Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Ricardo del Olmo Becario Hospital Clínic i Provincial Barcelona – España Hospital María Ferrer Fundación CIDEA Buenos Aires - Argentina Asma Severo, Asma No Controlado, Asma de Difícil Control ¿Son lo mismo o diferentes? Asma Severo, Asma No Controlado, Asma de Difícil Control ¿Son lo mismo o diferentes?

2
Asma Severa: Definiciones, Pasado y Presente – Definiciones previas (ATS y ERS): Altas dosis de tratamiento según consideración de guías internacionales – Definición 2013 ATS-ERS: Altas dosis de CI+LABA y/o corticoides sistémicos. Y simplifica criterios menores: Altas dosis de tratamiento para lograr el control, o control nunca alcanzado a pesar del tratamiento a dosis plenas 1° Paso Confirmación del diagnóstico 2° Paso Asma Severa vs Leve-Moderada 3° Paso Establecer si hay o no control Sin definiciones respecto a heterogeneidad, biomarcadores o patobiología Asma Severo, Asma No Controlado, Asma de Difícil Control ¿Son lo mismo o diferentes? Asma Severo, Asma No Controlado, Asma de Difícil Control ¿Son lo mismo o diferentes?

3
Asma Severa: Difícil Control – Altas dosis de Corticoides Inhalados (Fluticasona ± 1000 mcg o equivalente) – + 2° medicación de control (LABA) (o uso de Corticoides Sistémicos) para lograrlo – o persistencia de “descontrol” a pesar de este tratamiento Pacientes bajo control pero que empeoran al reducir las dosis de medicación, también forman parte del grupo Asma Severo, Asma No Controlado, Asma de Difícil Control ¿Son lo mismo o diferentes? Asma Severo, Asma No Controlado, Asma de Difícil Control ¿Son lo mismo o diferentes?

4
Control vs No control – Impacto en la calidad de vida: ACQ consistentemente > 1.5 o ACT < 20 durante evaluación de 3 meses – Exacerbaciones frecuentes: 2 o mas en el año previo, con uso de corticoides sistémicos > 3 días en c/evento – Exacerbaciones graves: 1 hospitalización o Ingreso a UCI o Asistencia Respiratoria en el último año – Deterioro funcional: VEF 1 < 80% (con ↓VEF 1 /CVF) al disminuir medicación UNO de ellos significa Pérdida del Control Asma Severo, Asma No Controlado, Asma de Difícil Control ¿Son lo mismo o diferentes? Asma Severo, Asma No Controlado, Asma de Difícil Control ¿Son lo mismo o diferentes?

5
Asma sin Tratamiento de Control Adecuado vs Asma de Difícil Control en Hospital María Ferrer 147 pacientes, 164 internaciones consecutivas 37 pacientes (25%) en grupo 1 (TRSA) (84% mujeres). 110 pacientes (75%) grupo 2 (DTTSA) y ninguno grupo 3. Diferencias estadísticamente significativas en “Grupo 1 Refractaria” vs “Grupo 2 Acceso Inadecuado” – Edad (51.3±14.9 vs. 39.8±13,5 ys., P<0.0001), – Mas de 1 internación previa (54% vs 28%, P<0.05), – Tabaquismo activo (5.4% vs 20% P< 0.0001), – Sinusitis (40.5% vs 19.6% P<0.05), – Antecedentes de enfermedad psiquiátrica (40.5% vs 22%, P<0.05) and – Prevalencia de síntomas de RGE (63.9% vs 46% P<0.05). – Mujeres de grupo 1 (TRSA) con mayor edad (P<0.05) y IMC (P<0.05) que grupo 2 (DTTSA). – Sin diferencias en nivel educativo, edad de inicio del asma, Rinitis Alérgica,, nivel de ac. Láctico o FeNO. ERSCongress Barcelona 2013 Sin diferencias en VEF 1 (%) al ingreso
 grupo 2 (DTTSA) y ninguno grupo 3. Diferencias estadísticamente significativas en Grupo 1 Refractaria vs Grupo 2 Acceso Inadecuado – Edad (51.3±14.9 vs. 39.8±13,5 ys., P<0.0001), – Mas de 1 internación previa (54% vs 28%, P<0.05), – Tabaquismo activo (5.4% vs 20% P< ), – Sinusitis (40.5% vs 19.6% P<0.05), – Antecedentes de enfermedad psiquiátrica (40.5% vs 22%, P<0.05) and – Prevalencia de síntomas de RGE (63.9% vs 46% P<0.05). – Mujeres de grupo 1 (TRSA) con mayor edad (P<0.05) y IMC (P<0.05) que grupo 2 (DTTSA). – Sin diferencias en nivel educativo, edad de inicio del asma, Rinitis Alérgica,, nivel de ac. Láctico o FeNO. ERSCongress Barcelona 2013 Sin diferencias en VEF 1 (%) al ingreso.")
6
43,9% usan 400 dosis al mes (13 disparos al día) 43,9% usan 400 dosis al mes (13 disparos al día) Uso de Salbutamol como Rescate Menos de 15 días 15-30 días 1-2 meses Más de 2 meses Sin datos
 43,9% usan 400 dosis al mes (13 disparos al día) Uso de Salbutamol como Rescate Menos de 15 días días 1-2 meses Más de 2 meses Sin datos")
7
Nunca Control del Asma Visitas a guardia en el último año Control del Asma Visitas a guardia en el último año 1 vez 2 veces Mas de 2 veces

