorvastatin titrated to achieve a low-density lipoprotein (LDL) level of mg/dl, patients were randomized in a double-blind manner to treatment with torcetrapib (60 mg; n = 591) in addition to atorvastatin compared with atorvastatin alone with matching placebo (n = 597). Intravascular ultrasonography was performed at baseline and at 24 months. Principal Findings Mean atorvastatin dose was 23 mg in both groups. High-density lipoprotein (HDL) cholesterol at follow-up was higher in the torcetrapib group than the atorvastatin alone group (72.1 mg/dl vs mg/dl, p < 0.001); LDL levels were lower in the torcetrapib group (70.1 mg/dl vs mg/dl, p < 0.001). Median C-reactive protein levels at follow-up were higher in the torcetrapib group than the atorvastatin alone group (1.8 mg/l vs. 1.5 mg/l, p = 0.02). Systolic blood pressure was higher at follow-up in the torcetrapib group (126.4 mm Hg vs mm Hg, p < 0.001), as was diastolic blood pressure (76.0 mm Hg vs mm Hg, p < 0.001), representing an increase in blood pressure in the torcetrapib group of 6.5/2.8 mm Hg. The primary endpoint of change from baseline in percent atheroma volume did not differ between treatment groups (0.12% for torcetrapib vs. 0.19% for atorvastatin alone, p = 0.72), nor did change in atheroma volume of the most diseased 10 mm segment (-4.1 mm3 for torcetrapib vs mm3 for atorvastatin alone, p = 0.12). Reduction in normalized total atheroma volume was greater in the torcetrapib group compared with atorvastatin alone (-9.4 mm3 vs mm3, p = 0.02). All-cause death occurred in 1.4% of the torcetrapib group and 1.0% of the atorvastatin alone group. The composite of death from coronary heart disease, nonfatal myocardial infarction (MI), nonfatal stroke, hospitalization for unstable angina, or coronary revascularization did not differ between groups (21.0% for torcetrapib vs. 19.6% for atorvastatin alone). Blood pressure-related adverse events occurred more frequently in the torcetrapib group (23.7% vs. 10.6%), as did an increase in blood pressure of >15 mm Hg (9.0% vs. 3.2%). Interpretation Among patients with coronary disease, treatment with the CETP inhibitor torcetrapib in addition to atorvastatin therapy was not associated with a difference in change in percent atheroma volume compared with atorvastatin alone at 24-month follow-up. Torcetrapib was effective in raising HDL in the present study. However, there was no effect on atherosclerosis progression, despite having the expected impact on increasing HDL and lowering LDL. Commercial development of torcetrapib was recently stopped after a large trial showed an increase in mortality with torcetrapib, along with an increase in blood pressure. The present study, while much smaller than the other trial, did not show a difference in mortality with torcetrapib, but there were only 14 deaths in the trial. The study did show an increase in blood pressure with torcetrapib. The cause for the increase in mortality is not known at this time, as full results of the safety trial have not yet been presented or published. It is also not known if the increase in blood pressure and mortality is a class effect of the CETP inhibitors or if it is specific to torcetrapib. Conditions • Coronary heart disease Therapies • Lipid-lowering agent • Lipid-lowering agent / HMG CoA Reductase Inhibitor / Atorvastatin Study Design Randomized. Blinded. Patients Enrolled: 1,188 Mean Follow-Up: 24 months Mean Patient Age: Mean age, 57 years % Female: 30 Primary Endpoints Change in percent atheroma volume Secondary Endpoints Normalized total atheroma volume, and change in atheroma volume in the most diseased 10 mm segment Patient Population Age years, clinically indicated cardiac catheterization showing ≥1 stenosis on angiography with ≥20% narrowing, and if the target vessel had less than 50% obstruction throughout a segment of 40 mm or longer Exclusions: Left main coronary artery with >50% obstruction, blood pressure >140/90 mm Hg despite treatment, triglyceride >500 mg/dl, or creatinine >1.7 times the upper limit of normal References: Nissen SE, Tardif JC, Nicholls SJ, et al. Effect of torcetrapib on the progression of coronary atherosclerosis. N Engl J Med 2007;356: Presented by Dr. Steven E. Nissen at the American College of Cardiology Annual Scientific Session, New Orleans, LA, March 2007. 24 meses de seguimiento Objetivo Primario: Cambio en el porcentaje del volúmen del ateroma Objetivo secundario: Volumen total de ateroma normalizado; cambio en el volumen de ateroma en el segmento de 10 mm más afectado N Engl J Med 2007;356:
 inhibitor, in addition to atorvastatin compared with atorvastatin alone on disease progression among patients with coronary disease. Drugs/Procedures Used Following a 4- to 10-week run-in phase in which all patients were treated with atorvastatin titrated to achieve a low-density lipoprotein (LDL) level of mg/dl, patients were randomized in a double-blind manner to treatment with torcetrapib (60 mg; n = 591) in addition to atorvastatin compared with atorvastatin alone with matching placebo (n = 597). Intravascular ultrasonography was performed at baseline and at 24 months. Principal Findings Mean atorvastatin dose was 23 mg in both groups. High-density lipoprotein (HDL) cholesterol at follow-up was higher in the torcetrapib group than the atorvastatin alone group (72.1 mg/dl vs mg/dl, p < 0.001); LDL levels were lower in the torcetrapib group (70.1 mg/dl vs mg/dl, p < 0.001). Median C-reactive protein levels at follow-up were higher in the torcetrapib group than the atorvastatin alone group (1.8 mg/l vs. 1.5 mg/l, p = 0.02). Systolic blood pressure was higher at follow-up in the torcetrapib group (126.4 mm Hg vs mm Hg, p < 0.001), as was diastolic blood pressure (76.0 mm Hg vs mm Hg, p < 0.001), representing an increase in blood pressure in the torcetrapib group of 6.5/2.8 mm Hg. The primary endpoint of change from baseline in percent atheroma volume did not differ between treatment groups (0.12% for torcetrapib vs. 0.19% for atorvastatin alone, p = 0.72), nor did change in atheroma volume of the most diseased 10 mm segment (-4.1 mm3 for torcetrapib vs mm3 for atorvastatin alone, p = 0.12). Reduction in normalized total atheroma volume was greater in the torcetrapib group compared with atorvastatin alone (-9.4 mm3 vs mm3, p = 0.02). All-cause death occurred in 1.4% of the torcetrapib group and 1.0% of the atorvastatin alone group. The composite of death from coronary heart disease, nonfatal myocardial infarction (MI), nonfatal stroke, hospitalization for unstable angina, or coronary revascularization did not differ between groups (21.0% for torcetrapib vs. 19.6% for atorvastatin alone). Blood pressure-related adverse events occurred more frequently in the torcetrapib group (23.7% vs. 10.6%), as did an increase in blood pressure of >15 mm Hg (9.0% vs. 3.2%). Interpretation Among patients with coronary disease, treatment with the CETP inhibitor torcetrapib in addition to atorvastatin therapy was not associated with a difference in change in percent atheroma volume compared with atorvastatin alone at 24-month follow-up. Torcetrapib was effective in raising HDL in the present study. However, there was no effect on atherosclerosis progression, despite having the expected impact on increasing HDL and lowering LDL. Commercial development of torcetrapib was recently stopped after a large trial showed an increase in mortality with torcetrapib, along with an increase in