Descargar la presentación
La descarga está en progreso. Por favor, espere

1
en la primera línea del cáncer renal avanzado
Pazopanib en la primera línea del cáncer renal avanzado Pazopanib en el tratamiento del Carcinoma de Células Renales Luis León Servicio de Oncología Médica Santiago de Compostela

2
Pazopanib bloquea moléculas clave implicadas en la angiogénesis
PDGFR VEGFR-1 VEGFR-2 VEGFR-3 c-KIT P P P P Tumour cell membrane P RAS PI3K FAK PLC Proliferation Survival Migration 1. Sonpavde et al. Expert Opin Investig Drugs 2008;17:253–61.

3
Inhibidor multikinasa
Pazopanib 32 Sunitinib 54 Sorafenib 25 Kinases inhibited with IC50 <1 μM 1. Kumar et al. Br J Cancer 2009;101:1717–23. Figure adapted from Karaman et al. Nat Biotechnol 2008;26:127–32.

4
Datos de Eficacia Nico Munuera

5
Phase II study: VEG Inclusion ECOG performance status 0 or 1 Treatment-naïve or one prior cytokine or bevacizumab failure Patients with advanced or metastatic RCC (N=225) Pazopanib 800 mg once daily for 12 weeks Complete/partial response Stable disease Progressive disease Randomization 30% pretratados, citoquinas solo 24%, Cit + QT < 1%; Cit + Avastin 2% Se modificó el estudio tras incluir 60 pts y observar un 38% respuestas Pazopanib 800 mg once daily (n=170) Pazopanib 800 mg once daily (n=27) Matching placebo (n=28) Patients received pazopanib after interim analysis Clinicaltrials.gov identifier NCT Hutson et al. J Clin Oncol 2010;28:475–80. US NIH. Available from: (last updated Jan 6, 2011)
 Pazopanib 800 mg once daily. for 12 weeks. Complete/partial. response. Stable disease. Progressive. disease. Randomization. 30% pretratados, citoquinas solo 24%, Cit + QT < 1%; Cit + Avastin 2% Se modificó el estudio tras incluir 60 pts y observar un 38% respuestas. Pazopanib 800 mg once daily (n=170) Pazopanib 800 mg once daily (n=27) Matching placebo (n=28) Patients received pazopanib after interim analysis. Clinicaltrials.gov identifier NCT Hutson et al. J Clin Oncol 2010;28:475–80. US NIH. Available from: term=pazopanib+renal&rank=2 (last updated Jan 6, 2011)")
6
Objetivos del estudio (revisados)1
Objetivo principal % de respuestas según RECIST (PFS antes de la modificación) Objetivos secundarios Duración de respuesta PFS durante la fase de aleatorización Seguridad y tolerabilidad Análisis global PFS Análisis global PFS: *Specified in analysis plan but not included in protocol Hutson et al. J Clin Oncol 2010;28:475–80.
 Objetivos secundarios. Duración de respuesta. PFS durante la fase de aleatorización. Seguridad y tolerabilidad. Análisis global PFS. Análisis global PFS: *Specified in analysis plan but not included in protocol. Hutson et al. J Clin Oncol 2010;28:475–80.")
7
Características de los pacientes
Characteristic Patients (N=225) Mean age, years (range) 59.8 (32–81) Gender, n (%) Female Male 69 (31) 156 (69) Prior nephrectomy, n (%) 205 (91) Prior radiotherapy, n (%) 43 (19) Prior systemic therapy, n (%) No prior systemic therapy Prior systemic therapy* 155 (69) 70 (31) MSKCC risk criteria, n (%)† Favourable Intermediate Poor Unknown 97 (43) 92 (41) 5 (2) 31 (14)‡ *Cytokine, chemotherapy, hormonal or bevacizumab-based regimens; †For 162 patients, calcium instead of corrected-calcium was used to derive their total MSKCC risk factor; ‡31 patients were missing data on ≥1 of the 5 risk factors and, thus, did not have sufficient data to be assigned to a risk category Hutson et al. J Clin Oncol 2010;28:475–80.
 Mean age, years (range) 59.8 (32–81) Gender, n (%) Female Male. 69 (31) 156 (69) Prior nephrectomy, n (%) 205 (91) Prior radiotherapy, n (%) 43 (19) Prior systemic therapy, n (%) No prior systemic therapy Prior systemic therapy* 155 (69) 70 (31) MSKCC risk criteria, n (%)† Favourable Intermediate Poor Unknown. 97 (43) 92 (41) 5 (2) 31 (14)‡ *Cytokine, chemotherapy, hormonal or bevacizumab-based regimens; †For 162 patients, calcium instead of corrected-calcium was used to derive their total MSKCC risk factor; ‡31 patients were missing data on ≥1 of the 5 risk factors and, thus, did not have sufficient data to be assigned to a risk category. Hutson et al. J Clin Oncol 2010;28:475–80.")
9
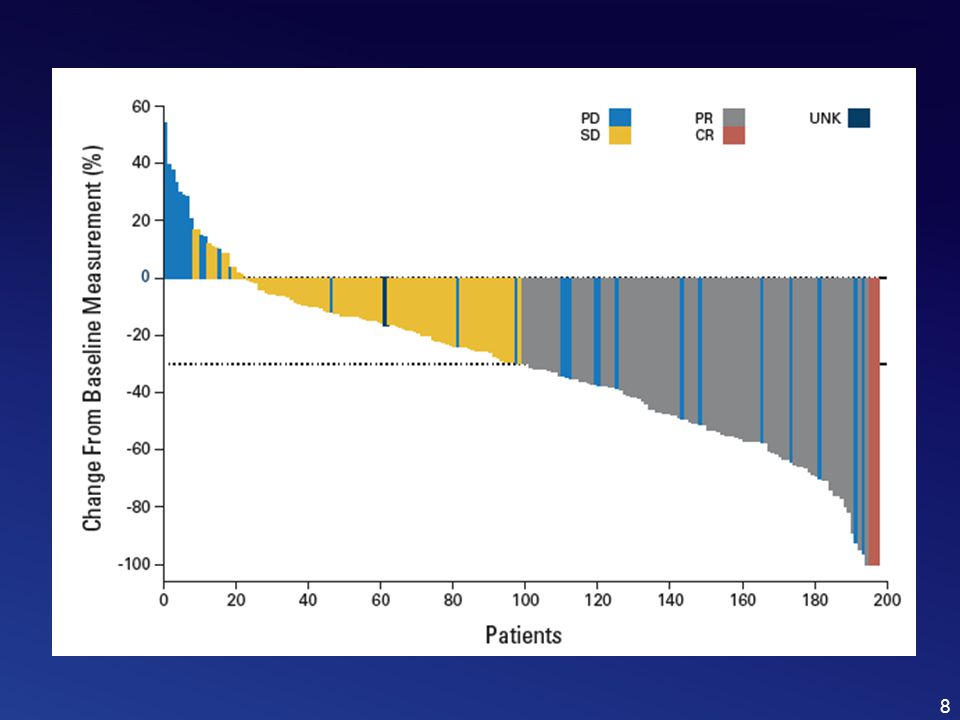
Tasa de respuesta global1
Hutson et al. J Clin Oncol 2010;28:475–80.