8
Resultados de Inflamación vs Celularidad Análisis de 65 pacientes

9
IL8EosinofilicosNeutrofilicosPaucigranulociticos Mean481,6931121,1 Std. Error85,24128,138,74

10
Pacientes Eosinofílicos (n = 37, 5 ADC : 14 %) Pacientes Neutrofílicos (n = 4, 3 ADC: 75 %) Pacientes Paucigranulocíticos (n = 15, 1 ADC: 6.5%)
 Pacientes Neutrofílicos (n = 4, 3 ADC: 75 %) Pacientes Paucigranulocíticos (n = 15, 1 ADC: 6.5%)")
11
Pero entonces… ¿Los pacientes con asma grave son o no diferentes?

12
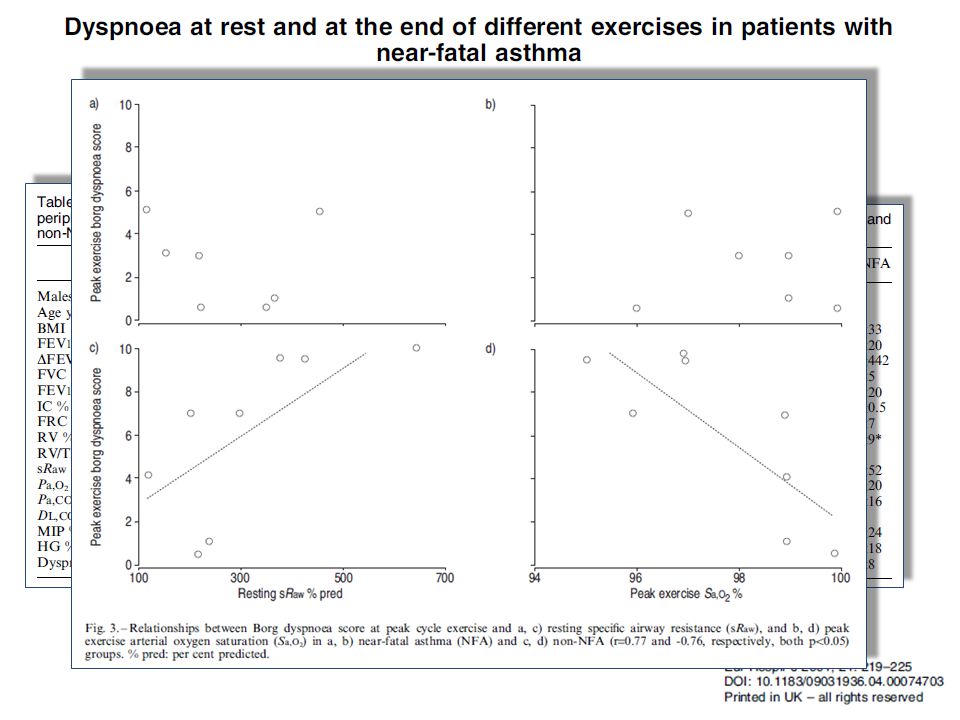
Las pruebas funcionales “inestables”…

