Descargar la presentación
La descarga está en progreso. Por favor, espere

1
JUAN LUIS JARAMILLO VALENCIA Residente Urología Universidad CES
ESTRATEGIAS DE PRESERVACIÓN VESICAL EN CÁNCER MÚSCULO-INVASIVO Tienen algún uso? JUAN LUIS JARAMILLO VALENCIA Residente Urología Universidad CES

2
EPIDEMIOLOGÍA Neoplasía mas común de sistema urinario
90% células transicionales nuevos casos y muertes en USA En la actualidad el tratamiento de elección en musculoinvasor es la qimio neoadyudaante seguido por la cistectomía radical + linfadenectomia 73 años Premo, Christopher. Trimodality Therapy un Bladder Cancer: Who, What and When. Urol Clin N Am 42 (2015) Adjuvant chemotherapy for muscle invasive urothelial carcinoma of the bladder. Up to date. 2015
 Adjuvant chemotherapy for muscle invasive urothelial carcinoma of the bladder. Up to date")
3
EPIDEMIOLOGÍA 12° 4° 70% no son músculo-invasores al diagnóstico
12° ° 70% no son músculo-invasores al diagnóstico La profundidad de la invasión es el factor pronóstico mas importante en la sobrevida y la recurrencia fourth most common cancer in men and the 12th most common cancer in women in the United States and Europe Premo, Christopher. Trimodality Therapy un Bladder Cancer: Who, What and When. Urol Clin N Am 42 (2015)
")
4
Opciones de manejo??

5
TERAPIAS CONSERVADORAS
RTU RTU + braquiterapia Cistectomía parcial Radiación + quimioterapia Recurrencia 5 años: 50% Problemas : alto riesgo de recurrecia en cualquien parte del sistema urinario E ha estimado riesgo de recurrencia hasta del 50% a 5 años Bladder preservation treatment options for muscleinvasive urothelial bladder cáncer, UpToDate 2015

6
J. A. Witjes (Chair), E. Compérat, N. C. Cowan
J.A. Witjes (Chair), E. Compérat, N.C. Cowan. Guidelines on Muscle-invasive and Metastatic Bladder Cancer. European Association of Urology 2015
, E. Compérat, N.C. Cowan. Guidelines on Muscle-invasive and Metastatic Bladder Cancer. European Association of Urology")
7
NO ES UNA ALTERANTIVA ACEPTABLE
RADIOTERAPIA INDICACIÓN Pacientes de edad avanzada Paliación de síntomas locales Recurrencia después de Rt sola 70% Sobrevida a 5 años 20-40% All available data suggest that concurrent chemotherapy-RT is more effective than RT alone (level of evidence [LoE]: 1b In most North American trials, treatment includes an initial course of RT to a total dose of 39.6 to 45 Gy directed at the pelvic lymph nodes below the bifurcation of the common iliac vessels, the prostate in men, and the whole bladde The rationale for including pelvic lymph nodes in the initial portion of the radiation treatment field relates to the high rate of occult lymph node involvement in regions typically targeted with pelvic RT33 and the finding that extensive lymphadenectomy at the time of RC improves survival, suggesting that treatment of these lymph nodes has therapeutic efficacy NO ES UNA ALTERANTIVA ACEPTABLE Radical cystectomy and bladdersparing treatments for urothelial bladder cancer. UpToDate2015

8
RADIOTERAPIA Componente crítico de TMT Variable
Dosis de irradiación Esquemas de fraccionamiento Secuencias de tratamiento Volumen de tratamiento Técnicas: Radioterapia de intensidad modulada (IMRT) Radioterapia guiada por imágenes (IGRT) 64-66 Gy en fracciones 55 Gy en 20 fracciones Premo, Christopher. Trimodality Therapy un Bladder Cancer: Who, What and When. Urol Clin N Am 42 (2015)
 Radioterapia guiada por imágenes (IGRT) Gy en fracciones. 55 Gy en 20 fracciones. Premo, Christopher. Trimodality Therapy un Bladder Cancer: Who, What and When. Urol Clin N Am 42 (2015)")
9
Simulacíón previa con vejiga vacia con poco contraste
Premo, Christopher. Trimodality Therapy un Bladder Cancer: Who, What and When. Urol Clin N Am 42 (2015)
")
10
RADIOTERAPIA DE INTENSIDAD MODULADA
Premo, Christopher. Trimodality Therapy un Bladder Cancer: Who, What and When. Urol Clin N Am 42 (2015)
")
11
Datos no concluyentes, por lo cual aún no se recomienda
BRAQUITERAPIA INDICACIONES Únicos Menores de 5 cm Datos no concluyentes, por lo cual aún no se recomienda Radical cystectomy and bladdersparing treatments for urothelial bladder cancer. UpToDate2015

