Descargar la presentación
La descarga está en progreso. Por favor, espere

1
FARMACOS HIPOGLUCEMIANTES
INSULINA y análogos 2. ANTIDIABETICOS ORALES: a) insulino-tropicos (SU,ME) b) insulino-sensibilizadores (BI,TIA) c) anti-hiperglicemiantes (Inh de alfa-glucosidasa e Inh de lipasa pancreatica). d) Incretinas: Agonistas de recep glucagon-like peptidos e inh de enzima dipeptidyl peptidasa 4.
 insulino-tropicos (SU,ME) b) insulino-sensibilizadores (BI,TIA) c) anti-hiperglicemiantes (Inh de alfa-glucosidasa e Inh de lipasa pancreatica). d) Incretinas: Agonistas de recep glucagon-like peptidos e inh de enzima dipeptidyl peptidasa 4.")
2
FARMACOS HIPOGLICEMIANTES INSULINA1
- Hormona polipeptidica de 51 aa con 2 cadenas (A de 21aa y B 30aa). - Sintetizada y secretada c beta de pancreas - x estimulo glucosidico. - Favorece el consumo de glucosa en tejidos perifericos.
. - Sintetizada y secretada c beta de pancreas. - x estimulo glucosidico. - Favorece el consumo de glucosa en tejidos perifericos.")
3
50% (11,13,14 U en desayuno, alm y merienda)
40-60 U/d 50% (basal, U/h) 50% (11,13,14 U en desayuno, alm y merienda)
 50% (11,13,14 U en desayuno, alm y merienda)")
4
TRANSPORTE de GLUCOSA

5
INSULINA ORIGEN y TIPOS
Al inicio, extraída de pancreas de animales (cerdo, alanina x treonina en posic 30 de cadena B; o bovinos) formacion de Ac. Insulinas “humanas”. Modificaciones de animales o x tecnicas recombinantes. Hoy análogos de insulina humana.
 formacion de Ac. Insulinas humanas . Modificaciones de animales o x tecnicas recombinantes. Hoy análogos de insulina humana.")
6
Acciones biológicas Efecto eminentemente anabólico. Induce a la captación tisular de glucosa (excepto en el SN) Síntesis de glucógeno en Hig y músculo esquelético. Síntesis intracelular de proteínas. Captación tisular de aminoácidos. Síntesis de glucosa a partir de aminoac.
 Síntesis de glucógeno en Hig y músculo esquelético. Síntesis intracelular de proteínas. Captación tisular de aminoácidos. Síntesis de glucosa a partir de aminoac.")
7
ACCION BIOLOGICA d) INCRETINAS:
a) Agonistas de recep glucagon-like peptidos b) Inh de enzima dipeptidyl peptidasa 4 (DPP-4). ACCION BIOLOGICA Síntesis de glucógeno
 Agonistas de recep glucagon-like peptidos. b) Inh de enzima dipeptidyl peptidasa 4 (DPP-4). ACCION BIOLOGICA. Síntesis de glucógeno.")
8
DOSIFICACION ACCION BIFASICA. Asocian rapidas y prl

9
INSULINAS CLASIFICACION
ANALOGOS de INSULINA HUMANA Insulina Aspart (Novolog) Insulina Lispro (humalog). 3. Insulina Glargina (lantus). VENTAJAS: acción ultrarápida y >tiempo de acción (24 h), potencia moderada.
 Insulina Lispro (humalog). 3. Insulina Glargina (lantus). VENTAJAS: acción ultrarápida y >tiempo de acción (24 h), potencia moderada.")
10
VIAS DE ADMINISTRACION
Vía subcutánea Vía intramuscular Vía intravenosa Vía oral Vía inhalatoria Via i.peritoneal Jeringuilla a 45o A New Way to Inhale, Not Inject, Insulin. October 10, 2009 PEOPLE with diabetes often inject themselves with insulin at mealtime to help control their blood sugar levels. But a new, palm-size device may let them discretely inhale a dose of insulin instead of using a needle. The insulin powder, called Afresa, is inhaled into the lungs, dissolves there and then travels into the bloodstream.

11
VIAS DE ADMINISTRACION
s.c. : 1periumbilical, 2brazos, 3muslos (1, 45%+ biodisponibilidad que 3). >absorcion por actividad fisica, masaje local y calor. frio. Forma de inyectar (jeringuillas, 45o) Mezcla de preparados. En 5’(glargina no con I regular o rapida). Insulina IM o IV?. Hiperglicemia severa o coma diabetico Rectal, oral y nasal (liposomas cargadas de insulina).
. >absorcion por actividad fisica, masaje local y calor. frio. Forma de inyectar (jeringuillas, 45o) Mezcla de preparados. En 5’(glargina no con I regular o rapida). Insulina IM o IV . Hiperglicemia severa o coma diabetico. Rectal, oral y nasal (liposomas cargadas de insulina).")
12
VÌAS DE ADMINISTRACIÒN
En muslos en horas del día?

13
Dosificacion: Insulina RAPIDA
Cada 4-6 h, s.c. 1 U actrapid….. 100 kcal de alimento. 1-2 U ………… 20g hidratos de carbono. U……. bajar mg/dl de glicemia. U …… en DM descompensados.

14
Dosificacion: Insulina INTERMEDIA (NPH) y LENTA. s.c.
U/kg/d, en monodosis (am) o bi-dosis (70% am). “Mezclas”comerciales: Rapida+intermedia o lenta: Rapida tid (35% desay, 20% alm y 25% merien) + NPH (20%) pm o en desayuno. Mezcla en “casa”: am: 1U de rapida x cada 3-4 de NPH; pm:1U rapida x cada 2U de NPH.
 o bi-dosis (70% am). Mezclas comerciales: Rapida+intermedia o lenta: Rapida tid (35% desay, 20% alm y 25% merien) + NPH (20%) pm o en desayuno. Mezcla en casa : am: 1U de rapida x cada 3-4 de NPH; pm:1U rapida x cada 2U de NPH.")
15
Ultrarapida (Lyspro, Aspart). 0.04-0.20 U/kg s.c./ingesta alimentaria.
Dosificacion: ANALOGOS de INSULINA Ultrarapida (Lyspro, Aspart) U/kg s.c./ingesta alimentaria. Accion prolongada (glargina) U/kg en am ó pm.
 U/kg s.c./ingesta alimentaria. Accion prolongada (glargina) U/kg en am ó pm.")
16
REACCIONES ADVERSAS: HIPOGLICEMIA Lipotimia o desmayo

17
pacientes en fase I CONSCIENTE
EFECTOS SECUNDARIOS HIPOGLICEMIA X: - dosis excesivas de insulina, - deficiente ingesta alimentaria, - Esfuerzo fisico exagerado Recomend g de HC x c/30-45 min de actividad fisica. pacientes en fase II Hay del nivel del sensorio pacientes en fase I CONSCIENTE NO DEBEN RECIBIR NINGUNA SOLUCION x VIA ORAL, como máximo la colocación de AZUCAR en POLVO bajo la lengua I.v. Dx 5-10% a chorro. diaforesis taquicardia Cefaleas SE CONTROLA con INGESTA de HIDRATOS de CARBONO de ABSORCION RAPIDA e INTERMEDIA (agua azucarada, vaso de leche, zumo de frutas, caramelos).
.")
18
INSULINA TX hipoglicemia:
Fase III (coma hipoglicemico) i.v. bolo g de glucosa y luego infusion continua o, 1 amp de GLUCAGON 1 mg im o iv (reversion de la hipoglicemia en minutos).
 i.v. bolo g de glucosa y luego infusion continua o, 1 amp de GLUCAGON 1 mg im o iv (reversion de la hipoglicemia en minutos).")
19
INSULINA Lipodistrofia o lipoatrofia.
Suspension de Insulina? = cetoacidosis diabetica en horas. Lipodistrofia o lipoatrofia. Celulitis y abscesos sc.