blood pressure. The present study, while much smaller than the other trial, did not show a difference in mortality with torcetrapib, but there were only 14 deaths in the trial. The study did show an increase in blood pressure with torcetrapib. The cause for the increase in mortality is not known at this time, as full results of the safety trial have not yet been presented or published. It is also not known if the increase in blood pressure and mortality is a class effect of the CETP inhibitors or if it is specific to torcetrapib. Conditions • Coronary heart disease. Therapies • Lipid-lowering agent • Lipid-lowering agent / HMG CoA Reductase Inhibitor / Atorvastatin. Study Design. Randomized. Blinded. Patients Enrolled: 1,188. Mean Follow-Up: 24 months. Mean Patient Age: Mean age, 57 years. % Female: 30. Primary Endpoints Change in percent atheroma volume. Secondary Endpoints Normalized total atheroma volume, and change in atheroma volume in the most diseased 10 mm segment. Patient Population Age years, clinically indicated cardiac catheterization showing ≥1 stenosis on angiography with ≥20% narrowing, and if the target vessel had less than 50% obstruction throughout a segment of 40 mm or longer. Exclusions: Left main coronary artery with >50% obstruction, blood pressure >140/90 mm Hg despite treatment, triglyceride >500 mg/dl, or creatinine >1.7 times the upper limit of normal. References: Nissen SE, Tardif JC, Nicholls SJ, et al. Effect of torcetrapib on the progression of coronary atherosclerosis. N Engl J Med 2007;356: Presented by Dr. Steven E. Nissen at the American College of Cardiology Annual Scientific Session, New Orleans, LA, March meses de seguimiento. Objetivo Primario: Cambio en el porcentaje del volúmen del ateroma. Objetivo secundario: Volumen total de ateroma normalizado; cambio en el volumen de ateroma en el segmento de 10 mm más afectado. N Engl J Med 2007;356:")
53
ILLUSTRATE : Objetivo primario
Cambio en el porcentaje del volúmen del ateroma El cambio en el porcentaje del volúmen del ateroma no fue diferente entre los grupos de tratamiento p = 0.72 Cambio del volúmen del ateroma desde la evaluación de inicio(%) n = 591 n = 597 N Engl J Med 2007;356:
 n = 591. n = 597. N Engl J Med 2007;356:")
54
La frecuencia de eventos CV adversos fue similar en ambos grupos
La frecuencia de eventos CV adversos fue similar en ambos grupos. Sin embargo los pacientes con torcetrapib–atorvastatina tenian mas eventos adversos hipertensivos (23.7% vs. 10.6%) y TA >140/90 mm Hg (21.3% vs. 8.2%). Un aumento sostenido de la TA 15 mm Hg en TA sistolica se aprecio en el 9.0% de los pacientes con torcetrapib–atorvastatina frente a un 3.2% en el grupo de atorvastatina .
 y TA >140/90 mm Hg (21.3% vs. 8.2%). Un aumento sostenido de la TA 15 mm Hg en TA sistolica se aprecio en el 9.0% de los pacientes con torcetrapib–atorvastatina frente a un 3.2% en el grupo de atorvastatina .")
55
ILLUSTRATE : Conclusiones
Torcetrapib demostró en este estudio ser una estrategia efectiva en aumentar los niveles de HDL. Sin embargo, no hubo ningún efecto sobre la progresión de ateroesclerosis, a pesar de haber logrado el efecto esperado al incrementar el HDL y bajar los niveles de LDL. N Engl J Med 2007;356:

56
Description The goal of the trial was to evaluate the effect of treatment with torcetrapib, a cholesteryl ester transfer protein (CETP) inhibitor, in addition to atorvastatin compared with atorvastatin alone on disease progression among patients with heterozygous familial hypercholesterolemia. Drugs/Procedures Used Following a 6- to 14-week run-in phase in which all patients were treated with atorvastatin titrated to achieve National Cholesterol Education Program (NCEP) recommended low-density lipoprotein (LDL) levels, patients were randomized in a double-blind manner to treatment with torcetrapib (60 mg; n = 450) in addition to atorvastatin compared with atorvastatin alone with matching placebo (n = 454). Carotid ultrasound was performed at randomization and every 6 months for 24 months. Principal Findings Baseline lipid means were high-density lipoprotein (HDL) of 52 mg/dl, LDL of 138 mg/dl, total cholesterol of 213 mg/dl, and triglycerides of 97 mg/dl. Average dose of atorvastatin used in the study was 56.5 mg. At study end, HDL cholesterol was significantly increased from baseline in the torcetrapib group to 81.5 mg/dl, but stayed at 52 mg/dl in the atorvastatin monotherapy group (p < for between-group comparison). Likewise, LDL reductions were greater with torcetrapib than atorvastatin monotherapy (final LDL mg/dl vs mg/dl, p < 0.001). All other final lipid parameters also favored the torcetrapib group. There was no difference in the primary endpoint of annualized rate of change in maximum carotid intima-media thickness (CIMT) for 12 carotid segments between treatment groups ( mm/year for the torcetrapib group vs mm/year for atorvastatin monotherapy, p = 0.87). Change in maximum CIMT for each of the four common carotid-artery sites showed progression in the torcetrapib group and regression in the atorvastatin monotherapy group ( mm/year vs mm/year, p = 0.02 between groups), as did change in mean CIMT for each of the four common carotid artery sites ( mm/year vs mm/year, p = between groups). Serious adverse events occurred more frequently in the torcetrapib group (12.4% vs. 8.6%), as did serious cardiovascular events (5.3% vs. 2.4%). Final systolic blood pressure was 2.8 mm Hg higher in the torcetrapib group than the atorvastatin monotherapy group (121.7 mm Hg vs mm Hg). Interpretation Among patients with heterozygous familial hypercholesterolemia, treatment with the CETP inhibitor torcetrapib in addition to atorvastatin was not associated with a reduction in disease progression or regression compared with atorvastatin alone through 2 years of treatment. Despite a marked increase in HDL cholesterol and reduction in LDL cholesterol during the study, torcetrapib was not associated with regression of atherosclerotic disease and was actually shown to have worsening disease progression compared with atorvastatin monotherapy for the secondary endpoints of maximum CIMT and mean CIMT in the common carotid. These findings add to the growing body of pathophysiologic information surrounding torcetrapib. However, none of the data presented so far provide a clear-cut explanation for the increase in mortality that was reported in the large outcomes trial with torcetrapib. Full results of the outcomes trial are not yet available. As with other trials of torcetrapib, blood pressure was increased in the present study with torcetrapib. Conditions • Hypercholesterolemia / Hyperlipidemia Therapies • Lipid-lowering agent • Lipid-lowering agent / HMG CoA Reductase Inhibitor / Atorvastatin Study Design Randomized. Blinded. Patients Enrolled: 904 Mean Follow-Up: 24 months Mean Patient Age: Mean age, 46 years % Female: 51 Primary Endpoints Annualized rate of change in maximum IMT for 12 carotid segments Secondary Endpoints Maximum CIMT for each site; mean CIMT common carotid Patient Population Heterozygous familial hypercholesterolemia and eligible for statin treatment, as per NCEP Adult Treatment Panel III References: Kastelein JJ, van Leuven SI, Burgess L, et al. Effect of Torcetrapib on Carotid Atherosclerosis in Familial Hypercholesterolemia. N Engl J Med 2007;356:356: Presented by Dr. John J. Kastelein at the American College of Cardiology Annual Scientific Session, New Orleans, LA, March 2007.