12
Mejores resultados: Terapia trimodal (TMT)
RTU Vesical / Quimioradioterapia concurrente CR Salvamento J.A. Witjes (Chair), E. Compérat, N.C. Cowan. Guidelines on Muscle-invasive and Metastatic Bladder Cancer. European Association of Urology 2015
, E. Compérat, N.C. Cowan. Guidelines on Muscle-invasive and Metastatic Bladder Cancer. European Association of Urology")
13
TERAPIA MULTIMODAL RC: 70%
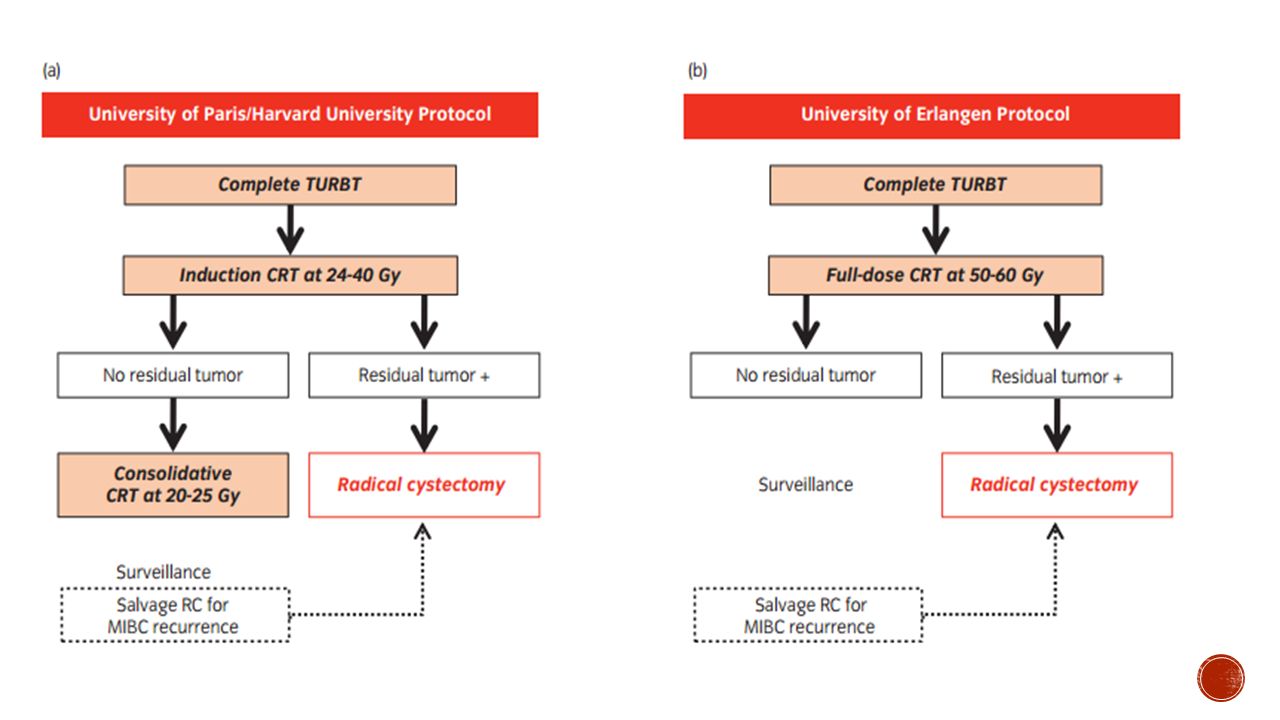
RTUV + radiación + quimioterapia : “terapia trimodal” 1980 Universidad de París, Harvard y Erlanger RC: 70% Respuesta completa a la quimioradiacion : citología negativa después del tratamiento, tumor no visible o biopsias negativas en la cistscopia La respuesta completa en pacientes con T2-T4a sometidos a terapia multimodal es del 70% Overview of the initial approach and management of urothelial bladder cancer. UpToDate.2015

14
CRITERIOS DE SELECCIÓN
complete response (CR) to induction therapy with concurrent chemoradiation has typically been defined as negative results on urine cytologic analysis, as well as no visible tumor and negative results on biopsies at cystoscopy . The CR rate for patients with T2-T4a disease treated with TMT is approximately 70% Premo, Christopher. Trimodality Therapy un Bladder Cancer: Who, What and When. Urol Clin N Am 42 (2015)
 to induction therapy with concurrent chemoradiation has typically been defined as negative results on urine cytologic analysis, as well as no visible tumor and negative results on biopsies at cystoscopy . The CR rate for patients with T2-T4a disease treated with TMT is approximately 70% Premo, Christopher. Trimodality Therapy un Bladder Cancer: Who, What and When. Urol Clin N Am 42 (2015)")
15
OTROS CANDIDATOS No candidatos a cirugía
Deseo de conservar vejiga nativa Cáncer urotelial Tumores unifocales <5cm No ubicación en el domo los no uroteliales tiene menor respuesta a la quimioterapia y radioterapia Overview of the initial approach and management of urothelial bladder cancer. UpToDate.2015 Bladder preservation treatment options for muscleinvasive urothelial bladder cáncer, UpToDate 2015

16
FACTORES ASOCIADO A RESPUESTA COMPLETA
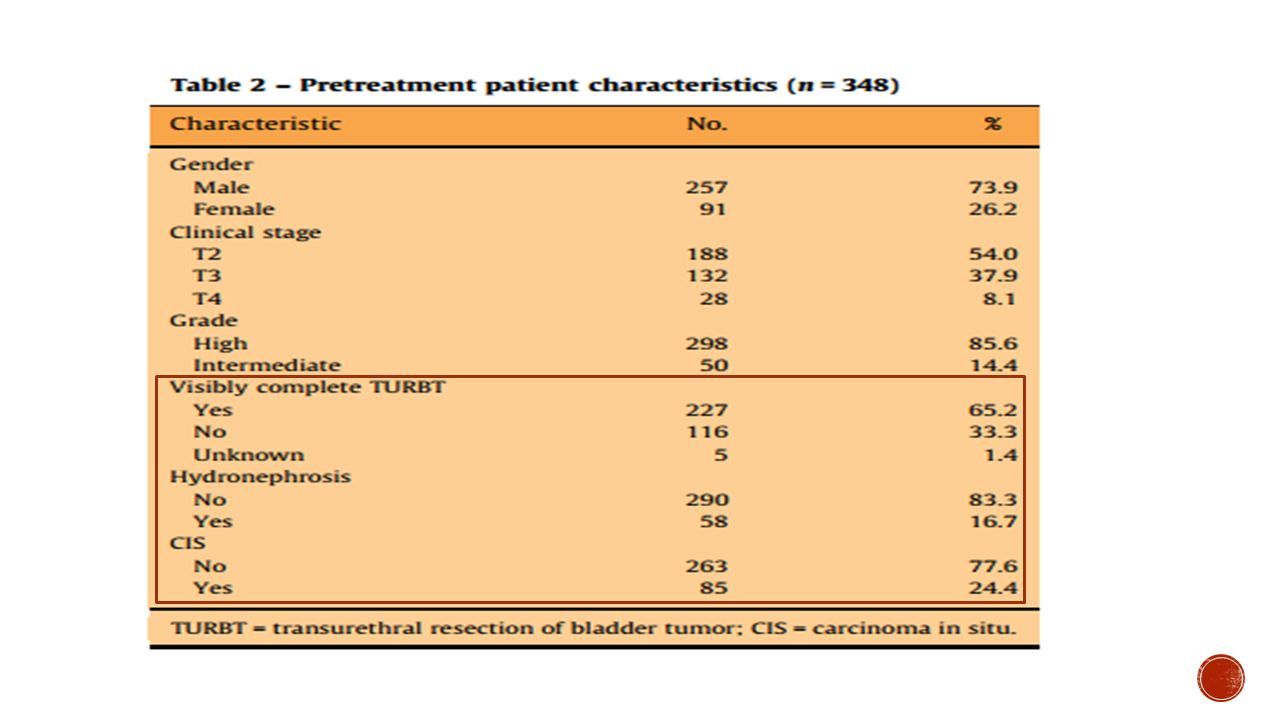
RTUV Completa Estadio tumoral Hidronefrosis Multifocalidad CIS Función vesical basal rate of response to induction therapy may not always be known, as many recent trials, such as bladder cancer 2001 (BC2001) and Radiation Therapy Oncology Group (RTOG) 0926, do not include cystoscopic reassessment after induction the Erlangen series showed that completeness of resection after initial TURBT was an independent predictor of CR Multiple tumors or multifocal disease has been suggested as a predictive factor for decreased response rates to TMT. . Multifocality may not predict for lower rates of CR but is associated with a higher risk for local relapse ogie suggested that the presence of extensive CIS should be considered a relative and not absolute contraindication to TMT because the presence of CIS affects only the risk of recurrence after TMT and not survival. Premo, Christopher. Trimodality Therapy un Bladder Cancer: Who, What and When. Urol Clin N Am 42 (2015)
 and. Radiation Therapy Oncology Group (RTOG) 0926, do not include cystoscopic reassessment after induction. the Erlangen series showed that completeness of resection after initial TURBT was an independent predictor of CR. Multiple tumors or multifocal disease has been suggested as a predictive factor for decreased response rates to TMT. . Multifocality may not predict for lower rates of CR but is associated with a higher risk for local relapse. ogie suggested that the presence of extensive CIS should be considered a relative and not absolute contraindication to TMT because the presence of CIS affects only the risk of recurrence after TMT and not survival. Premo, Christopher. Trimodality Therapy un Bladder Cancer: Who, What and When. Urol Clin N Am 42 (2015)")
17
Resección Transuretral
CANDIDATOS Únicos Ubicación en trígono o paredes laterales 79% cuando es una RTU visible Vs 57% cuando no es visible Radical cystectomy and bladdersparing treatments for urothelial bladder cancer. UpToDate2015