20
HIPOGLICEMIANTES ORALES

21
HIPOGLUCEMIANTES ORALES CLASIFICACION (X mecanismo de accion)
1. Insulino sensibilizadores: 2.1. Biguanidas: metformina (Glucofage) 2.2. Tiazolidindionas o glitazonas: rosiglitazona, pioglitazona 2. Insulino tropicos: 1.1. Sulfonilureas: glibenclamida (euglucon, daonil), gliclazida (diamicron), clorpropamida (diabinese, melitase), tolazamida (tolinase), glimepidine, tolbulamida. 1.2. Meglitinidas: nateglinida y repaglinida
 2.2. Tiazolidindionas o glitazonas: rosiglitazona, pioglitazona. 2. Insulino tropicos: 1.1. Sulfonilureas: glibenclamida (euglucon, daonil), gliclazida (diamicron), clorpropamida (diabinese, melitase), tolazamida (tolinase), glimepidine, tolbulamida Meglitinidas: nateglinida y repaglinida.")
22
3. Anti hiperglicemiantes:
3.1. Inhibidores de alfa-glucosidasa: acarbosa y miglitol (Glyset). 3.2. Inhibidores de lipasa pancreatica: orlistat
 Inhibidores de lipasa pancreatica: orlistat.")
23
-Inhibidores de la Biguanidas: 2. INSULINO-TROPICOS
SENSIBILIZADORAS 2. INSULINO-TROPICOS 3. ANTI-HIPERGLICEMIANTES (ascarbosa y miglitol) -Inhibidores de la lipasa pancreatica (orlistat)
 -Inhibidores de la. lipasa pancreatica (orlistat)")
24
SULFUNILUREAS (Insulinotropicas) Clasificación de las SU
De Duración Corta Glibenclamida (droga prototipo) Tolbutamida Glipizida Gliquidona Gliciclamida De Duración intermedia Glicazida (droga prototipo) Acetohexamida Glibormurida De duración prolongada Cloropropamida (Diabinese)
 Tolbutamida Glipizida Gliquidona Gliciclamida. De Duración intermedia. Glicazida (droga prototipo) Acetohexamida Glibormurida. De duración prolongada. Cloropropamida (Diabinese)")
25
MECANISMO DE ACCIÓN

26
HIPOGLUCEMIANTES ORALES 1. Insulinotropicos:
1.2. MEGLITINIDAS Nagletinida (Starlix tab mg) y Repaglimida (Prandin). -Son insulinotropicos o liberadores o secretagogos. -Mec acción = a SU. Opera cerrando los canales de K en cel beta de pancreas. -Accion + rapida q’ SU -Hipoglicemias raras.
 y Repaglimida (Prandin). -Son insulinotropicos o liberadores o secretagogos. -Mec acción = a SU. Opera cerrando los canales de K en cel beta de pancreas. -Accion + rapida q’ SU. -Hipoglicemias raras.")
27
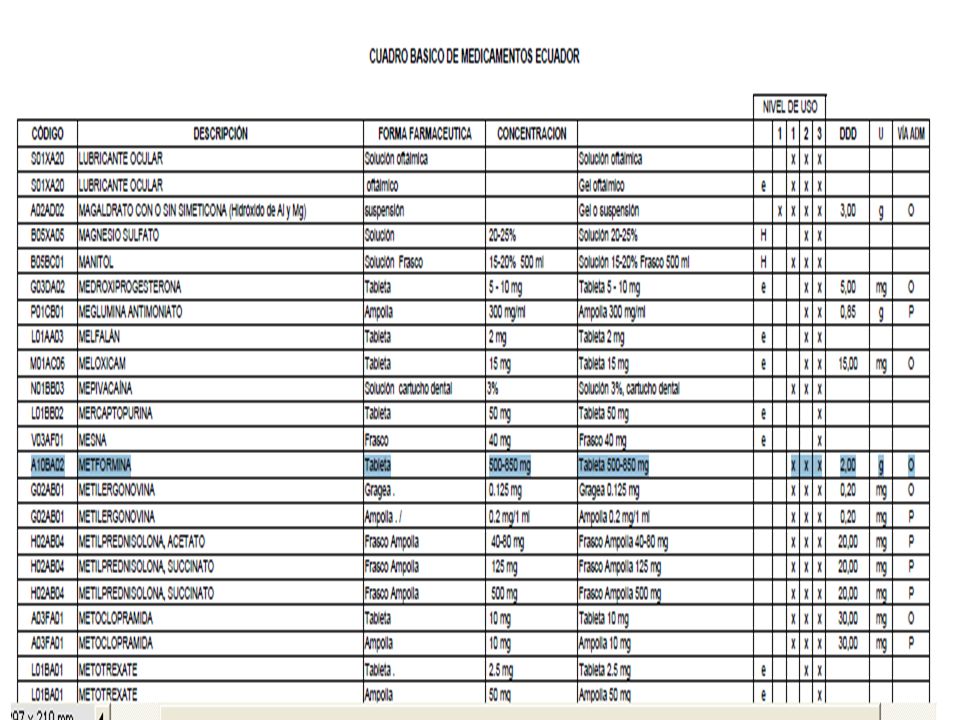
METFORMINA 2. INSULINO SENSIBILIZADORES 2.1. BIGUANIDAS
Cada Tableta recubierta contiene Metformina Clorhidrato 500 u 850 mg Dosis inicial: 500 mg 2 veces al día u 850 mg diarios con las comidas, incremente 500 mg por semana dos veces al día o 850 mg cada 2 semanas