13
Las pruebas funcionales “inestables”… (19 pacientes con BC durante la espirometría) 13 pacientes (68%) sufrieron episodios de asma casi fatal 9 pacientes (47%) tenían VEF 1 > 65% del predicho en la visita inicial 6 pacientes (32%) tuvieron una caída de su VEF 1 >50%.
 13 pacientes (68%) sufrieron episodios de asma casi fatal 9 pacientes (47%) tenían VEF 1 > 65% del predicho en la visita inicial 6 pacientes (32%) tuvieron una caída de su VEF 1 >50%.")
16
¿Los pacientes con asma grave son o no diferentes? La gravedad es una situación que puede ser inherente a la enfermedad en sí, pero también un hecho puntual en la historia de un paciente en particular Un evento de riesgo vital se puede presentar inesperadamente en un paciente que por otros aspectos puede estar en control y poco/nada sintomático (inesperado) Existen enfermos con propensión a eventos críticos con riesgo vital a pesar del adecuado acceso al tratamiento (Fatality prone) El control o falta del mismo es una situación de necesaria evaluación retrospectiva o prospectiva, pero que implica concepto de tiempo e intensidad de la medicación de control usada El concepto de Difícil Control implica adecuada indicación de dosis máximas de los mejores controladores, tiempo suficiente de uso, adherencia total, y a pesar de ello no poder cumplir con las expectativas ideales del paciente y médico La mayoría de los pacientes pueden lograr un control adecuado si usan bien medicación controladora (esteroides inhalados) El uso del esputo inducido (eosinofilia), FeNO, Periostina, dosaje de IgE o eosinofilia en sangre periférica puede marcar perfil TH2 elevado. La ausencia de los mismos perfil TH2 bajo Entonces si… Son diferentes
 Existen enfermos con propensión a eventos críticos con riesgo vital a pesar del adecuado acceso al tratamiento (Fatality prone) El control o falta del mismo es una situación de necesaria evaluación retrospectiva o prospectiva, pero que implica concepto de tiempo e intensidad de la medicación de control usada El concepto de Difícil Control implica adecuada indicación de dosis máximas de los mejores controladores, tiempo suficiente de uso, adherencia total, y a pesar de ello no poder cumplir con las expectativas ideales del paciente y médico La mayoría de los pacientes pueden lograr un control adecuado si usan bien medicación controladora (esteroides inhalados) El uso del esputo inducido (eosinofilia), FeNO, Periostina, dosaje de IgE o eosinofilia en sangre periférica puede marcar perfil TH2 elevado. La ausencia de los mismos perfil TH2 bajo Entonces si… Son diferentes.")
17
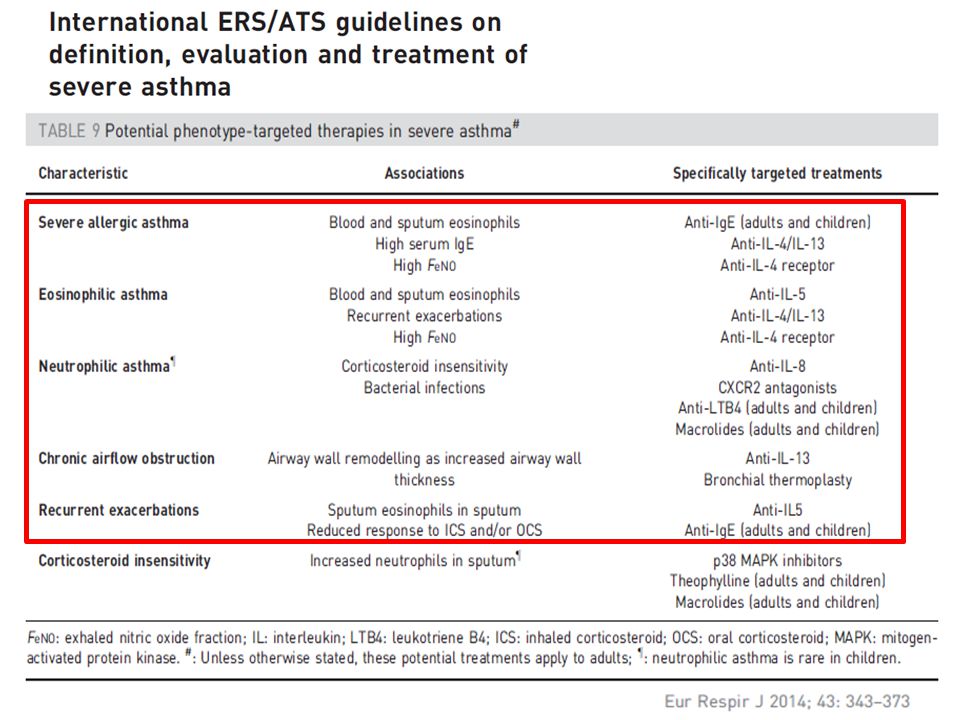
En el árbol de decisión hay que buscar Opciones terapéuticas diferentes Lo que puedo usar y lo que viene… En el árbol de decisión hay que buscar Opciones terapéuticas diferentes Lo que puedo usar y lo que viene…