18
La incidencia de P0 en pacientes cT2 es del 31% con una sobrevvida a 5 años del 85% : sugieren que algunos pacientes con musculoinvaso pueden ser tratador solo con TUV Analizaron una serie prospectiva de pacientes con musculoinvasor como monoterapia con minimo 15 años de seguimiento Criterios de exclusión Tumor residual macroscópico, hidronefrosis o compromiso ganglionar, tumores mayores a 3 cm Segumiento Cistoscopia cada 3 meses por 2 años, luego cada 6 meses por 3 años y luego anualmente Imágenes : TAC o RNM + rx de torax cada 3 meses por 1 años, luego cada 6 meses por 4 años CONCLUSION Radical transurethral bladder tumor resection is a reliable therapeutic approach for patients with muscle invasive bladder cancer after complete tumor resection and with negative biopsies of the tumor bed. These results are consistent in all age ranges.

19
RESECCIÓN TRANSURETRAL
“Es conocido que la RTU de vejiga sola brinda un control oncológico inadecuado en cáncer vesical músculo-invasor con altas tasas de recurrencia y progresión” It is generally recognised that TUR alone provides inadequate cancer control and leads to a high rate of BCa recurrence and progression Criti cal Analysis of Bladder Sparing with Trimodal Therapy in Muscle-invasive Bladder Cancer: A Systematic Review- e u r o p e a n u r o l o g y ( )
")
20
RESECCIóN TRAnSURETRAL
RTOG Erlangen Massachusetts General Hospital tasas de RC (79% vs 57%) Una RTUV menos que completa no es un contraindicación absoluta para preservación vesical Premo, Christopher. Trimodality Therapy un Bladder Cancer: Who, What and When. Urol Clin N Am 42 (2015)
 Una RTUV menos que completa no es un contraindicación absoluta para preservación vesical. Premo, Christopher. Trimodality Therapy un Bladder Cancer: Who, What and When. Urol Clin N Am 42 (2015)")
21
HIDRONEFROSIS Predictor etapa avanzada y disminución de OS RTOG 89-03:
OS a 5 años 33% y sin 54% Ha sido criterio de exclusión en varios ensayos de TMT. RTOG 89-03 RC HNF 38% y sin 64% Hospital General de Massachusetts tasa RC con HNF 52% y sin 77% Pacientes con HNF malos candidatos para preservación vesical Premo, Christopher. Trimodality Therapy un Bladder Cancer: Who, What and When. Urol Clin N Am 42 (2015)
")
22
MODALIDADES TRT SPLIT CONTINUO
Massachusetts General Hospital (MGH) y Radiation Therapy Oncology Group (RTOG) RTUV QT RDT Inducción Cistoscopia CR: QT-RDT Consolidación No CR: Cistectomía radical The University of Erlangen RTUV CRT curso completo No respuesta cistectomía salvamento Continuo : cistoscopia + biopsia +citología una vez se termine 1 a 3 meses después de terminado el ciclo
 y Radiation Therapy Oncology Group (RTOG) RTUV. QT RDT Inducción. Cistoscopia. CR: QT-RDT Consolidación. No CR: Cistectomía radical. The University of Erlangen. RTUV. CRT curso completo. No respuesta. cistectomía salvamento. Continuo : cistoscopia + biopsia +citología una vez se termine 1 a 3 meses después de terminado el ciclo.")
24
Búsqueda literatura en Ingles 1990 – 2013
Comparación Regimen continuo y dos fases (Split)
")
25
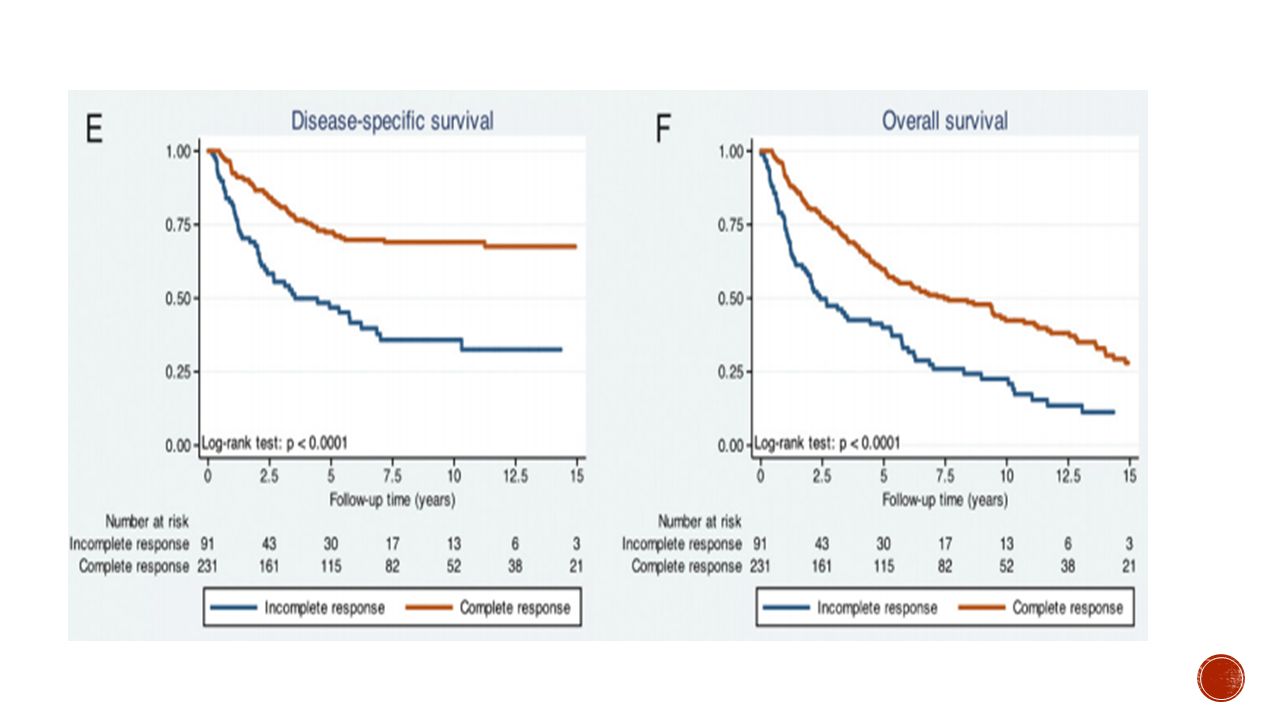
therate of complete response (CR), local muscle-invasive local failure (LF), salvage cystectomy (SC), 5-year overall survival (OS) and 5-yearbladder intact survival (BIS) from 3315 patients
, local muscle-invasive local failure (LF), salvage cystectomy (SC), 5-year overall survival (OS) and 5-yearbladder intact survival (BIS) from 3315 patients")
26
OS 5 años No hubo diferencias significativas entre los dos regímenes de tratamiento
Los peores resultados se observaron en pacientes con estadio> T2 o uropatía obstructiva > Eficaz terapia continua > RC Mejor la continua en cuando a tasas de remisión completa y cistectomías de salvamente

