Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Dr. Patricio Ibáñez L. Departamento de Gastroenterología
Cápsula Endoscopica Dr. Patricio Ibáñez L. Departamento de Gastroenterología

2
Evaluación del Intestino Delgado
Push Enteroscopy CT Enterography Small Bowel MRI’s Intra-operative enteroscopy Double Balloon Enteroscopy

4
Cápsula Diámetro 11mm: Largo 26mm Domo óptico: Iluminado por (LED’s)
Lente Color camera chip Transmisor 2 baterías (silver oxide)
")
5
Características de la Cápsula
Toma 2 imágenes por segundo En promedio se obtienenen 50,000 imágenes (8 h) Magnificación: 8x Recubrimiento de Cápsula: no-adherente Desechable
 Magnificación: 8x. Recubrimiento de Cápsula: no-adherente. Desechable.")
6
“Endoscopia fisiológica”
Intestino es visualizado en su estado normal No hay “ trauma endoscopico” No hay insuflación como artefacto Se puede hacer bajo anticoaculación

7
GE Junction Duodenum Jejunum Ileocecal Valve

8
Phlebectasia AVM Lymphangectasia Bleeding Lesion

9
Lymphoma GIST Polypoid Mass Polyp

10
NSAID stricture Radiation Enteritis Sprue Villous Drop Out

11
Hallazgos sutiles Punteado blanquecino en las vellosidades: Inlamatorio o neoplasico? “Q-tip” lesion

12
Ileitis Inflammatory polyp Linear Erosions Crohn’s disease

13
¿Cómo lo hacemos? Ayunas noche previa 12 Hr
Se aplican sensores en el paciente Se instala un cinturón con bateria y grabador (data recorder) Ingiere la cápsula (8-9 am) Puede tomar líquidos 2 hrs después Puede comer después de 4 hr Evitar estar cerca de otro paciente/cápsula. Debe volver 7-8 hrs después
 Ingiere la cápsula (8-9 am) Puede tomar líquidos 2 hrs después. Puede comer después de 4 hr. Evitar estar cerca de otro paciente/cápsula. Debe volver 7-8 hrs después.")
14
Indicaciones Sangrado Intestinal de origen oscuro
Anemia de origen no precisado Sospecha de Enfermedad de Crohn Sospecha de Enfermedad Celiaca Imagen de I Delgado anormal Sospecha de malabsorción Dolor abdominal sin causa clara Vigilancia de polipos en Sd Poliposos hereditarios

15
Complicaciones Retención : 1-5% Obstrucción: 0.5 % Aspiración: Raro
Cheifetz AS . Am Journal Gastro 2006

16
Contraindicaciones Absolutas: Relativas: Sospecha de obstrucción
Embarazo Relativas: Trastornos de motilidad Diverticulosis intestino delgado

17
Consentimiento CE no reemplaza evaluación de estómago y colon
Riesgo incluye obstrucción (puede requerir procedimiento para ser retirada) No hacer MR hasta que la CE ha pasado Puede no verse completo el ID
 No hacer MR hasta que la CE ha pasado. Puede no verse completo el ID.")
18
Tiempo de Tránsito Promedio
Estómago: 1 hra. Intestino Delgado: 4 hrs. Eliminación de Cápsula: 2-3 días

