Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Propiedad intelectual y derechos de autor El material didáctico de este sitio es ofrecido gratuitamente y forma parte de los temas preparados por los Doctores Ernesto Gil Deza y Felipe Gustavo Gercovich del Instituto Oncológico Henry Moore para la Maestría en Educación Médica de la Facultad de Medicina de Tucumán. El mismo puede ser empleado libremente citando las fuentes correspondientes, pero no puede utilizarse con fines comerciales. En el caso de realizar alguna publicación empleando este material solicitar autorización previa a los autores. Si realiza modificaciones le rogamos que nos la haga llegar, pues de esta manera se logrará un perfeccionamiento del material didáctico que deseamos difundir libremente. Las opiniones reflejadas en este material son de exclusiva responsabilidad de los autores y no reflejan la opinión de las instituciones. Por favor háganos saber su crítica, es la única manera que conocemos para mejorar y superarnos. Gracias. Prof. Ernesto Gil Deza Prof. Felipe Gustavo Gercovich

2
Taller de bioética Maestría médica Facultad de Medicina Universidad Nacional de Tucumán Ernesto Gil Deza Felipe Gustavo Gercovich

3
Objetivo del taller “… the goal of teaching ethics to health care practitioners is not only to convey information about available moral theories but also to cultivate moral sensitivity in practical situations …” Suzanne M. Jaeger PhD Teaching health care ethics: the importance of moral sensitivity for moral reasoning Nursing Philosophy Volume 2 Issue 2 Page 131 - July 2001

4
Condiciones Libertad Participación Comunicación Respeto Honestidad

5
Por eso predicamos con el ejemplo Libre consentimiento de participación

6
Seguimos con el conocimiento mutuo Lea cuidadosamente el instructivo y llene la siguiente ficha.

7
Mientras tanto me presento yo… 43 años (04 de Agosto de 1959) Casado 3 hijos Cátedra de Oncología en Postgrado USAL Recibido en 1984 (Fac. Medicina UNT) Promedio general de la carrera: 9.72 Idioma inglés: nivel b (lee y escribe) Bioética: nivel b (análisis de casos )
 Promedio general de la carrera: 9.72 Idioma inglés: nivel b (lee y escribe) Bioética: nivel b (análisis de casos ).")
8
Bioética Aspectos generales e investigaciones con seres humanos Cuidado del paciente muriente Cuidado del paciente muriente Etica de la prescripción médica Etica de la prescripción médica

9
http//cme.nci.nih.gov/

17
Taller de bioética Costumbre Religión Moral Ética Ley Norma Guía

18
Taller de bioética Costumbre – Modo/moda - Hábito Religión: preformal – formal – institucional - informal Moral Etica Ley Norma Guía

19
Taller de bioética Costumbre Religión Moral (arte) y práctica de las buenas costumbres – seculares o religiosas Etica (ciencia) y teoría de los fundamentos y razones de las conductas deseables Ley: Norma Guía
 y práctica de las buenas costumbres – seculares o religiosas Etica (ciencia) y teoría de los fundamentos y razones de las conductas deseables Ley: Norma Guía")
20
Taller de bioética Costumbre Religión Moral Etica Ley: mínimo de moral exigible Norma: conducta impuesta Guía: conducta sugerida