27
Estudio multicéntrico, fase 3 , Asignación aleatoria
360 pacientes radioterapia con o sin quimioterapia concurrente QT fluorouracilo y mitomicina

28
RESULTADOS A los 2 años A los 5 años
supervivencia libre de enfermedad locorregional QT RDT 67% RDT 54% seguimiento de 69,9 A los 5 años supervivencia global QT RDT 48% RDT 35% EA grado 3 o 4 > quimiorradioterapia 36,0% vs. 27,5%

29
RT externa a la vejiga y linfáticos pélvicos: Dosis inicial de 40 Gy
RT externa a la vejiga y linfáticos pélvicos: Dosis inicial de 40 Gy Refuerzo vesical de 54 Gy QT: cisplatino y mitomicina+ 5 fluorouracilo A systematic literature search in the PubMed and Cochrane databases was performed from 1980 to July 2013 Optimal bladder-preservation treatment includes a safe transurethral resection of the bladder tumour as complete as possible followed by radiation therapy (RT) with concurrent radiosensitising chemotherapy Un esquema de radiación estándar incluye RT externa a la vejiga y linfáticos pélvicos a una dosis inicial de 40 Gy y con un refuerzo vesical de 54 Gy: hasta obtener una dosis total de Gy Radiosensitising chemotherapycon r cisplatin and mitomycin C plus 5-fluorouracil cystoscopic assessment with systematic rebiopsy should be performed at TMT completion or early after TMT induction. Thus, nonresponders are identified early to promptly offer salvage RC of neoadjuvant or adjuvant chemotherapy. Critical to The best cancers eligible for bladder preservation are those with low-volume T2 disease without hydronephrosis or extensive carcinoma in situ Dosis total Gy
 with concurrent radiosensitising chemotherapy. Un esquema de radiación estándar incluye RT externa a la vejiga y linfáticos pélvicos a una dosis inicial de 40 Gy y con un refuerzo vesical de 54 Gy: hasta obtener una dosis total de Gy. Radiosensitising chemotherapycon r cisplatin and mitomycin C plus 5-fluorouracil. cystoscopic assessment with systematic rebiopsy should be performed at TMT completion or early after TMT induction. Thus, nonresponders are identified early to promptly offer salvage RC. of neoadjuvant or adjuvant chemotherapy. Critical to. The best cancers eligible for bladder preservation are those with low-volume T2 disease without hydronephrosis or extensive carcinoma in situ. Dosis total Gy.")
30
most planned radiation regimens included RT to a limited pelvic region (typically to the mid-sacroiliac region, with an upper limit of the common iliac artery bifurcation The rationale for including a limited pelvic field is that regional nodal involvement is not uncommon in muscle-invasive disease; yet, by limiting the nodal fields in size and dose (40–45 Gy), the treatments are designed to potentially conserve the small bowel for future urinary diversions, if necessary To date, in most ofprotocols, chemotherapy with cisplatin is the usual radiosensitising drug in those with adequate renal function and remains a standard ofcare as no published head-to-head phase 3 trial has examined noncisplatin regimens versus cisplatin in BCa patients treated with TMT with regard to efficacy and the safety profile
, the treatments are designed to potentially conserve the small bowel for future urinary diversions, if necessary. To date, in most ofprotocols, chemotherapy with cisplatin is the usual radiosensitising drug in those with adequate renal function and remains a standard ofcare as no published head-to-head phase 3 trial has examined noncisplatin regimens versus cisplatin in BCa patients treated with TMT with regard to efficacy and the safety profile.")
31
Resultados 5 años CS: 25-30% OS: 36-82% CSS: 50-82%
sobrevida especifca por cancer 50-82% a 5 años Sobrevida global % a 5 años Cistectomia de salvamento 25-30% a 5 años No hay datos que soporten el beneficio del uso de quimioterapia neadyudante o adyudante CONCLUSIO : la terapia trimodal es una buena opscon en pacientes muy bien seleccionados