29
2. INSULINO SENSIBILIZADORES 2.1. BIGUANIDAS (metformina)
")
30
2. INSULINO SENSIBILIZADORES
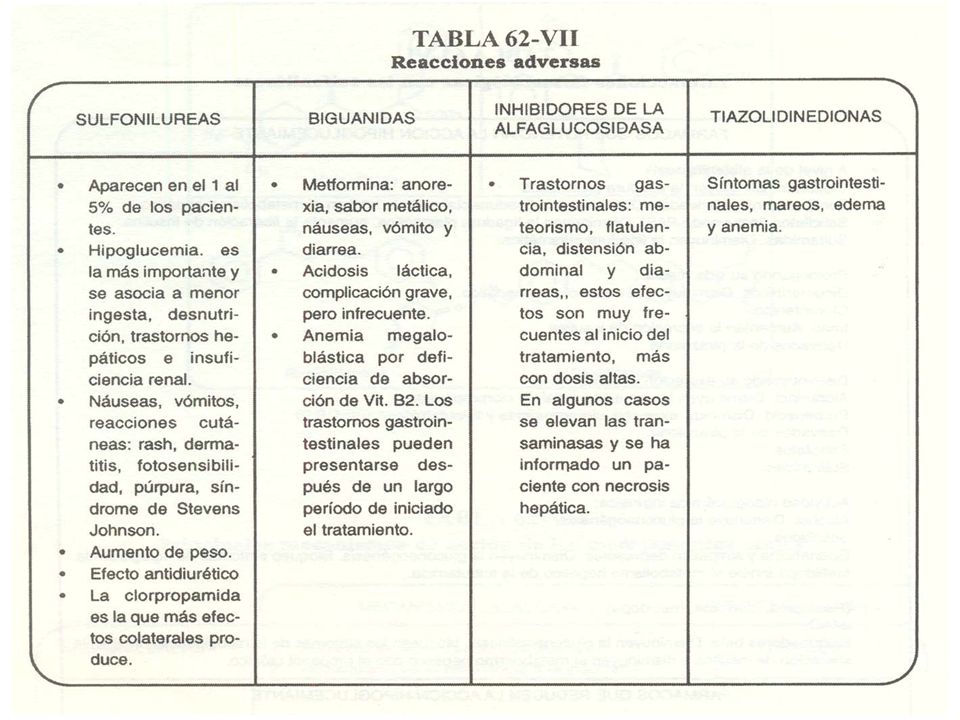
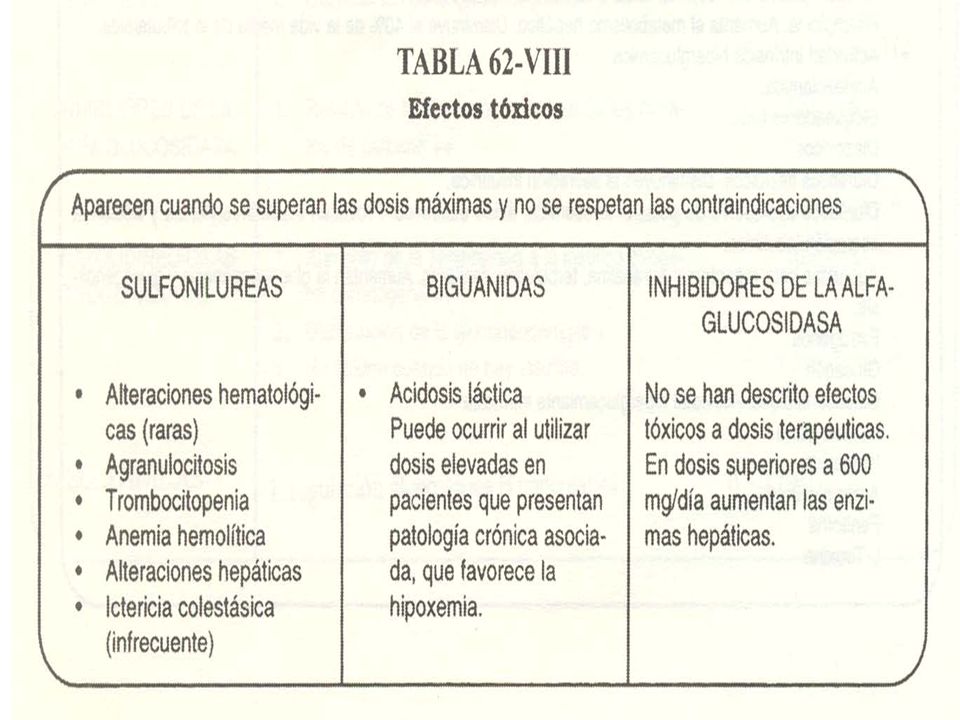
2.1. BIGUANIDAS REACCIONES ADVERSAS: METFORMINA: -Trastornos G-I: Anorexia, sabor metálico, n-v. -Anemia megaloblastica -Acidosis lactica !

31
Fármaco utilizado por diabéticos tiene propiedades anti- cancerígenas 21 de enero del EFE, Barcelona Estudios han comprobado que la metformina, uno de los compuestos más utilizados en el tratamiento de la diabetes, reduce el riesgo de padecer cáncer de mama. Investigadores españoles han desvelado que la metformina, uno de los fármacos más utilizados en el tratamiento de la diabetes II, tiene un efecto anticancerígeno en los tumores de mama. Too Ca ovario.

32
2. INSULINO SENSIBILIZADORES 2. 2
2. INSULINO SENSIBILIZADORES 2.2. TIAZOLIDINDIONAS (glitazonas) Rosiglitazona (retirada x ataques cardiacos), pioglitazona (riesgo de Ca vejiga), ciglitazona y troglitazona (retirada por hepatotx). <eficaces q’ SU y Metformina. hiperglicemia, hiperinsulinismo, mejora la dislipidemia (x actividad de insulina). gluconeogenesis hepatica y cantidad de acidos grasos.
 Rosiglitazona (retirada x ataques cardiacos), pioglitazona (riesgo de Ca vejiga), ciglitazona y troglitazona (retirada por hepatotx). <eficaces q’ SU y Metformina. hiperglicemia, hiperinsulinismo, mejora la dislipidemia (x actividad de insulina). gluconeogenesis hepatica y cantidad de acidos grasos.")
33
HIPOGLUCEMIANTES ORALES TIAZOLIDINDIONAS (glitazonas)
En DM-2 solos o + otros hipoglicem orales Efecto luego de 6-12 h Demoran 1-3 meses para efectos mx hipoglic. Reacciones adversas: Edema, anemia, peso. Vigilar la función hepatica.

