Descargar la presentación
La descarga está en progreso. Por favor, espere

1
TEMA 9.-CONSEJO GENÉTICO Y MEDICINA FETAL.
FÁRMACOS Y EMBARAZO

2
“To wrest from nature the secrets which have perplexed philosophers in all ages, to track to their sources the causes of diseases, to correlate the vast stores of knowledge, that they may be quickly avalaible for the prevention and cure of disease - these are our ambitions.” (William Osler, Montreal Medical Journal, 1902).
.")
5
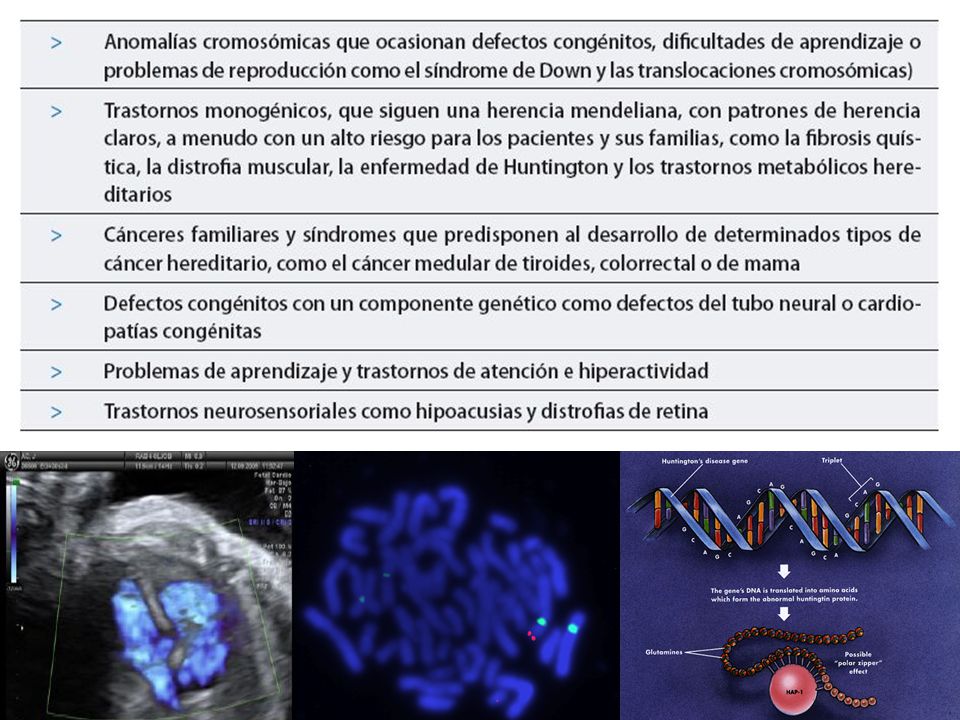
GENÉTICA Y SALUD El 8% de las personas es diagnosticado antes de los 25 años de una enfermedad que tiene un componente genético Enfermedades Monogénicas ,6/1000 Autosómicas dominantes ,4/1000 Autosómicas recesivas ,7/1000 Ligadas al X ,5/1000 Anomalias cromosómicas ,8/1000 Enfermedades Multifactoriales ,4/1000 Anomalías congénitas ,6/1000 Otras ,6/1000