19
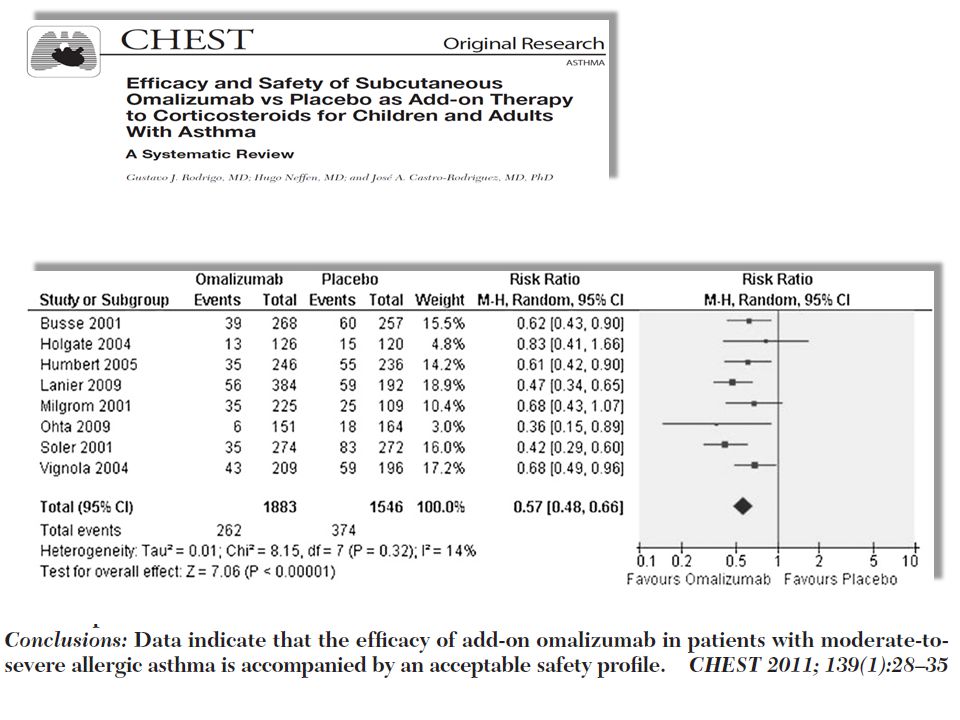
Omalizumab: Anticuerpo monoclonal humanizado contra IgE 10 años desde su registro Evaluación de seguridad: >9500 pacientes en programas clínicos > 400.000 pte/Tto/año post-market Omalizumab reduce el nivel de múltiples marcadores inflamatorios 1–6 Omalizumab reduce la respuesta temprana y tardía luego de exposición al antígeno 7,8 Eosinofilia periférica, en esputo y en submucosa bronquial 1 IL-2, IL-4, IL-5, IL-13 y GM-CSF 1–4 T-lymphocytes y B-lymphocytes 5 FeNO 6 1. Noga O, et al. J Allergy Clin Immunol 2006;117:1493–9; 2. Holgate S, et al. Allergy 2009;64:1728‒36; 3. Simon HU, et al. Eur J Immunol 2003;33:834–9; 4. Corren J. Discov Med 2012;13:305‒12; 5. Djukanović R, et al. Am J Respir Crit Care Med 2004;170:583–93; 6. Hanania HA, et al. Am J Respir Crit Care Med 2013;Mar 7 [Epub ahead of print]; 7. Fahy J, et al. Am J Respir Crit Care Med 1997;155:1828‒34; 8. van Rensen ELJ, et al. Allergy 2009;64:72–80.

20
Rabe KF, et al. Allergy 2011;66:1142–51; Galli SJ, Tsai M. Nat Med 2012;18:693–704.

22
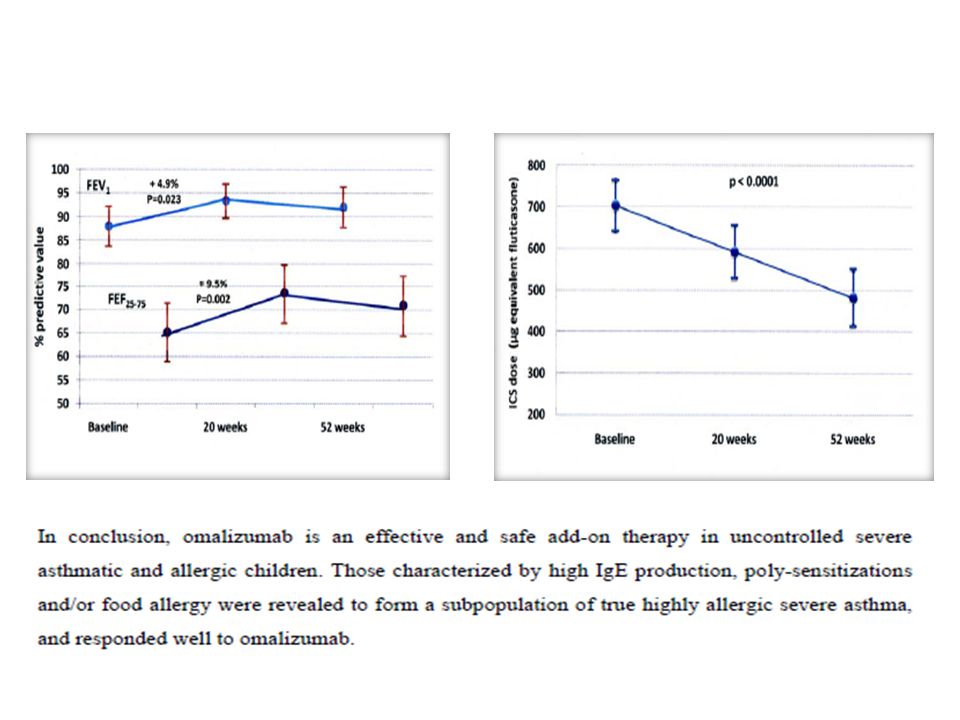
ERJ Express. Published on March 21, 2013 as doi: 10.1183/09031936.00149812 Add-on omalizumab in children with severe allergic asthma: a one year real life survey