10
Pazopanib es superior a placebo en PFS1
1.0 Median: 51.7 weeks2 (95% CI: 43.9, 60.3) 0.8 Week 12 randomization point Log-rank, p= 6.2 months (4.6, 10.9) 0.6 11.9 months (10.0, –) Proportion progression-free 0.4 0.2 Pazopanib Placebo Importante, los datos de los ptes que pasaron a cross-over no fueron censurados, por lo que incluyeron en el análisis final 0.0 10 20 30 40 50 60 70 80 90 100 Weeks on study La comparación de PFS por un comité independiente demostró una ventaja a favor de pazopanib Los pacientes cruzados a pazopanib no se censuraron Hutson et al. J Clin Oncol 2010;28:475–80.
 0.8. Week 12 randomization point. Log-rank, p= months. (4.6, 10.9) months. (10.0, –) Proportion progression-free Pazopanib. Placebo. Importante, los datos de los ptes que pasaron a cross-over no fueron censurados, por lo que incluyeron en el análisis final Weeks on study. La comparación de PFS por un comité independiente demostró una ventaja a favor de pazopanib. Los pacientes cruzados a pazopanib no se censuraron. Hutson et al. J Clin Oncol 2010;28:475–80.")
11
Phase III study: VEG Patients with advanced/ metastatic RCC (N=435) Stratification ECOG performance status 0 versus 1 Prior nephrectomy Treatment-naïve (n=233) versus one cytokine failure (n=202) Randomization 2:1 Pazopanib 800 mg once daily (n=290) Matching placebo (n=145) Option to receive pazopanib via an open-label study at progression Clinicaltrials.gov identifier NCT VEG open-label study 71 patients enrolled* Sternberg et al. J Clin Oncol 2010;28: 11 11
 versus one cytokine failure (n=202) Randomization 2:1. Pazopanib 800 mg once daily (n=290) Matching placebo (n=145) Option to receive pazopanib via an open-label study at progression. Clinicaltrials.gov identifier NCT VEG open-label study. 71 patients enrolled* Sternberg et al. J Clin Oncol 2010;28:")
12
Objetivos secundarios
Objetivos del estudio1 Objetivo principal PFS Objetivos secundarios OS ORR Duración de respuesta Seguridad y tolerabilidad Análisis global PFS Otros: calidad de vida Sternberg et al. J Clin Oncol 2010;28:

