Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Staphylococcus aureus Meticilino resistente (MRSA)
Dr. Elio Ochoa Maldonado Infectólogo Plan de seguridad del paciente Programa de prevencion de infecciones Hospital del IESS Guayaquil

2
50 años masculino, hernia discal- IQ, cultivo muestra transoperatorio:
SAMR

3
42 años masculino, Trauma Fx tibia – clavo endomedular - IQ, cultivo muestra transoperatorio:
SAMR

4
35 años masculino, Politraumatismo, SDRA, larga internacion, ARM, cultivo : SAMR

5
Staphylococcus aureus Meticilino resistente
Primer reporte en 1961 en el Reino Unido En 1963 se reporta el primer brote en USA A partir de 1990 se reporta en la comunidad Cepas comunitarias diferententes a las hospitalarias En USA: USA300, 400 Europa: productoras de leucocidinas Ecuador: PVL

6
Staphylococcus aureus Meticilino resistente
Mutaciones cromosomicas gen mecA Suelen presentar otras mutaciones que confieren resistencia a varios antibiot Alteracion de las PBP, ( sitio diana) Fatores de virulencia Adhesion a fibrinogeno, cell Evasion del sistema inmune Adhesion alfa toxin, beta gamma delta hemolisinas
 Fatores de virulencia. Adhesion a fibrinogeno, cell. Evasion del sistema inmune. Adhesion alfa toxin, beta gamma delta hemolisinas.")
7
Staphylococcus aureus Meticilino resistente
COMUNITARIAS HOSPITALARIAS

8
Most Invasive MRSA Infections Are Healthcare-Associated
14% 86% Community-Associated Healthcare-Associated Klevens et al JAMA 2007;298:

10
MRSA Strain Characteristics Were Initially Distinct
MRSA in Healthcare MRSA in the Community Prevalent genotypes (U.S.) USA100, USA200 USA300, USA400 Antimicrobial resistance Multiple agents Few agents SCCmec (genetic element carrying mecA resistance gene) Types I-III Types IV, V PVL toxin gene Rare Common These community strains do not appear to have been transferred from the hospitals. Patients with MRSA acquired in the community usually have no previous contact with healthcare centers clinical manifestations are also different, Community strains cause mostly skin and soft tissue infections, but rarely cause upper respiratory or urinary tract infections, which are common with healthcare strains The community strains are only resistant to beta-lactams and sometimes other antimicrobial group, in contrast to the multi-resistant pattern of the healthcare strains This different antimicrobial susceptibility is explained by a distinct genetic background and, although still in debate, the difference in clinical manifestations may be due to the presence in community strains of toxins such as PVL or Panton Vanlentine Leukocidine, that causes severe inflammation
 USA100, USA200. USA300, USA400. Antimicrobial resistance. Multiple agents. Few agents. SCCmec (genetic element carrying mecA resistance gene) Types I-III. Types IV, V. PVL toxin gene. Rare. Common. These community strains do not appear to have been transferred from the hospitals. Patients with MRSA acquired in the community usually have no previous contact with healthcare centers. clinical manifestations are also different, Community strains cause mostly skin and soft tissue infections, but rarely cause upper respiratory or urinary tract infections, which are common with healthcare strains. The community strains are only resistant to beta-lactams and sometimes other antimicrobial group, in contrast to the multi-resistant pattern of the healthcare strains. This different antimicrobial susceptibility is explained by a distinct genetic background. and, although still in debate, the difference in clinical manifestations may be due to the presence in community strains of toxins such as PVL or Panton Vanlentine Leukocidine, that causes severe inflammation.")
11
MRSA Was the Most Commonly Identified Cause of Purulent SSTIs Among Adult ED Patients (EMERGEncy ID Net), August 2004 59% (97% USA300) 54% 39% 15% 55% 74% 51% 68% 60% 60% 72% 67% Moran et al NEJM 2006;355:
 54% 39% 15% 55% 74% 51% 68% 60% 60% 72% 67% Moran et al NEJM 2006;355:")
12
COMUNITARIA