6
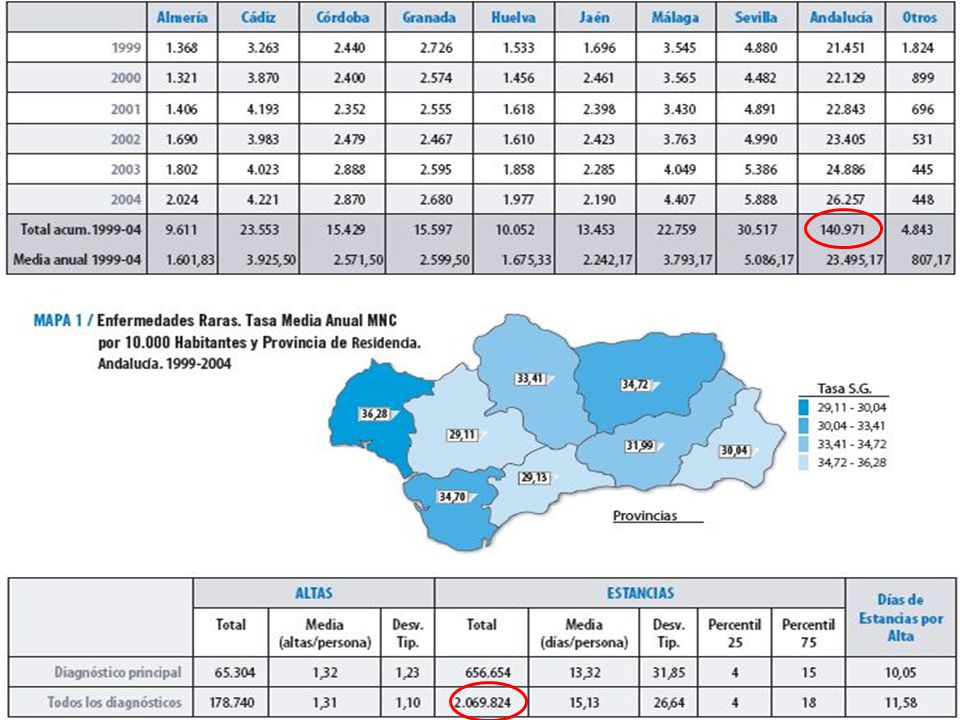
ENFERMEDAD RARA ES AQUELLA ENFERMEDAD CON UNA PREVALENCIA DE
1/1350 (NIH) 1/2000 (UE) ENTRE LAS ENFERMEDADES RARAS >> 80% PRESENTA UNA BASE GENÉTICA AFECTAN A DE PERSONAS EN LA UE
 1/2000 (UE) ENTRE LAS ENFERMEDADES RARAS >> 80% PRESENTA UNA BASE GENÉTICA. AFECTAN A DE PERSONAS EN LA UE.")
10
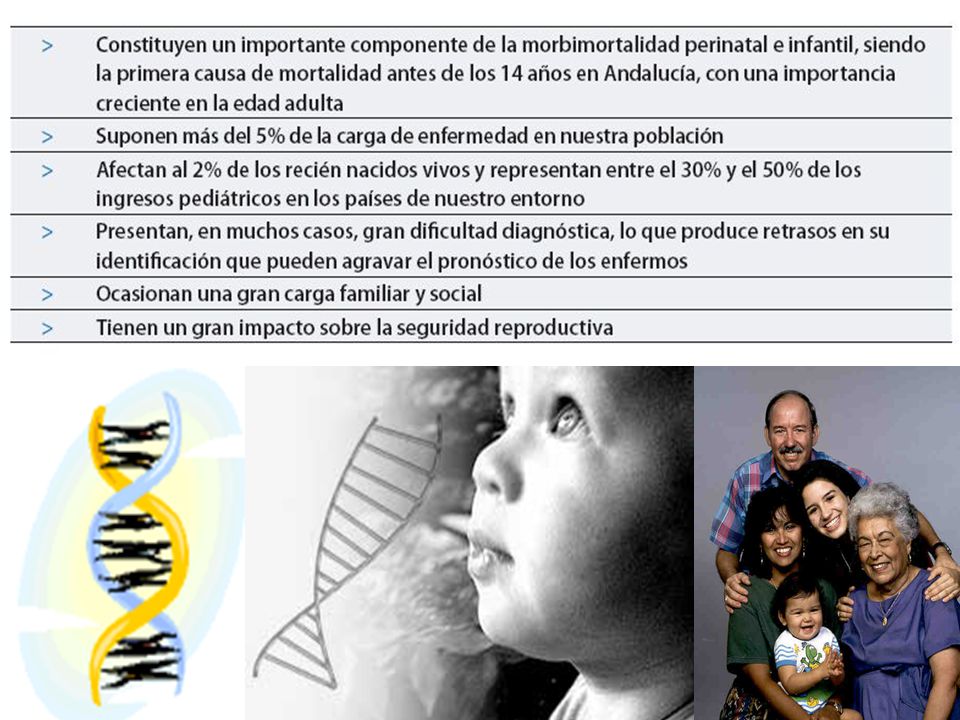
EFECTO DE LAS ENFERMEDADES DE BASE GENÉTICA
Esperanza de Vida Calidad de Vida Reproducción Adaptación Individual, Familiar y Social

11
Análisis Genéticos en Genética Clínica
Los análisis genéticos detectan cambios en la información genética relacionados con problemas de salud Los análisis genéticos pueden usarse tanto para el manejo médico de una enfermedad, como para la toma de decisiones personales. Los análisis genéticos pueden afectar no sólo al paciente, también a sus familias. Los análisis genéticos se deben realizar en un contexto que incluya Consejo Genético, y deben incluir Consentimiento Informado e interpretación de los resultados.

12
Tipos de Análisis Genéticos
Análisis Diagnóstico o Sintomático -vs- Análisis Predictivo / Presintomático Análisis Clínico vs Análisis de Investigación

13
CONSEJO GENÉTICO El Consejo Genético es un proceso de comunicación orientado a manejar los problemas asociados a la aparición, o el riesgo de aparición, de un trastorno de base genética en un individuo o una familia.

14
¿Cual es mi riesgo de desarrollar …?