13
Característica basales1
Characteristic Pazopanib (n=290) Placebo (n=145) Median age, year (range) 59 (28–85) 60 (25–81) Gender, % male 68 75 Most common metastatic sites, % Lung Lymph node Bone Liver 74 54 28 26 73 59 22 Number of organs involved, % 1 and 2 ≥3 45 55 48 52 ECOG performance status, % 1 42 58 41 MSKCC risk category, % Favourable Intermediate Poor Unknown* 3 39 53 3 4 *Missing results for one or more of the five risk criteria The study protocol was finalized in November 2005 to enrol patients with cytokine-pretreated RCC1 Sorafenib and sunitinib were subsequently approved for advanced RCC in December 2005 and January 2006, respectively Subsequently, the VEG study population was expanded to include patients with treatment-naïve, advanced RCC1 Placebo was retained as a comparator because: Sunitinib and sorafenib were not approved or not readily available in many of the participating study countries Using placebo in a randomized, double-blind design allowed better characterization of the safety and efficacy profiles of pazopanib Pazopanib was provided as a treatment option for patients who progressed on the placebo arm The ethical aspects for selecting a placebo control was carefully considered based on the guidelines from regulatory authorities and the ICH Sternberg et al. J Clin Oncol 2010;28:
 Placebo. (n=145) Median age, year (range) 59 (28–85) 60 (25–81) Gender, % male Most common metastatic sites, % Lung. Lymph node. Bone. Liver Number of organs involved, % 1 and 2. ≥ ECOG performance status, % MSKCC risk category, % Favourable. Intermediate. Poor. Unknown* *Missing results for one or more of the five risk criteria. The study protocol was finalized in November 2005 to enrol patients with cytokine-pretreated RCC1. Sorafenib and sunitinib were subsequently approved for advanced RCC in December 2005 and January 2006, respectively. Subsequently, the VEG study population was expanded to include patients with treatment-naïve, advanced RCC1. Placebo was retained as a comparator because: Sunitinib and sorafenib were not approved or not readily available in many of the participating study countries. Using placebo in a randomized, double-blind design allowed better characterization of the safety and efficacy profiles of pazopanib. Pazopanib was provided as a treatment option for patients who progressed on the placebo arm. The ethical aspects for selecting a placebo control was carefully considered based on the guidelines from regulatory authorities and the ICH. Sternberg et al. J Clin Oncol 2010;28:")
14
Porcentaje de respuestas
Pazopanib Placebo p<0.001 Sternberg et al. J Clin Oncol 2010;28:

15
Supervivencia libre de progresión en toda la población1
1.0 Median PFS (months) Placebo 4.2 Pazopanib 9.2 0.8 Hazard ratio (95% CI) 0.46 (0.34, 0.62) p value (1-sided) <0.0001 0.6 Proportion progression-free 0.4 0.2 Pazopanib Placebo 0.0 5 10 15 20 Number at risk, n Pazopanib Placebo Time (month) 290 145 159 38 76 14 29 2 6 In the overall study population, PFS was significantly greater in pazopanib- versus placebo-treated patients (p<0.0001) Sternberg et al. J Clin Oncol 2010;28:
 Placebo Pazopanib Hazard ratio (95% CI) 0.46 (0.34, 0.62) p value (1-sided) < Proportion progression-free Pazopanib. Placebo Number at risk, n. Pazopanib. Placebo. Time (month) In the overall study population, PFS was significantly greater in pazopanib- versus placebo-treated patients (p<0.0001) Sternberg et al. J Clin Oncol 2010;28:")
16
Supervivencia libre de progresión en los pacientes no pretratados1,2
1.0 Median PFS (months) Placebo 2.8 Pazopanib 11.1 0.8 Hazard ratio (95% CI) 0.40 (0.27, 0.60) p value (1-sided) <0.0001 0.6 Proportion progression-free 0.4 0.2 Pazopanib Placebo 0.0 5 10 15 20 Number at risk, n Pazopanib Placebo Time (month) 155 78 84 22 39 7 11 2 1 In the treatment-naïve subpopulation, PFS was significantly greater in pazopanib- versus placebo-treated patients (p<0.0001) Sternberg et al. J Clin Oncol 2010;28:
 Placebo Pazopanib Hazard ratio (95% CI) 0.40 (0.27, 0.60) p value (1-sided) < Proportion progression-free Pazopanib. Placebo Number at risk, n. Pazopanib. Placebo. Time (month) In the treatment-naïve subpopulation, PFS was significantly greater in pazopanib- versus placebo-treated patients (p<0.0001) Sternberg et al. J Clin Oncol 2010;28:")
17
Supervivencia libre de progresión en los pacientes tratados con citoquinas1,2
1.0 Placebo 4.2 Pazopanib 7.4 Hazard ratio (95% CI) 0.54 (0.35, 0.84) p value (1-sided) <0.001 Median PFS (months) 0.8 0.6 Proportion progression-free 0.4 0.2 Pazopanib Placebo 0.0 5 10 15 20 Number at risk, n Pazopanib Placebo Time (month) 135 67 75 16 37 7 18 5 In the cytokine-pretreated subpopulation, PFS was significantly greater in pazopanib- versus placebo-treated patients (p<0.001) Sternberg et al. J Clin Oncol 2010;28:
 0.54 (0.35, 0.84) p value (1-sided) < Median PFS (months) Proportion progression-free Pazopanib. Placebo Number at risk, n. Pazopanib. Placebo. Time (month) In the cytokine-pretreated subpopulation, PFS was significantly greater in pazopanib- versus placebo-treated patients (p<0.001) Sternberg et al. J Clin Oncol 2010;28:")
18
Beneficio en todos los subgrupos
Baseline factor Hazard ratio (95% CI) Primary analysis MSKCC risk: favourable MSKCC risk: intermediate Female Male Age <65 years Age ≥65 years ECOG performance status 0 ECOG performance status 1 0.2 0.4 0.6 0.8 1.0 1.2 p<0.001 by log-rank test for all Favours pazopanib Favours placebo PFS was significantly improved with pazopanib across all sub-groups: Age, gender, PS and MSKCC risk status Sternberg et al. J Clin Oncol 2010;28:
 Primary analysis. MSKCC risk: favourable. MSKCC risk: intermediate. Female. Male. Age <65 years. Age ≥65 years. ECOG performance status 0. ECOG performance status p<0.001 by log-rank test for all. Favours pazopanib. Favours placebo. PFS was significantly improved with pazopanib across all sub-groups: Age, gender, PS and MSKCC risk status. Sternberg et al. J Clin Oncol 2010;28:")
19
Objetivo principal: OS
1.0 Hazard ratio=0.91 95% CI (0.71–1.16) p=0.224 0.8 Median OS Pazopanib: 22.9 months Placebo: 20.5 months 0.6 Proportion surviving 0.4 Pazopanib Placebo 0.2 90% power to detect 50% improvement in the overall study population Final OS analysis performed when 290 deaths were accrued OS is confounded by: Open-label crossover study (n=80) running in parallel with the randomized Phase III study Early and frequent crossover of placebo patients to pazopanib Crossover occurred as early as 6 weeks 54% of placebo patients crossed Prolonged pazopanib treatment following crossover 54% of placebo patients crossed over Time of crossover 0.0 10 20 30 40 Time (months) Patients at risk Pazopanib Placebo 290 145 213 93 147 71 95 53 25 9 Sternberg et al. Annals Oncol 2010; 21(Suppl 8): Abstract LBA22 and oral presentation
 p= Median OS. Pazopanib: 22.9 months. Placebo: 20.5 months Proportion surviving Pazopanib. Placebo % power to detect 50% improvement in the overall study population. Final OS analysis performed when 290 deaths were accrued. OS is confounded by: Open-label crossover study (n=80) running in parallel with the randomized Phase III study. Early and frequent crossover of placebo patients to pazopanib. Crossover occurred as early as 6 weeks. 54% of placebo patients crossed. Prolonged pazopanib treatment following crossover. 54% of placebo patients crossed over. Time of crossover Time (months) Patients at risk. Pazopanib. Placebo Sternberg et al. Annals Oncol 2010; 21(Suppl 8): Abstract LBA22 and oral presentation.")
20
Toxicidad