34
Brasil también ordena la retirada del mercado de rosiglitazona AVANDIA
To: "'Essential Drugs in Spanish'" Río de Janeiro, 29 sep (EFE) El Gobierno brasileño ordenó hoy la retirada del mercado de la medicina contra la diabetes Avandia, una medida similar a la adoptada la semana pasada por la Agencia Europa del Medicamento (EMEA) debido al riesgo de ataques cardíacos. FDA también había anunciado la semana pasada restricciones a la venta de la medicina producida por la multinacional GlaxoSmithKline aunque mantuvo la autorización para su distribución y comercialización. "Entre los problemas identificados durante la evaluación del Avandia está la alta probabilidad de ocurrencia de infarto de miocardio, insuficiencia cardíaca, derrame y otros disturbios cardíacos asociados al uso del producto", agrega la nota.
 El Gobierno brasileño ordenó hoy la retirada del mercado de la medicina contra la diabetes Avandia, una medida similar a la adoptada la semana pasada por la Agencia Europa del Medicamento (EMEA) debido al riesgo de ataques cardíacos. FDA también había anunciado la semana pasada restricciones a la venta de la medicina producida por la multinacional GlaxoSmithKline aunque mantuvo la autorización para su distribución y comercialización. Entre los problemas identificados durante la evaluación del Avandia está la alta probabilidad de ocurrencia de infarto de miocardio, insuficiencia cardíaca, derrame y otros disturbios cardíacos asociados al uso del producto , agrega la nota.")
35
Pioglitazone and the risk of bladder cancer BMJ 2012;344:e3500
Risks seem to outweigh benefits as yet more evidence emerges Therapeutic strategies must be chosen with an accurate and updated assessment of both expected benefits and potential risks to sustain the confidence of patients and guarantee safety. Azoulay and colleagues found that more than two years daily exposure to pioglitazone doubled the risk of bladder cancer.1 They also found an association between bladder cancer and both the dose and the duration of pioglitazone treatment . Firstly, it has recently been shown that pioglitazone has a pharmacological profile comparable to that of the glitazar compounds.2 These dual α and γ peroxisome proliferator activated receptor agonists were developed to improve both glucose and lipid metabolic parameters but were rapidly withdrawn mainly on the grounds of carcinogenic effects in animals. Secondly, before marketing authorisation (1999 in the United States, 2000 in Europe), preclinical data on pioglitazone reported the occurrence of bladder cancers in male rats.3 These data were added to the pioglitazone Summary of Product Characteristics without specific information for prescribers, particularly recommendations for patient selection and monitoring. That the risk of bladder cancer might be comparable in humans was rejected by a mechanistic hypothesis that involved pioglitazone induced urolithiasis leading to chronic irritation of the bladder in rats. Surprisingly, urine analysis data from clinical trials were not extensively investigated. Later, in 2011, experimental work showed that although an acid forming diet reduced both the number of calculi and bladder cancers in male rats, the diet did not reduce the incidence of hyperplasia.4 Thirdly, in the 2005 report of the PROactive randomised clinical trial, which compared pioglitazone with placebo, the number of true bladder cancers was not correctly counted in the placebo arm, which masked the difference between groups.5 Fourthly, additional information from postmarketing observational studies suggests a positive association between chronic exposure to pioglitazone and bladder cancer. These studies included one study of the US Food and Drug Administration (FDA) Adverse Event Reporting System (reporting odds ratio 4.30, 95% confidence interval 2.82 to 6.52)6; one interim analysis of the US Kaiser Permanente Northern California prospective cohort (exposure >2 years: hazard ratio 1.4, 1.03 to 2.0),7which resulted in an FDA warning on September 20108; and one retrospective cohort from the French health insurance database (overall hazard ratio 1.22, 1.05 to 1.43; exposure >2 years 1.34, 1.04 to 1.79),9 which led to the suspension of pioglitazone in France in June Since then, two retrospective cohorts using the Taiwanese reimbursement database failed to show any significant association: one may have lacked statistical power,11 and the other could not exclude a potential increased risk for exposure greater than three years (odds ratio 1.56, 0.51 to 4.74).12 Lastly, on 20 December 2011, the last version of the Summary of Product Characteristics for pioglitazone showed that, in a meta-analysis of randomised clinical trials, cases of bladder cancer were reported more often with pioglitazone (19 cases in 12 506 patients; 0.15%) than in control groups (seven cases in 10 212 patients; 0.07%), with a hazard ratio of 2.64 (1.11 to 6.31; P=0.029).3 Since then, the European Medicines Agency stated that pioglitazone is contraindicated in patients with current bladder cancer, a history of bladder cancer, or uninvestigated macroscopic haematuria, and that risk factors for bladder cancer should be assessed before starting pioglitazone treatment. Patients are advised to report macroscopic haematuria or other urinary symptoms promptly.13 These criteria may not be sufficient to avoid the exposure of patients at risk and to properly monitor treated patients. Taking into account Azoulay and colleagues’ current findings and given the consistency of these results, the relative strength of the association, the dose-response effect, the known pharmacodynamic characteristics of pioglitazone, and evidence of a significant association in a meta-analysis of randomised trials, it can confidently be assumed that pioglitazone increases the risk of bladder cancer. It also seems that this association could have been predicted earlier. Worldwide, exposure to pioglitazone is estimated to be more than 20 million patient years.13Considering that the benefit of pioglitazone in reducing cardiovascular events is questionable, prescribers who are ultimately responsible for therapeutic choices can legitimately question whether the benefit-risk ratio of pioglitazone is still acceptable for their patients with diabetes.
, preclinical data on pioglitazone reported the occurrence of bladder cancers in male rats.3 These data were added to the pioglitazone Summary of Product Characteristics without specific information for prescribers, particularly recommendations for patient selection and monitoring. That the risk of bladder cancer might be comparable in humans was rejected by a mechanistic hypothesis that involved pioglitazone induced urolithiasis leading to chronic irritation of the bladder in rats. Surprisingly, urine analysis data from clinical trials were not extensively investigated. Later, in 2011, experimental work showed that although an acid forming diet reduced both the number of calculi and bladder cancers in male rats, the diet did not reduce the incidence of hyperplasia.4. Thirdly, in the 2005 report of the PROactive randomised clinical trial, which compared pioglitazone with placebo, the number of true bladder cancers was not correctly counted in the placebo arm, which masked the difference between groups.5. Fourthly, additional information from postmarketing observational studies suggests a positive association between chronic exposure to pioglitazone and bladder cancer. These studies included one study of the US Food and Drug Administration (FDA) Adverse Event Reporting System (reporting odds ratio 4.30, 95% confidence interval 2.82 to 6.52)6; one interim analysis of the US Kaiser Permanente Northern California prospective cohort (exposure >2 years: hazard ratio 1.4, 1.03 to 2.0),7which resulted in an FDA warning on September 20108; and one retrospective cohort from the French health insurance database (overall hazard ratio 1.22, 1.05 to 1.43; exposure >2 years 1.34, 1.04 to 1.79),9 which led to the suspension of pioglitazone in France in June Since then, two retrospective cohorts using the Taiwanese reimbursement database failed to show any significant association: one may have lacked statistical power,11 and the other could not exclude a potential increased risk for exposure greater than three years (odds ratio 1.56, 0.51 to 4.74).12. Lastly, on 20 December 2011, the last version of the Summary of Product Characteristics for pioglitazone showed that, in a meta-analysis of randomised clinical trials, cases of bladder cancer were reported more often with pioglitazone (19 cases in patients; 0.15%) than in control groups (seven cases in patients; 0.07%), with a hazard ratio of 2.64 (1.11 to 6.31; P=0.029).3. Since then, the European Medicines Agency stated that pioglitazone is contraindicated in patients with current bladder cancer, a history of bladder cancer, or uninvestigated macroscopic haematuria, and that risk factors for bladder cancer should be assessed before starting pioglitazone treatment. Patients are advised to report macroscopic haematuria or other urinary symptoms promptly.13 These criteria may not be sufficient to avoid the exposure of patients at risk and to properly monitor treated patients. Taking into account Azoulay and colleagues’ current findings and given the consistency of these results, the relative strength of the association, the dose-response effect, the known pharmacodynamic characteristics of pioglitazone, and evidence of a significant association in a meta-analysis of randomised trials, it can confidently be assumed that pioglitazone increases the risk of bladder cancer. It also seems that this association could have been predicted earlier. Worldwide, exposure to pioglitazone is estimated to be more than 20 million patient years.13Considering that the benefit of pioglitazone in reducing cardiovascular events is questionable, prescribers who are ultimately responsible for therapeutic choices can legitimately question whether the benefit-risk ratio of pioglitazone is still acceptable for their patients with diabetes.")
36
FDA, April, 15th 2014 The U.S. Food and Drug Administration today approved Tanzeum (albiglutide) subcutaneous injection to improve glycemic control, along with diet and exercise, in adults with type 2 diabetes. Type 2 diabetes affects approximately 24 million people and accounts for more than 90 percent of diabetes cases diagnosed in the United States. Over time, high blood sugar levels can increase the risk for serious complications, including heart disease, blindness, and nerve and kidney damage. Tanzeum is a glucagon-like peptide-1 (GLP-1) receptor agonist, a hormone that helps normalize blood sugar levels. The drug’s safety and effectiveness were evaluated in eight clinical trials involving more than 2,000 patients with type 2 diabetes. Patients participating in the trials showed an improvement in their HbA1c level (hemoglobin A1c or glycosylated hemoglobin, a measure of blood sugar control).
 subcutaneous injection to improve glycemic control, along with diet and exercise, in adults with type 2 diabetes. Type 2 diabetes affects approximately 24 million people and accounts for more than 90 percent of diabetes cases diagnosed in the United States. Over time, high blood sugar levels can increase the risk for serious complications, including heart disease, blindness, and nerve and kidney damage. Tanzeum is a glucagon-like peptide-1 (GLP-1) receptor agonist, a hormone that helps normalize blood sugar levels. The drug’s safety and effectiveness were evaluated in eight clinical trials involving more than 2,000 patients with type 2 diabetes. Patients participating in the trials showed an improvement in their HbA1c level (hemoglobin A1c or glycosylated hemoglobin, a measure of blood sugar control).")
37
ACCION BIOLOGICA d) INCRETINAS:
a) Agonistas recep glucagon-like peptidos (GLP-1) b) Inh de enzima dipeptidyl peptidasa 4 (DPP-4). ACCION BIOLOGICA Síntesis de glucógeno
 Agonistas recep glucagon-like peptidos (GLP-1) b) Inh de enzima dipeptidyl peptidasa 4 (DPP-4). ACCION BIOLOGICA. Síntesis de glucógeno.")
38
3. ANTI-HIPERGLICEMIANTES 3. 1
3. ANTI-HIPERGLICEMIANTES 3.1. INHIBIDORES de ALFA-GLUCOSIDASA: Acarbosa y miglitol (Glyset) 3.2. INHIBIDORES LIPASA PANCREATICA (orlistat) 3.2. INH de LIPASA PANCREATICA 3.1. Inh competitivos de alfa-glucosidasas intestinales (digieren los sacaridos a monosacaridos) = retraso o ↓absorcion hiperglicemia. 3.2. sintesis post-prandial de lipidos (VLDL y trigliceridos). Tomar antes de comer!.
 3.2. INHIBIDORES LIPASA PANCREATICA (orlistat) 3.2. INH de LIPASA PANCREATICA Inh competitivos de alfa-glucosidasas intestinales (digieren los sacaridos a monosacaridos) = retraso o ↓absorcion hiperglicemia sintesis post-prandial de lipidos (VLDL y trigliceridos). Tomar antes de comer!.")
39
Over-the-counter medicines: in whose best interests?
The Lancet, Volume 373, Issue 9661, Page 354, 31 January 2009 Last week, the European Union (EU) approved the anti-obesity drug, orlistat, for sale over-the-counter (OTC). Orlistat is already available OTC in the USA and Australia. The EU decision means that this drug can now be sold by pharmacists throughout Europe to people with a body-mass index over 28 in 60 mg tablets—half the recommended daily dose—after consultation. The EU decision falls in line with its view that no medicine should remain as prescription only unless necessary for safety reasons. However, better accessibility to orlistat may not necessarily be in the best interests of the public. Orlistat has limited effect in the management of obesity—the average weight loss per year is only 2·5 kg. Making this drug available OTC will add false credibility to the notion that there is an easy pill-popping solution to obesity rather than long-term lifestyle changes—part of the holistic approach necessary in the management of all obese patients. OTC sales of orlistat will be much more expensive than through prescription only—roughly £1·47 (US$2) per day in England, for example, versus the £7·10 cost per monthly prescription. And although pharmacists will discuss side-effects such as steatorrhoea, lack of medical supervision means that overuse could lead to undiagnosed nutritional deficiencies.
 approved the anti-obesity drug, orlistat, for sale over-the-counter (OTC). Orlistat is already available OTC in the USA and Australia. The EU decision means that this drug can now be sold by pharmacists throughout Europe to people with a body-mass index over 28 in 60 mg tablets—half the recommended daily dose—after consultation. The EU decision falls in line with its view that no medicine should remain as prescription only unless necessary for safety reasons. However, better accessibility to orlistat may not necessarily be in the best interests of the public. Orlistat has limited effect in the management of obesity—the average weight loss per year is only 2·5 kg. Making this drug available OTC will add false credibility to the notion that there is an easy pill-popping solution to obesity rather than long-term lifestyle changes—part of the holistic approach necessary in the management of all obese patients. OTC sales of orlistat will be much more expensive than through prescription only—roughly £1·47 (US$2) per day in England, for example, versus the £7·10 cost per monthly prescription. And although pharmacists will discuss side-effects such as steatorrhoea, lack of medical supervision means that overuse could lead to undiagnosed nutritional deficiencies.")
43
HIPOGLUCEMIANTES ORALES CLASIFICACION (X mecanismo de accion)
1. Insulinotropicos: 1.1. Sulfonilureas: glibenclamida (euglucon, daonil), gliclazida (diamicron), clorpropamida (diabinese, melitase), tolazamida (tolinase), glimepidine, tolbulamida. 1.2. Meglitinidas: nateglinida y repaglinida 2. Insulino sensibilizadores: 2.1. Biguanidas: metformina (Glucofage) 2.2. Tiazolidindionas o glitazonas: rosiglitazona, pioglitazona. 3. Anti-hiperglicemiantes: 3.1. Inhibidores de alfa-glucosidasa: acarbosa y miglitol (Glyset). 3.2. Inhibidores de lipasa pancreatica: orlistat
, gliclazida (diamicron), clorpropamida (diabinese, melitase), tolazamida (tolinase), glimepidine, tolbulamida Meglitinidas: nateglinida y repaglinida. 2. Insulino sensibilizadores: 2.1. Biguanidas: metformina (Glucofage) 2.2. Tiazolidindionas o glitazonas: rosiglitazona, pioglitazona. 3. Anti-hiperglicemiantes: 3.1. Inhibidores de alfa-glucosidasa: acarbosa y. miglitol (Glyset) Inhibidores de lipasa pancreatica: orlistat.")
44
EDULCORANTES Sustitutos del azúcar común Confieren sabor dulce a los alimentos, sin producir obesidad o descompensación en pctes con D.M. Poder Edulcorante? Comparando el sabor de una sust en solucion con 30 g de azucar dusueltos en 1 L de agua a 20 oC.