21
Filosofía moral vs. ética El objeto de la filosofía moral son las actividades humanas orientadas a un fin, teniendo en cuenta que el hombre actúe en forma voluntaria y libre. Hombre: Inteligencia (abstracta) y Voluntad (libre) libre –Coerciones –Coacciones
 y Voluntad (libre) libre –Coerciones –Coacciones.")
22
La ética: descriptiva, analítica y de la ciencia, procura emplear el método científico y los conocimientos científicos del individuo y la sociedad para definir una conducta deseable. P (x,x ’ /RUCD) Mario Bunge Etica, Ciencia y Técnica Filosofía moral vs. ética
 Mario Bunge Etica, Ciencia y Técnica Filosofía moral vs. ética.")
23
Etica médica Hipócrates Platón Tomás de Aquino Descartes Kant Freud Beauchamp Secular Utilitarista Virtuosa (Benef) Respetuosa (Aut.) Equitativa (Just) Abierta Transdisciplinaria
 Respetuosa (Aut.) Equitativa (Just) Abierta Transdisciplinaria")
24
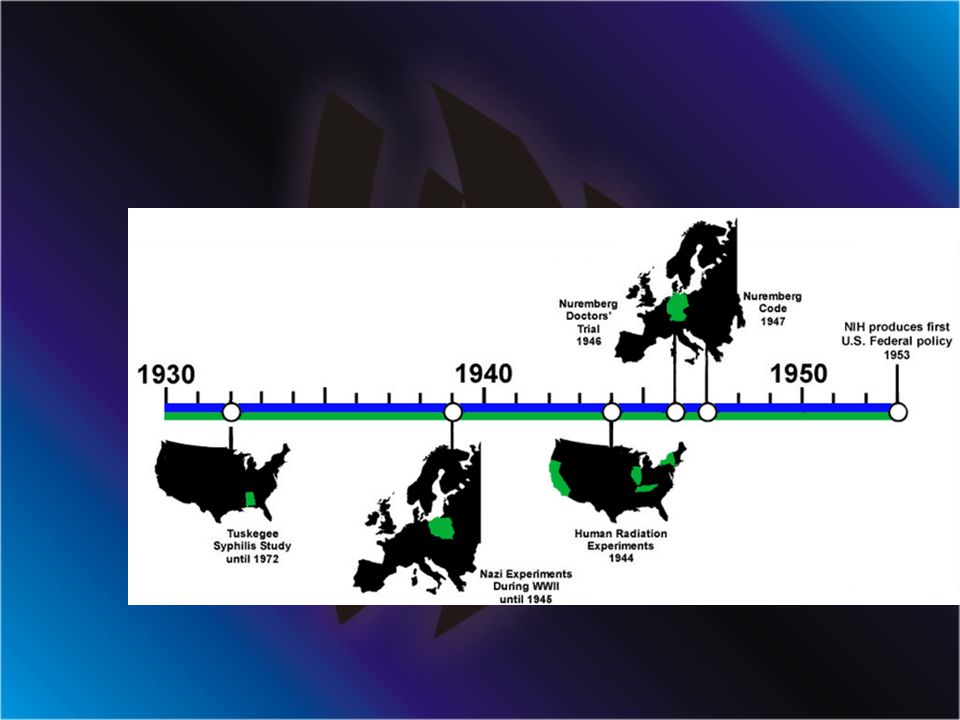
Historia de un esfuerzo por mejorar Hipócrates y “primero no dañar” Celso y su oposición a la “vivisección” 1830 en Inglaterra ley del consentimiento 1865 Claude Bernard “Principios de moralidad para clínicos y cirujanos” – No experimentar cuando puede esperarse daño aunque sea interesante. 1900 Prusia: no experimentar en minusválidos ni incompetentes. 1910 Paul Ehrlich: fármacoterapia igual responsabilidad que cirugía. 1931 Alemania “Guias para terapias innovativas y experimentación científica”

25
Bioética 1 Evidencia de un comportamiento médico cuestionable –Investigaciones clínicas –Torturas –Pena de muerte –Prisiones –Manicomios –Minorías étnicas

27
Investigaciones Nazis Inyectar gasolina intravenosa Inyectar virus vivos Mantener cepas de tifus usando como medios de cultivos prisioneros Inmersión en agua helada Prueba del paracaidista Ulceras cutáneas con fósforo

28
NUREMBERG EL JUICIO A LOS MEDICOS Los Jueces Los fiscales

29
NUREMBERG EL JUICIO A LOS MEDICOS Los acusados

30
Los experimentos

31
Código de Nuremberg 1945

32
NUREMBERG CODE The duty and responsibility for ascertaining the quality of the consent rests upon each individual who initiates, directs or engages in the experiment. It is a personal duty and responsibility which may not be delegated to another with impunity. 1.The voluntary consent of the human subject is absolutely essential. This means that the person involved should have legal capacity to give consent; should be so situated as to be able to exercise free power of choice, without the intervention of any element of force, fraud, deceit, duress, over-reaching, or other ulterior form of constraint or coercion; and should have sufficient knowledge and comprehension of the elements of the subject matter involved as to enable him to make an understanding and enlightened decision. This latter element requires that before the acceptance of an affirmative decision by the experimental subject there should be made known to him the nature, duration, and purpose of the experiment; the method and means by which it is to be conducted; all inconveniences and hazards reasonable to be expected; and the effects upon his health or person which may possibly come from his participation in the experiment.