32
RTUV+quimioradición 64-65Gy Re-biopsia 40Gy
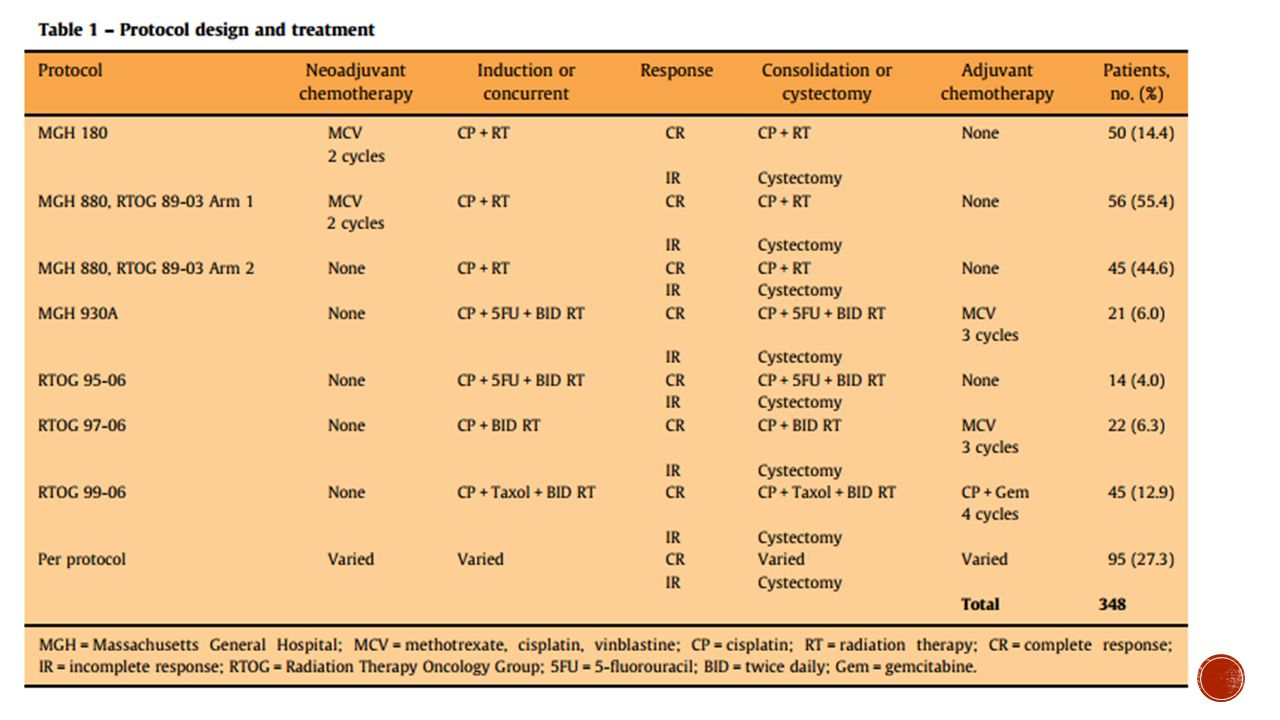
348 pacientes T2-T4 RTUV+quimioradición 64-65Gy Re-biopsia 40Gy 348 paciesntes , T2T4 RTUV + quimioradiacion 64-65Gy + quimioterapia con cisplatino (algunos pacientes recibieron quimio neoadyudante o qui io adyudante ) Todos biopsia después de 40 Gy Segumiento promedio 7.7 años Respuesta comleta después de la quimioradiacion 72% y 78% para ls paociente con enfermedad T2 Sobrevida global 5 años 52% , 10 ALÑOS 35% Cistectomia radica se neesito en 102 pacientes (29%) : 60 por mala respuesta a la quimioradiacion y 42 por ivasion durate el seguimiento Seguimiento rebipsia examen bimanual bajo anestesia general citología y radiología cistoscopia cada 3 meses por el rimer año, luego cada 3-4 meses en el segundo año y uego cada 6 meses por 3 años
 Todos biopsia después de 40 Gy. Segumiento promedio 7.7 años. Respuesta comleta después de la quimioradiacion 72% y 78% para ls paociente con enfermedad T2. Sobrevida global 5 años 52% , 10 ALÑOS 35% Cistectomia radica se neesito en 102 pacientes (29%) : 60 por mala respuesta a la quimioradiacion y 42 por ivasion durate el seguimiento. Seguimiento rebipsia examen bimanual bajo anestesia general citología y radiología. cistoscopia cada 3 meses por el rimer año, luego cada 3-4 meses en el segundo año y uego cada 6 meses por 3 años.")
35
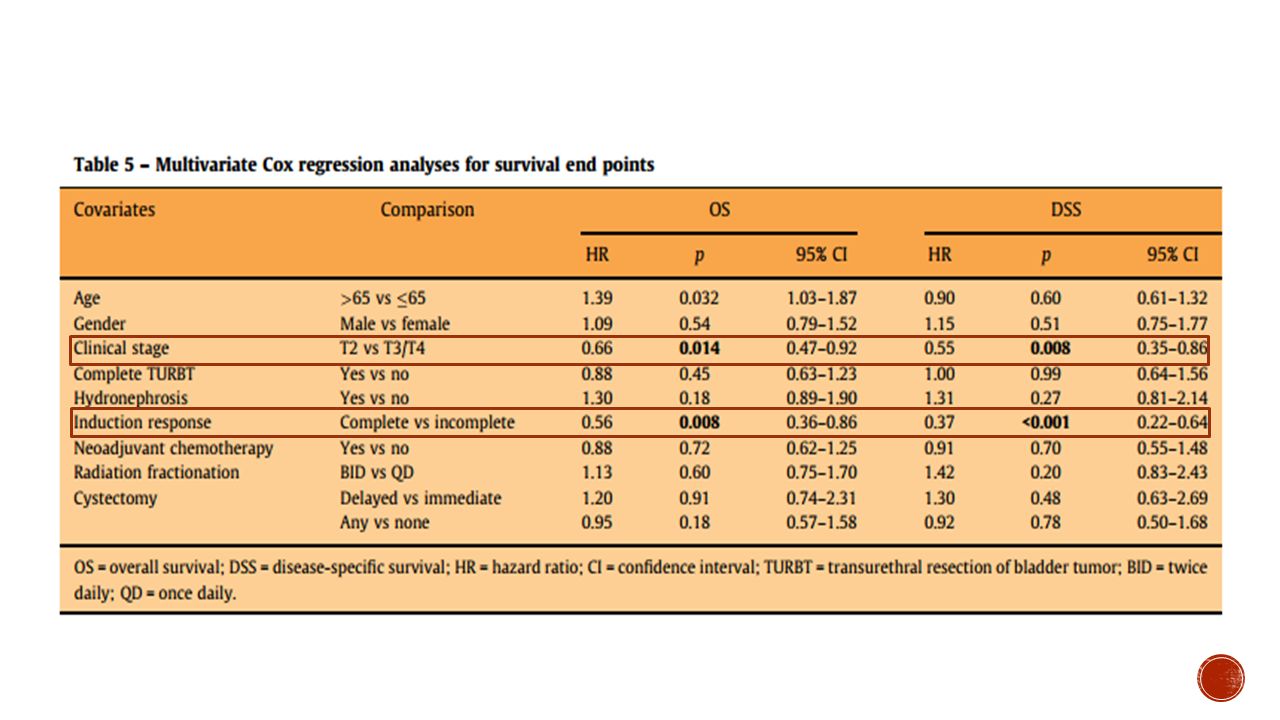
T2 5 años 74% 10 años 67% 15 años 63% T3–4 5 años 53%, 10 años 49%
DSS : T2 5 años 74%, 10 años 67%, 15 años 63% T3–4 5 años 53%, 10 años 49%, 15 años 49%, OS T2 5 años 61%, 10 años 43%, 15 años 28% T3–4 5 años 41%, 10 años 27%, 15 años16% T2 5 años 74% 10 años 67% 15 años 63% T3–4 5 años 53%, 10 años 49% 15 años 49% T2 5 años 61% 10 años 43% 15 años 28% T3–4 5 años 41% 10 años 27% 15 años16%