45
Edulcorantes energéticos
y no energéticos 1. 2. Polialcoholes . Lactitol

46
EDULCORANTES ENERGETICOS
FRUCTOSA GLUCOSA POLIALCOHOLES O SACAROSA lactitol manitol < PODER EDULCORANTE QUE EL AZUCAR. Sorbitol Xilitol

47
FRUCTOSA Monosacarido en FRUTAS y MIEL
Se absorbe a través del I.D. y pasa por el hígado (poco influye en glicemia). 30% se convierte en glucosa, 70% es metabolizado. Diabético puede ingerir g/d. 1 g de fructosa = 4 Kcal.
. 30% se convierte en glucosa, 70% es metabolizado. Diabético puede ingerir g/d. 1 g de fructosa = 4 Kcal.")
48
SE CONVIERTE en GLUCOSA en el HIGADO !. Produce = calorías q` glucosa.
-alcohol-azúcar En: algas rojas y frutas (peras, manz, cerezas, melocotones. sorbitol La ingesta de grandes cant. puede provocar diarrea. NO ADM. en DIABETICOS sin CONTROL de GLUCEMIA En: helados, xa endulzar caramelos y chicles, bombones de fruta, chocolate y glosinas. SE CONVIERTE en GLUCOSA en el HIGADO !. Produce = calorías q` glucosa.

49
NO TIENE VENTAJAS SOBRE OTROS EDULCORANTES
XILITOL Sabor dulce=sacarosa= calorías NO TIENE VENTAJAS SOBRE OTROS EDULCORANTES

50
manitol De la manosa Su uso poco frecuente
Algas, hierbas hongos,frutas Su uso poco frecuente

51
lactitol Galletas, helados , mermeladas, pasteles De Lactosa
Ideal en repostería x` tolera altas oT 1 gr = 2 kcal Galletas, helados , mermeladas, pasteles Ingerida en exceso: diarrea, flatulencia