33
2 The experiment should be such as to yield fruitful results for the good of society, unprocurable by other methods or means of study, and not random and unnecessary in nature. 3The experiment should be so designed and based on the results of animal experimentation and a knowledge of the natural history of the disease or other problem under study that the anticipated results will justify the performance of the experiment. 4The experiment should be so conducted as to avoid all unnecessary physical and mental suffering and injury. 5No experiment should be conducted where there is an a priori reason to believe that death or disabling injury will occur; except, perhaps, in those experiments where the experimental physicians also serve as subjects.

34
6.The degree of risk to be taken should never exceed that determined by the humanitarian importance of the problem to be solved by the experiment. 7. Proper preparations should be made and adequate facilities provided to protect the experimental subject against even remote possibilities of injury, disability, or death. 8. The experiment should be conducted only by scientifically qualified persons. The highest degree of skill and care should be required through all stages of the experiment of those who conduct or engage in the experiment. 9. During the course of the experiment the human subject should be at liberty to bring the experiment to an end if he has reached the physical or mental state where continuation of the experiment seems to him to be impossible. 10. During the course of the experiment the scientist in charge must be prepared to terminate the experiment at any stage, if he has probable cause to believe, in the exercise of the good faith, superior skill and careful judgment required of him that a continuation of the experiment is likely to result in injury, disability, or death to the experimental subject.

35
Tuskegee 1939 - 1975 Taliaferro, Clark ¿ Qué tienen en común todos ellos ?

36
Estudio Tuskegee Alabama 400 varones de raza negra afectados por sífilis y 200 controles. Engañados para el seguimiento sin tratamiento – bad blood- 1932 – 1972 a pesar de evidencias desde 1942 de que el grupo con sífilis evolucionaba peor que el control y que desde 1940 estaba disponible la penicilina

37
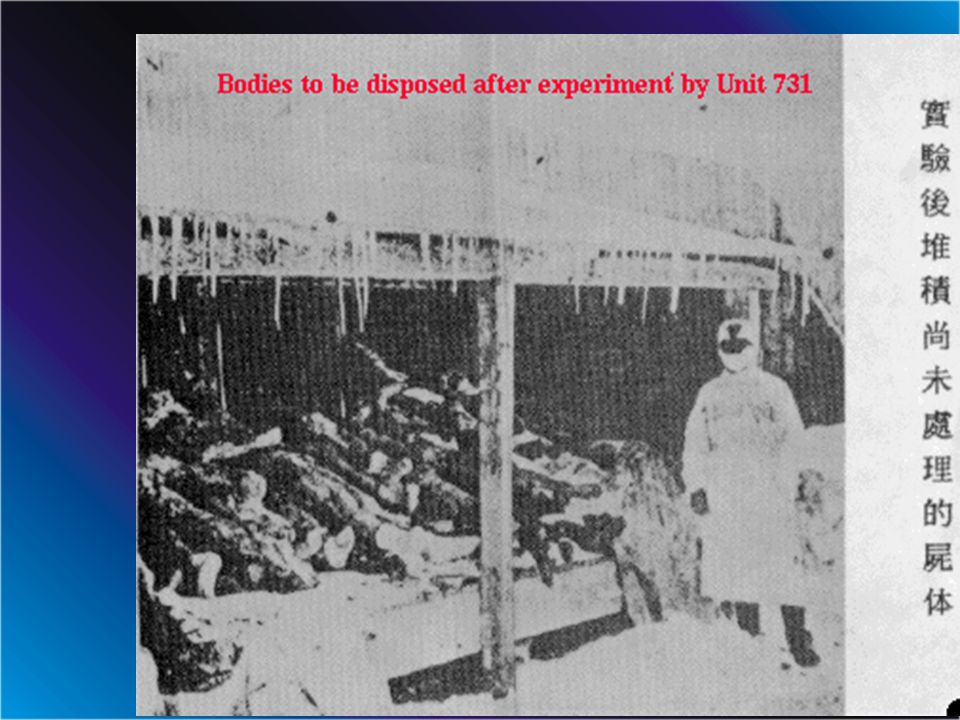
UNIDAD 731 JAPON

38
Ishii Shiro

39
Cirugía sin anestesia

41
Vivisección de una joven embarazada

42
Torre en memoria de los muertos en la unidad 731

43
Fisiología de Hierro y Calcio MIT y Harvard University 1949

44
Estudio con iones radioactivos Fe - Ca

47
Jewish Chronical Disease Hospital Study Nueva York 1963

49
Jewish Chronic Disease Hospital Study Rechazo de células cancerosas Pacientes “sanos” debilitados No se explicó el estudio para no generar miedo. Se consideró que no había riesgo porque los sanos rechazarían las células