37
Las P en negrilla están relacionadas con mejoría en la sobrevida global y la supervivencia especifica por enfermedad

39
Para pacientes no candidatos a cistectomía, la terapia trimodal es una opción de preservación vesical con altas tasas de sobrevida a largo plazo . Se requiere de un equipo multidisciplinario para lograr estos resultados.

40
Exclusión: compromiso nodal o metástasis
6 estudios 5 estudios fase II (RTOG 8802, , 9706, 9906, and 0233) 1 studio fase III (RTOG 8903) Exclusión: compromiso nodal o metástasis T2 61% T3 35% T4 4% Seguimiento 4.3 años ( 7.8 años sobrevivientes) (205) 468 pacientes, en 6 estudios five phase II studies (RTOG 8802, 9506, 9706, 9906, and 0233) and one phase III study (RTOG 8903 T2-T4a, 66 años T2 61% T3 35% T4 4% Exclusion: compromiso nodal o metástasis Seguimiento promedi 4.3 años , pero los sobrevivientes hasta 7.8 años (205) RESULTADOS
 1 studio fase III (RTOG 8903) Exclusión: compromiso nodal o metástasis. T2 61% T3 35% T4 4% Seguimiento 4.3 años ( 7.8 años sobrevivientes) (205) 468 pacientes, en 6 estudios five phase II studies (RTOG 8802, 9506, 9706, 9906, and 0233) and one phase III study (RTOG T2-T4a, 66 años. T2 61% T3 35% T4 4% Exclusion: compromiso nodal o metástasis. Seguimiento promedi 4.3 años , pero los sobrevivientes hasta 7.8 años (205) RESULTADOS.")
41
RC después de quimioradiación: 69% Sobrevida enfermedad especifica
5 años 71% 10 años 65% Recaída enfermedad músculo invasora 5 años 13 % 10 años 14% Recaída de enfermedad no invasora : 5 años 31% 10 años 36% Metástasis a distancia: 10 años 35% Sobrevida global : 5 años 57% 10 años 36%

42
Respuesta completa después de quimioradiacion 69%
Sbrevida especifica de enfemedad: 5 aos 71% y 10 años 65% Reciada de enfermedad musculos invasora 5 años 13 % y 10 años 14% Recaida de enfermedad no invasora : 31% a 5 años y 36% a 10 años Metastaisis a distencia : 31 % a 5 años y 35% a10 años Sobrevida global : 5 años 57% Y 10 ÑAOS 36% Del los 205 pacienets que estaban vivos a los 5 aos : 80% tenían la vejiga intacta

43
La sobrevida especifica por enfermedad en la terapia trimodal en los diferentes estudios es comparable con la cistectomía inmediata en paciente con tumor músculo invasor en estadios similares. Dada la baja tasa de recurrencia a largo plazo, la terapia trimodal es considerada una alternativa a la cistectomía, especialmente en pacientes que no son buenos candidatos a cirugía. C o n c l u s i o n This pooled analysis of multicenter, prospective RTOG bladder-preserving CMT protocols demonstrates long-term DSS comparable to modern immediate cystectomy studies, for patients with similarly staged MIBC. Given the low incidence of late recurrences with long-term follow-up, CMT can be considered as an alternative to radical cystectomy, especially in elderly patients not well suited for surgery.