 recommended low-density lipoprotein (LDL) levels, patients were randomized in a double-blind manner to treatment with torcetrapib (60 mg; n = 450) in addition to atorvastatin compared with atorvastatin alone with matching placebo (n = 454). Carotid ultrasound was performed at randomization and every 6 months for 24 months. Principal Findings Baseline lipid means were high-density lipoprotein (HDL) of 52 mg/dl, LDL of 138 mg/dl, total cholesterol of 213 mg/dl, and triglycerides of 97 mg/dl. Average dose of atorvastatin used in the study was 56.5 mg. At study end, HDL cholesterol was significantly increased from baseline in the torcetrapib group to 81.5 mg/dl, but stayed at 52 mg/dl in the atorvastatin monotherapy group (p < for between-group comparison). Likewise, LDL reductions were greater with torcetrapib than atorvastatin monotherapy (final LDL mg/dl vs mg/dl, p < 0.001). All other final lipid parameters also favored the torcetrapib group. There was no difference in the primary endpoint of annualized rate of change in maximum carotid intima-media thickness (CIMT) for 12 carotid segments between treatment groups ( mm/year for the torcetrapib group vs mm/year for atorvastatin monotherapy, p = 0.87). Change in maximum CIMT for each of the four common carotid-artery sites showed progression in the torcetrapib group and regression in the atorvastatin monotherapy group ( mm/year vs mm/year, p = 0.02 between groups), as did change in mean CIMT for each of the four common carotid artery sites ( mm/year vs mm/year, p = between groups). Serious adverse events occurred more frequently in the torcetrapib group (12.4% vs. 8.6%), as did serious cardiovascular events (5.3% vs. 2.4%). Final systolic blood pressure was 2.8 mm Hg higher in the torcetrapib group than the atorvastatin monotherapy group (121.7 mm Hg vs mm Hg). Interpretation Among patients with heterozygous familial hypercholesterolemia, treatment with the CETP inhibitor torcetrapib in addition to atorvastatin was not associated with a reduction in disease progression or regression compared with atorvastatin alone through 2 years of treatment. Despite a marked increase in HDL cholesterol and reduction in LDL cholesterol during the study, torcetrapib was not associated with regression of atherosclerotic disease and was actually shown to have worsening disease progression compared with atorvastatin monotherapy for the secondary endpoints of maximum CIMT and mean CIMT in the common carotid. These findings add to the growing body of pathophysiologic information surrounding torcetrapib. However, none of the data presented so far provide a clear-cut explanation for the increase in mortality that was reported in the large outcomes trial with torcetrapib. Full results of the outcomes trial are not yet available. As with other trials of torcetrapib, blood pressure was increased in the present study with torcetrapib. Conditions • Hypercholesterolemia / Hyperlipidemia. Therapies • Lipid-lowering agent • Lipid-lowering agent / HMG CoA Reductase Inhibitor / Atorvastatin. Study Design. Randomized. Blinded. Patients Enrolled: 904. Mean Follow-Up: 24 months. Mean Patient Age: Mean age, 46 years. % Female: 51. Primary Endpoints Annualized rate of change in maximum IMT for 12 carotid segments. Secondary Endpoints Maximum CIMT for each site; mean CIMT common carotid. Patient Population Heterozygous familial hypercholesterolemia and eligible for statin treatment, as per NCEP Adult Treatment Panel III. References: Kastelein JJ, van Leuven SI, Burgess L, et al. Effect of Torcetrapib on Carotid Atherosclerosis in Familial Hypercholesterolemia. N Engl J Med 2007;356:356: Presented by Dr. John J. Kastelein at the American College of Cardiology Annual Scientific Session, New Orleans, LA, March")
57
Changes in Levels of High-Density Lipoprotein (HDL) and Low-Density Lipoprotein (LDL) Cholesterol in Patients Receiving Atorvastatin Alone or Atorvastatin plus Torcetrapib Figure 1. Changes in Levels of High-Density Lipoprotein (HDL) and Low-Density Lipoprotein (LDL) Cholesterol in Patients Receiving Atorvastatin Alone or Atorvastatin plus Torcetrapib. Panels A and C show the levels of HDL and LDL cholesterol, respectively, in the study patients, and Panels B and D show the percent changes in HDL and LDL cholesterol, respectively, from baseline to 24 months, including a comparison of the percent change between the torcetrapib-atorvastatin group and the atorvastatin-only group for both HDL and LDL cholesterol (right-hand columns). To convert values for cholesterol to millimoles per liter, multiply by Kastelein J et al. N Engl J Med 2007;356:
 and Low-Density Lipoprotein (LDL) Cholesterol in Patients Receiving Atorvastatin Alone or Atorvastatin plus Torcetrapib. Panels A and C show the levels of HDL and LDL cholesterol, respectively, in the study patients, and Panels B and D show the percent changes in HDL and LDL cholesterol, respectively, from baseline to 24 months, including a comparison of the percent change between the torcetrapib-atorvastatin group and the atorvastatin-only group for both HDL and LDL cholesterol (right-hand columns). To convert values for cholesterol to millimoles per liter, multiply by Kastelein J et al. N Engl J Med 2007;356:")
58
Average Maximum Carotid Intima-Media Thickness during 24 Months of Treatment
Los eventos hipertensivos fueron mas comunes en el grupo de tratamiento combinado (8.9% vs. 3.7%), y los valores de tensión arterial >140/90 fueron superiores en el grupo de torcetrapib. Un aumento sostenido de mas de 15 mm hg de TA sistólica ocurrió en un 2,2 % de pacientes con torcetrapib y atorvastatina frente a un 0,9 % de los pacientes tratados con solo atorvastatina. Figure 2. Average Maximum Carotid Intima-Media Thickness during 24 Months of Treatment. The graph shows the average maximum carotid intima-media thickness in 12 carotid segments evaluated in the study patients treated with either atorvastatin monotherapy or a combination of torcetrapib and atorvastatin. I bars represent the standard deviati on. Kastelein J et al. N Engl J Med 2007;356:
, y los valores de tensión arterial >140/90 fueron superiores en el grupo de torcetrapib. Un aumento sostenido de mas de 15 mm hg de TA sistólica ocurrió en un 2,2 % de pacientes con torcetrapib y atorvastatina frente a un 0,9 % de los pacientes tratados con solo atorvastatina. Figure 2. Average Maximum Carotid Intima-Media Thickness during 24 Months of Treatment. The graph shows the average maximum carotid intima-media thickness in 12 carotid segments evaluated in the study patients treated with either atorvastatin monotherapy or a combination of torcetrapib and atorvastatin. I bars represent the standard deviati. on. Kastelein J et al. N Engl J Med 2007;356:")
59
RADIANCE 1: Conclusiones
El uso de torcetrapib en pacientes con hipercolesterolemia familiar no resulto en regresion de la arteriosclerosis, evaluada por por una medidad combinada de grosor de la pared de la arteria carotida, e incluso causo progresion de la enfermedad en los segmentos de la carotida comun. Este efecto ocurrio pese a un incremento no paralelo en los niveles de HDL colesterol (52%) y a una reduccion sustancial de LDL colesterol (21 %)
 y a una reduccion sustancial de LDL colesterol (21 %)")
60