50
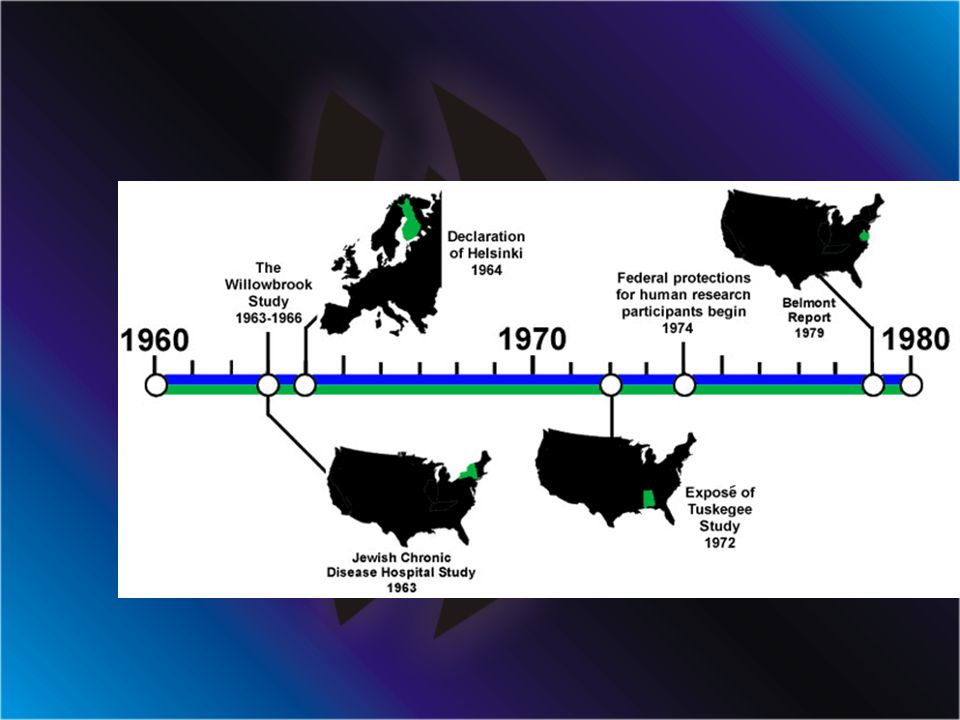
Willowbrook Study Nueva York 1963

53
DESARROLLO DE LA ETICA MEDICA De la deontología a la bioética. Empirismo Utilitarismo Kantianismo: deber ser Etica de principios Etica de valores

54
PRINCIPIOS BIOETICOS No maleficencia Beneficencia Autonomía Justicia

55
The Belmont Report Office of the Secretary Ethical Principles and Guidelines for the Protection of Human Subjects of Research The National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research April 18, 1979

56
National Commission for the Protection of Human Subjects of Biomedical and Behavioral Research Members of the Commission Kenneth John Ryan, M.D., Chairman, Chief of Staff, Boston Hospital for Women. Joseph V. Brady, Ph.D., Professor of Behavioral Biology, Johns Hopkins University. Robert E. Cooke, M.D., President, Medical College of Pennsylvania. Dorothy I. Height, President, National Council of Negro Women, Inc. Albert R. Jonsen, Ph.D., Associate Professor of Bioethics, University of California at San Francisco. Patricia King, J.D., Associate Professor of Law, Georgetown University Law Center. Karen Lebacqz, Ph.D., Associate Professor of Christian Ethics, Pacific School of Religion. *** David W. Louisell, J.D., Professor of Law, University of California at Berkeley. Donald W. Seldin, M.D., Professor and Chairman, Department of Internal Medicine, University of Texas at Dallas. ***Eliot Stellar, Ph.D., Provost of the University and Professor of Physiological Psychology, University of Pennsylvania. *** Robert H. Turtle, LL.B., Attorney, VomBaur, Coburn, Simmons & Turtle, Washington, D.C. *** Deceased.

