Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Síndrome de QT Prolongado
Dra. Laura Sanziani Hospital Italiano – Sanatorio Los Arroyos

2
SQTL: Historia 1957: 1er reporte SQTL 1963-1964: Síndrome Romano-Ward
: 25 casos de SQTL reportados 1971: 1er Tto SQTL (Estelectomía izquierda) 1979: Comenzó el Registro de SQTL : + 10 genes responsables identificados Jervell and Lange-Nielsen provided the first documented description of this syndrome in They described a family with 4 deaf children with QT prolongation and syncope. 3 of the children died suddenly. The parents, and 2 other children had normal ECGs and normal hearing. This report was critical to the development of current knowledge regarding LQTS. Romano in 1963, and Ward in 1964 separately reported patients who were not deaf, but had an almost identical cardiac disorder. Later called the “Romano-Ward syndrome,” this disorder was realized to be much more common than the “Jervell-Lange-Nielsen syndrome.” The genetic transmission was thought to be autosomal dominant. Between 1958 and 1970, there are only 25 cases of LQTS reported. In 1971, Moss and McDonald performed the first successful therapy for LQTS in a patient who had not responded to any other antiarrhythmic therapy: left cardiac sympathetic denervation to shorten the QT interval. In 1979,Drs. Moss, Schwartz, and Crampton started the International Registry for LQTS, with headquarters in Rochester, NY. Between 1991 and 2001, a total of 6 LQTS genes were identified, 3 of which were reported between March 1995 and January 1996.
 1979: Comenzó el Registro de SQTL : + 10 genes responsables identificados. Jervell and Lange-Nielsen provided the first documented description of this syndrome in They described a family with 4 deaf children with QT prolongation and syncope. 3 of the children died suddenly. The parents, and 2 other children had normal ECGs and normal hearing. This report was critical to the development of current knowledge regarding LQTS. Romano in 1963, and Ward in 1964 separately reported patients who were not deaf, but had an almost identical cardiac disorder. Later called the Romano-Ward syndrome, this disorder was realized to be much more common than the Jervell-Lange-Nielsen syndrome. The genetic transmission was thought to be autosomal dominant. Between 1958 and 1970, there are only 25 cases of LQTS reported. In 1971, Moss and McDonald performed the first successful therapy for LQTS in a patient who had not responded to any other antiarrhythmic therapy: left cardiac sympathetic denervation to shorten the QT interval. In 1979,Drs. Moss, Schwartz, and Crampton started the International Registry for LQTS, with headquarters in Rochester, NY. Between 1991 and 2001, a total of 6 LQTS genes were identified, 3 of which were reported between March 1995 and January")
3
LQTS Congénito - Romano-Ward (RW) - Jervell-Lange-Nielsen (JLN)
- Esporádico Adquirido

4
LQTS Congénito: Fenotipia - Romano-Ward (RW)
- Jervell-Lange-Nielsen (JLN) - Esporádico
 - Esporádico.")
5
QT largo Congénito Sme. RW
Autosómica dominante Audición normal Más frecuente de los QTL hereditarios

6
QT Largo Congénito Sme de JLN
Autosómico recesivo Asocia sordera neurosensorial 1.6 a 6 casos/millón de habitantes

7
QTL Congénito Formas esporádicas
10 al 15 % de los casos Audición normal Carácter hereditario no identificado Pentrancia incompleta???

8
SQTL: Aspectos clínicos
Signos y Síntomas: Síncope Convulsiones MS Palpitaciones o dolor precordial Symptoms include: The presence of palpitations or children may describe as “chest pain” Recurrent syncope Seizures SCD can occur if the symptoms are ignored ECG signs include: QTc abnormal or borderline Evidence of Torsade de pointes is also common Patients at higher risk are those with deafness, female, syncope, and documented torsades or VF.