Description The goal of the trial was to evaluate the effect of treatment with torcetrapib, a cholesteryl ester transfer protein (CETP) inhibitor, in addition to atorvastatin compared with atorvastatin alone on disease progression among patients with mixed hyperlipidemia. Drugs/Procedures Used Following a run-in phase in which all patients were treated with atorvastatin titrated to an achieved low-density lipoprotein (LDL) level of 2.59, 3.37, or 4.14 mmol/L, dependent on their calculated cardiac risk, patients were randomized in a double-blind manner to treatment with torcetrapib (60 mg; n = 377) in addition to atorvastatin compared with atorvastatin alone with matching placebo (n = 375). Carotid ultrasound was performed at randomization and every 6 months for 24 months. Principal Findings Baseline lipid means were high-density lipoprotein (HDL) of 1.23 mmol/L, LDL of 2.60 mmol/L, total cholesterol of 4.77 mmol/L, and triglycerides of 1.88 mmol/L. Average dose of atorvastatin used in the study was 13.3 mg in the torcetrapib plus atorvastatin group and 13.2 mg in the atorvastatin monotherapy group. At study end, HDL cholesterol was significantly increased from baseline in the torcetrapib group to 2.00 mmol/L, but stayed at 1.21 mmol/L in the atorvastatin monotherapy group (p < for between-group comparison). Likewise, LDL reductions were greater with torcetrapib than atorvastatin monotherapy (final LDL 2.17 mmol/L vs mmol/L, p < 0.001). All other final lipid parameters also favored the torcetrapib group. There was no difference in the primary endpoint of annualized rate of change in maximum carotid intima-media thickness (CIMT) for 12 carotid segments between treatment groups (0.025 mm/y for the torcetrapib group vs mm/y for atorvastatin monotherapy, p = 0.46). The rate of change differed in several subgroups. Change in maximum CIMT for each of the four common carotid-artery sites also did not differ between the torcetrapib group and the atorvastatin monotherapy group (0.022 mm/y vs mm/y, p = 0.65), nor did change in mean CIMT for the common carotid artery (0.013 mm/y vs mm/y, p = 0.06). Serious vascular adverse events occurred in 17 patients in the torcetrapib group and 13 patients in the atorvastatin alone group. Final systolic blood pressure was 5.4 mm Hg higher in the torcetrapib group than the atorvastatin monotherapy group (127.9 mm Hg vs mm Hg, p < 0.001). Interpretation Among patients with mixed hyperlipidemia, treatment with the CETP inhibitor torcetrapib in addition to atorvastatin was not associated with a reduction in disease progression or regression compared with atorvastatin alone through 2 years of treatment. In a large outcomes trial, mortality was increased with torcetrapib, prompting the trial to be discontinued and the development of the drug to be discontinued; however, the reason for the increased mortality is unknown at this time since the full findings of the trial have not yet been reported. As with other imaging trials of torcetrapib in different populations, torcetrapib was not associated with regression of atherosclerotic disease despite a marked increase in HDL cholesterol and reduction in LDL cholesterol during the study. Blood pressure increased significantly with torcetrapib in the present study, as has been observed in other trials of torcetrapib. Conditions • Hypercholesterolemia / Hyperlipidemia Therapies • Lipid-lowering agent • Lipid-lowering agent / HMG CoA Reductase Inhibitor / Atorvastatin Study Design Placebo controlled. Randomized. Blinded. Patients Screened: 2,918 Patients Enrolled: 752 Mean Follow-Up: Mean 22 months Mean Patient Age: Mean age, 57 years % Female: 36 Primary Endpoints Annualized rate of change in maximum IMT for 12 carotid segments Secondary Endpoints Annualized rate of change in maximum CIMT for each site; mean CIMT common carotid Patient Population Triglycerides >1.7 mmol/L and a concurrent LDL cholesterol that was high enough to qualify for statin treatment according to the US National Cholesterol Education Program (NCEP) Adult Treatment Panel guidelines References: Bots ML, Visseren FL, Evans GW, et al. Torcetrapib and carotid intima-media thickness in mixed dyslipidaemia (RADIANCE 2 study): a randomised, double-blind trial. Lancet 2007;370: Presented by Dr. John J. Kastelein at the American College of Cardiology Annual Scientific Session, New Orleans, LA, March 2007. Lancet 2007; 370: 153–60
 level of 2.59, 3.37, or 4.14 mmol/L, dependent on their calculated cardiac risk, patients were randomized in a double-blind manner to treatment with torcetrapib (60 mg; n = 377) in addition to atorvastatin compared with atorvastatin alone with matching placebo (n = 375). Carotid ultrasound was performed at randomization and every 6 months for 24 months. Principal Findings Baseline lipid means were high-density lipoprotein (HDL) of 1.23 mmol/L, LDL of 2.60 mmol/L, total cholesterol of 4.77 mmol/L, and triglycerides of 1.88 mmol/L. Average dose of atorvastatin used in the study was 13.3 mg in the torcetrapib plus atorvastatin group and 13.2 mg in the atorvastatin monotherapy group. At study end, HDL cholesterol was significantly increased from baseline in the torcetrapib group to 2.00 mmol/L, but stayed at 1.21 mmol/L in the atorvastatin monotherapy group (p < for between-group comparison). Likewise, LDL reductions were greater with torcetrapib than atorvastatin monotherapy (final LDL 2.17 mmol/L vs mmol/L, p < 0.001). All other final lipid parameters also favored the torcetrapib group. There was no difference in the primary endpoint of annualized rate of change in maximum carotid intima-media thickness (CIMT) for 12 carotid segments between treatment groups (0.025 mm/y for the torcetrapib group vs mm/y for atorvastatin monotherapy, p = 0.46). The rate of change differed in several subgroups. Change in maximum CIMT for each of the four common carotid-artery sites also did not differ between the torcetrapib group and the atorvastatin monotherapy group (0.022 mm/y vs mm/y, p = 0.65), nor did change in mean CIMT for the common carotid artery (0.013 mm/y vs mm/y, p = 0.06). Serious vascular adverse events occurred in 17 patients in the torcetrapib group and 13 patients in the atorvastatin alone group. Final systolic blood pressure was 5.4 mm Hg higher in the torcetrapib group than the atorvastatin monotherapy group (127.9 mm Hg vs mm Hg, p < 0.001). Interpretation Among patients with mixed hyperlipidemia, treatment with the CETP inhibitor torcetrapib in addition to atorvastatin was not associated with a reduction in disease progression or regression compared with atorvastatin alone through 2 years of treatment. In a large outcomes trial, mortality was increased with torcetrapib, prompting the trial to be discontinued and the development of the drug to be discontinued; however, the reason for the increased mortality is unknown at this time since the full findings of the trial have not yet been reported. As with other imaging trials of torcetrapib in different populations, torcetrapib was not associated with regression of atherosclerotic disease despite a marked increase in HDL cholesterol and reduction in LDL cholesterol during the study. Blood pressure increased significantly with torcetrapib in the present study, as has been observed in other trials of torcetrapib. Conditions • Hypercholesterolemia / Hyperlipidemia. Therapies • Lipid-lowering agent • Lipid-lowering agent / HMG CoA Reductase Inhibitor / Atorvastatin. Study Design. Placebo controlled. Randomized. Blinded. Patients Screened: 2,918. Patients Enrolled: 752. Mean Follow-Up: Mean 22 months. Mean Patient Age: Mean age, 57 years. % Female: 36. Primary Endpoints Annualized rate of change in maximum IMT for 12 carotid segments. Secondary Endpoints Annualized rate of change in maximum CIMT for each site; mean CIMT common carotid. Patient Population Triglycerides >1.7 mmol/L and a concurrent LDL cholesterol that was high enough to qualify for statin treatment according to the US National Cholesterol Education Program (NCEP) Adult Treatment Panel guidelines. References: Bots ML, Visseren FL, Evans GW, et al. Torcetrapib and carotid intima-media thickness in mixed dyslipidaemia (RADIANCE 2 study): a randomised, double-blind trial. Lancet 2007;370: Presented by Dr. John J. Kastelein at the American College of Cardiology Annual Scientific Session, New Orleans, LA, March Lancet 2007; 370: 153–60.")