57
1. Respect for Persons. -- Respect for persons incorporates at least two ethical convictions: first, that individuals should be treated as autonomous agents, and second, that persons with diminished autonomy are entitled to protection. The principle of respect for persons thus divides into two separate moral requirements: the requirement to acknowledge autonomy and the requirement to protect those with diminished autonomy.

58
An autonomous person is an individual capable of deliberation about personal goals and of acting under the direction of such deliberation. To respect autonomy is to give weight to autonomous persons' considered opinions and choices while refraining from obstructing their actions unless they are clearly detrimental to others. To show lack of respect for an autonomous agent is to repudiate that person's considered judgments, to deny an individual the freedom to act on those considered judgments, or to withhold information necessary to make a considered judgment, when there are no compelling reasons to do so.

59
In most cases of research involving human subjects, respect for persons demands that subjects enter into the research voluntarily and with adequate information.

60
2. Beneficence. -- Persons are treated in an ethical manner not only by respecting their decisions and protecting them from harm, but also by making efforts to secure their well- being. Such treatment falls under the principle of beneficence. The term "beneficence" is often understood to cover acts of kindness or charity that go beyond strict obligation. In this document, beneficence is understood in a stronger sense, as an obligation. Two general rules have been formulated as complementary expressions of beneficent actions in this sense: (1) do not harm and (2) maximize possible benefits and minimize possible harms.
 do not harm and (2) maximize possible benefits and minimize possible harms..")
61
3. Justice. -- Who ought to receive the benefits of research and bear its burdens? This is a question of justice, in the sense of "fairness in distribution" or "what is deserved." An injustice occurs when some benefit to which a person is entitled is denied without good reason or when some burden is imposed unduly. Another way of conceiving the principle of justice is that equals ought to be treated equally.

62
There are several widely accepted formulations of just ways to distribute burdens and benefits. Each formulation mentions some relevant property on the basis of which burdens and benefits should be distributed. These formulations are (1)to each person an equal share, (2)to each person according to individual need, (3)to each person according to individual effort, (4)to each person according to societal contribution, and (5)to each person according to merit.
to each person an equal share, (2)to each person according to individual need, (3)to each person according to individual effort, (4)to each person according to societal contribution, and (5)to each person according to merit..")
63
Questions of justice have long been associated with social practices such as punishment, taxation and political representation. Until recently these questions have not generally been associated with scientific research. However, they are foreshadowed even in the earliest reflections on the ethics of research involving human subjects. For example, during the 19th and early 20th centuries the burdens of serving as research subjects fell largely upon poor ward patients, while the benefits of improved medical care flowed primarily to private patients. Subsequently, the exploitation of unwilling prisoners as research subjects in Nazi concentration camps was condemned as a particularly flagrant injustice. In this country, in the 1940's, the Tuskegee syphilis study used disadvantaged, rural black men to study the untreated course of a disease that is by no means confined to that population. These subjects were deprived of demonstrably effective treatment in order not to interrupt the project, long after such treatment became generally available.

64
1.Informed Consent. 2. Assessment of Risks and Benefits 3. Selection of Subjects

65
Primer muerte por terapia génica

66
Declaración de Helsinki 1964 - 2000

67
WORLD MEDICAL ASSOCIATION DECLARATION OF HELSINKI.pdf.pdf The Helsinki Declaration in Norwegian.Norwegian Ethical Principles for Medical Research Involving Human Subjects Adopted by the 18th WMA General Assembly Helsinki, Finland, June 1964 and amended by the 29th WMA General Assembly, Tokyo, Japan, October 1975 35th WMA General Assembly, Venice, Italy, October 1983 41st WMA General Assembly, Hong Kong, September 1989 48th WMA General Assembly, Somerset West, Republic of South Africa, October 1996 and the 52nd WMA General Assembly, Edinburgh, Scotland, October 2000

68
A. INTRODUCTION 1. The World Medical Association has developed the Declaration of Helsinki as a statement of ethical principles to provide guidance to physicians and other participants in medical research involving human subjects. Medical research involving human subjects includes research on identifiable human material or identifiable data. 2. It is the duty of the physician to promote and safeguard the health of the people. The physician's knowledge and conscience are dedicated to the fulfillment of this duty.