19
Cápsula en sangrado GI obscuro
Cápsula presenta mejor rendimiento diagnóstico que: Enteroscopia (56 vs 26 %) E-TAC (78 vs 22%) ; Cápsula + E-TAC 96% Angiografía Tasa de detección aumenta cuando la cápsula es precoz (< 48 hrs) Útil para definir sitio de sangrado previo a enteroscopia o cirugía Delvaux, M., Fassler, I. & Gay, G. Clinical usefulness of the endoscopic video capsule as the initial intestinal investigation in patients with obscure digestive bleeding: validation of a diagnostic strategy based on the patient outcome after 12 months. Endoscopy 36, 1067–1073 (2004). Milano, A. et al. A prospective evaluation of iron deficiency anemia in the GI endoscopy setting: role of standard endoscopy, videocapsule endoscopy, and CT‑enteroclysis. Gastrointest. Endosc. 73, 1002–1008 (2011). Saperas, E. et al. Capsule endoscopy versus computed tomographic or standard angiography for the diagnosis of obscure gastrointestinal bleeding. Am. J. Gastroenterol. 102, 731–737 (2007). Pasha, S. F. et al. Double-balloon enteroscopy and capsule endoscopy have comparable diagnostic yield in small-bowel disease: a meta-analysis. Clin. Gastroenterol. Hepatol. 6, 671–676 (2008). One study included 100 consecutive patients with obscure bleeding [55]. Patients were categorized into three groups; the diagnostic yield of VCE was highest in the group with ongoing overt bleeding (92 percent), compared with those with previous overt bleeding (13 percent) or guaiac positive stools and iron deficiency anemia (44 percent). The most common findings were angiectasia (29 percent) and Crohn's disease (6 percent). Other factors associated with an increased yield of VCE include older age, male sex, current hospitalization, increasing transfusion requirements, and the presence of connective disuse disease [53,58]. Endoscopy 2004: 36, 1067–1073. Gastrointest. Endosc. 2011: 73, 1002–1008.
 E-TAC (78 vs 22%) ; Cápsula + E-TAC 96% Angiografía. Tasa de detección aumenta cuando la cápsula es precoz (< 48 hrs) Útil para definir sitio de sangrado previo a enteroscopia o cirugía. Delvaux, M., Fassler, I. & Gay, G. Clinical usefulness of the endoscopic video capsule as the initial intestinal investigation in patients with obscure digestive bleeding: validation of a diagnostic strategy based on the patient outcome after 12 months. Endoscopy 36, 1067–1073 (2004). Milano, A. et al. A prospective evaluation of iron deficiency anemia in the GI endoscopy setting: role of standard endoscopy, videocapsule endoscopy, and CT‑enteroclysis. Gastrointest. Endosc. 73, 1002–1008 (2011). Saperas, E. et al. Capsule endoscopy versus computed tomographic or standard angiography for the diagnosis of obscure gastrointestinal bleeding. Am. J. Gastroenterol. 102, 731–737 (2007). Pasha, S. F. et al. Double-balloon enteroscopy and capsule endoscopy have comparable diagnostic yield in small-bowel disease: a meta-analysis. Clin. Gastroenterol. Hepatol. 6, 671–676 (2008). One study included 100 consecutive patients with obscure bleeding [55]. Patients were categorized into three groups; the diagnostic yield of VCE was highest in the group with ongoing overt bleeding (92 percent), compared with those with previous overt bleeding (13 percent) or guaiac positive stools and iron deficiency anemia (44 percent). The most common findings were angiectasia (29 percent) and Crohn s disease (6 percent). Other factors associated with an increased yield of VCE include older age, male sex, current hospitalization, increasing transfusion requirements, and the presence of connective disuse disease [53,58]. Endoscopy 2004: 36, 1067–1073. Gastrointest. Endosc. 2011: 73, 1002–1008.")
20
Aines vs aspirina ? LDA (78) AINEs (40) Lesiones 2.49 ± 3.15