61
Atorvastatina Atorvastatina + Torcetrapib Lancet 2007; 370: 153–60

62
Barter PJ, et al. N Engl J Med 2007;357:2109-2122
Description The goal of the trial was to evaluate the effect of treatment with torcetrapib, a cholesteryl ester transfer protein (CETP) inhibitor, in addition to atorvastatin compared with atorvastatin alone on clinical events among patients at high risk for cardiovascular events. Drugs/Procedures Used Following a 4 to 10 week run-in period of lifestyle counseling and atorvastatin treatment if needed, titrated to achieve LDL levels <100 mg/dl, patients were randomized in a double-blind manner to torcetrapib plus atorvastatin (n = 7,533) or atorvastatin plus placebo (n = 7,534). The trial was to continue for a mean follow-up of 4.5 years. Principal Findings The trial was discontinued early after median of 550 days of follow-up at the recommendation of the Data Safety Monitoring Board due to an increase in events in the torcetrapib group. At study entry, 46% of patients had a prior MI and 69% of patients had been revascularized. Diabetes was present in 44% of patients and 7% had heart failure. The increase in high-density lipoprotein (HDL) cholesterol at 12 month follow-up was greater in the torcetrapib group than the atorvastatin alone group (+34.2 mg/dl vs mg/dl, p < 0.001). Likewise, reductions in LDL levels were greater in the torcetrapib group (-21.5 mg/dl vs mg/dl, p < 0.001). Systolic blood pressure at 12 months increased by 5.4 mm Hg in the torcetrapib group and 0.9 mm Hg in the atorvastatin alone group, p < 0.001). Diastolic blood pressure also increased to a greater degree with torcetrapib (+2.0 mm Hg vs mm Hg, p < 0.001). Increases were also observed in sodium, bicarbonate, and aldosterone in the torcetrapib group. The primary endpoint of major cardiovascular event was higher in the torcetrapib group than the atorvastatin alone group (6.2% vs. 5.0%, HR 1.25, p = 0.001). All-cause mortality occurred more frequently in the torcetrapib group (1.2% vs. 0.8%, HR 1.58, p = 0.006), with a directional increase in both CV death (n = 49 vs. n = 35) and non-CV death (n = 40 vs. n = 20). To further explore the impact of the increase in blood pressure with torcetrapib on mortality, additional post-hoc analysis was conducted. Converse to what would be expected, patients with an increase in SBP ≤2.5 mm Hg actually had more deaths than patients with an increase in SBP >2.5 mm Hg (1.5% vs. 0.9%). Mortality was also higher in those with a greater decrease in potassium (1.5% vs. 1.0% for those with vs. without a decrease ≥0.1 mmol/L) and a greater increase in bicarbonate (1.5% vs. 0.9% for those with vs. without an increase >0.7 mmol/L). Interpretation Among patients at high risk for cardiovascular events, treatment with the CETP inhibitor torcetrapib in addition to atorvastatin therapy was associated with an increase in the primary endpoint of major cardiovascular events and an increase in mortality compared with atorvastatin alone. Torcetrapib was highly effective in raising HDL in the present study, as well as lowering LDL. The prior ILLUSTRATE study showed no effect on atherosclerosis progression with torcetrapib, despite having the expected impact on increasing HDL and lowering LDL. The increase in blood pressure observed in the trial was expected to explain in part the increase in mortality, but further analysis of the data showed that those with a greater increase in systolic blood pressure actually had a lower mortality rate than patients with less of an increase in blood pressure. The increase in mortality appeared to be in both cardiovascular and non-cardiovascular causes. Another possible explanation for the increase in mortality raised by the investigators was the increase in aldosterone, or potentially an adverse effect of the CETP inhibition itself, although the conclusive cause is not known. Conditions • Coronary heart disease Therapies • Lipid-lowering agent Study Design Placebo controlled. Randomized. Blinded. Patients Enrolled: 15067 Mean Patient Age: Mean age 61.3 years Mean Follow-Up: Median follow-up 550 days % Female: 22 Primary Endpoints Major cardiovascular event, defined as death from coronary heart disease, nonfatal myocardial infarction (MI), stroke, or hospitalization for unstable angina. Secondary Endpoints Individual components of the primary endpoint, death from any cause, and the change from baseline in LDL and HDL cholesterol levels. Patient Population Age 45 to 75 years; either history of cardiovascular (CV) disease, including MI, stroke, acute coronary syndrome, unstable