9
Sme QT Prolongado Características ECG
Intervalo QT Morfología de la onda T Alternancia de la onda T Pausas/Bradicardia Sinusal T de P

10
QT Prolongado

11
SQTL: Patrones en ECG Circ 1992;85[Suppl I]:I140-I144
Although the long QT syndrome often presents as unexplained syncope, the ECG is the definitive factor in differential diagnosis of the syndrome. This slide displays examples of delayed repolarization patterns observed in lead II of the ECG in patients with long QT syndrome. (Reproduced with permission from Moss AJ: Clinical features of idiopathic long QT syndrome. Circulation 1992;85[Suppl I]:I140-I144.) Circ 1992;85[Suppl I]:I140-I144
![SQTL: Patrones en ECG Circ 1992;85[Suppl I]:I140-I144](http://slideplayer.es/slide/3123007/11/images/11/SQTL%3A+Patrones+en+ECG+Circ+1992%3B85%5BSuppl+I%5D%3AI140-I144.jpg "Although the long QT syndrome often presents as unexplained syncope, the ECG is the definitive factor in differential diagnosis of the syndrome. This slide displays examples of delayed repolarization patterns observed in lead II of the ECG in patients with long QT syndrome. (Reproduced with permission from Moss AJ: Clinical features of idiopathic long QT syndrome. Circulation 1992;85[Suppl I]:I140-I144.) Circ 1992;85[Suppl I]:I140-I144.")
12
QT Largo: patrones en ECG
Additional examples of delayed repolarization patterns observed in lead II of the ECG in patients with long QT syndrome. (Reproduced with permission from Moss AJ: Clinical features of idiopathic long QT syndrome. Circulation 1992;85[Suppl I]:I140-I144.) Circ 1992;85[Suppl I]:I140-I144
 Circ 1992;85[Suppl I]:I140-I144.")
13
Intervalo QT Prolongado

14
QT Largo: Diagnóstico No olvidar:
* 10% de los portadores asintomáticos tienen QT normal * 15% de la población normal tiene un QT entre 450 y 470 miliseg.

15
Sme QT Prolongado Características ECG
Intervalo QT Morfología de la onda T Alternancia de la onda T Pausas/Bradicardia Sinusal

16
Morfología de la onda T en los diferentes genotipos de SQTL
Moss AJ, et al. Circulation 1995;92:

17
Bases del Sme de QT prolongado
Major currents underlying the ventricular action potential. As shown on the lower left, interventions that decrease outward currently (primarily through K+ channels), or increase inward current (through Na+ or Ca2+ channels) during the plateau, delay repolarization at the level of the ECG and individual action potentials, and prolong QT interval (upper left). The generic action potential on the right shows the major currents flowing during the cardiac cycle. The five LQTS genes and the currents they underlie are shown in bold. (Reprinted with permission from the authors and the Journal of Cardiac Electrophysiology. 1999;10: ). JCE 1999;10:
, or increase inward current (through Na+ or Ca2+ channels) during the plateau, delay repolarization at the level of the ECG and individual action potentials, and prolong QT interval (upper left). The generic action potential on the right shows the major currents flowing during the cardiac cycle. The five LQTS genes and the currents they underlie are shown in bold. (Reprinted with permission from the authors and the Journal of Cardiac Electrophysiology. 1999;10: ). JCE 1999;10:")
18
TAQUICARCIAS VENTRICULARES POLIMORFAS
QT LARGO CONGÉNITO LQT1 cromosoma 11 gen KCNQ1 LQT2 cromosoma 7 gen HERG LQT3 cromosoma 3 gen SCN5A