44
RESULTADOS TERAPIA TRIMODAL
Resultados prospectivos y retrospectivos similares a los obtenidos después de cistectomía radical en OS CR 70% OS 73% Sobrevida cáncer especifica 50% -82%. Conservación vesical 80% a los 5 años Guillaume Ploussard. Critical Analysis of Bladder Sparing with Trimodal Therapy in Muscle-invasive Bladder Cancer: A Systematic Review. European Urology. 66 (2014) 120–137
 120–137.")
45
v Premo, Christopher. Trimodality Therapy un Bladder Cancer: Who, What and When. Urol Clin N Am 42 (2015)
")
46
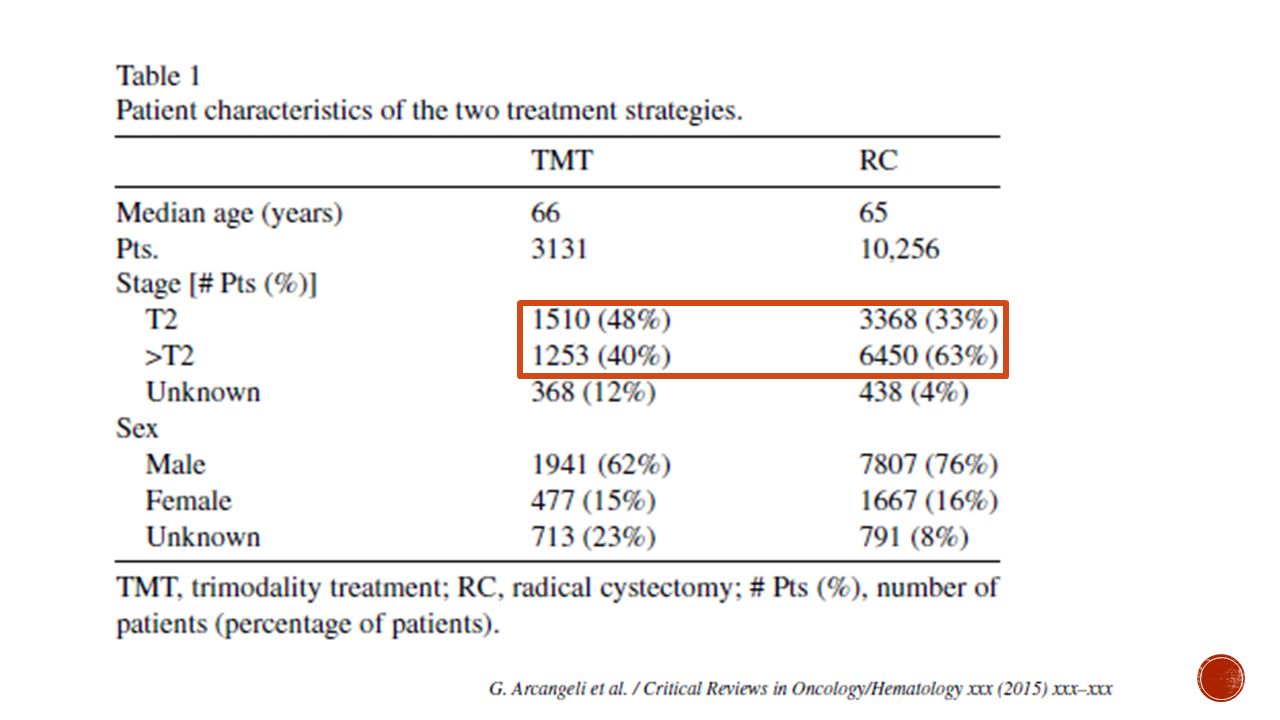
TMT inferior a la cistectomía?
Discrepancia en 50% entre clínica y espécimen La terapia trimodal es una alterantiva o es equiparable a ciectomia radica ???’ bladder preservation strategy by TMT is still perceived by many urologists to be inferior in terms of survival when compared with RC, although no randomized trials support this bias Clinical staging is known to under-stage a large portion of patients compared with surgical staging. The stage discrepancy can occur in up to 50% of patients .

47
MATERIALES Y METODOS Ausencia de ensayos aleatorizados controlados
estudios prospectivos y retrospectivos. No se incluyeron pacientes con ganglios regionales clínicamente positivos Not included were studies on patients with clinically positive regional nodes or distant metastases or non muscle-invasive cancer, or patients receiving partial cystectomy or radiotherapy alone the endpoint of interest for the present analysis was limited to 5-year OS rate

49
The median 5-year OS rate was 57% in the TMT group, when compared with 52% (P = 0.04), 51% (P = 0.02) and 53% (P = 0.38) in the whole group receiving RC or the group treated with RC alone or RC + chemotherapy, respectively The hazard risk (HR) of mortality of patients treated with TMT or RC was 1.22 (95% CI = 1.13–1.32) with an absolute benefit of 5% in favor of the former. The HR of mortality from TMT persisted significantly better not only versus the group treated with RC alone (HR = 1.22; 95% CI = 1.12–1.32), but also versus the group receiving RC + chemotherapy (HR = 1.22; 95% CI = 1.09–1.36)
, but also versus the group receiving RC + chemotherapy (HR = 1.22; 95% CI = 1.09–1.36).")
50
DISCUSIÓN La mayoría ECA fase III no llegan a su fin
Falta de interés de muchos urólogos Problema de la asignación al azar No adherencia TMT Muestra heterogénea tipo paciente, estadio tumoral, modalidad de tratamiento y presentación de datos

51
CONCLUSIóN Verdadera ventaja en OS a 5 años de TMT sobre RC
No diferencia en subgrupos T2 o > T2 TMT debería opción de tratamiento en vez de una alternativa a la RC en el tratamiento para MIBC Elección bien informada Preferencias y necesidades individuales Compared with RC, TMT seems to be associated with a better outcome for patients with muscle-invasive bladder cancer (MIBC)
")
52
TOXICIDAD AGUDA DE TMT Toxicidad tolerable
Principales hematológica, gastrointestinal y genitourinario neuropatía QT Cisplatino BC2001 : No aumento de toxicidad grado 3-4 con QT concurrente en comparación con RT sola Guillaume Ploussard. Critical Analysis of Bladder Sparing with Trimodal Therapy in Muscle-invasive Bladder Cancer: A Systematic Review. European Urology. 66 (2014) 120–137
 120–137.")
53
Guillaume Ploussard. Critical Analysis of Bladder Sparing with Trimodal Therapy in Muscle-invasive Bladder Cancer: A Systematic Review. European Urology. 66 (2014) 120–137
 120–137.")
54
TOXICIDAD TARDIA No datos suficientes toxicidad después de 5 años
La tasa de estas complicaciones varía entre estudio Toxicidad G I -II GU 10% a 25% GI 5% a 6% urgencia, nocturia, disuria, diarrea, proctitis , cistitis hemorrágica, estenosis uretral Guillaume Ploussard. Critical Analysis of Bladder Sparing with Trimodal Therapy in Muscle-invasive Bladder Cancer: A Systematic Review. European Urology. 66 (2014) 120–137
 120–137.")
55
SEGUIMIENTO EN TERAPIA CONSERVADORA
Cistoscopia y citología Cada 3 meses por los primeros 2 años Cada 6 meses 2-5 años Luego cada año Overview of the initial approach and management of urothelial bladder cancer. UpToDate.2015

56
RECURRENCIA DESPUÉS DE MANEJO CONSERVADOR
Cistectomía de salvamento: sobrevida 40-50% (lo que representa % menos comparado con la cirugía inmediata) Radical cystectomy and bladdersparing treatments for urothelial bladder cancer. UpToDate2015
 Radical cystectomy and bladdersparing treatments for urothelial bladder cancer. UpToDate2015.")
57
CISTECTOMÍA PARCIAL CONTRAINDICACIONES INDICACIONES CIS Único
Localización anterior o domo En divertículos CIS Compromiso de uretra Recurrencia de tumores vesicales o uroteliales altos Se popularizo en 1950 pero por las altas tasas de recurrencia tan altas asta del 80% Margen 2 cm Radical cystectomy and bladdersparing treatments for urothelial bladder cancer. UpToDate2015