angina, peripheral vascular disease, and cardiac revascularization, 30 days to 5 years before screening, or type 2 diabetes without previous CV disease who met American Diabetes Association criteria or were receiving hypoglycemic agents. Exclusions: Evidence of an unstable medical condition; life expectancy <5 years; LDL cholesterol level <100 mg/dl if the patient was not receiving a lipid-altering drug; CV event during the run-in period or uncontrolled hypertension or if the LDL cholesterol target level had not been reached at the end of the run-in period. References: Barter PJ, et al. Effects of Torcetrapib in Patients at High Risk for Coronary Events. N Engl J Med 2007;357: Presented by Dr. Philip J. Barter at the American Heart Association Annual Scientific Session, Orlando, FL, November 2007. Perspective: The metabolic changes suggest torcetrapib-induced hyperaldosteronism, which resulted in a modest increase in systolic blood pressure, hypokalemia, and relative alkalosis, but the increase in mortality and cardiovascular events in <2 years would not seem to be due to that alone. The study was designed for a mean 4.5-year follow-up, powered to detect a 20% reduction in events, and was terminated after a median follow-up of 550 days, suggesting some off-target effects that were not evident in animal studies and small clinical trials. Fortunately, due to the number of study participants, investigators were able to detect the risk of torcetrapib despite <2% absolute difference in endpoints at 2 years. Other CETP inhibitors are used in clinical trials, which do not have an effect on blood pressure. It remains to be seen whether increasing the cholesterol content of HDL particles by CETP inhibition is beneficial, or possibly that the cholesterol-rich HDL particles are dysfunctional or even proatherogenic. Improving reverse cholesterol transport via HDL is perhaps the most important remaining and reachable target for reducing cardiovascular mortality in this decade. Melvyn Rubenfire, M.D., F.A.C.C. Barter PJ, et al. N Engl J Med 2007;357:
 inhibitor, in addition to atorvastatin compared with atorvastatin alone on clinical events among patients at high risk for cardiovascular events. Drugs/Procedures Used Following a 4 to 10 week run-in period of lifestyle counseling and atorvastatin treatment if needed, titrated to achieve LDL levels <100 mg/dl, patients were randomized in a double-blind manner to torcetrapib plus atorvastatin (n = 7,533) or atorvastatin plus placebo (n = 7,534). The trial was to continue for a mean follow-up of 4.5 years. Principal Findings The trial was discontinued early after median of 550 days of follow-up at the recommendation of the Data Safety Monitoring Board due to an increase in events in the torcetrapib group. At study entry, 46% of patients had a prior MI and 69% of patients had been revascularized. Diabetes was present in 44% of patients and 7% had heart failure. The increase in high-density lipoprotein (HDL) cholesterol at 12 month follow-up was greater in the torcetrapib group than the atorvastatin alone group (+34.2 mg/dl vs mg/dl, p < 0.001). Likewise, reductions in LDL levels were greater in the torcetrapib group (-21.5 mg/dl vs mg/dl, p < 0.001). Systolic blood pressure at 12 months increased by 5.4 mm Hg in the torcetrapib group and 0.9 mm Hg in the atorvastatin alone group, p < 0.001). Diastolic blood pressure also increased to a greater degree with torcetrapib (+2.0 mm Hg vs mm Hg, p < 0.001). Increases were also observed in sodium, bicarbonate, and aldosterone in the torcetrapib group. The primary endpoint of major cardiovascular event was higher in the torcetrapib group than the atorvastatin alone group (6.2% vs. 5.0%, HR 1.25, p = 0.001). All-cause mortality occurred more frequently in the torcetrapib group (1.2% vs. 0.8%, HR 1.58, p = 0.006), with a directional increase in both CV death (n = 49 vs. n = 35) and non-CV death (n = 40 vs. n = 20). To further explore the impact of the increase in blood pressure with torcetrapib on mortality, additional post-hoc analysis was conducted. Converse to what would be expected, patients with an increase in SBP ≤2.5 mm Hg actually had more deaths than patients with an increase in SBP >2.5 mm Hg (1.5% vs. 0.9%). Mortality was also higher in those with a greater decrease in potassium (1.5% vs. 1.0% for those with vs. without a decrease ≥0.1 mmol/L) and a greater increase in bicarbonate (1.5% vs. 0.9% for those with vs. without an increase >0.7 mmol/L). Interpretation Among patients at high risk for cardiovascular events, treatment