19
QT LARGO CONGÉNITO: Genotipia

20
QT LARGO CONGÉNITO: Genotipia
Sme. JLN

21
LQTS: Consideraciones genotipo-fenotipo
10 genotipos; ~300 mutaciones diferentes Diferencias clínicas entre LQT1, LQT2, & LQT3 Variabilidad Clínica dentro de un mismo genotipo Variabilidad Clínica entre miembros de una familia con la misma mutación genética sugiere la presencia de genes moduladores Researchers have already identified 6 genes that are affected, with more than 200 mutations identified to date. (By analogy, contrast this to cystic fibrosis, in which only 1 gene is thought to be responsible, with more than 800 different mutations). Many more mutations could still be unidentified. Even individuals in the same family, with the same gene and the same mutation, can have significant variations in severity. This provides support to the theory that there are modifying factors, which as of yet are undefined.
. Many more mutations could still be unidentified. Even individuals in the same family, with the same gene and the same mutation, can have significant variations in severity. This provides support to the theory that there are modifying factors, which as of yet are undefined.")
22
Gatillos para síncope o MSC
3 factores principales que contribuyen a síncope o MSC Ejercicio (LQT1), especialmente natación Emociones, stress emocional, estímulos acústicos (LQT2) Evento durante el sueño o reposo, (LQT2 o LQT3) Exercise is a source of physical stress, that induces an increase in heart rate and a release of catecholamines. Research has shown that swimming is a gene-specific trigger for cardiac events in LQTS. Emotional stress can include fear, anger, stressful events or arousals during normal daily activities, or arousal due to a noise or startling during sleep. Events during sleep are difficult to document. Events here would not include those triggered by arousal (startling or noise). These are most likely related to a decrease in heart rate. Exercise is the most common triggering event in LQT1. Emotions or emotional stress are the most common trigger in LQT2, and events occurring during sleep are more common in LQT2 or LQT3. Circ 2001;103:89-95 Mayo Clin Proc. 1999;74:
, especialmente natación. Emociones, stress emocional, estímulos acústicos (LQT2) Evento durante el sueño o reposo, (LQT2 o LQT3) Exercise is a source of physical stress, that induces an increase in heart rate and a release of catecholamines. Research has shown that swimming is a gene-specific trigger for cardiac events in LQTS. Emotional stress can include fear, anger, stressful events or arousals during normal daily activities, or arousal due to a noise or startling during sleep. Events during sleep are difficult to document. Events here would not include those triggered by arousal (startling or noise). These are most likely related to a decrease in heart rate. Exercise is the most common triggering event in LQT1. Emotions or emotional stress are the most common trigger in LQT2, and events occurring during sleep are more common in LQT2 or LQT3. Circ 2001;103:89-95 Mayo Clin Proc. 1999;74:")
23
Relación gen : gatillo específico
Porcentaje This study identified patients of a known genotype, who had experienced significant cardiac events. Triggers for cardiac events according to 3 genotypes: percentage of patients in each genotype, and the pattern of triggers within each genotype. (Schwartz, et al. Circulation. 2001;103:89-95). In the LQT1 variant, exercise is a trigger for >60%, while barely 3% are triggered while at rest. In the LQT2 variant, a significant number of events occur due to emotional stress or while at rest, while exercise is a trigger in only 13%. In LQT3, the majority of events appear to occur during sleep or at rest. LQT1 is the only variant that has a high percentage of events occurring during exercise, and thus is very different from LQT2 or LQT3. LQT1 patients would be advised not to participate in competitive athletic activities. Circ 2001;103:89-95
. In the LQT1 variant, exercise is a trigger for >60%, while barely 3% are triggered while at rest. In the LQT2 variant, a significant number of events occur due to emotional stress or while at rest, while exercise is a trigger in only 13%. In LQT3, the majority of events appear to occur during sleep or at rest. LQT1 is the only variant that has a high percentage of events occurring during exercise, and thus is very different from LQT2 or LQT3. LQT1 patients would be advised not to participate in competitive athletic activities. Circ 2001;103:")
24
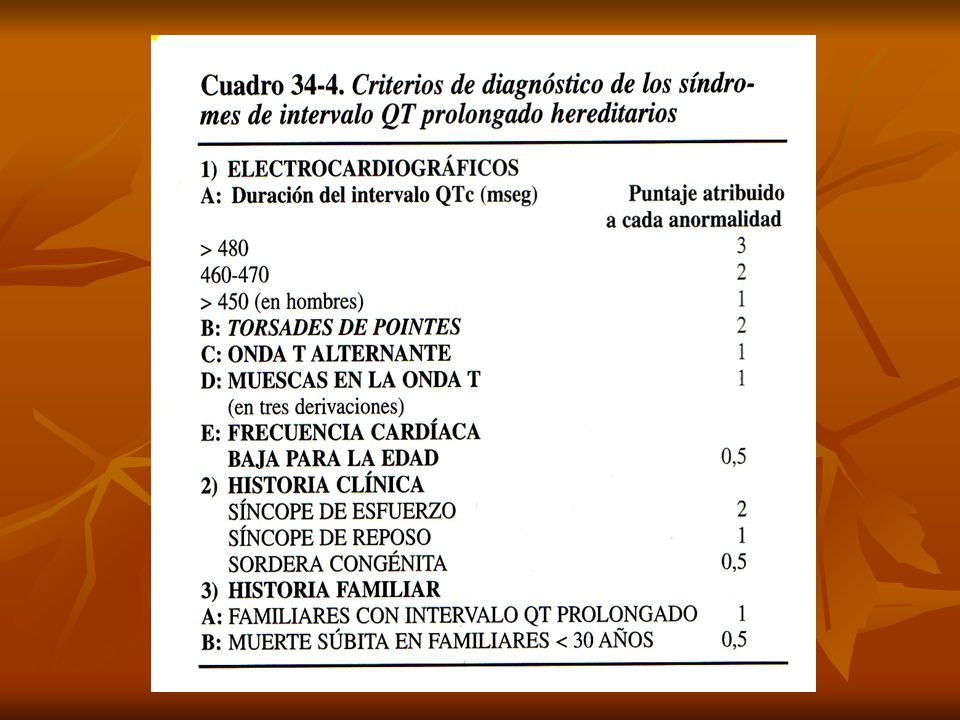
SQTL: Criterios diagnósticos
Hallazgos ECG: QTc, TdP, muescas en onda T, baja FC para la edad. HC: Síncope, convulsiones, PC abortado. Historia familiar: miembros con QT largo, MS inexplicada en familiares directos a una edad < 55 años. The 3 major components of information needed are: A detailed ECG A thorough clinical history, including onset, frequency and predisposing factors of the syncopal episodes A thorough family history Circ 1993;88:

26
Intervalo QTc y riesgo The risk increases significantly with increased QTc above 440ms.

27
Intervalo QTc y riesgo Risk for Cardiac Event QTc AJC 1993;72:21B
The risk increases significantly with increased QTc above 440ms. QTc AJC 1993;72:21B

28
Probabilidad de eventos cardíacos
Note that the peak incidence for cardiac events is from birth through adolescence for LQT1 and LQT2, with the peak incidence occurring later in LQT3. In all 3 genotypes, males are at risk primarily through age 25, and females have a persistent risk up to age 40. No. de ptes. LQT LQT LQT NEJM 1998;339:

29
QTL: criterios de alto riesgo
Sordera congénita Síncope recurrente por TV AF de MS o PC resuscitado QT > 0.50 seg/0.60 seg. QTL 3

30
LQTS: quién está en riesgo de MS?
PC abortado Historia familiar de MS inexplicada Síncope Torsade de pointes Alternancia de la onda T QTc prolongado Highest risk patients are those who have already experienced a SCD event, those with recurrent syncope, those with ECG evidence of torsade de pointes, alternation of the T-wave, and those with significantly prolonged QT. Family history may include unexplained car accident, drowning, or other sudden death.

31
TAQUICARCIAS VENTRICULARES POLIMORFAS
ESTRATIFICACION Priori S, NEJM;

32
LQTS: Intentando hallar marcadores de riesgo
Niñez - Varones: *QTc > 500’’’ *Síncope previo - Mujeres: Circulation 2008-Apr 29;117(17): Post 40 (Se mantiene el riesgo de MS) - Mujeres - Síncope reciente (< 2 años) - LQT 3 Circulation 2008-Apr 29;117(17):
: Post 40 (Se mantiene el riesgo de MS) - Mujeres. - Síncope reciente (< 2 años) - LQT 3. Circulation 2008-Apr 29;117(17):")
33
LQTS Congénito - Romano-Ward (RW) - Jervel-Lange-Nilsen (JLN)
- Esporádico Adquirido

34
Causas de Torsades de Pointes secundarias

35
Gen mayor: Interacciones
Genes no mayores Canales Iónicos Genes no mayores Factores Estructurales Ambiente celular Genes no mayores Genes no mayores Red Intercelular