52
(Azucar) (dextrosa)
 (dextrosa)")
53
EDULCORANTES NO ENERGETICOS
O ACALORICOS Tienen un sabor intensamente dulce: sacarina, ciclamato, aspartame, sucralosa, acesulfamo k. Sacarina (hermesetas tab y liquido) -Artificial -+ utilizado, v + potente q` sacarosa, barato. -Ca vejiga (ratas). – Sabor metálico. No aporta H.C. ni energía
 -Artificial. -+ utilizado, v + potente q` sacarosa, barato. -Ca vejiga (ratas). – Sabor metálico. No aporta H.C. ni energía.")
54
ciclamato -Artificial -30 veces más edulcorante que la sacarosa.
-Ca vejiga = sacarina (ratas) NO AUMENTA EL REQUERIMIENTO DE INSULINA
 NO AUMENTA EL REQUERIMIENTO DE INSULINA.")
55
Información de la Food and Drug Administration (FDA, por sus siglas en inglés), instancia oficial que prohibió el ciclamato de sodio en EU señala que la sustancia puede causar cáncer y también se ha estudiado su relación con casos de esterilidad entre sus consumidores.
, instancia oficial que prohibió el ciclamato de sodio en EU señala que la sustancia puede causar cáncer y también se ha estudiado su relación con casos de esterilidad entre sus consumidores.")
56
EDULCORANTES ASPARTAME (Coca Cola, 0 calorias)
Compuesto x 2 aa: L-aspartato y derivado de fenilalanina. 190 v + dulce que glucosa. 20 mg endulzan = 1 tsp de azucar. - Se pierde la capacidad edulcorante al ser calentado!. mg/d (max 2 g) = seguro
 = seguro.")
57
= o > eficacia q otros y < riesgo de hipoglicemia
Nuevas drogas: 1. Péptidos Agonistas de R glucagon-like 1 (GLP-1) (incretinas), produc x c. L de ID (Exenatide FDA 2005 y liraglutide.. Pero GI s.effects, pancreatitis e IM varias veces). 2. Inhibidores de Dipeptidil peptidasa (DPP-4) (Linagliptina,sitagliptin, saxagliptin) INCRETINAS: Too reducen el apetito y retardan el vaciado gástrico. Animales:Estimula prolif de c. B e inh su apoptosis Puede disminuir PA Mejora niveles de triglicer -Cardioprotectores -Bajan de peso -Retardan o detienen la progresion de la enf = o > eficacia q otros y < riesgo de hipoglicemia
 (incretinas), produc x c. L de ID (Exenatide FDA 2005 y liraglutide.. Pero GI s.effects, pancreatitis e IM varias veces). 2. Inhibidores de Dipeptidil peptidasa (DPP-4) (Linagliptina,sitagliptin, saxagliptin) INCRETINAS: Too reducen el apetito y. retardan el vaciado gástrico. Animales:Estimula prolif de. c. B e inh su apoptosis. Puede disminuir PA. Mejora niveles de triglicer. -Cardioprotectores. -Bajan de peso. -Retardan o detienen la. progresion de la enf. = o > eficacia q otros y. < riesgo de hipoglicemia.")
58
May2, 2011. The U.S. FDA today approved Trayenta (linagliptin) tablets, used with diet and exercise, to improve blood glucose control in adults with Type 2 diabetes. Trayenta increases the level of hormones that stimulate the release of insulin after a meal by blocking the enzyme dipeptidyl peptidase-4 or DPP-4 People with Type 2 diabetes do not produce or respond normally to insulin, a hormone that regulates the amount of glucose in the blood. Over time, high blood glucose levels can increase the risk for serious complications, including heart disease, blindness, and nerve and kidney damage. Tradjenta has been studied as a stand-alone therapy and in combination with other Type 2 diabetes therapies including metformin, glimepiride, and pioglitazone. Tradjenta has not been studied in combination with insulin, and should not be used to treat people with Type 1 diabetes or in those who have increased ketones in their blood or urine (diabetic ketoacidosis). The most common side effects of Trayenta are upper respiratory infection, stuffy or runny nose, sore throat, muscle pain, and headache.
 tablets, used with diet and exercise, to improve blood glucose control in adults with Type 2 diabetes. Trayenta increases the level of hormones that stimulate the release of insulin after a meal by blocking the enzyme dipeptidyl peptidase-4 or DPP-4. People with Type 2 diabetes do not produce or respond normally to insulin, a hormone that regulates the amount of glucose in the blood. Over time, high blood glucose levels can increase the risk for serious complications, including heart disease, blindness, and nerve and kidney damage. Tradjenta has been studied as a stand-alone therapy and in combination with other Type 2 diabetes therapies including metformin, glimepiride, and pioglitazone. Tradjenta has not been studied in combination with insulin, and should not be used to treat people with Type 1 diabetes or in those who have increased ketones in their blood or urine (diabetic ketoacidosis). The most common side effects of Trayenta are upper respiratory infection, stuffy or runny nose, sore throat, muscle pain, and headache.")
59
NEWS Reports of pancreatitis are times more likely with GLP-1 drugs, analysis finds BMJ 2013;346:f2607 A class of antidiabetes drugs is associated with an increase in safety alerts for pancreatitis and pancreatic cancer, a new analysis has found. The Institute for Safe Medication Practices, a US non-profit organisation that promotes the safe use of drugs, monitored reports of serious adverse events to the US Food and Drug Administration from 1 July 2011 to 30 June 2012 concerning five glucagon-like peptide-1 (GLP-1) based agents (exenatide, liraglutide, sitagliptin, saxagliptin, and linagliptin) used to lower blood glucose concentrations. It compared these against the rates of adverse event reporting for a control group of drugs comprising other drugs used to treat type 2 diabetes (three sulfonylureas and metformin) and drugs for treating other diseases. GLP-1 is one of the many hormones involved in the complex process of regulating blood glucose concentrations, and the drugs that modify the circulating GLP-1 concentration do so in one of two ways. Exenatide and liraglutide are analogues of GLP-1 itself and are taken by injection. Sitagliptin, saxagliptin, and linagliptin are oral agents that prevent the rapid breakdown of GLP-1 by inhibiting the enzyme dipeptidylpeptidase-4.
 based agents (exenatide, liraglutide, sitagliptin, saxagliptin, and linagliptin) used to lower blood glucose concentrations. It compared these against the rates of adverse event reporting for a control group of drugs comprising other drugs used to treat type 2 diabetes (three sulfonylureas and metformin) and drugs for treating other diseases. GLP-1 is one of the many hormones involved in the complex process of regulating blood glucose concentrations, and the drugs that modify the circulating GLP-1 concentration do so in one of two ways. Exenatide and liraglutide are analogues of GLP-1 itself and are taken by injection. Sitagliptin, saxagliptin, and linagliptin are oral agents that prevent the rapid breakdown of GLP-1 by inhibiting the enzyme dipeptidylpeptidase-4.")
60
EDITORIAL N Engl J Med 2011; 365:2030-2031
Obesity Treatment in Primary Care — Are We There Yet?. Susan Z. Yanovski, M.D. The U.S. Preventive Services Task Force recommends that clinicians arrange for their obese patients to receive intensive, multicomponent behavioral weight-loss counseling.1 However, less than 50% of primary care physicians (PCPs) report that they consistently provide diet and weight-control advice to their adult patients with weight-related disease, and less than 25% regularly refer patients for further management or track their weight-control behaviors over time.2 Recognizing the need for effective weight-management treatments that can be implemented in the primary care setting, the National Heart, Lung, and Blood Institute funded the Practice-based Opportunities for Weight Reduction consortium,3 a group of independent but coordinated comparative-effectiveness trials of weight-loss interventions delivered in primary care settings to obese patients with cardiovascular risk factors. The primary outcome was weight change at 2 years. In this issue of the Journal, the results of two of these studies4,5 are presented. In the study by Wadden et al.,4 usual care (counseling provided at quarterly PCP office visits) was compared with the addition of brief lifestyle counseling (monthly, 15-minute, in-person counseling visits by trained medical assistants) and with enhanced lifestyle counseling (brief lifestyle counseling plus a toolbox that included meal replacements and weight-loss medications). Although weight loss in the brief-lifestyle-counseling group (2.9 kg) and the usual-care group (1.7 kg) did not differ significantly at 2 years, participants in the enhanced-lifestyle-counseling group lost significantly more weight (4.6 kg) than did those in either of the other two groups and were more