25
Garcia, et al. Chest 144(2):411-419, 2013 Omalizumab en asma intríseca ? Change in FEV 1 (% pred.) FCεRI expression on dendritic cells FEV 1 Exacerbations Omalizumab Placebo 16 weeks OmalizumabPlacebo p=0.029 Exacerbations Omalizumab vs. placebo 0.8 vs. 1.4, p=0.278 41 patients with severe non- allergic asthma 55 yrs., IgE 155 IU/ml, FEV 1 66%
 FCεRI expression on dendritic cells FEV 1 Exacerbations Omalizumab Placebo 16 weeks OmalizumabPlacebo p=0.029 Exacerbations Omalizumab vs. placebo 0.8 vs. 1.4, p= patients with severe non- allergic asthma 55 yrs., IgE 155 IU/ml, FEV 1 66%.")
32
The EXCELS study: long-term use of omalizumab Malignancy rates – all malignancies Ratio of rates 0.84 (95% CI: 0.62, 1.13) CI = confidence interval (95% CI: 14.2, 17.9) (95% CI: 16.5, 22.0) † † All non-omalizumab patients prior to any treatment with omalizumab Difference in rates –3.06 (95% CI: –9.19, 2.03) Long AA, et al. Am J Respir Crit Care Med 187;2013:A3869 295 events 190 events