15
LA PRACTICA CLÍNICA EN EL CONSEJO GENÉTICO
Valoración Clínica Arbol Familiar Sospecha Diagnóstica Diagnóstico Riesgo de recurrencia Posibilidades de Prevención EXPRESIVIDAD PENETRANCIA HETEROGENEIDAD VARIABILIDAD Pruebas Específicas @nálisis de la Información Pronóstico Individual Prevención Complicaciones Tratamiento Estudio de Portadores Diagnóstico Prenatal Diagnóstico Preimplantatorio Terapia Conducta Obstétrica

16
Análisis molecular directo
98pb F508 95pb F508 heteroduplex

17
Anomalías Congénitas Cardíacas y
Genética Clínica Consejo Genético Basado en el Fenotipo (pre-posnatal) Análisis Genético (citogenético, citogenética molecular) Historia Natural y resultados esperables Problema y aproximación perinatal
 Análisis Genético (citogenético, citogenética molecular) Historia Natural y resultados esperables. Problema y aproximación perinatal.")
18
Diagnóstico Genético Preimplantatorio
Análisis genético de los preembriones obtenidos por técnicas de fecundación in vitro antes de ser transferidos al útero.

19
DIAGNÓSTICO PREDICTIVO

20
Management of BRCA Mutation-Positive Individual
ASCO Positive BRCA1 or BRCA2 test result Possible testing for other adult relatives Increased surveillance Lifestyle changes Chemo- prevention Prophylactic surgery

21
CONSEJO GENÉTICO Objetivos
Ayudar al individuo y/o familia a: Entender la situación médica, incluyendo diagnóstico, curso probable de la enfermedad y el tratamiento. Conocer cómo la herencia contribuye al trastorno, así como el riesgo de recurrencia de la enfermedad. Comprender las alternativas para manejar el riesgo de recurrencia y/o ocurrencia. Elegir el manejo más efectivo según el riesgo, metas familiares, normas éticas y creencias religiosas, y actuar de acuerdo con dicha decisión. Favorecer la adaptación del individuo y la familia a la enfermedad y al riesgo de recurrencia.

22
Objetivos del Consejo Genético
Dar Información Decisión Informada Cuál es la enfermedad? Informar de los aspectos médicos de la enfermedad Explicar la herencia : Discutir la probabilidad de que ocurra otra vez y opciones Hablar de pronóstico y tratamiento

23
Hablar de decisiones Hacerse o no análisis genéticos
Tener o no más hijos Si es posible (y como) prevenir la aparición/ recurrencia de la enfermedad
 prevenir la aparición/ recurrencia de la enfermedad.")
24
Apoyo a TODA la familia Atención a otros miembros de la familia
Disponibilidad de análisis genéticos para familiares en riesgo

25
CONSEJO GENÉTICO. Indicaciones
Enfermedad genética conocida en el paciente Enfermedad genética conocida en la familia Riesgo Recurrencia familiar Enfermedad degenerativa o progresiva Síndrome polimalformativo conocido Síndrome polimalformativo no conocido Retraso mental y/o malformaciones Síndromes de cáncer hereditario…

26
Consejo Genético No directivo
No hay que hacer análisis genéticos siempre!

27
Historia Familiar Pedigree de tres generaciones como mínimo
Numero de familiares en primer grado con … Otras enfermedades crónicas/degenerativas, RM/CA … en la familia Background étnico Edad del diagnóstico Historia de la enfermedad y tratamientos en otros miembros de la familia afectos. Edad del exitus Clave para reconocer el patrón hereditario, la penetrancia, expresividad, y la heterogeneidad clínica y genética 27 27

28
CONSEJO GENÉTICO. Estimación del riesgo
Riesgo empírico: se utiliza para la mayor parte de las enfermedades multifactoriales/poligénicas y para la mayoría de las alteraciones cromosómicas. Se basa en los datos poblacionales observados y puede variar según la zona o ante la presencia de otro afecto en la familia. Riesgo mendeliano: sólo puede estimarse cuando está claramente establecido que la enfermedad se debe a la herencia de un único gen. Habrá de tenerse en cuenta el tipo de herencia: recesiva, dominante o ligada al cromosoma X. Existe, sin embargo, una serie de características de estas enfermedades que pueden complicar la estimación del riesgo y el proceso de Consejo Genético en general: Heterogeneidad genética Penetrancia Expresividad variable Riesgo modificado: el riesgo a priori, basado en la herencia mendeliana, se modifica con datos específicos de la familia a estudiar. Se utiliza especialmente en enfermedades recesivas ligadas al X.

29
PENETRANCIA EXPRESIVIDAD HETEROGENEIDAD
PROPORCION DE INDIVIDUOS CON UNA MUTACION GENETICA QUE PRESENTAN UNA MANIFESTACION FENOTÍPICA. Penetrancia del 50-80% de la pacientes con mutacion del gen BRCA-1. Es decir del 50 al 80% de las muhjeres que tienen una mutacion en el gen BRCA-1 van a desarrollar un cancer de mama hereditario.