likely to lose at least 5% of their initial body weight (35% in the enhanced-lifestyle-counseling group, vs. 26% in the brief-lifestyle-counseling group and 22% in the usual-care group). In the study by Appel et al.,5 participants from six primary care practices were randomly assigned to a self-directed weight-loss program (control group); to in-person individual sessions plus group sessions, along with electronic and telephone contacts delivered by office-based lifestyle coaches (in-person support); or to a commercial call center–directed group in which coaches delivered all lifestyle interventions by telephone, Internet, and (remote support). Physicians supported the delivery of the interventions, reviewed participants' weight status, and at routine medical visits encouraged participants to be engaged with the weight-loss treatment. Weight loss at 2 years was similar in the groups that received in-person support (5.1 kg) and remote support (4.5 kg) and was significantly greater than the weight loss in the control group (0.8 kg). Participants assigned to either the in-person or the remote lifestyle intervention were twice as likely as those assigned to the control group to have lost 5% or more of their initial body weight at 2 years (41% for the in-person group and 38% for the remote group, vs. 19% for the control group).
 report that they consistently provide diet and weight-control advice to their adult patients with weight-related disease, and less than 25% regularly refer patients for further management or track their weight-control behaviors over time.2. Recognizing the need for effective weight-management treatments that can be implemented in the primary care setting, the National Heart, Lung, and Blood Institute funded the Practice-based Opportunities for Weight Reduction consortium,3 a group of independent but coordinated comparative-effectiveness trials of weight-loss interventions delivered in primary care settings to obese patients with cardiovascular risk factors. The primary outcome was weight change at 2 years. In this issue of the Journal, the results of two of these studies4,5 are presented. In the study by Wadden et al.,4 usual care (counseling provided at quarterly PCP office visits) was compared with the addition of brief lifestyle counseling (monthly, 15-minute, in-person counseling visits by trained medical assistants) and with enhanced lifestyle counseling (brief lifestyle counseling plus a toolbox that included meal replacements and weight-loss medications). Although weight loss in the brief-lifestyle-counseling group (2.9 kg) and the usual-care group (1.7 kg) did not differ significantly at 2 years, participants in the enhanced-lifestyle-counseling group lost significantly more weight (4.6 kg) than did those in either of the other two groups and were more likely to lose at least 5% of their initial body weight (35% in the enhanced-lifestyle-counseling group, vs. 26% in the brief-lifestyle-counseling group and 22% in the usual-care group). In the study by Appel et al.,5 participants from six primary care practices were randomly assigned to a self-directed weight-loss program (control group); to in-person individual sessions plus group sessions, along with electronic and telephone contacts delivered by office-based lifestyle coaches (in-person support); or to a commercial call center–directed group in which coaches delivered all lifestyle interventions by telephone, Internet, and (remote support). Physicians supported the delivery of the interventions, reviewed participants weight status, and at routine medical visits encouraged participants to be engaged with the weight-loss treatment. Weight loss at 2 years was similar in the groups that received in-person support (5.1 kg) and remote support (4.5 kg) and was significantly greater than the weight loss in the control group (0.8 kg). Participants assigned to either the in-person or the remote lifestyle intervention were twice as likely as those assigned to the control group to have lost 5% or more of their initial body weight at 2 years (41% for the in-person group and 38% for the remote group, vs. 19% for the control group).")
61
A well-recognized issue that affects the sustainability of behavioral interventions is that attendance at face-to-face counseling sessions decreases substantially over time. In the study by Wadden et al., participants in both the brief-lifestyle-counseling and the enhanced-lifestyle-counseling groups attended fewer than half the scheduled counseling visits during year 2. Similarly, in the study by Appel et al., those assigned to the in-person group participated in only 2 of 24 recommended face-to-face individual and group sessions between month 7 and the end of the trial. In contrast, those assigned to the remote group participated in a median of 16 of 18 recommended telephone contacts during that time. Given that remotely delivered coaching resulted in weight-loss outcomes similar to those of in-person visits, the use of mobile technologies to deliver behavioral weight-loss treatment in primary care appears to be promising. Such interventions may present fewer barriers to adherence than interventions delivered in person, since they allow for greater scheduling flexibility, decreased travel time, and lower transportation costs. In addition, a telephone-based coaching program has the potential for widespread implementation in multiple practice settings, including geographically isolated areas. Both these studies provide evidence that PCPs can deliver safe and effective weight-loss interventions in primary care settings. However, there are important caveats. Although described as “effectiveness” rather than “efficacy” studies, both studies provided treatments (including lifestyle coaching, counseling, and, in the case of the Wadden study, meal replacements and medications) at no cost to the participants. Whether patients would be willing to pay for these therapies, or insurers would be willing to reimburse for them, is not known. Determining the costs and cost-effectiveness of these and other treatments in primary care settings is crucial. In addition, these two studies were not powered to detect differences in cardiovascular risk reduction, and there were no consistent between-group differences with respect to lipid levels, glucose levels, or blood pressure at 2 years. Particularly when one is augmenting behavioral treatments with medication, it is critical to assess the impact of such interventions on obesity-related coexisting conditions. Finally, although more than one third of patients may respond to lifestyle counseling with weight loss of at least 5% of their baseline weight, many obese persons do not successfully achieve or maintain weight losses sufficient to improve their health by means of lifestyle changes alone. Some patients will require additional treatments (e.g., medications or bariatric surgery) as an adjunct to, but not a replacement for, lifestyle interventions. Continued research on ways to enhance patients' adherence to long-term lifestyle changes should improve the reach and effectiveness of behavioral treatments for obesity in primary care settings. The opinions expressed herein are those of the author and do not necessarily reflect the views of the National Institutes of Health or the Department of Health and Human Services.
 at no cost to the participants. Whether patients would be willing to pay for these therapies, or insurers would be willing to reimburse for them, is not known. Determining the costs and cost-effectiveness of these and other treatments in primary care settings is crucial. In addition, these two studies were not powered to detect differences in cardiovascular risk reduction, and there were no consistent between-group differences with respect to lipid levels, glucose levels, or blood pressure at 2 years. Particularly when one is augmenting behavioral treatments with medication, it is critical to assess the impact of such interventions on obesity-related coexisting conditions. Finally, although more than one third of patients may respond to lifestyle counseling with weight loss of at least 5% of their baseline weight, many obese persons do not successfully achieve or maintain weight losses sufficient to improve their health by means of lifestyle changes alone. Some patients will require additional treatments (e.g., medications or bariatric surgery) as an adjunct to, but not a replacement for, lifestyle interventions. Continued research on ways to enhance patients adherence to long-term lifestyle changes should improve the reach and effectiveness of behavioral treatments for obesity in primary care settings. The opinions expressed herein are those of the author and do not necessarily reflect the views of the National Institutes of Health or the Department of Health and Human Services.")