with the CETP inhibitor torcetrapib in addition to atorvastatin therapy was associated with an increase in the primary endpoint of major cardiovascular events and an increase in mortality compared with atorvastatin alone. Torcetrapib was highly effective in raising HDL in the present study, as well as lowering LDL. The prior ILLUSTRATE study showed no effect on atherosclerosis progression with torcetrapib, despite having the expected impact on increasing HDL and lowering LDL. The increase in blood pressure observed in the trial was expected to explain in part the increase in mortality, but further analysis of the data showed that those with a greater increase in systolic blood pressure actually had a lower mortality rate than patients with less of an increase in blood pressure. The increase in mortality appeared to be in both cardiovascular and non-cardiovascular causes. Another possible explanation for the increase in mortality raised by the investigators was the increase in aldosterone, or potentially an adverse effect of the CETP inhibition itself, although the conclusive cause is not known. Conditions • Coronary heart disease. Therapies • Lipid-lowering agent. Study Design. Placebo controlled. Randomized. Blinded. Patients Enrolled: Mean Patient Age: Mean age 61.3 years. Mean Follow-Up: Median follow-up 550 days. % Female: 22. Primary Endpoints Major cardiovascular event, defined as death from coronary heart disease, nonfatal myocardial infarction (MI), stroke, or hospitalization for unstable angina. Secondary Endpoints Individual components of the primary endpoint, death from any cause, and the change from baseline in LDL and HDL cholesterol levels. Patient Population Age 45 to 75 years; either history of cardiovascular (CV) disease, including MI, stroke, acute coronary syndrome, unstable angina, peripheral vascular disease, and cardiac revascularization, 30 days to 5 years before screening, or type 2 diabetes without previous CV disease who met American Diabetes Association criteria or were receiving hypoglycemic agents. Exclusions: Evidence of an unstable medical condition; life expectancy <5 years; LDL cholesterol level <100 mg/dl if the patient was not receiving a lipid-altering drug; CV event during the run-in period or uncontrolled hypertension or if the LDL cholesterol target level had not been reached at the end of the run-in period. References: Barter PJ, et al. Effects of Torcetrapib in Patients at High Risk for Coronary Events. N Engl J Med 2007;357: Presented by Dr. Philip J. Barter at the American Heart Association Annual Scientific Session, Orlando, FL, November Perspective: The metabolic changes suggest torcetrapib-induced hyperaldosteronism, which resulted in a modest increase in systolic blood pressure, hypokalemia, and relative alkalosis, but the increase in mortality and cardiovascular events in <2 years would not seem to be due to that alone. The study was designed for a mean 4.5-year follow-up, powered to detect a 20% reduction in events, and was terminated after a median follow-up of 550 days, suggesting some off-target effects that were not evident in animal studies and small clinical trials. Fortunately, due to the number of study participants, investigators were able to detect the risk of torcetrapib despite <2% absolute difference in endpoints at 2 years. Other CETP inhibitors are used in clinical trials, which do not have an effect on blood pressure. It remains to be seen whether increasing the cholesterol content of HDL particles by CETP inhibition is beneficial, or possibly that the cholesterol-rich HDL particles are dysfunctional or even proatherogenic. Improving reverse cholesterol transport via HDL is perhaps the most important remaining and reachable target for reducing cardiovascular mortality in this decade. Melvyn Rubenfire, M.D., F.A.C.C. Barter PJ, et al. N Engl J Med 2007;357:")
63
Hombres o mujeres postmenopausicas 45 a 75 años