30
PENETRANCIA EXPRESIVIDAD HETEROGENEIDAD
GRADO DE EXPRESIÓN CLÍNICA (FENOTIPO) DE UNA MUTACIÓN DE UN GEN (NO LINEAL, GENES MODIFICADORES, GÉNERO, ETNIA,…)
 DE UNA MUTACIÓN DE UN GEN (NO LINEAL, GENES MODIFICADORES, GÉNERO, ETNIA,…)")
31
SÍNDROME DE SMITH-LEMLI-OPITZ
Trastorno autosómico recesivo que se caracteriza por múltiples anomalías congénitas entre las que se incluyen microcefalia, retraso mental, facie inusual, y anomalías genitales. El defecto bioquímico es la falta de 7-dehidrocolesterol-delta-7-reductasa, lo que produce niveles anormalmente elevados de 7-dehidrocolesterol y bajos niveles de colesterol. Nowaczyck et al, 2001

32
SÍNDROME DE SMITH-LEMLI-OPITZ
Nowaczyck et al, 2001

33
SÍNDROME DE SMITH-LEMLI-OPITZ
Nowaczyck et al, 2001

34
PENETRANCIA EXPRESIVIDAD HETEROGENEIDAD
Heterogeneidad alélica: fenotipo originado por diferentes mutaciones en el mismo gen. Heterogeneidad genética: Un fenotipo originado por mutaciones en diferentes genes.

35
Análisis de las mutaciones más frecuentes en Fibrosis Quística
G542X G551D R553X 1717-1G>A N1303K R117H 621+1G>T W1282X 1078 del T R334W R1162X A455E 3659 del C kbC>T D1507 S1251N R347P D1152H E60X 2183AA>G 711+1G>T 1898+1G>A 3120+1G>A 2184delA G85E 2789+5G>A I148T R560T Enfermedad de herencia autosómica recesiva. Gen responsable: CFTR (Cystic Fibrosis transmembrane regulator) Localización molecular: 7q31 Alteración molecular: mutaciones en el gen CFTR
 Localización molecular: 7q31. Alteración molecular: mutaciones en el gen CFTR.")
36
DISTROFIAS DE CINTURAS RECESIVAS (Limb Girdle Muscular Dystrophies Type 2
Localización génica Símbolo del gen Producto génico 15q15.1-q21.1 LGMD2A CAPN3 = calpaína 3 2p13 LGMD2B DYSF = disferlina 13q12 LGMD2C SGCG = -sarcoglicano 17q12-q LGMD2D SGCA = -sarcoglicano 4q12 LGMD2E SGCB = -sarcoglicano 5q33-q34 LGMD2F SGCD = -sarcoglicano 17q11-q12 LGMD2G TCAP = telethonina 9q31-q34.1 LGMD2H TRIM32 19q LGMD2I FKRP = fukutin related protein 2q LGMD2J TNTN = titina Las distrofias de cinturas constituyen un grupo heterogéneo de entidades, que comparten una afectación predominante de la debilidad a nivel de la musculatura de cintura pélvica o de la cintura escapular.

37
NO Análisis Genético Expresividad Penetrancia
Distribución en la población Heterogeneidad Variabilidad NO Validación Diagnóstico Fenotipo probable

38
El viaje del paciente en CG
Recoger la historia familiar Estimación del riesgo de recurrencia Análisis genéticos (si hay!, validez y utilidad clínica), incluyendo CG Seguimiento, incluyendo opciones reproductivas
, incluyendo CG. Seguimiento, incluyendo opciones reproductivas.")
39
Trabajo en Equipo Genetista Clínico
Medicina Diagnóstico y manejo clínico (opciones reproductivas) Diagnóstico Sindrómico Otros profesionales clínicos (geografía e historia) y no clínicos
 Diagnóstico Sindrómico. Otros profesionales clínicos (geografía e historia) y no clínicos.")
40
DIAGNÓSTICO PRENATAL
AVANCE TECNOLÓGICO AVANCE INSTRUMENTAL AVANCE EN ANESTESIA AVANCE EN PERINATOLOGÍA AVANCE EN GENÉTICA CLÍNICA DIAGNÓSTICO PRENATAL MEDICINA FETAL TERAPIA FETAL 40

41
Nuestra capacidad para el dx de anomalías fetales se ha multiplicado en las últimas 2 décadas
Esos avances han contribuído no sólo a la aplicación clínica del DP, también al manejo de la RCF, anemia fetal y TTTS. Las aplicaciones de la exploración ecográfica fetal y DP en el embarazo crecen de forma exponencial, proporcionando información clínica relevante desde las 12 semanas hasta el término del embarazo.