33
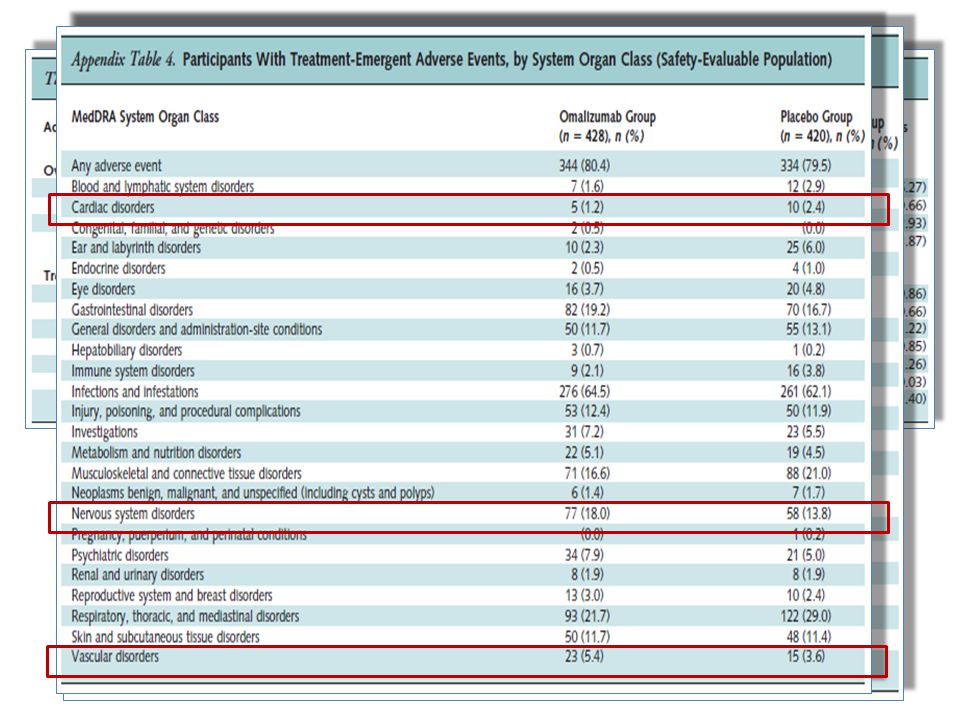
FDA Drug Safety Communication: FDA approves label changes for asthma drug Xolair (omalizumab), including describing slightly higher risk of heart and brain adverse events This update is in follow-up to the Early Communication about an Ongoing Safety Review of Omalizumab (marketed as Xolair) issued on July 16, 2009. [9-26-2014] Safety AnnouncementJuly 16, 2009 Safety Announcement A U.S. Food and Drug Administration (FDA) review of safety studies suggests a slightly increased risk of problems involving the heart and blood vessels supplying the brain among patients being treated with the asthma drug Xolair (omalizumab) than in those who were not treated with Xolair. As a result, we have added information about these potential risks to the drug label. Patients taking Xolair should continue to take the medication as prescribed and discuss any questions or concerns with their health care professionals. FDA approved Xolair in 2003 to treat patients 12 years and older with moderate to severe persistent asthma who have a positive skin or blood test to year-round allergens in the air and whose symptoms are not well-controlled by asthma medicines called inhaled corticosteroids. Xolair has been shown to decrease the number of asthma attacks in these patients. Our review of a 5-year safety study found a slightly higher rate of heart and brain blood vessel problems occurred in patients being treated with Xolair compared to those patients not treated with Xolair. The heart and brain blood vessel problems included mini-strokes known as transient ischemic attacks or TIAs; heart attacks; sudden, unexpected chest pain; high blood pressure in the arteries of the lungs called pulmonary hypertension; and blood clots in the lungs and veins. Although the data are suggestive of a serious safety signal, due to weaknesses in how the safety study was designed and carried out, we are unable to definitively confirm or determine the exact increased level of these risks with Xolair. Some previous clinical trials have shown slightly higher rates of various cancers in patients treated with Xolair compared with non-Xolair-treated patients. Our review of the 5-year safety study found no difference in the rates of cancer between those patients being treated with Xolair and those who were not being treated with Xolair. However, due to limitations in the 5-year study, we cannot rule out a potential risk of cancer with Xolair, so we have added this information to the Warnings and Precautions section of the drug label. Our review of a 5-year safety study found a slightly higher rate of heart and brain blood vessel problems occurred in patients being treated with Xolair compared to those patients not treated with Xolair. The heart and brain blood vessel problems included mini-strokes known as transient ischemic attacks or TIAs; heart attacks; sudden, unexpected chest pain; high blood pressure in the arteries of the lungs called pulmonary hypertension; and blood clots in the lungs and veins. Although the data are suggestive of a serious safety signal, due to weaknesses in how the safety study was designed and carried out, we