62
EEUU aprueba un nuevo medicamento para controlar la obesidad
Actualizado miércoles 18/07/2012 10:24 horas FDA ha autorizado un nuevo fármaco para ayudar a pacientes obesos a perder peso. Qsymia se convierte así en el segundo tratamiento autorizado con este fin en pocas semanas, después de que las autoridades de EEUU diesen luz verde a Belviq, el primer tratamiento antiobesidad desde 1999. La nueva píldora, fabricada por Vivus Inc., está pensada para pacientes adultos con un índice de masa corporal de al menos 30; o de al menos 27 y que además padezcan hipertensión, diabetes 2 o altos niveles de colesterol, ha señalado la FDA en un comunicado. La obesidad es una "gran preocupación de salud pública" en EEUU y Qsymia, siempre utilizada en combinación con ejercicios y una dieta baja en calorías "ofrece otra opción de tratamiento para el manejo del peso crónico", ha declarado Janet Woodcock, directora del centro que investiga y evalúa los nuevos fármacos en la FDA. El índice de masa corporal (BMI) mide la grasa corporal en base al peso y estatura de la persona, y los médicos lo utilizan para definir el problema de obesidad o sobrepeso en los pacientes. Según los Centros para el Control y Prevención de Enfermedades (CDC, en inglés), más de una tercera parte de los adultos en EEUU son considerados obesos. La obesidad ha sido vinculada con una extensa serie de problemas médicos. Qsymia es una combinación de dos fármacos: la fentermina, que suprime el apetito, y el topiramato, un anticonvulsivo de acción prolongada que causa una sensación de saciedad y que normalmente se receta para las migrañas y para controlar la epilepsia. La FDA evaluó la eficacia y seguridad de Qsymia mediante dos pruebas realizadas durante un año entre cerca de obesos y personas con sobrepeso, con o sin problemas de salud relacionados con el peso. Los pacientes que recibieron la dosis recomendada de 7,5 miligramos de fentermina y 46 de topiramato perdieron en promedio 6,7% de su peso corporal. Mientras, los que recibieron una dosis más alta de 15 miligramos de fentermina y 92 de topiramato, perdieron en promedio 8,9% de su peso total, explicó la FDA. Las autoridades de la FDA advirtieron de que la Qsymia no debe usarse durante el embarazo porque puede causar daños al feto, y recomendó que las mujeres en edad reproductiva utilicen algún método anticonceptivo mientras estén bajo tratamiento. La FDA aprobó en junio pasado la píldora Belviq también para ayudar a bajar de peso, el primer medicamento aprobado por el Gobierno de EEUU con esos fines desde 1999. Antes de la aprobación Belviq, sólo un fármaco antiobesidad había sido aprobado para su uso a largo plazo -'Xenical' de Roche, que se utilizó muy poco debido a una pérdida de peso modesta y a sus efectos desagradables en el sistema digestivo-. Durante estos años, y por su mercado potencial, muchos han sido los intentos de colocar en el mercado píldoras para la dieta, pero la gran mayoría presentaba diversos problemas de seguridad, como en el caso de Orlistat, lo que llevó a la FDA a ser renuentes con la aprobación de este tipo de medicamentos.
 mide la grasa corporal en base al peso y estatura de la persona, y los médicos lo utilizan para definir el problema de obesidad o sobrepeso en los pacientes. Según los Centros para el Control y Prevención de Enfermedades (CDC, en inglés), más de una tercera parte de los adultos en EEUU son considerados obesos. La obesidad ha sido vinculada con una extensa serie de problemas médicos. Qsymia es una combinación de dos fármacos: la fentermina, que suprime el apetito, y el topiramato, un anticonvulsivo de acción prolongada que causa una sensación de saciedad y que normalmente se receta para las migrañas y para controlar la epilepsia. La FDA evaluó la eficacia y seguridad de Qsymia mediante dos pruebas realizadas durante un año entre cerca de obesos y personas con sobrepeso, con o sin problemas de salud relacionados con el peso. Los pacientes que recibieron la dosis recomendada de 7,5 miligramos de fentermina y 46 de topiramato perdieron en promedio 6,7% de su peso corporal. Mientras, los que recibieron una dosis más alta de 15 miligramos de fentermina y 92 de topiramato, perdieron en promedio 8,9% de su peso total, explicó la FDA. Las autoridades de la FDA advirtieron de que la Qsymia no debe usarse durante el embarazo porque puede causar daños al feto, y recomendó que las mujeres en edad reproductiva utilicen algún método anticonceptivo mientras estén bajo tratamiento. La FDA aprobó en junio pasado la píldora Belviq también para ayudar a bajar de peso, el primer medicamento aprobado por el Gobierno de EEUU con esos fines desde Antes de la aprobación Belviq, sólo un fármaco antiobesidad había sido aprobado para su uso a largo plazo - Xenical de Roche, que se utilizó muy poco debido a una pérdida de peso modesta y a sus efectos desagradables en el sistema digestivo-. Durante estos años, y por su mercado potencial, muchos han sido los intentos de colocar en el mercado píldoras para la dieta, pero la gran mayoría presentaba diversos problemas de seguridad, como en el caso de Orlistat, lo que llevó a la FDA a ser renuentes con la aprobación de este tipo de medicamentos.")
63
EEUU aprueba el primer fármaco antiobesidad en 13 años
Precisamente Belviq también sufrió el rechazo de esta agencia en Por aquel entonces, los animales a los que habían sometido a estas pastillas desarrollaron diferentes tumores y cundió la preocupación. Sin embargo, lejos de desanimarse, Arena Farmacéutica volvió a presentar su fármaco apoyado en nuevos datos que consiguieron aliviar las preocupaciones de la Agencia de Seguridad. Una ayuda modesta para adelgazar Sin embargo, Belviq tampoco se presenta como la gran ayuda para perder peso. En los dos ensayos clínicos principales en los que se basa, los que tomaron el medicamento perdieron un promedio de 5,8% de su peso después de un año, mientras que los que tomaron un placebo perdieron un 2,5%. ¿Y cómo actúa? Dos veces al día, Belviq activa un receptor en el cerebro, la serotonina 2C, de manera que bloquea las señales de apetito en el cerebro, haciendo que los pacientes se sientan llenos con pequeñas cantidades de comida. Algunos defensores de los pacientes y los médicos que tratan la obesidad dicen que hay una fuerte necesidad de nuevos medicamentos para ayudar "a llenar la brecha existente entre la dieta y el ejercicio para que el paciente no se desanime" y en un intento para paliar un problema, el de la obesidad, cada vez más extendido y capaz de causar problemas de corazón y diabetes. "La obesidad amenaza el bienestar general de los pacientes y es un importante problema de salud pública", dijo la doctora Janet Woodcock, directora del centro de evaluación de medicamentos de la FDA, en un comunicado, "de ahí que se necesiten nuevos métodos que ayuden a adelgazar". Arena Farmacéutica dijo que aunque todavía no tenían una fecha concreta de comercialización, la idea es que para el año que viene ya se venda. Efectos secundarios Aunque está indicado en general para el uso de aquellos adultos que tengan un índice de masa corporal de 30 o mayor, la FDA también ha puesto sus límites. Así, no se aconseja su ingesta a las mujeres embarazadas o en periodo de lactancia y como efectos secundarios se indican la depresión, los lapsus de memoria y las migrañas. Pero la principal preocupación es que Belviq pueda funcionar de forma similar a la fenfluramina, un fármaco que fue parte de la popular combinación fen-phen, y que fue retirado al comprobar que dañaba las válvulas del corazón. Aunque la Agencia estadounidense ya ha asegurado que cree poco probable que Belviq dé estos problemas, recomienda que la gente deje de tomar el medicamento si no se pierde un 5% de peso en 12 semanas, debido a que no son susceptibles de beneficiarse y no debe ser expuesto a los riesgos. De todas formas, la farmacéutica se ha comprometido a llevar a cabo seis estudios después del medicamento una vez que se comercialice para determinar si el fármaco aumenta el riesgo de ataques cardíacos y accidentes cerebrovasculares.

Presentaciones similares


















 developed ischemia with exercise. During a mean follow-up of 4.5 3.4 years, 313 patients died, and 183 patients had.>")