43
Aumento Translucencia Nucal 11-14 semanas gestación
ECOGRAFIA PRECOZ (11-14 SEMANAS DE GESTACIÓN) Aumento Translucencia Nucal 11-14 semanas gestación Aumento de la tasa de pérdidas fetales Enfermedades de base genética Anomalías congénitas (cardíacas)
 Aumento Translucencia Nucal semanas gestación. Aumento de la tasa de pérdidas. fetales. Enfermedades de base genética. Anomalías congénitas (cardíacas)")
44
En la última década surge el concepto de la Ecografía Genética.
Búsqueda de imágenes (marcadores) que nos ayudaran al cribado de fetos con anomalías cromosómicas. Se convierte en un examen fundamental para el Diagnóstico Prenatal. Se pueden utilizar tanto en primer como segundo trimestre. Sin embargo la precocidad es cada vez mas importante. Foto de eco a.bermejo AYUDADOS POR UNA MEJORA EN LA CALIDAD DE LOS SISTEMAS DE EXPLORACION. Cada vez con mejor sensibilidad.
 que nos ayudaran al cribado de fetos con anomalías cromosómicas. Se convierte en un examen fundamental para el Diagnóstico Prenatal. Se pueden utilizar tanto en primer como segundo trimestre. Sin embargo la precocidad es cada vez mas importante. Foto de eco a.bermejo AYUDADOS POR UNA MEJORA EN LA CALIDAD DE LOS SISTEMAS DE EXPLORACION. Cada vez con mejor sensibilidad.")
45
MARCADORES 1er TRIMESTRE

46
Consentimiento informado
Las gestantes deben recibir información adecuada. Consentimiento informado El personal, las gestantes y su familia deben conocer los objetivos específicos y las limitaciones de la exploración ecográfica que se va a realizar. Comunicación resultados adversos

48
Análisis molecular directo
98pb F508 95pb F508 heteroduplex

49
Análisis molecular directo
188pb copia telomérica 163pb copia centromérica

50
Sondas centroméricas: X, Y, 18
Sondas LSI: 13 y 21

51
Síndrome de DiGeorge/VCFS
3’ TUPLE 1 D22S553 D22S609 D22S942 110 Kb N25 D22S75 CTP CLATHRIN LSI TUPLE 1 22q11.2 cen Tel

52
LA MEDICINA FETAL SE SITÚA EN UN CONTEXTO PERINATAL, EN EL QUE LA ETAPA FETAL Y NEONATAL CONSTITUYEN MOMENTOS CONSECUTIVOS DE UNA PARTE CRÍTICA DEL DESARROLLO HUMANO QUE AFECTARÁ TAMBIÉN A LA EDAD ADULTA LA GENÉTICA CLÍNICA ES UN COMPONENTEFUNDAMENTAL DE LA TERAPIA FETAL. LAS CLAVES: HISTORIA NATURAL, DETECCIÓN Y SELECCIÓN DE CASOS.

53
Ecografía de alta resolución Ecocardiografía Procedimientos invasivos
Consejo Genético CRIBADO DE ANOMALÍAS CONGÉNITAS TERAPIA FETAL

54
Concepto medfet. El propósito no es la IVE, sino proporcionar la información y cuidados que necesita cada paciente. Ello significa que los fetos y recién nacidos que puedan ser tratados médica o quirúrgicamente estén en las mejores condiciones para recibir la mejor atención posible. Concepto SVA.

55
Conocimiento del problema fetal y su historia natural
CENTRO ESPECIALIZADO Planificar momento, lugar y tipo de parto Terapia prenatal, perinatal y/o neonatal

56
Riesgo/Beneficio de la Intervención Fetal
Riesgo de la intervención Complic Fetales Historia natural de la Patología Fetal complic Maternas Letalidad Morbilidad Intervención Fetal Observación

57
Riesgo/Beneficio de la Intervención Fetal
Historia natural de la Patología Fetal Riesgo de la intervención Morbilidad Complic Maternas Letalidad Complica Fetales Intervención Fetal Observación