are unable to definitively confirm or determine the exact increased level of these risks with Xolair. Some previous clinical trials have shown slightly higher rates of various cancers in patients treated with Xolair compared with non-Xolair-treated patients. Our review of the 5-year safety study found no difference in the rates of cancer between those patients being treated with Xolair and those who were not being treated with Xolair. However, due to limitations in the 5-year study, we cannot rule out a potential risk of cancer with Xolair, so we have added this information to the Warnings and Precautions section of the drug label.
 review of safety studies suggests a slightly increased risk of problems involving the heart and blood vessels supplying the brain among patients being treated with the asthma drug Xolair (omalizumab) than in those who were not treated with Xolair. As a result, we have added information about these potential risks to the drug label. Patients taking Xolair should continue to take the medication as prescribed and discuss any questions or concerns with their health care professionals. FDA approved Xolair in 2003 to treat patients 12 years and older with moderate to severe persistent asthma who have a positive skin or blood test to year-round allergens in the air and whose symptoms are not well-controlled by asthma medicines called inhaled corticosteroids. Xolair has been shown to decrease the number of asthma attacks in these patients. Our review of a 5-year safety study found a slightly higher rate of heart and brain blood vessel problems occurred in patients being treated with Xolair compared to those patients not treated with Xolair. The heart and brain blood vessel problems included mini-strokes known as transient ischemic attacks or TIAs; heart attacks; sudden, unexpected chest pain; high blood pressure in the arteries of the lungs called pulmonary hypertension; and blood clots in the lungs and veins. Although the data are suggestive of a serious safety signal, due to weaknesses in how the safety study was designed and carried out, we are unable to definitively confirm or determine the exact increased level of these risks with Xolair. Some previous clinical trials have shown slightly higher rates of various cancers in patients treated with Xolair compared with non-Xolair-treated patients. Our review of the 5-year safety study found no difference in the rates of cancer between those patients being treated with Xolair and those who were not being treated with Xolair. However, due to limitations in the 5-year study, we cannot rule out a potential risk of cancer with Xolair, so we have added this information to the Warnings and Precautions section of the drug label. Our review of a 5-year safety study found a slightly higher rate of heart and brain blood vessel problems occurred in patients being treated with Xolair compared to those patients not treated with Xolair. The heart and brain blood vessel problems included mini-strokes known as transient ischemic attacks or TIAs; heart attacks; sudden, unexpected chest pain; high blood pressure in the arteries of the lungs called pulmonary hypertension; and