58
THE JOURNAL OF UROLOGY, Vol. 175, 2058-2062, June 2006
pacientes Sobrevida 67% Sobrevida libre de recurrencia 39% Sobrevida especifica por enfermedad 87% a 5 años todos Seguimiento 72.6 meses 19/37 (51% no tuvieron recurrencia , 9(24) recurrencia superficial y 9 (24%) recurrencia avanzada En el analisis multivariado un estadio atologico alto fue asociad cn menor tiempo de recurrencia (HR 3.4, p 0.04 use of adjuvant chemotherapy (HR 0.18, p 0.03) was associated with prolonged advanced recurrence-free survival, however adjuvant chemotherapy did not impact overall survival. THE JOURNAL OF UROLOGY, Vol. 175, , June 2006
 recurrencia superficial y 9 (24%) recurrencia avanzada. En el analisis multivariado un estadio atologico alto fue asociad cn menor tiempo de recurrencia (HR 3.4, p use of adjuvant chemotherapy (HR 0.18, p 0.03) was associated with prolonged advanced recurrence-free survival, however adjuvant chemotherapy did not impact overall survival. THE JOURNAL OF UROLOGY, Vol. 175, , June")
59
THE JOURNAL OF UROLOGY, Vol. 175, 2058-2062, June 2006
Conclusion: paciente s seleccionados con Ca musculoinvasor particularmente sin historia de tumor vesical previo , generalmente lo usaban cuando había que reimplantar el uréter THE JOURNAL OF UROLOGY, Vol. 175, , June 2006

60
Tamaño tumoral: asociado a recurrencia, <p 0,03
Tumor único Recurrencia?? 5 años Libre de recurrencia 64% Sobevida enfermdad especifica:84% Sobrevida global: 70%, 25 pacientes Tumor único, recibieron rt localizada previamente , dosis única de quimio intravesical y luego BCG posoperatoria Querian evaluar las variables de recurrencia 25 patient TURBT), all had a solitary primary T2 (68%) or T1HG (32%) lesion with no evidence of carcinoma in situ. At follow-up (mean 45.3 meses 5-year recurrence-free 64% disease-specific84% and overall 70%, . 8% of patients experienced intravesical non–muscle-invasive tumor recurrences and were treated with TURBT and intravesical chemotherapy. Twenty percent recurred with locally dvanced tumors or visceral metastasis and were treated with systemic chemotherapy, local resection or cystectomy, On univariate analysis, only tumor size at time of partial cystectomy (P .03) was significantly associated with tumor recurrence Tamaño tumoral: asociado a recurrencia, <p 0,03
, all had a solitary primary T2 (68%) or T1HG (32%) lesion with no evidence of carcinoma in situ. At follow-up (mean 45.3 meses. 5-year recurrence-free 64% disease-specific84% and overall 70%, . 8% of patients experienced intravesical non–muscle-invasive tumor recurrences and were treated with TURBT and intravesical chemotherapy. Twenty percent recurred with locally dvanced tumors or visceral metastasis and were treated with systemic chemotherapy, local resection or cystectomy, On univariate analysis, only tumor size at time of partial cystectomy (P .03) was significantly associated with tumor recurrence. Tamaño tumoral: asociado a recurrencia, <p 0,03.")
61
CISTECTOMÍA RADICAL Sobrevida 50-65% (80% pT2)
El estadio tumoral y compromiso nodal son predictores independientes de sobrevida Pacientes con enfermedad localmente avanzada donde los resultados son menores Tasa de complicaciones del 30% y mortalidad perioperatoria 2-3% Adjuvant chemotherapy for muscle invasive urothelial carcinoma of the bladder. Up to date. 2015

62
CISTECTOMÍA RADICAL Mortlidad de la cistectomía a 90 días
< 69 años : 2% 70-79 aos : 5 % > 80 años : 9 % El segumiento a largo plazo ha demostrado que los procedimieos minimamente invasivos no tiene equivalencaia oncológica con respecto a los proceimientos sbiertos Bladder preservation treatment options for muscleinvasive urothelial bladder cáncer, UpToDate 2015

63
Platinum-based combination chemotherapy showed a significant benefit to overall survival (combined hazard ratio [HR] 0·87 [95% CI 0·78–0·98, p=0·016]; 13% reduction in risk of death; 5% absolute benefit at 5 years [1–7]; overall survival increased from 45% to 50%). This effect was observed irrespective of the type of local treatment, and did not vary between subgroups of patients Lancet 2003; 361: 1927–34
![Platinum-based combination chemotherapy showed a significant benefit to overall survival (combined hazard ratio [HR] 0·87 [95% CI 0·78–0·98, p=0·016]; 13% reduction in risk of death; 5% absolute benefit at 5 years [1–7]; overall survival increased from 45% to 50%). This effect was observed irrespective of the type of local treatment, and did not vary between subgroups of patients](http://slideplayer.es/slide/9130993/27/images/63/Platinum-based+combination+chemotherapy+showed+a+significant+benefit+to+overall+survival+%28combined+hazard+ratio+%5BHR%5D+0%C2%B787+%5B95%25+CI+0%C2%B778%E2%80%930%C2%B798%2C+p%3D0%C2%B7016%5D%3B+13%25+reduction+in+risk+of+death%3B+5%25+absolute+benefit+at+5+years+%5B1%E2%80%937%5D%3B+overall+survival+increased+from+45%25+to+50%25%29.+This+effect+was+observed+irrespective+of+the+type+of+local+treatment%2C+and+did+not+vary+between+subgroups+of+patients.jpg "Lancet 2003; 361: 1927–34.")
64
E U R O P E A N U R O L O G Y ( ) – 5 3 3
 – 5 3 3")
65
NEOADYUDANCIA A todos antes de la cirugía: menor riesgo de recurrencia y aumenta la sobrevida con respecto a la cirugía sola Pero el administrarlo no justifica que se retrase la cirugía Radical cystectomy and bladdersparing treatments for urothelial bladder cancer. UpToDate2015

66
CONCLUSIONES Las terapias conservadoras son una ALTERNATIVA a la cistectomía radical, aunque existan estudios con resultados similares en cuanto a OS y DSS, ya que muchos de ellos tienen sesgos. Considerar la terapia cnservadora en pacientes altamente seleccionados con facilidad en el seguimiento, lo cual es poco probable en nuestra población. Seguir de manera estricta los criterios de selección para la escogencia de los pacientes que se beneficien de este tipo de terapia. Ofrecer a todos los pacientes con enfermedad músculo-invasora la cistectomía radical coma el GOLD STANDARD.

Presentaciones similares










 O BEVACIZUMAB MAS MFOLFOX6, EN PACIENTES CON CANCER COLORRECTAL.>")



.>")