58
Terapia farmalocógica
Administración de fármacos a la madre para que lleguen al feto a través de la placenta y permita la remisión de su sintomatología. Dentro de este grupo se incluiría el tratamiento para: Arritmias fetales, en especial las que cursan con algún grado de taquicardia fetal. Infecciones maternas que afectarían al feto a través de la contaminación vertical. En este grupo destacaría el tratamiento de infección por toxoplasmosis. Cirugía fetal Cirugía ecoguiada, que permite el acceso a distintos compartimientos ovulares y fetales, como: Cordocentesis para el tratamiento de las alteraciones sanguíneas fetales, en especial las anemias. Colocación de drenaje (shunts) para el vaciamiento constante por acumulación de líquidos en el feto, como los derrames pleurales y las malformaciones adenomatoideas quísticas. Valvuloplastias cardiacas para permitir el paso de sangre a través de válvulas estenóticas que condicionan un hipodesarrollo del compartimiento anterógrado (estenosis aórticas y pulmonares). Oclusión de cordón en caso de malformación discordante en gestaciones gemelares monocoriales y retraso de crecimiento selectivo severo en las gestaciones gemelares monocoriales. Cirugía fetoscópica sobre los anexos ovulares y el feto: Coagulación láser de las anastomosis vasculares fetales en caso de transfusión fetofetal y retraso de crecimiento selectivo en las gestaciones gemelares monocoriales. Ablación láser de bridas amnióticas Colocación de balón endotraqueal en los casos de hernia diafragmática congénita. Cirugía fetal abierta: EXIT (ex útero intrapartum treatment). Cirugía fetal (defectos del tubo neural).
 para el vaciamiento constante por acumulación de líquidos en el feto, como los derrames pleurales y las malformaciones adenomatoideas quísticas. Valvuloplastias cardiacas para permitir el paso de sangre a través de válvulas estenóticas que condicionan un hipodesarrollo del compartimiento anterógrado (estenosis aórticas y pulmonares). Oclusión de cordón en caso de malformación discordante en gestaciones gemelares monocoriales y retraso de crecimiento selectivo severo en las gestaciones gemelares monocoriales. Cirugía fetoscópica sobre los anexos ovulares y el feto: Coagulación láser de las anastomosis vasculares fetales en caso de transfusión fetofetal y retraso de crecimiento selectivo en las gestaciones gemelares monocoriales. Ablación láser de bridas amnióticas. Colocación de balón endotraqueal en los casos de hernia diafragmática congénita. Cirugía fetal abierta: EXIT (ex útero intrapartum treatment). Cirugía fetal (defectos del tubo neural).")
66
Medicines during pregnancy
Increased public awareness and concern since the thalidomide tragedy. Many pregnancies are unplanned and medicines will have been taken inadvertently. Medicines can not always be avoided, especially in the treatment of long-term conditions.