blood clots in the lungs and veins. Although the data are suggestive of a serious safety signal, due to weaknesses in how the safety study was designed and carried out, we are unable to definitively confirm or determine the exact increased level of these risks with Xolair. Some previous clinical trials have shown slightly higher rates of various cancers in patients treated with Xolair compared with non-Xolair-treated patients. Our review of the 5-year safety study found no difference in the rates of cancer between those patients being treated with Xolair and those who were not being treated with Xolair. However, due to limitations in the 5-year study, we cannot rule out a potential risk of cancer with Xolair, so we have added this information to the Warnings and Precautions section of the drug label..")
36
Anti - IgE Omalizumab QGE031 Anticuerpo Anti-receptor-IgE (anti-M1 prime) Otros biológicos en Asma Anti - IL-5 Mepolizumab Reslizumab Benralizumab (Anticuerpo Anti-receptor-IL-5) Anti - IL-13 Lebrikizumab Tralokinumab Anti - IL-4 Dupilumab (Anticuerpo Anti-receptor-IL-4)
 Otros biológicos en Asma Anti - IL-5 Mepolizumab Reslizumab Benralizumab (Anticuerpo Anti-receptor-IL-5) Anti - IL-13 Lebrikizumab Tralokinumab Anti - IL-4 Dupilumab (Anticuerpo Anti-receptor-IL-4)")
37
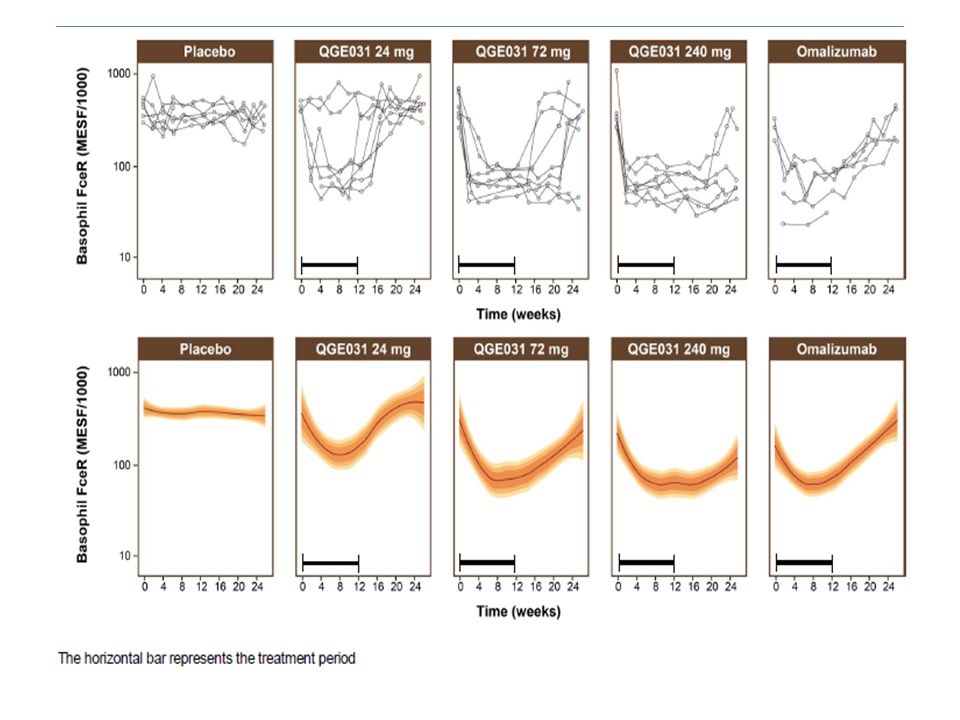
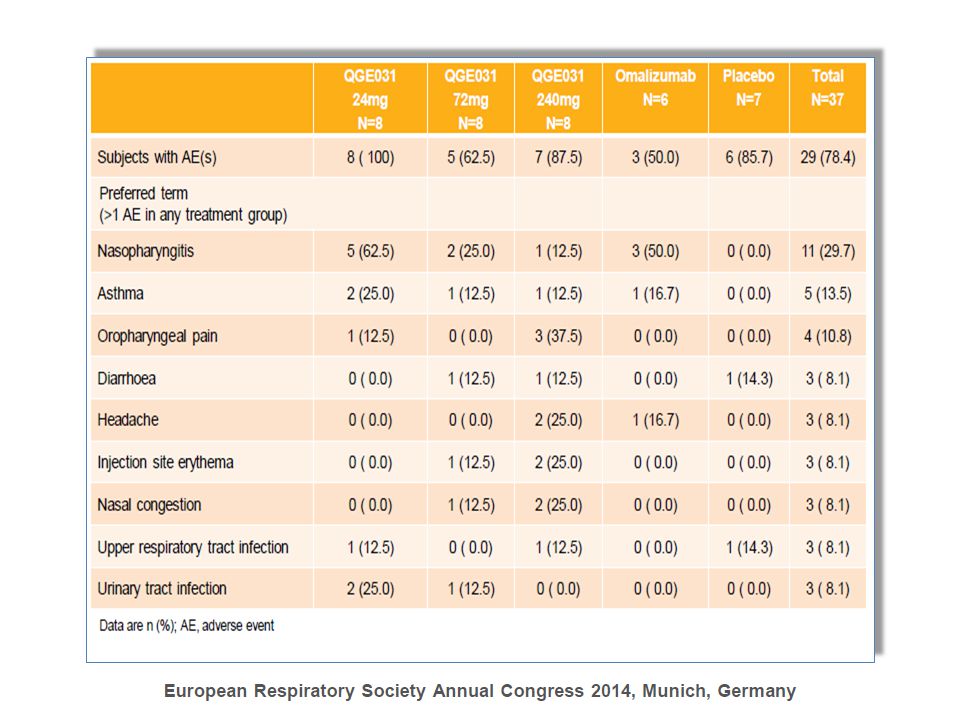
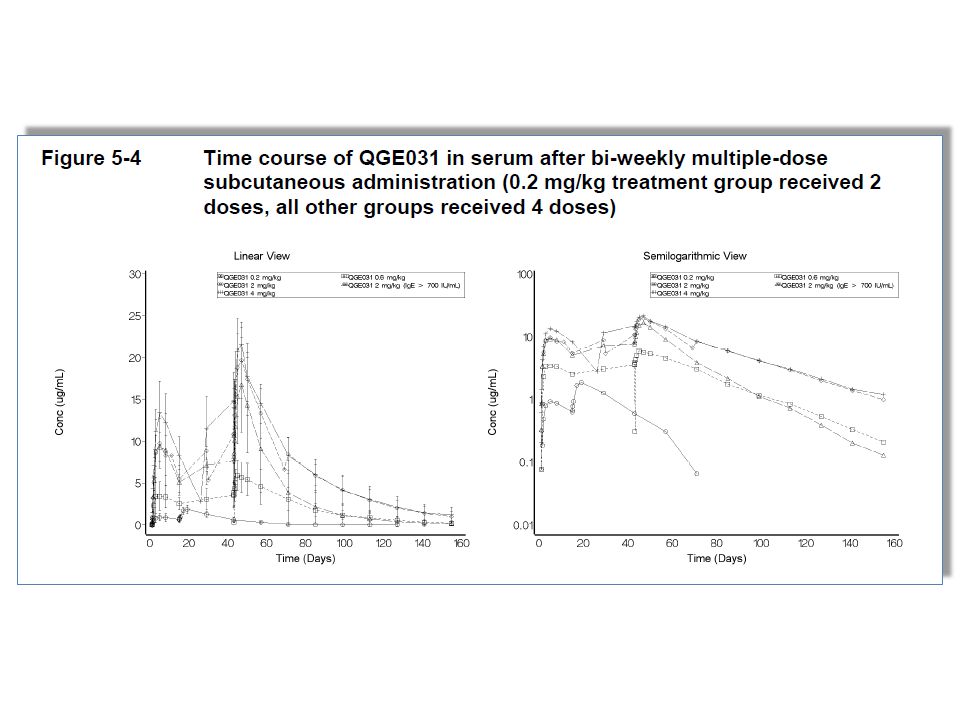
QGE-031: Propiedades químicas y datos preclínicos El próximo anti-IgE Licenciado por Tanox* in 2006 Propiedades Químicas – Ac Monoclonal Humanizado IgG1k de alta afinidad IgE (Kd=130pM, omalizumab Kd=6.8nM) – Diseñado para evitar anafilaxia – Formulación líquida con buena estabilidad (12 meses) Datos Pre-Clínicos – 54 veces mayor afinidad que Omalizumab a IgE – Bloqueo de la degranulación de basófilos y mastocitos mediada por IgE (~50 veces superior a Omalizumab) – QGE031 no causa toxicidad en simios a dosis SC 150mg/kg – 773 pacientes en estudios Fase I-II Mayor eficacia terapéutica?
 – Diseñado para evitar anafilaxia – Formulación líquida con buena estabilidad (12 meses) Datos Pre-Clínicos – 54 veces mayor afinidad que Omalizumab a IgE – Bloqueo de la degranulación de basófilos y mastocitos mediada por IgE (~50 veces superior a Omalizumab) – QGE031 no causa toxicidad en simios a dosis SC 150mg/kg – 773 pacientes en estudios Fase I-II Mayor eficacia terapéutica")
42
Pelaia, et al. Nat Rev Drug Discov 2012 Dupilumab Otros biológicos en asma

43
Dupilumab en asma eosinofílica Dupilumab (anti-IL-4 receptor) 300 mg s.c./week Placebo Wenzel, et al. N Engl J Med 368(26):2455-2466, 2013 12 weeks Exacerbaciones (% pacientes) Asthma patients on ICS + LABA ≥ 300 eos./µL blood or ≥3% sputum eos. - 87% p<0.001 [%] Exacerbaciones
: , weeks Exacerbaciones (% pacientes) Asthma patients on ICS + LABA ≥ 300 eos./µL blood or ≥3% sputum eos. - 87% p<0.001 [%] Exacerbaciones.")
44
Dupilumab en asma eosinofílica Tiempo a la 1° exacerbación Wenzel, et al. N Engl J Med 368(26):2455-2466, 2013
: ,")
45
Basal 1° mes 2° mes 3° mes

50
ESPUTO INDUCIDO Esputo Inducido Abrazando el futuro Muchas Gracias Augusto

Presentaciones similares

















>")