21
Efectos de clase en ensayo fase III (VEG105192)1
Pazopanib (n=290) Placebo (n=145) Adverse event All grades, % Proteinuria 9 Hypothyroidism 7 (3)2 Hand–foot syndrome 6 <1 Mucositis/stomatitis 4/4 <1/0 Arterial thromboembolic 3* *2% of arterial thromboembolic events were Grade 3 or worse in severity En revisión de fase II y III por Wolter la incidencia de hipotiroidismo fue del 3% Sternberg et al. J Clin Oncol 2010;28: ; 2. Wolter ASCO 2011
 Placebo. (n=145) Adverse event. All grades, % Proteinuria. 9. Hypothyroidism. 7 (3)2. Hand–foot syndrome. 6. <1. Mucositis/stomatitis. 4/4. <1/0. Arterial thromboembolic. 3* *2% of arterial thromboembolic events were Grade 3 or worse in severity. En revisión de fase II y III por Wolter la incidencia de hipotiroidismo fue del 3% Sternberg et al. J Clin Oncol 2010;28: ; 2. Wolter ASCO")
23
Efectos adversos de Pazopanib en ensayos fase II y III
*presentes en ≥10% of pacientes Adverse event VEG VEG Pazopanib (n=225), % Pazopanib (n=290), % Placebo (n=145), % All grade Grade 3 Grade 4 All grade All grade* Diarrhoea 63 4 52 3 <1 9 Hypertension 41 40 10 Hair colour changes 43 38 Nausea 42 26 Anorexia 24 22 2 Vomiting 20 21 8 Fatigue 46 5 19 1 Asthenia – 14 Abdominal pain 16 11 Headache *In study VEG105192, 4 and 3% of patients in the pazopanib and placebo arms, respectively, had Grade 5 adverse events Ver bien el estudio porque cifras no coincide con la de la diapo que viene en 2 más Hutson et al. J Clin Oncol 2010;28:475–80. . Sternberg et al. J Clin Oncol 2010;28:
, % Pazopanib (n=290), % Placebo (n=145), % All grade. Grade 3. Grade 4. All. grade. All grade* Diarrhoea <1. 9. Hypertension Hair colour changes Nausea Anorexia Vomiting Fatigue Asthenia. – 14. Abdominal pain Headache. *In study VEG105192, 4 and 3% of patients in the pazopanib and placebo arms, respectively, had Grade 5 adverse events. Ver bien el estudio porque cifras no coincide con la de la diapo que viene en 2 más. Hutson et al. J Clin Oncol 2010;28:475–80. . Sternberg et al. J Clin Oncol 2010;28:")
24
Pazopanib: elevación de transaminasas y Br
Proportion of subjects, % Pazopanib (n=290) Placebo (n=145) All grades Grade 3 Grade 4 ALT increase 53 10 2 22 1 AST increase 7 <1 19 Br increase 36 3 Alkaline phosphatase 27 35 Liver enzyme elevations were largely reversible following dose modification, interruption or cessation1 Many subjects were able to continue on pazopanib and adapted Fatal hepatic events were reviewed across the entire safety database (N=1830) Out of 1830 subjects there were two fatal cases, which were possibly attributable to pazopanib. This is equivalent to 0.1% (95% CI: 0.03, 0.4)1 4595 General Poster Session (Board #4C), Sun, 8:00 AM-12:00 PM Risk of high-grade liver toxicity with pazopanib in patients with cancer: A meta-analysis. S. Kapadia, S. Hapani, S. Wu; SUNY Stony Brook University Medical Center, Stony Brook, NY; Division of Hematology and Medical Oncology, Department of Medicine, Stony Brook University Medical Center, Stony Brook, NY; Stony Brook University Medical Center, Stony Brook, NY Background: Pazopanib, as an oral receptor tyrosine kinase inhibitor, has been approved for the treatment of advanced renal cell cancer (RCC) and undergoing evaluation in other tumors. Hepatotoxicity is a concern for clinical application. This study was conducted to determine the risk of high-grade liver toxicity with pazopanib by a systematic review and meta-analysis of clinical trials. Methods: Databases from PubMed, Web of Science and abstracts presented at ASCO meetings up to December 2010 were searched to identify relevant studies. Eligible studies included prospective clinical trials in which pazopanib was started at 800 mg daily as a monotherapy. Summary incidence rates, relative risks, and 95% confidence intervals (CIs) were calculated using a fixed-effects or random-effects model, depending on the heterogeneity of the included studies. Results: A total of 1,155 patients with a variety of solid tumors from eight clinical trials were included for the analysis. The incidence of all-grade ALT elevation was 41.7% (95% CI: %), with 8.2% (95% CI: %) being high-grade. Interestingly, there was a significant difference in the incidence of high-grade ALT elevation between RCC and non-RCC patients (10.9% vs 5.7%, p0.012). The incidence of all-grade AST elevation was 39.3% (95% CI %), with 6.4% (95% CI: %) being