67
Medicines during pregnancy
Background rate of 2-3% for major congenital malformations. Over 75% of these are of unknown aetiology. Virtually all medicines cross the placenta and reach the foetus in measurable concentrations. Medicines do not need to cross the placenta to affect the foetus. Background rate in the general population 2-3%, estimated that 1-2% due to drugs. Medicines do not need to cross the placenta to affect the foetus – Examples: - e.g. insulin does not cross the placenta (due to it’s high molecular weight) but the glucose produced during episodes of maternal hyperglycaemia may pass across causing the foetus to produce insulin that cannot be cleared. - e.g. vasoconstriction of placental vasculature can harm foetus.
 but the glucose produced during episodes of maternal hyperglycaemia may pass across causing the foetus to produce insulin that cannot be cleared. - e.g. vasoconstriction of placental vasculature can harm foetus.")
68
Teratogen Any agent which given in pregnancy that directly or indirectly causes structural or functional abnormalities in the foetus or child after birth. Teratogens do not cause abnormalities in all foetus exposed at critical period, e.g. thalidomide (highly teratogenic), caused abnormalities in less than half of all foetuses exposed during the critical period.
, caused abnormalities in less than half of all foetuses exposed during the critical period.")
69
Identification Of Teratogens
Many possible causes for a birth defect (genetic, physiological, nutrition, medicines, pollutants). Extremely difficult to determine whether or not a particular agent is a teratogen. Clinical trials of medicines in pregnant women is usually unethical. Difficult to extrapolate findings in animal studies to a human pregnancy. Risk of teratogenecity may increase if the number of different medicines is increased. Useful to point out that in epilepsy it is extremely difficult to determine whether or not a particular agent is a teratogen. It is thought that the disease itself contributes to the risk of adverse outcome and the medicines taken contribute to this risk. The problem is decided how much each component contributes to the documented overall increased risk of malformation. Teratogenecity is often dose dependent. There is normally a threshold dose below which drug does not exert any teratogenic effects. Risk of teratogenecity may increase if the number of concomitant drugs is increased, e.g. in epilepsy, the risk of teratogenecity increases as the number of antiepileptics increases. Animal Studies Rodents are often used to evaluate safety of drugs in pregnancy, but their physiology, metabolism and development are very different to humans. It cannot be assumed that a drug that does not cause embroyotoxicity, foetotoxicity or teratogenecity in animal studies can be used ‘safely’ in human pregnancies. However if a drug does cause foetal toxicity in several animal species, this is an indicator that the same effect may occur in man.
. Extremely difficult to determine whether or not a particular agent is a teratogen. Clinical trials of medicines in pregnant women is usually unethical. Difficult to extrapolate findings in animal studies to a human pregnancy. Risk of teratogenecity may increase if the number of different medicines is increased. Useful to point out that in epilepsy it is extremely difficult to determine whether or not a particular agent is a teratogen. It is thought that the disease itself contributes to the risk of adverse outcome and the medicines taken contribute to this risk. The problem is decided how much each component contributes to the documented overall increased risk of malformation. Teratogenecity is often dose dependent. There is normally a threshold dose below which drug does not exert any teratogenic effects. Risk of teratogenecity may increase if the number of concomitant drugs is increased, e.g. in epilepsy, the risk of teratogenecity increases as the number of antiepileptics increases. Animal Studies. Rodents are often used to evaluate safety of drugs in pregnancy, but their physiology, metabolism and development are very different to humans. It cannot be assumed that a drug that does not cause embroyotoxicity, foetotoxicity or teratogenecity in animal studies can be used ‘safely’ in human pregnancies. However if a drug does cause foetal toxicity in several animal species, this is an indicator that the same effect may occur in man.")
70
Examples Cocaine CNS, intestinal & kidney damage
Anticonvulsants (carbamazepine, valproate) Multiple malformations, Spina bifida Retinoids/Vitamin A Cranio-facial, CVS & CNS defects Warfarin Foetal warfarin syndrome Alcohol Foetal alcohol syndrome/effects Anticonvulsants - in an epileptic pregnant women, would need to control her epilepsy as the disease itself could cause harm to the unborn child, but also consider the risks of each anticonvulsant and choose the anticonvulsant(s) with the best profile and most experience of use in pregnancy. The chosen medication(s) should be used at the lowest effective dose. Retinoids – e.g. isotretinoin (Roaccutane) for acne – must exclude pregnancy before treatment and use effective contraception for 1 month before, during and for 1 month after treatment. Effective contraception is advised to be at least one but preferable two, forms of contraception including a barrier method. Note – vitamin A may be contained within multivitamin preparations. Alcohol (for recommendations see later slide) Foetal alcohol syndrome = restricted growth, heart defects,
 Multiple malformations, Spina bifida. Retinoids/Vitamin A. Cranio-facial, CVS & CNS defects. Warfarin. Foetal warfarin syndrome. Alcohol. Foetal alcohol syndrome/effects. Anticonvulsants - in an epileptic pregnant women, would need to control her epilepsy as the disease itself could cause harm to the unborn child, but also consider the risks of each anticonvulsant and choose the anticonvulsant(s) with the best profile and most experience of use in pregnancy. The chosen medication(s) should be used at the lowest effective dose. Retinoids – e.g. isotretinoin (Roaccutane) for acne – must exclude pregnancy before treatment and use effective contraception for 1 month before, during and for 1 month after treatment. Effective contraception is advised to be at least one but preferable two, forms of contraception including a barrier method. Note – vitamin A may be contained within multivitamin preparations. Alcohol (for recommendations see later slide) Foetal alcohol syndrome = restricted growth, heart defects,")
71
Timing Of Exposure 1st Trimester (1- 12 weeks post LMP)
Up to 4 weeks, “all or nothing” effect Weeks 3-8, major organ systems being formed 2nd Trimester (4th – 6th month) Cerebellum & urogential system still forming Growth and functional development 3rd Trimester (6th – 9th month) Specific effects e.g. NSAIDs (pulmonary hypertension) B-blockers (hypoglycaemia) Near Term/During labour Adverse effects on labour or on neonate after delivery. LMP = last menstrual period. Take care with weeks presented by caller as often women count from conception rather than from last menstrual period. “All or nothing” effect Exposure to a drug during the pre-embryonic phase of pregnancy, which lasts until the 17th day after conception, which will either result in survival of the intact embryo or death. If most cells are affected the pregnancy is spontaneously miscarried. If only a few cells are damaged the embryo is normally unaffected. Most women will not have missed their first period and not even realise they are pregnant. 2 weeks post conception = ~ 4weeks into pregnancy. The period of maximal susceptibility to teratogenic effects is usually the first ten weeks postconception (i.e. up to 12 weeks after last menstrual period), when the women is often not aware of the pregnancy. However, it is not only the first trimester that is important when assessing potential foetal toxicity, with some drugs and chemicals there are risks associated with exposure later in pregnancy.