Atorvastatina fase de run-in hasta alcanzar LDL <100 mg/dL 4-10 weeks Torcetrapib + dosis de atorvastatina titulada Seguimiento planeado a 4,5 años Dosis de atorvastatina titulada Poblacion a estudio Sujetos End point primario Hombres o mujeres postmenopausicas 45 a 75 años Elegibles para uso de estatinas Cualquier nivel de HDL c Historia de CI o riesgo equivalente 15,000 7 paises Eventos cardiovasculares mayores ILLUMINATE is a multicenter, double-blind, parallel-group, clinical end point trial that is being conducted at 250 sites in 7 countries. Approximately 13,000 subjects with CHD or CHD risk equivalent will be randomized to treatment without regard to their baseline HDL-C levels. The primary end point is a composite of CHD death, nonfatal MI, or stroke. The study population includes men and women, 45 to 75 years of age, who have a prior history of CHD or a CHD risk equivalent and who are eligible for statin treatment. Baseline HDL-C level is not a feature of the inclusion or exclusion criteria. Subjects initially enter an atorvastatin run-in period during which atorvastatin treatment is initiated. Subjects previously treated with other statins are switched to an equivalent dose of atorvastatin. The atorvastatin dose is then titrated to a target LDL-C level of <100 mg/dL (2.6 mmol/L). Following attainment of the LDL-C goal, patients are randomized to either torcetrapib/atorvastatin or atorvastatin alone. In both treatment arms, the dose of atorvastatin is that established during the atorvastatin run-in phase. Follow-up is driven by end points (984 events) and estimated to last approximately 4.5 years. The primary end point is a composite of CHD death, nonfatal MI, or stroke. Barter PJ, et al. N Engl J Med 2007;357:
. Following attainment of the LDL-C goal, patients are randomized to either torcetrapib/atorvastatin or atorvastatin alone. In both treatment arms, the dose of atorvastatin is that established during the atorvastatin run-in phase. Follow-up is driven by end points (984 events) and estimated to last approximately 4.5 years. The primary end point is a composite of CHD death, nonfatal MI, or stroke. Barter PJ, et al. N Engl J Med 2007;357:")
64
El aumento de eventos cardiovasculares y de mortalidad suspendio el estudio el 2 Diciembre 2006
Comparado con Atorvastatina, Torcetrapib/Atorva aumento HDL-C en un 72% y redujo LDL-C en un 25% End point Atorvastatin (n=7534), n Atorvastatin + torcetrapib (n=7533), n Hazard ratio (95% CI) p Major CV events 373 464 1.25 (1.09–1.44) 0.001 Deaths 59 93 1.58 (1.14–2.19) 0.006
, n. Atorvastatin + torcetrapib (n=7533), n. Hazard ratio (95% CI) p. Major CV events (1.09–1.44) Deaths (1.14–2.19)")
65
Causas de muerte Muerte cardiovascular 35 49 Atorvastatina (n=59 )
Torcetrapib/ Atorvastatina (n=93) Muerte cardiovascular 35 49 Muerte subita 25 26 IAM fatal 6 8 ACV fatal 6 Otras muertes cardiacas 1 4 Insuficiencia cardiaca fatal 1 2 Otras muertes vasculares 2 3 Muerte no cardiovascular 20 40 Cancer 14 24 Infeccion 9 Otras causas no cardiovasculares 2 4 Trauma/suicidio/homicidio 4 3 Razon desconocida 4 4 Barter PJ, et al. N Engl J Med 2007;357:
 Muerte cardiovascular Muerte subita IAM fatal ACV fatal. 6. Otras muertes cardiacas Insuficiencia cardiaca fatal Otras muertes vasculares Muerte no cardiovascular Cancer Infeccion. 9. Otras causas no cardiovasculares Trauma/suicidio/homicidio Razon desconocida Barter PJ, et al. N Engl J Med 2007;357:")
66
Analisis post hoc en el grupo de Atorvastatina-Torcetrapib
Hazard ratios para muerte por Cardiopatia isquemica o IAM no fatal por quintiles de HDLc (grupo de referencia es HDL-C < 60 mg/dL ) 1.00 1.0 0.8 0.67 *P<0.05 * 0.57 0.6 * * CHD Death or Non-Fatal MI (Hazard Ratio) 0.47 0.43 0.4 0.2 <60 60-70 71-80 81-93 >93 Quintiles of HDL-C (mg/dL) at Month 3 Cox proportional hazard model adjusted for age, gender and baseline HDL-C. Excludes 265 patients with missing month 3 HDL-C.
 *P<0.05. * * * CHD Death or Non-Fatal MI. (Hazard Ratio) < >93. Quintiles of HDL-C (mg/dL) at Month 3. Cox proportional hazard model adjusted for age, gender and baseline HDL-C. Excludes 265 patients with missing month 3 HDL-C.")
67
Efectos farmacológicos de torcetrapib no relacionados a la inhibición de CETP
En los pacientes bajo tratamiento con torcetrapib/atorvastatina (pero no en los pacientes con solo atorvastatina) existía de forma significativa: Aumento de la tensión arterial Reducción del potasio sérico Aumento del bicarbonato sérico Aumento del sodio sérico Aumento de los niveles de aldosterona Estos cambios son consistentes con una activación del sistema renina-angiotensina
 existía de forma significativa: Aumento de la tensión arterial. Reducción del potasio sérico. Aumento del bicarbonato sérico. Aumento del sodio sérico. Aumento de los niveles de aldosterona. Estos cambios son consistentes con una activación del sistema renina-angiotensina.")
68
MAPA- 24 H DISLIPEMIA

Presentaciones similares
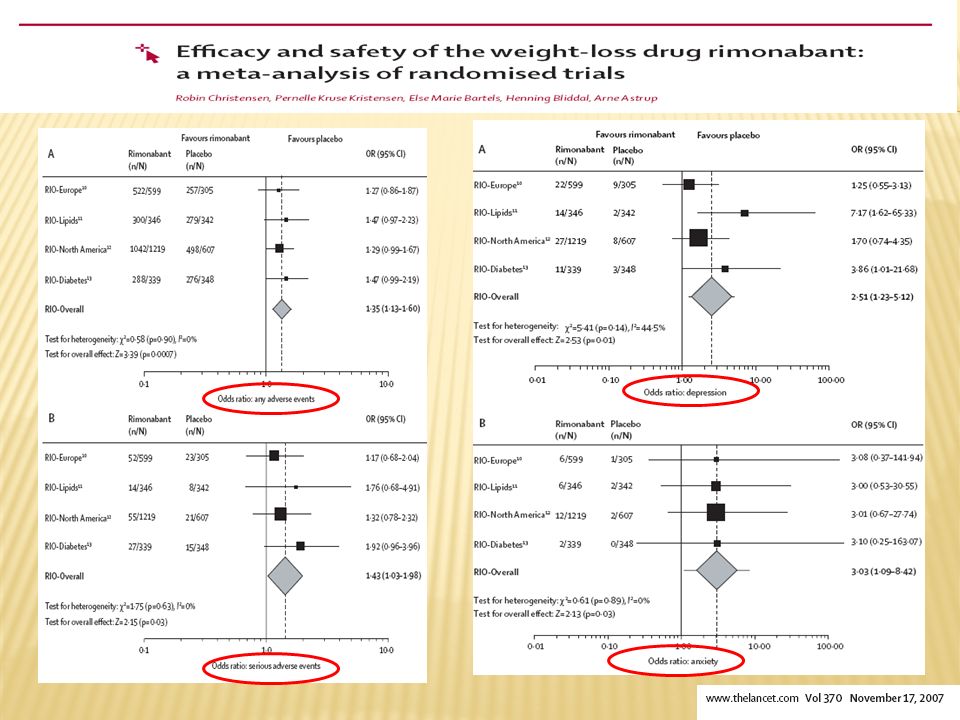
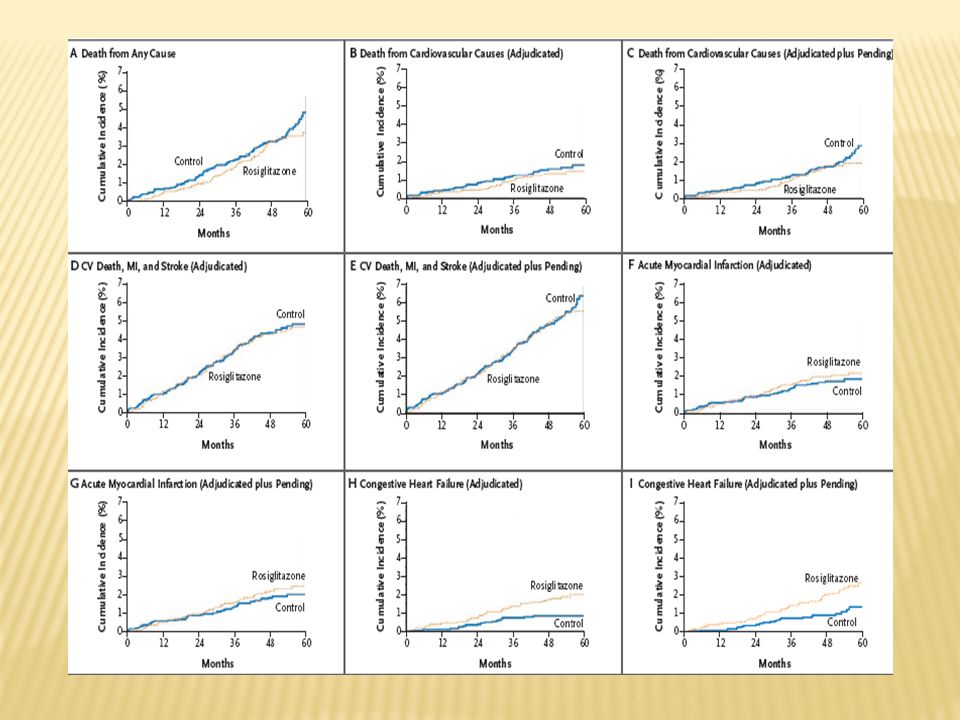
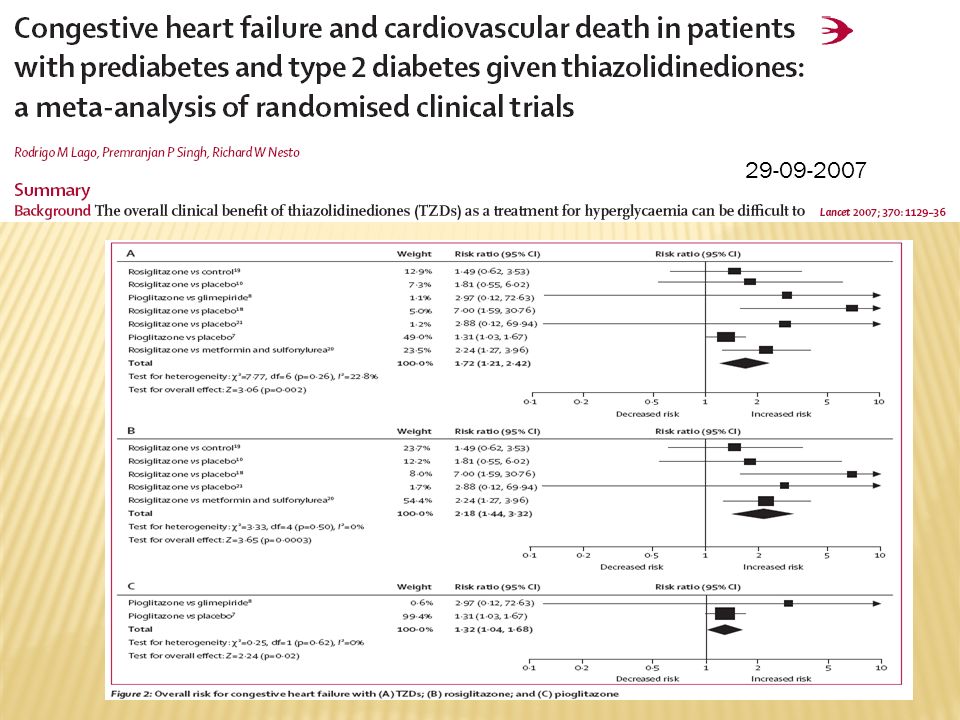
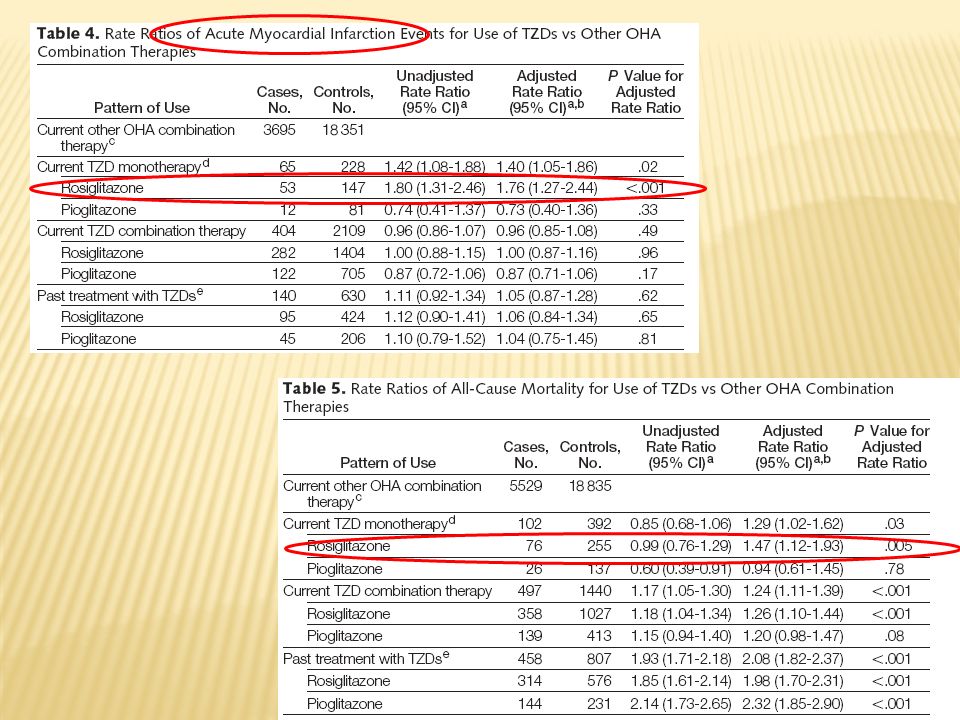
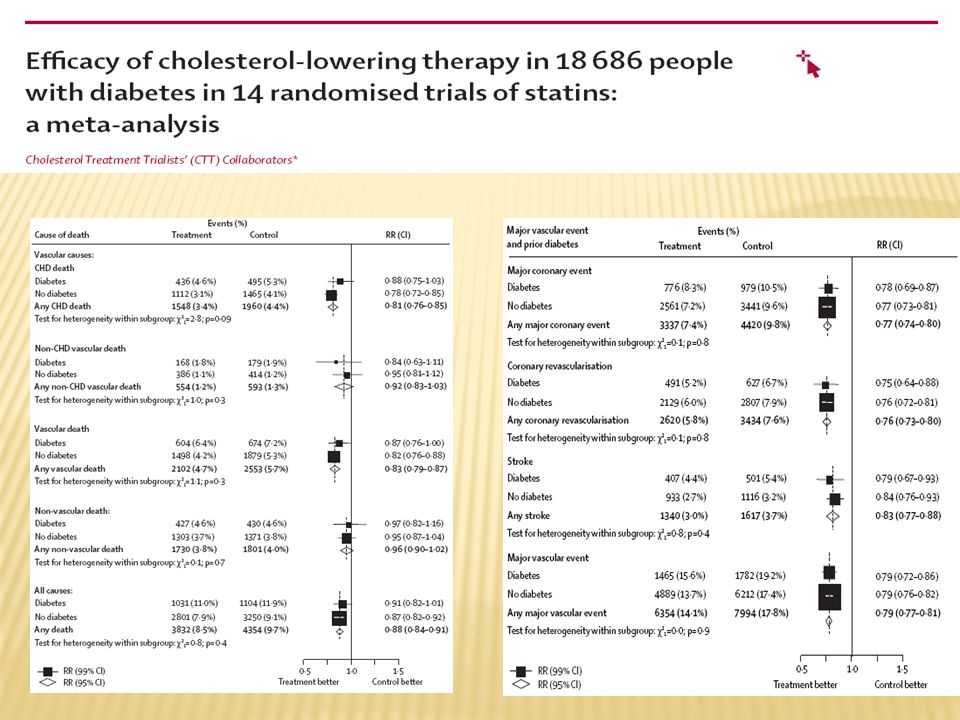



>")









en Ateroesclerosis. Seguridad y Eficacia Presentado en el.>")