high-grade. There was no significant difference in the incidence of high-grade AST elevation between RCC and non-RCC patients (7.4% vs 4.8%, p0.22). In comparison with controls, pazopanib significantly increased the risk of high-grade ALT elevation (RR,7.95;95% CI: , p0.001) and high-grade AST elevation (RR 9.01, 95% CI: , p0.01). Conclusions: Pazopanib is associated with substantial risk of high-grade hepatotoxicity, which may vary with tumor types. Close monitoring and appropriate management are recommended during the therapy. Insuficiencia hepática No se ha establecido completamente la seguridad y la farmacocinética de pazopanib en pacientes con insuficiencia hepática (ver sección 4.4). Las recomendaciones posológicas en pacientes con insuficiencia hepática están basadas en los estudios farmacocinéticos de pazopanib en pacientes con diferentes grados de disfunción hepática (ver sección 5.2). La administración de pazopanib en pacientes con insuficiencia hepática leve o moderada debe realizarse con precaución y estrecha vigilancia debido al posible aumento de la exposición al medicamento. Se recomienda que los pacientes con alteraciones leves de los parámetros hepáticos (definidas como valores normales de bilirrubina y cualquier grado de elevación de alanina aminotransferasa (ALT) o como una elevación de los valores de bilirrubina (> 35 % bilirrubina directa) de hasta 1,5 veces el límite superior de la normalidad (LSN) independientemente de los valores de ALT) sean tratados inicialmente con 800 mg de pazopanib una vez al día. Se recomienda una dosis reducida de pazopanib de 200 mg una vez al día en pacientes con insuficiencia hepática moderada (definida como elevación de los valores de bilirrubina de > 1,5 a 3 veces el LSN independientemente de los valores de ALT) En ensayos clínicos con pazopanib, se observó un incremento de las transaminasas séricas (ALT, AST) y de la bilirrubina (ver sección 4.8). Se han notificado incrementos aislados de ALT y AST, que en la mayoría de los casos, no presentaron elevaciones concomitantes de fosfatasa alcalina o bilirrubina. Se deben monitorizar las pruebas hepáticas en suero antes de iniciar el tratamiento con pazopanib y al menos una vez cada 4 semanas durante los 4 primeros meses de tratamiento, y según esté clínicamente indicado. Después de este período deben continuar con una monitorización periódica. • Los pacientes con elevaciones aisladas de transaminasas ≤ 8 X límite superior de la normalidad (LSN) pueden continuar el tratamiento con pazopanib con una monitorización semanal de la función hepática hasta que las transaminasas vuelvan al Grado 1 o a la situación inicial. • Los pacientes con las transaminasas > 8 X LSN deben interrumpir el tratamiento con pazopanib hasta que vuelvan al Grado 1 o a la situación inicial. Si el beneficio potencial de reiniciar el tratamiento con pazopanib se considera mayor que el riesgo de hepatotoxicidad, se debe reiniciar el tratamiento con pazopanib con una dosis reducida y revisar los análisis del suero hepático semanalmente durante 8 semanas (ver sección 4.2). Si después de reiniciar el tratamiento con pazopanib se repiten las elevaciones de transaminas > 3 X LSN, se debe interrumpir el tratamiento con pazopanib. • Si se producen simultáneamente elevaciones de las transaminasas > 3 X LSN con elevaciones de bilirrubina > 2 X LSN, se debe realizar un fraccionamiento de la bilirrubina. Si la bilirrubina directa (conjugada) es > 35 % de la bilirrubina total, se debe interrumpir el tratamiento con pazopanib. US FDA. Available from: Kapadia, ASCO 2011.
 Placebo. (n=145) All grades. Grade 3. Grade 4. ALT increase AST increase. 7. < Br increase Alkaline phosphatase Liver enzyme elevations were largely reversible following dose modification, interruption or cessation1. Many subjects were able to continue on pazopanib and adapted. Fatal hepatic events were reviewed across the entire safety database (N=1830) Out of 1830 subjects there were two fatal cases, which were possibly attributable to pazopanib. This is equivalent to 0.1% (95% CI: 0.03, 0.4) General Poster Session (Board #4C), Sun, 8:00 AM-12:00 PM. Risk of high-grade liver toxicity with pazopanib in patients with cancer: A. meta-analysis. S. Kapadia, S. Hapani, S. Wu; SUNY Stony Brook University Medical Center, Stony Brook, NY; Division. of Hematology and Medical Oncology, Department of Medicine, Stony