 Cerebellum & urogential system still forming. Growth and functional development. 3rd Trimester (6th – 9th month) Specific effects e.g. NSAIDs (pulmonary hypertension) B-blockers (hypoglycaemia) Near Term/During labour. Adverse effects on labour or on neonate after delivery. LMP = last menstrual period. Take care with weeks presented by caller as often women count from conception rather than from last menstrual period. All or nothing effect. Exposure to a drug during the pre-embryonic phase of pregnancy, which lasts until the 17th day after conception, which will either result in survival of the intact embryo or death. If most cells are affected the pregnancy is spontaneously miscarried. If only a few cells are damaged the embryo is normally unaffected. Most women will not have missed their first period and not even realise they are pregnant. 2 weeks post conception = ~ 4weeks into pregnancy. The period of maximal susceptibility to teratogenic effects is usually the first ten weeks postconception (i.e. up to 12 weeks after last menstrual period), when the women is often not aware of the pregnancy. However, it is not only the first trimester that is important when assessing potential foetal toxicity, with some drugs and chemicals there are risks associated with exposure later in pregnancy.")
72
Potential Adverse Effects
Spontaneous abortions Intra-uterine growth retardation Prematurity Stillbirths Obstetric complications Neonatal side effects Withdrawal reactions Drug side effects in neonate Whilst foetal malformations are the most obvious adverse pregnancy outcome that medicines can cause, there are others. Examples of medicines causing effects above: Spontaneous abortions – isotretinoin IUGR – street drugs Prematurity / stillbirths – warfarin Obstetric complications – NSAIDs can cause excessive maternal bleeding Neonatal side effects –normally due to exposure near term e.g. withdrawal (CNS medicines – opioids or benzodiazepines) and predictable pharmacological effects (beta blockers causing hypoglycaemia, bradycardia) Intrauterine exposure can have delayed and lasting effects (diethylstilboestrol)
 and predictable pharmacological effects (beta blockers causing hypoglycaemia, bradycardia) Intrauterine exposure can have delayed and lasting effects (diethylstilboestrol)")
73
General Advice for Medicines in Pregnancy
Consider non-drug treatments. Avoid all medicines in the 1st trimester if possible. Only prescribe medicines if absolutely necessary. Assess benefit/risk ratio for both mother & infant. Avoid new medicines as usually more experience with well-established ones. Also bear in mind that drug pharmacokinetics will change in mother when pregnant. If pregnant woman has chronic conditions (e.g. asthma, hypertension) – monitoring will need to be intensified during pregnancy.
 – monitoring will need to be intensified during pregnancy.")
74
General Advice for Medicines in Pregnancy
Use the lowest effective dose for as short a time as possible. Avoid polypharmacy Diet & alcohol recommendations Folic acid 400mcg pre-conception and until week 12 of pregnancy Foods to avoid in Pregnancy: Foods containing raw/undercooked eggs – e.g. home made mayo, ice cream, mousse – risk of Salmonella Certain cheeses – mould ripened soft chesses (Brie/Camembert), blue cheeses (Stilton/Danish Blue) – risk of Listeria Unpasteurised milk Liver/liver products (e.g. pate) – due to Vitamin A content Peanuts/peanut products Shark, marlin, swordfish and limit the amount of tuna you eat (limit to two steaks or 4 cans of tuna/week -due to mercury content) Alcohol: UK’s Chief Medical Officers advise that pregnant women or women trying to conceive should avoid drinking alcohol. If they choose to drink, to protect your baby, they should not drink more than one or two units of alcohol once or twice a week and should not get drunk. One unit = ½ pint ordinary strength beer, lager or cider Single measure of a spirit (25ml) ½ standard glass of wine (175ml) 2/3 bottle of alcopop Small glass of sherry or measure of vermouth
, blue cheeses (Stilton/Danish Blue) – risk of Listeria. Unpasteurised milk. Liver/liver products (e.g. pate) – due to Vitamin A content. Peanuts/peanut products. Shark, marlin, swordfish and limit the amount of tuna you eat (limit to two steaks or 4 cans of tuna/week -due to mercury content) Alcohol: UK’s Chief Medical Officers advise that pregnant women or women trying to conceive should avoid drinking alcohol. If they choose to drink, to protect your baby, they should not drink more than one or two units of alcohol once or twice a week and should not get drunk. One unit = ½ pint ordinary strength beer, lager or cider. Single measure of a spirit (25ml) ½ standard glass of wine (175ml) 2/3 bottle of alcopop. Small glass of sherry or measure of vermouth.")
75
Essential questions to ask
Is woman pregnant or planning to become pregnant? Her age? Has she already taken the medicine(s)? Has this been prescribed or self-treating? Medicine(s), indication, dose, frequency, route & duration of exposure? Number of weeks pregnant at time of exposure? How is pregnancy progressing? Any previous pregnancies & outcomes? Age – NA will have DoB on CAS record, but important to note that age is important as it can contribute to risk. If planning pregnancy – is she taking folic acid supplements 400mcg/day whilst trying to conceive and up to week 12 of pregnancy – to reduce the risk of neural tube defects in foetus. Some women on anti-epileptics or had a previous child with neural tube defects will be advised to take folic acid 5mg (will need to be prescribed)
 Has this been prescribed or self-treating Medicine(s), indication, dose, frequency, route & duration of exposure Number of weeks pregnant at time of exposure How is pregnancy progressing Any previous pregnancies & outcomes Age – NA will have DoB on CAS record, but important to note that age is important as it can contribute to risk. If planning pregnancy – is she taking folic acid supplements 400mcg/day whilst trying to conceive and up to week 12 of pregnancy – to reduce the risk of neural tube defects in foetus. Some women on anti-epileptics or had a previous child with neural tube defects will be advised to take folic acid 5mg (will need to be prescribed)")
76
When to refer If there is no information or information is unclear or conflicting Medicine has been taken but info sources say to avoid in pregnancy. If pregnant woman has taken a known teratogen If pregnant woman is on medicines to control long term conditions. Will need to discuss treatment plan with her Dr. Refresh memory on how to refer to UKMI

Presentaciones similares