36
QT largo adquirido: T de P
Hipomagnesemia

37
Sme QT Largo Congénito Torsión de Puntas

38
SQTL: Terapias disponibles y manejo

39
SQT largo: Tto. preventivo
Prohibición de deporte competitivo Evitar drogas que prolonguen el QT Bloqueantes Beta MPD Resección ganglionar simpática (Estelectomía izquierda: ocasionalmente utilizada en niños y pacientes refractarios a otras formas de terapia). CDI QT 3???...Drogas Clase I?...BB?...
. CDI. QT 3 ...Drogas Clase I ...BB ...")
40
Probabilidad de eventos cardíacos
Estimated cumulative probability of experiencing syncope, aborted cardiac arrest, or LQTS-related death on prescribed ß-blockers in LQTS patients who were asymptomatic (dotted line) or symptomatic (solid line) before starting ß-blockers. LQTS patients who were symptomatic prior to ß-blocker therapy have a much higher probability of experiencing another cardiac event. More than 30% of patients who were symptomatic prior to ß-blocker therapy will have another cardiac event within 5 years. Circ 2000;101:
 or symptomatic (solid line) before starting ß-blockers. LQTS patients who were symptomatic prior to ß-blocker therapy have a much higher probability of experiencing another cardiac event. More than 30% of patients who were symptomatic prior to ß-blocker therapy will have another cardiac event within 5 years. Circ 2000;101:")
41
Uso de BB: probabilidad acumulativa de MS relacionada con SQTL
Estimated cumulative probability of experiencing aborted cardiac arrest or death on ß-blocker therapy in LQTS patients who were asymptomatic (dotted line), experienced syncope only (dashed line), or had a prior aborted cardiac arrest (solid line) before ß-blockers. Vertical lines are 95% Confidence Intervals. Risk curves are for LQTS patients started on ß-blockers at >10 years of age; the risk curves are higher for those started at a younger age. Time periods off therapy for more than 2 days are excluded. Patients with a prior aborted SCD should receive an ICD, as they have a higher probability of experiencing another cardiac arrest or LQTS-related death. Circ 2000;101:
, experienced syncope only (dashed line), or had a prior aborted cardiac arrest (solid line) before ß-blockers. Vertical lines are 95% Confidence Intervals. Risk curves are for LQTS patients started on ß-blockers at >10 years of age; the risk curves are higher for those started at a younger age. Time periods off therapy for more than 2 days are excluded. Patients with a prior aborted SCD should receive an ICD, as they have a higher probability of experiencing another cardiac arrest or LQTS-related death. Circ 2000;101:")
42
SQTL: Eventos cardíacos antes y después de BB
Probandos MFA† (n=581) (n=288) Riesgo (pre- y post- B) Pre-B Post- B Pre- B Post B Pts con eventos * * Numero eventos * * Eventos/pt * * Eventos/pt/año * * This slide outlines 869 patients from the International LQTS Registry who were treated with beta-blockers. The goal of this study was to evaluate the effectiveness of beta-blockers in LQTS patients. It also looked at specific risk factors for syncope and SCD for patients who were already on beta-blocker therapy. Both the number of patients with events and the number of events decreased significantly after the initiation of ß-blocker therapy. In addition this reduction in events was seen in both probands and affected family members. Circ 2000;101: * P<0.01 vs. pre--blocker
 (n=288) Riesgo (pre- y post- B) Pre-B Post- B Pre- B Post B. Pts con eventos * 92 49* Numero eventos * * Eventos/pt * * Eventos/pt/año * * This slide outlines 869 patients from the International LQTS Registry who were treated with beta-blockers. The goal of this study was to evaluate the effectiveness of beta-blockers in LQTS patients. It also looked at specific risk factors for syncope and SCD for patients who were already on beta-blocker therapy. Both the number of patients with events and the number of events decreased significantly after the initiation of ß-blocker therapy. In addition this reduction in events was seen in both probands and affected family members. Circ 2000;101: * P<0.01 vs. pre--blocker.")
43
CONGÉNITO TRATAMIENTO
QT LARGO CONGÉNITO TRATAMIENTO LQT1 19% recurrencia Paro o MS % LQT2 31 % recurrencia Paro o MS % LQT3 50% recurrencia Paro o MS % NADOLOL o PROPANOLOL (*) b-Bloqueantes
 b-Bloqueantes.")
44
Limitaciones de los BB en SQTL
MSC puede ocurrir a pesar de TTO con BB Es problemático el cumplimiento de una terapia diaria a largo plazo Efectos indeseables conocidos de los BB Although -blockers reduce the number of cardiac events, syncopal events and SCD can still occur. The challenge is to have the patient continue to take the drugs, even if they are feeling well. In addition, in young, active, healthy patients, the side effects can hamper their activity tolerance. In standard doses, up to 15% of patients will not tolerate beta-blockers due to side effects. Common side effects include asthma, fatigue, sleep disturbances.