13
Staphylococcus aureus Estrategias de control

14
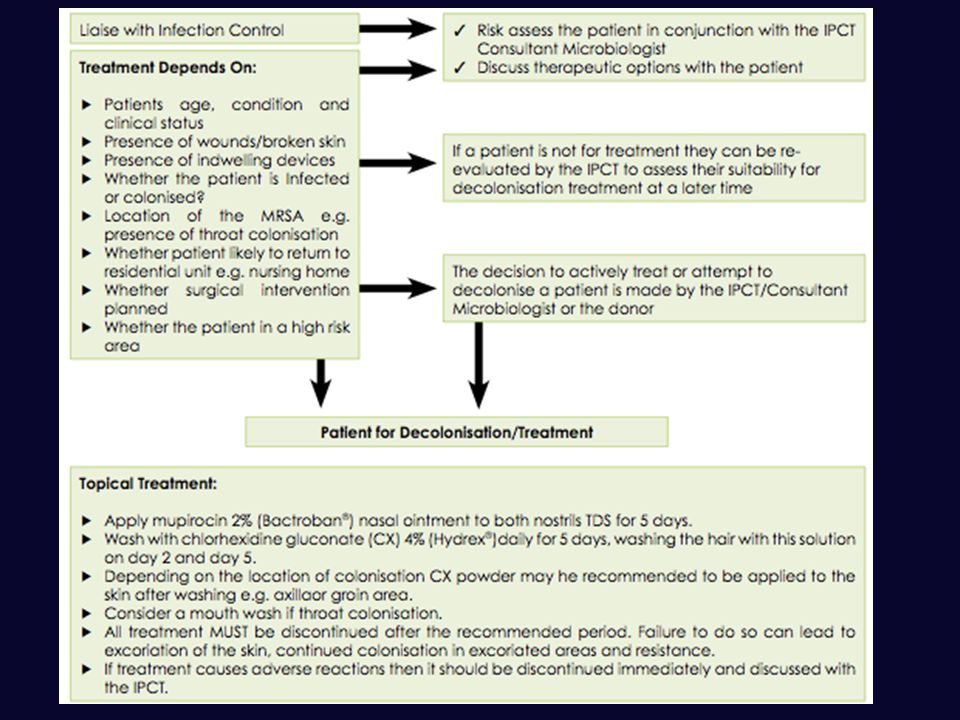
Guia IRLANDA 20013

16
TRATAMIENTO

17
Neumonía: Linezolide, Vancomicina, Clindamicina Bacteremia: Vancomicina, Daptomicina Partes blandas: complicada: Vanco, linezolide, dapto, clinda.

18
Partes blandas: NO complicada: TMS, clinda, Doxiciclina, Minociclina, SNC: Vanco, Line, TMS Osteomielitis: Vanco, Line, TMS, Rifa, Mino, Doxi

19
TRATAMIENTO BACTEREMIA

20
TRATAMIENTO BACTEREMIA

21
Clinical Considerations - Evaluation
MRSA belongs in the differential diagnosis of skin and soft tissue infections (SSTI’s) compatible with S. aureus infection: Abscesses, pustular lesions, “boils” “Spider bites” Cellulitis?
 compatible with S. aureus infection: Abscesses, pustular lesions, boils Spider bites Cellulitis")
22
Clinical Considerations - Evaluation
MRSA should also be considered in differential diagnosis of severe disease compatible with S. aureus infection: Osteomyelitis Empyema Necrotizing pneumonia Septic arthritis Endocarditis Sepsis syndrome Necrotizing fasciitis Purpura fulminans

23
MONITOREAR NIVEL SERICO OTROS ANTIMICROBIANOS
NEFROTOXICIDAD MONITOREAR NIVEL SERICO OTROS ANTIMICROBIANOS LINEZOLIDE DAPTO QUINU/DALFO

24
COLONIZACION

25
S. aureus Nasal Colonization National Health and Nutrition Examination Survey 2001-02
S. aureus: 32.4% = 89.4 M people MRSA: 0.8% = 2.3 M people MRSA colonization associated with age >= 60 years & being female

26
Staphylococcus aureus

27
PORTACION TRABAJADOR SALUD

28
AISLAMIENTO DE CONTACTO

29
Staphylococcus aureus Prevencion de Infecciones
Precauciones de contacto Higiene de manos Baño corporal con clorhexidina Higiene bucal Descolonizacion Monitoreo de personal de salud Limpieza ambiental Gestion de antimicrobianos (Stewardship)
")
30
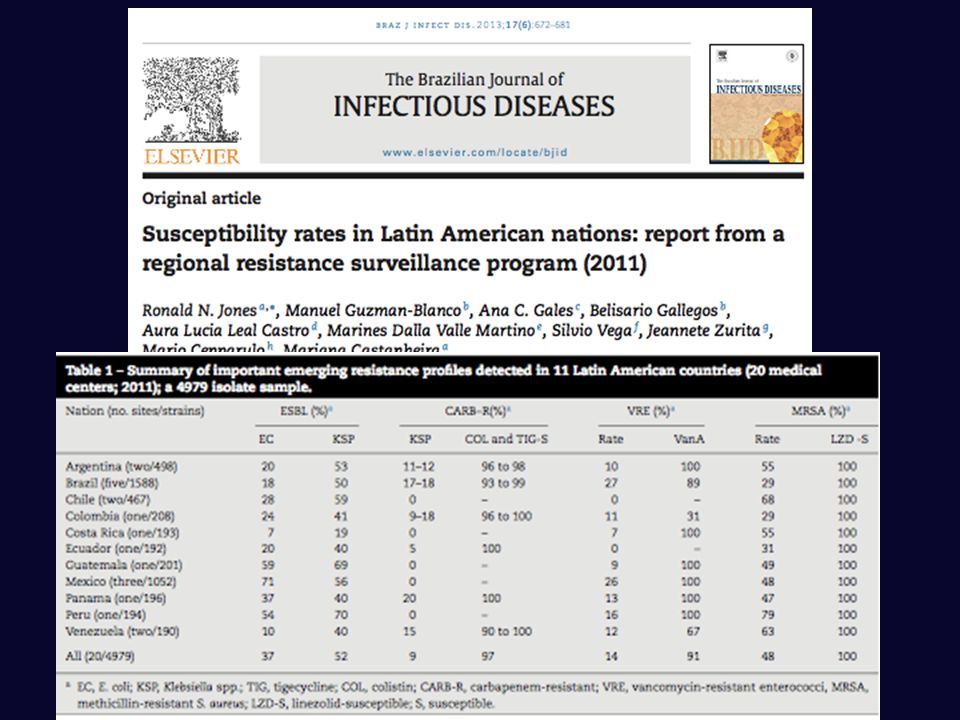
SAMR PROGRAMA DE VIGILANCIA ACTIVA

31
DEBEMOS DESCOLONIZAR LOS TRABAJADORES DE SALUD Y PACIENTES COLONIZADOS
?
33
GRACIAS

Presentaciones similares