Brook University Medical Center, Stony Brook, NY; Stony Brook University Medical Center, Stony Brook, NY. Background: Pazopanib, as an oral receptor tyrosine kinase inhibitor, has been approved for the treatment. of advanced renal cell cancer (RCC) and undergoing evaluation in other tumors. Hepatotoxicity is a concern. for clinical application. This study was conducted to determine the risk of high-grade liver toxicity with. pazopanib by a systematic review and meta-analysis of clinical trials. Methods: Databases from PubMed, Web of Science and abstracts presented at ASCO meetings up to December 2010 were searched to identify. relevant studies. Eligible studies included prospective clinical trials in which pazopanib was started at 800. mg daily as a monotherapy. Summary incidence rates, relative risks, and 95% confidence intervals (CIs) were calculated using a fixed-effects or random-effects model, depending on the heterogeneity of the. included studies. Results: A total of 1,155 patients with a variety of solid tumors from eight clinical trials. were included for the analysis. The incidence of all-grade ALT elevation was 41.7% (95% CI: %), with 8.2% (95% CI: %) being high-grade. Interestingly, there was a significant difference in the. incidence of high-grade ALT elevation between RCC and non-RCC patients (10.9% vs 5.7%, p0.012). The incidence of all-grade AST elevation was 39.3% (95% CI %), with 6.4% (95% CI: %) being high-grade. There was no significant difference in the incidence of high-grade AST elevation between. RCC and non-RCC patients (7.4% vs 4.8%, p0.22). In comparison with controls, pazopanib significantly. increased the risk of high-grade ALT elevation (RR,7.95;95% CI: , p0.001) and high-grade. AST elevation (RR 9.01, 95% CI: , p0.01). Conclusions: Pazopanib is associated with. substantial risk of high-grade hepatotoxicity, which may vary with tumor types. Close monitoring and. appropriate management are recommended during the therapy. Insuficiencia hepática. No se ha establecido completamente la seguridad y la farmacocinética de pazopanib en pacientes con. insuficiencia hepática (ver sección 4.4). Las recomendaciones posológicas en pacientes con. insuficiencia hepática están basadas en los estudios farmacocinéticos de pazopanib en pacientes con. diferentes grados de disfunción hepática (ver sección 5.2). La administración de pazopanib en. pacientes con insuficiencia hepática leve o moderada debe realizarse con precaución y estrecha. vigilancia debido al posible aumento de la exposición al medicamento. Se recomienda que los. pacientes con alteraciones leves de los parámetros hepáticos (definidas como valores normales de. bilirrubina y cualquier grado de elevación de alanina aminotransferasa (ALT) o como una elevación de. los valores de bilirrubina (> 35 % bilirrubina directa) de hasta 1,5 veces el límite superior de la. normalidad (LSN) independientemente de los valores de ALT) sean tratados inicialmente con 800 mg. de pazopanib una vez al día. Se recomienda una dosis reducida de pazopanib de 200 mg una vez al día. en pacientes con insuficiencia hepática moderada (definida como elevación de los valores de. bilirrubina de > 1,5 a 3 veces el LSN independientemente de los valores de ALT) En ensayos clínicos con pazopanib, se observó un incremento de las transaminasas séricas (ALT, AST) y de la bilirrubina (ver sección 4.8). Se han notificado incrementos aislados de ALT y AST, que. en la mayoría de los casos, no presentaron elevaciones concomitantes de fosfatasa alcalina o. bilirrubina. Se deben monitorizar las pruebas hepáticas en suero antes de iniciar el tratamiento con pazopanib y al. menos una vez cada 4 semanas durante los 4 primeros meses de tratamiento, y según esté clínicamente. indicado. Después de este período deben continuar con una monitorización periódica. • Los pacientes con elevaciones aisladas de transaminasas ≤ 8 X límite superior de la. normalidad (LSN) pueden continuar el tratamiento con pazopanib con una monitorización. semanal de la función hepática hasta que las transaminasas vuelvan al Grado 1 o a la situación. inicial. • Los pacientes con las transaminasas > 8 X LSN deben interrumpir el tratamiento con. pazopanib hasta que vuelvan al Grado 1 o a la situación inicial. Si el beneficio potencial de. reiniciar el tratamiento con pazopanib se considera mayor que el riesgo de