45
SQTL: Experiencia con MPD
Reduce la frecuencia de síncope en pacientes con eventos gatillados por bradicardia Su mayor utilidad se demuestra al combinarse con terapia BB No previene la MSC en terapia a largo plazo Pareciera más útil en pacientes con LQT3 y bradicardia A retrospective study followed 37 patients with idiopathic LQTS who received both -blocker and pacing therapy, to determine the efficacy of combined therapy. After an average of years, 28 of 37 patients remained without symptoms on combined therapy. Recurrent pacemaker malfunction causing symptoms was experienced in 3 patients, 3 patients died, and 3 patients had resuscitated cardiac arrest. An additional patient died of unrelated causes. The overall incidence of sudden death and aborted sudden death was 24% in all patients and 17% in compliant patients. Conclusion: Even with combined therapy, these patients remained at significant risk for sudden death. Circ. 1999;100: Hoy perdiendo terreno…

46
SQTL: Experiencia con CDI
CDI indicado en todo SQTL que presentó FV o PC abortado Previene MSC en ptes. con eventos cardíacos previos Provee un back-up para pacientes en TTO con BB quienes continúan sintomáticos Published beta-blocker and pacemaker studies document continued cardiac events with single or combination therapy. ICDs can treat breakthrough tachyarrhythmias to prevent sudden cardiac death.

47
Manejo segun genotipo LQT1 y LQT2 se benefician ppalmente. Con BB
El beneficio de BB en LQT3 es menos claro. CDI indicado (IIa-B) Si el paciente se presenta como sobreviviente de MSC o PC abortado Si los BB fallaron en prevenir eventos cardíacos: síncope, TV, MSC. Because the sympathetic nervous system plays a role in LQT1 and LQT2, these 2 genotypes benefit the most from ß-blocker therapy. The role of ß-blocker therapy in LQT3 is less well-defined, as no clear benefit has been documented in these patients. Since LQT3 involves a Na+ channel defect, exercise provides the benefit of shortening the QTc interval.
 Si el paciente se presenta como sobreviviente de MSC o PC abortado. Si los BB fallaron en prevenir eventos cardíacos: síncope, TV, MSC. Because the sympathetic nervous system plays a role in LQT1 and LQT2, these 2 genotypes benefit the most from ß-blocker therapy. The role of ß-blocker therapy in LQT3 is less well-defined, as no clear benefit has been documented in these patients. Since LQT3 involves a Na+ channel defect, exercise provides the benefit of shortening the QTc interval.")
48
SQTL: Presente y futuro
LQTS Registry: identificación de factores de riesgo Identificación de nuevos genes Test de esfuerzo para Dx y estratificación de riesgo Genes moduladores Terapia específica para cada mutación The Long QT Registry continues to evaluate specific risk factors for LQTS-related cardiac events. There is potential to identify additional genes, gene mutations, and modifier genes due to the great variability in current presentation of the disease. The goal is to continue to try to develop gene- and mutation-specific therapy.

49
QT Largo: Identificación genética?
Restringida Costosa Aún genes/mutaciones no identificados Heterogeneidad fenotípica Resultados + (70%-75%)
")
50
QT Largo: T de P Dependiente de catecolaminas (QT hereditario o primario) Pausa dependiente (QT secundario o adquirido)
 Pausa dependiente (QT secundario o adquirido)")
51
Taquicardias irregulares – QRS ancho

52
Holter (continuación)
")
53
Paciente con QT largo y síncope: Registro Holter

54
Torsión de Puntas: Tto agudo
CVE Aumento de la FC * Estimulación * Isoproterenol * Atropina Sulfato de Magnesio (50%) Corrección de anormalidades MTB Supresión de drogas responsables
 Corrección de anormalidades MTB. Supresión de drogas responsables.")
55
SQTL: Información en la WEB
Cardiac Arrhythmias Research and Education (CARE) Foundation: Cardiac Arrest Survivors Network (CASN): International Registry for Drug-Induced Arrhythmias, including drugs to use with caution or avoid in Long QT patients:
 Foundation: Cardiac Arrest Survivors Network (CASN): International Registry for Drug-Induced Arrhythmias, including drugs to use with caution or avoid in Long QT patients:")
Presentaciones similares

>")

