69
7. In current medical practice and in medical research, most prophylactic, diagnostic and therapeutic procedures involve risks and burdens. 8. Medical research is subject to ethical standards that promote respect for all human beings and protect their health and rights. Some research populations are vulnerable and need special protection. The particular needs of the economically and medically disadvantaged must be recognized. Special attention is also required for those who cannot give or refuse consent for themselves, for those who may be subject to giving consent under duress, for those who will not benefit personally from the research and for those for whom the research is combined with care. 9. Research Investigators should be aware of the ethical, legal and regulatory requirements for research on human subjects in their own countries as well as applicable international requirements. No national ethical, legal or regulatory requirement should be allowed to reduce or eliminate any of the protections for human subjects set forth in this Declaration.

70
10. It is the duty of the physician in medical research to protect the life, health, privacy, and dignity of the human subject.

71
12. Appropriate caution must be exercised in the conduct of research which may affect the environment, and the welfare of animals used for research must be respected.

72
13. The design and performance of each experimental procedure involving human subjects should be clearly formulated in an experimental protocol. This protocol should be submitted for consideration, comment, guidance, and where appropriate, approval to a specially appointed ethical review committee, which must be independent of the investigator, the sponsor or any other kind of undue influence. This independent committee should be in conformity with the laws and regulations of the country in which the research experiment is performed. The committee has the right to monitor ongoing trials. The researcher has the obligation to provide monitoring information to the committee, especially any serious adverse events. The researcher should also submit to the committee, for review, information regarding funding, sponsors, institutional affiliations, other potential conflicts of interest and incentives for subjects.

73
19. Medical research is only justified if there is a reasonable likelihood that the populations in which the research is carried out stand to benefit from the results of the research. 20. The subjects must be volunteers and informed participants in the research project. 21. The right of research subjects to safeguard their integrity must always be respected. Every precaution should be taken to respect the privacy of the subject, the confidentiality of the patient's information and to minimize the impact of the study on the subject's physical and mental integrity and on the personality of the subject.

74
22. In any research on human beings, each potential subject must be adequately informed of the aims, methods, sources of funding, any possible conflicts of interest, institutional affiliations of the researcher, the anticipated benefits and potential risks of the study and the discomfort it may entail. The subject should be informed of the right to abstain from participation in the study or to withdraw consent to participate at any time without reprisal. After ensuring that the subject has understood the information, the physician should then obtain the subject's freely-given informed consent, preferably in writing. If the consent cannot be obtained in writing, the non-written consent must be formally documented and witnessed. 23.When obtaining informed consent for the research project the physician should be particularly cautious if the subject is in a dependent relationship with the physician or may consent under duress. In that case the informed consent should be obtained by a well-informed physician who is not engaged in the investigation and who is completely independent of this relationship.

75
27. Both authors and publishers have ethical obligations. In publication of the results of research, the investigators are obliged to preserve the accuracy of the results. Negative as well as positive results should be published or otherwise publicly available. Sources of funding, institutional affiliations and any possible conflicts of interest should be declared in the publication. Reports of experimentation not in accordance with the principles laid down in this Declaration should not be accepted for publication.

76
29. The benefits, risks, burdens and effectiveness of a new method should be tested against those of the best current prophylactic, diagnostic, and therapeutic methods. This does not exclude the use of placebo, or no treatment, in studies where no proven prophylactic, diagnostic or therapeutic method exists.

77
CODE OF FEDERAL REGULATIONS TITLE 45 PUBLIC WELFARE DEPARTMENT OF HEALTH AND HUMAN SERVICES NATIONAL INSTITUTES OF HEALTH OFFICE FOR PROTECTION FROM RESEARCH RISKS PART 46 PROTECTION OF HUMAN SUBJECTS * * * Revised November 13, 2001 Effective December 13, 2001

78
REQUISITOS ETICOS DE LAS INVESTIGACIONES CLINICAS Pacto Internacional de Derechos Civiles y Políticos Art 7: Nadie será sometido a torturas ni a penas o tratos crueles, inhumanos o degradantes.

79
REQUISITOS ETICOS DE LAS INVESTIGACIONES CLINICAS Pacto Internacional de Derechos Civiles y Políticos Constitución de la Nación Argentina - 1994 Art 7: Nadie será sometido a torturas ni a penas o tratos crueles, inhumanos o degradantes. En particular nadie será sometido sin su libre consentimiento a experimentos médicos o científicos.