hepatotoxicidad, se. debe reiniciar el tratamiento con pazopanib con una dosis reducida y revisar los análisis del. suero hepático semanalmente durante 8 semanas (ver sección 4.2). Si después de reiniciar el. tratamiento con pazopanib se repiten las elevaciones de transaminas > 3 X LSN, se debe. interrumpir el tratamiento con pazopanib. • Si se producen simultáneamente elevaciones de las transaminasas > 3 X LSN con elevaciones. de bilirrubina > 2 X LSN, se debe realizar un fraccionamiento de la bilirrubina. Si la. bilirrubina directa (conjugada) es > 35 % de la bilirrubina total, se debe interrumpir el. tratamiento con pazopanib. US FDA. Available from: Kapadia, ASCO")
25
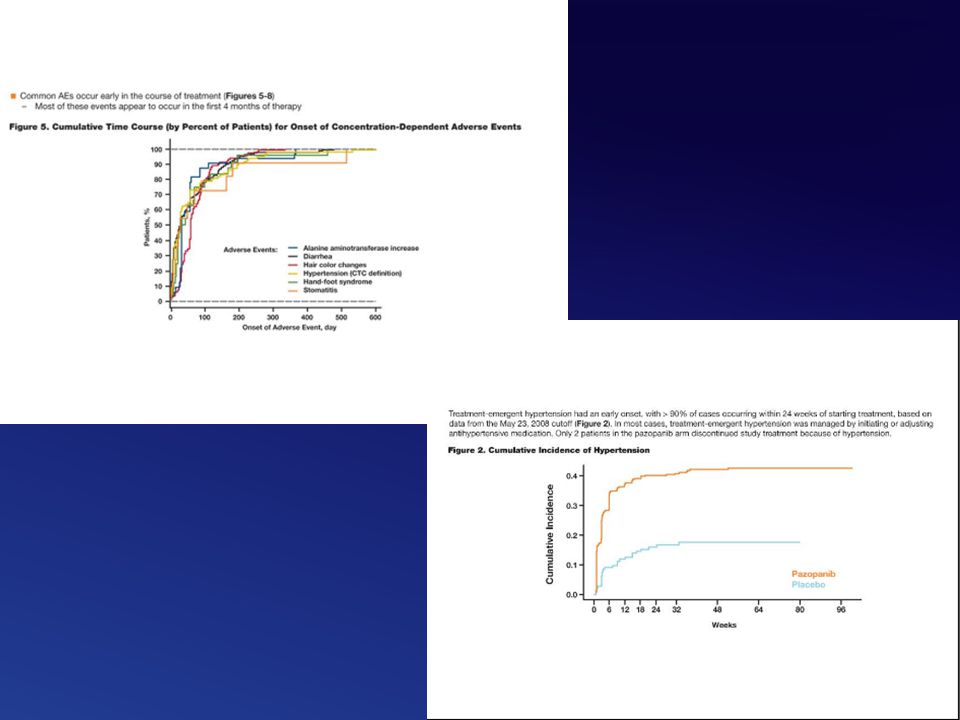
La elevación de ALT asociada a Pazopanib se produce de forma temprana1
0.16 0.14 0.12 0.10 Cumulative incidence 0.08 0.06 0.04 ALT >5X ULN (N=586) 0.02 0.0 6 12 24 32 48 64 80 96 112 Weeks Elevations in ALT levels were detected in the first 18 weeks of pazopanib treatment in the vast majority of subjects who developed such abnormalities US FDA. Available from:
 Weeks. Elevations in ALT levels were detected in the first 18 weeks of pazopanib treatment in the vast majority of subjects who developed such abnormalities. US FDA. Available from:")
26
Modificación o retraso de dosis debidos a efectos secundarios
VEG VEG ,3 Treatment modification Pazopanib (n=225) Pazopanib (n=290) Placebo (n=145) Dose reduction due to adverse events, % 31* 243 33 Treatment discontinuation due to adverse events, % 15 14† 3† *Subsequent re-escalations in approximately 50% of patients who reduced their dose of pazopanib; †Not including three patients who, in addition to adverse events, had concurrent other reasons at the time they discontinued participation in the study Hutson et al. J Clin Oncol 2010;28:475–80. Sternberg et al. J Clin Oncol 2010;28: GlaxoSmithKline. Data on file.
 Pazopanib (n=290) Placebo (n=145) Dose reduction due to adverse events, % 31* Treatment discontinuation due to adverse events, % † 3† *Subsequent re-escalations in approximately 50% of patients who reduced their dose of pazopanib; †Not including three patients who, in addition to adverse events, had concurrent other reasons at the time they discontinued participation in the study. Hutson et al. J Clin Oncol 2010;28:475–80. Sternberg et al. J Clin Oncol 2010;28: GlaxoSmithKline. Data on file.")
27
Comparison of 20% QoL Deterioration Rates for Pazopanib-Treated and Placebo Patients, EORTC QLQ-C30
All Patients Treatment-Naive Patients 100 100 Pazopanib Placebo Pazopanib Placebo 90 90 80 80 70 70 60 60 Event Rates (%) 50 Event Rates (%) 50 40 40 30 30 20 20 10 10 56 112 168 224 280 336 392 448 504 56 112 168 224 280 336 392 448 504 Number of Days Until Event Number of Days Until Event Cytokine-Pretreated Patients 100 Pazopanib Placebo 90 80 70 60 Event Rates (%) 50 40 30 20 10 56 112 168 224 280 336 392 Number of Days Until Event ASCO Annual Meeting; June 3-7, 2011; Chicago, IL.
 50. Event Rates (%) Number of Days Until Event. Number of Days Until Event. Cytokine-Pretreated Patients Pazopanib. Placebo Event Rates (%) Number of Days Until Event. ASCO Annual Meeting; June 3-7, 2011; Chicago, IL.")
28
HRQoL Deterioration ASCO Annual Meeting; June 3-7, 2011; Chicago, IL.
EORTC QLQ-C30 Global Health Status/QOL Scale EQ-5D Utility Index 1.0 1.0 0.9 0.9 0.8 0.8 0.7 0.7 Cumulative Distribution Function 0.6 Cumulative Distribution Function 0.6 0.5 0.5 0.4 Pazopanib Placebo 0.4 Pazopanib Placebo 0.3 0.3 0.2 0.2 0.1 0.1 10 20 30 40 50 60 70 80 90 100 10 20 30 40 50 60 70 80 90 100 HRQoL Deterioration From Baseline HRQoL Deterioration From Baseline EQ-5D VAS Score 1.0 0.9 0.8 0.7 For the EORTC QLQ-C30 global health status/QoL scale, cumulative distribution functions of HRQoL deterioration since baseline for pazopanib-treated and placebo patients intersect at 8%, 20%, and 33%, and coincide after 55%. These points of intersection indicate that the same proportion of pazopanib and placebo patients experienced HRQoL deterioration of these amounts; this suggests using 10%, 20%, and 30% as cutoff points for the time to deterioration analyses. Similar distributions observed for EQ-5D index and EQ-5D VAS Cumulative Distribution Function 0.6 0.5 0.4 Pazopanib Placebo 0.3 0.2 0.1 10 20 30 40 50 60 70 80 90 100 HRQoL Deterioration From Baseline ASCO Annual Meeting; June 3-7, 2011; Chicago, IL.