80
REQUISITOS ETICOS DE LAS INVESTIGACIONES CLINICAS 5330/97 IGNORANCIA DE RESULTADO PROTOCOLO ESCRITO OBJETIVOS CLAROS NUMERO SUFICIENTE DE PACIENTES CONSENTIMIENTO INFORMADO SELECCIÓN DE INVESTIGADORES REVISION POR COMITÉ DE ETICA INFORMACION DE EFECTOS ADVERSOS SEVEROS SEGURO DE INVESTIGACION

81
REQUISITOS ETICOS DE LAS INVESTIGACIONES CLINICAS CONSENTIMIENTO INFORMADO COMPLETO CLARO PUNTOS INSOSLAYABLES: CARÁCTER INVESTIGACIONAL LIBRE ACEPTACION NO IMPACTO EN RELACION MEDICO-PACIENTE. FIRMADO EN PRESENCIA DE UN TESTIGO

82
FASES DE INVESTIGACION FASE 0 = PRECLINICA FASE I = TOLERANCIA (DMT - TDL) FASE II = RESPUESTA FASE III = COMPARACION CON STANDARD FASE IV = FARMACOVIGILANCIA EL PROBLEMA DE LAS INVESTIGACIONES QUE NO SIGUEN ESTE DESARROLLO ES LA FALTA DE RESPETO POR LA PERSONA ENFERMA Y EL RETRASO DE LAS INVESTIGACIONES
 FASE II = RESPUESTA FASE III = COMPARACION CON STANDARD FASE IV = FARMACOVIGILANCIA EL PROBLEMA DE LAS INVESTIGACIONES QUE NO SIGUEN ESTE DESARROLLO ES LA FALTA DE RESPETO POR LA PERSONA ENFERMA Y EL RETRASO DE LAS INVESTIGACIONES")
83
Bioética y Sociedad Evidencias de un comportamiento humano cuestionable –Derechos políticos (Rev. Francesa – Americana) –Derechos humanos (Post guerras mundiales S.XX) –Liberación femenina (“Pill revolution”) –Liberación existencial (Hippies) –Ecología (“Green Revolution)
 –Derechos humanos (Post guerras mundiales S.XX) –Liberación femenina ( Pill revolution ) –Liberación existencial (Hippies) –Ecología ( Green Revolution).")
84
1971 - Van Rensselaer Potter (oncólogo): Bioethics: bridge to the future –Puente entre la ciencia de la vida y la ética de la vida. –“Los valores éticos no pueden separarse de los hechos biológicos” –“La ciencia sin conciencia no conduce sino a la ruina del hombre” –Hacer ética no es un quehacer sólo de filósofos sino que pasa a ser un deber y un derecho de todo hombre.

87
Jacques Testart (“padre” de Amande la primer niña probeta francesa en 1982) –1987: “Yo, Jacques Testart, investigador en el campo de la biogenética, he decidido acabar definitivamente con la carrera enloquecida hacia la novedad científica; no quiero ir más lejos. Abandono por razones éticas ciertos campos de la investigación. Es preciso un control sobre las técnicas humanas de la procreación”. (Gonzalo Higueras - ¿Prudencia o miedo? – Razón y Fe, Marzo de 1987, pag 315

88
Dilemas éticos en Revistas médicas

89
Transdiciplinaridad

90
Dilemas clásicos

91
Metodología

92
Adaptación

93
Medicación OTC...y de las otras

94
Confidencialidad

95
Equidad

96
Justicia

97
Relaciones institucionales

98
Credibilidad 1

99
Credibilidad 2

100
Desafíos de las noticias 1 Clarin 8 de Febrero de 2002

101
Conflictos de intereses 1 JAMA 7 de Febrero 2002

102
Conflictos de intereses 1 Clarin 8 de Febrero de 2002

103
Conflictos de intereses 2

104
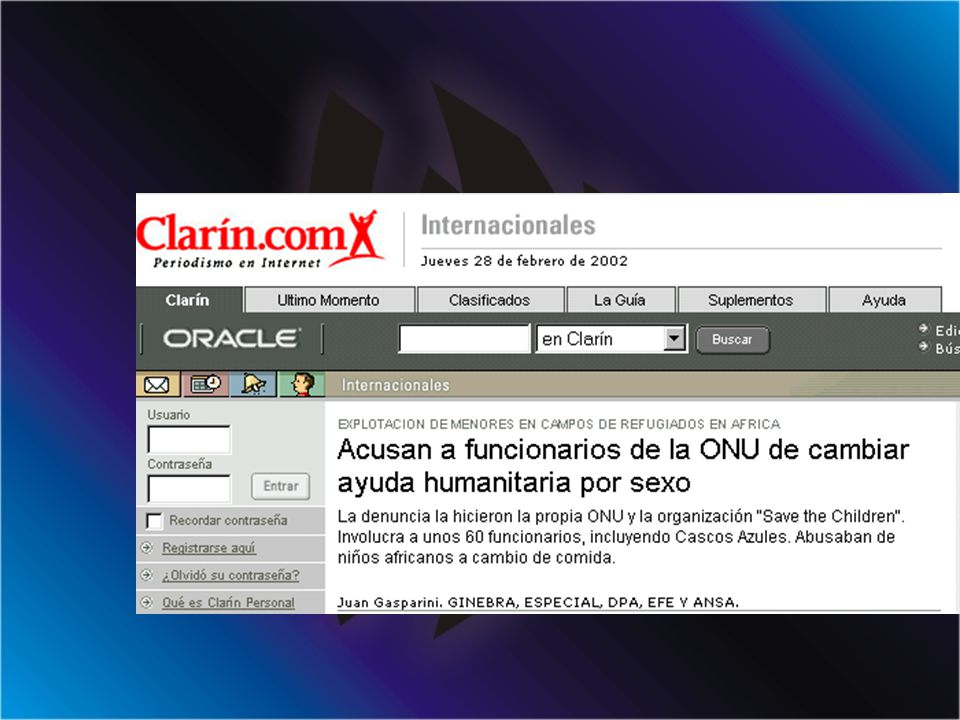
Desafíos de las noticias 2 Clarin 28 de Febrero de 2002

106
Clonación para transplante

107
Una lucha global contra este técnica

110
SEMIOLOGIA DE UN DILEMA ETICO Definición del problema (Motivo de consulta) –Conflicto de valores (fines o medios) Concepto de valor Axiología –Conflicto de comunicación (incomprensión) Comunicación Información –Conflicto de intereses (beneficios)
 –Conflicto de valores (fines o medios) Concepto de valor Axiología –Conflicto de comunicación (incomprensión) Comunicación Información –Conflicto de intereses (beneficios)")
111
Historia y significación (Enfermedad actual) –Cronología (secuencia temporal) Percepción Emociones –Causalidad (secuencia interpretativa) –Condicionantes (Five W : Who-What-When-Where-Why) –Requerimiento –Participantes SEMIOLOGIA DE UN DILEMA ETICO
 –Cronología (secuencia temporal) Percepción Emociones –Causalidad (secuencia interpretativa) –Condicionantes (Five W : Who-What-When-Where-Why) –Requerimiento –Participantes SEMIOLOGIA DE UN DILEMA ETICO")
112
Contrastación (Examen Físico) –Entrevista con el Requerido Cronología (secuencia temporal) –Percepción –Emociones Causalidad (secuencia interpretativa) Condicionantes –Evaluación de Historia Clínica y/o Documentos –Evaluación de lugar SEMIOLOGIA DE UN DILEMA ETICO
 –Entrevista con el Requerido Cronología (secuencia temporal) –Percepción –Emociones Causalidad (secuencia interpretativa) Condicionantes –Evaluación de Historia Clínica y/o Documentos –Evaluación de lugar SEMIOLOGIA DE UN DILEMA ETICO")
113
Terapéutica de un dilema ético Resolución arbitral Mediación Comité multidisciplinario –Hospitalario (institucional) –De investigaciones clínicas Justicia
 –De investigaciones clínicas Justicia")
114
Prevención de conflictos éticos Idoneidad Consistencia Coherencia Respeto Honestidad Humildad Veracidad Tolerancia

115
Prevención de mala praxis Prevención de conflictos éticos Registro completo

123
Aspectos generales e investigaciones con seres humanos Cuidado del paciente muriente Cuidado del paciente muriente Etica de la prescripción médica Etica de la prescripción médica Bioética

Presentaciones similares



 European Transfer Credit System (ECTS) Methodology in.>")

