29
(A) IL8 2767AT (rs1126647) (A) IL8 2767AT (rs1126647); (B) IL8 251TA
(rs4073); (C) HIF1A 1790GA (rs ). (C) HIF1A 1790GA (rs ) (B) IL8 251TA (rs4073) Se identifican 8 polimorfismos en genes relacionados con el metabolismo de Pazopanib, o con angiogénesis (IL-8) y HIF. No son marcadores pronósticos (no relacion con PFS ni RR en placebo). Si se validan se podría seleccionar tto en función de su presencia(p.e si están presentes no usar pazo y si otro farmaco).
; (C) HIF1A 1790GA (rs ). (C) HIF1A 1790GA (rs ) (B) IL8 251TA. (rs4073) Se identifican 8 polimorfismos en genes relacionados con el metabolismo de Pazopanib, o con angiogénesis (IL-8) y HIF. No son marcadores pronósticos (no relacion con PFS ni RR en placebo). Si se validan se podría seleccionar tto en función de su presencia(p.e si están presentes no usar pazo y si otro farmaco).")
30
CONCLUSIONES Pazopanib es superior a placebo (PFS) en primera línea de cáncer renal metastásico Pazopanib obtiene un porcentaje de respuestas del 30% en esta población La tolerancia a pazopanib es buena, y las toxicidades manejables Debe prestarse especial atención a las alteraciones en la función hepática Pazopanib no produce un deterioro en la calidad de vida Necesitamos marcadores predictivos de respuesta

31
¿Cuál es el camino?

32
Gracias

Presentaciones similares









>")




 O BEVACIZUMAB MAS MFOLFOX6, EN PACIENTES CON CANCER COLORRECTAL.>")