Comparison of Small-Bowel Mucosal Injury between Low-Dose Aspirin and Non-Aspirin Non-Steroidal Anti-Inflammatory Drugs: A Capsule Endoscopy Study. All patients were found to have small-bowel mucosal injuries on CE. T he two groups were compared for the number of small-bowel mucosal injuries and CE scores on the basis of the findings of CE. Conclusion: Small-bowel mucosal injuries were significantly milder in the LDA group than in the non-aspirin NSAID group, though reddened lesions were more frequent in the LDA group. © 2014 S. Karger AG, Base LDA (78) AINEs (40) Lesiones 2.49 ± 3.15 1.65 ± 3.04 Ulceras 1.56 ± 3.75 6.08 ± 10.4 Delvaux, M., Fassler, I. & Gay, G. Clinical usefulness of the endoscopic video capsule as the initial intestinal investigation in patients with obscure digestive bleeding: validation of a diagnostic strategy based on the patient outcome after 12 months. Endoscopy 36, 1067–1073 (2004). Milano, A. et al. A prospective evaluation of iron deficiency anemia in the GI endoscopy setting: role of standard endoscopy, videocapsule endoscopy, and CT‑enteroclysis. Gastrointest. Endosc. 73, 1002–1008 (2011). Saperas, E. et al. Capsule endoscopy versus computed tomographic or standard angiography for the diagnosis of obscure gastrointestinal bleeding. Am. J. Gastroenterol. 102, 731–737 (2007). Pasha, S. F. et al. Double-balloon enteroscopy and capsule endoscopy have comparable diagnostic yield in small-bowel disease: a meta-analysis. Clin. Gastroenterol. Hepatol. 6, 671–676 (2008). One study included 100 consecutive patients with obscure bleeding [55]. Patients were categorized into three groups; the diagnostic yield of VCE was highest in the group with ongoing overt bleeding (92 percent), compared with those with previous overt bleeding (13 percent) or guaiac positive stools and iron deficiency anemia (44 percent). The most common findings were angiectasia (29 percent) and Crohn's disease (6 percent). Other factors associated with an increased yield of VCE include older age, male sex, current hospitalization, increasing transfusion requirements, and the presence of connective disuse disease [53,58]. Digestion May 22;89(3):
 AINEs (40) Lesiones ± ± Ulceras ± ± Delvaux, M., Fassler, I. & Gay, G. Clinical usefulness of the endoscopic video capsule as the initial intestinal investigation in patients with obscure digestive bleeding: validation of a diagnostic strategy based on the patient outcome after 12 months. Endoscopy 36, 1067–1073 (2004). Milano, A. et al. A prospective evaluation of iron deficiency anemia in the GI endoscopy setting: role of standard endoscopy, videocapsule endoscopy, and CT‑enteroclysis. Gastrointest. Endosc. 73, 1002–1008 (2011). Saperas, E. et al. Capsule endoscopy versus computed tomographic or standard angiography for the diagnosis of obscure gastrointestinal bleeding. Am. J. Gastroenterol. 102, 731–737 (2007). Pasha, S. F. et al. Double-balloon enteroscopy and capsule endoscopy have comparable diagnostic yield in small-bowel disease: a meta-analysis. Clin. Gastroenterol. Hepatol. 6, 671–676 (2008). One study included 100 consecutive patients with obscure bleeding [55]. Patients were categorized into three groups; the diagnostic yield of VCE was highest in the group with ongoing overt bleeding (92 percent), compared with those with previous overt bleeding (13 percent) or guaiac positive stools and iron deficiency anemia (44 percent). The most common findings were angiectasia (29 percent) and Crohn s disease (6 percent). Other factors associated with an increased yield of VCE include older age, male sex, current hospitalization, increasing transfusion requirements, and the presence of connective disuse disease [53,58]. Digestion May 22;89(3):")
21
Long-term follow-up of patients undergoing capsule and double-balloon enteroscopy for identification and treatment of small-bowel vascular lesions: a prospective, multicenter study Risk of rebleeding after endoscopic therapy for SBVLs detected by video capsule enteroscopy (VCE). The secondary aim was to assess risk factors for rebleeding. A prospective, multicenter study (15 centers) was conducted, involving patients with obscure gastrointestinal bleeding and SBVL on VCE who were treated during double-balloon enteroscopy (DBE). The likelihood of bleeding was defined according to VCE findings, as high or low. Results: 183 DBE therapy , and 64 (35 %) had rebleeding during the 1 year follow-up period Cardiac disease (hazard ratio [HR] 2.04, 95 % confidence interval [CI] 1.20 - 3.48; P < 0.01) overt bleeding (HR 1.78, 95 %CI 1.07 - 2.97; P = 0.03) at presentation were associated with the risk of rebleeding. chronic renal failure and the risk of rebleeding was close to statistical significance (HR 1.77, 95 %CI 0.94 - 3.33; P = 0.08). Kaplan-Meier analysis suggested that patients treated during DBE for a lesion with low likelihood of bleeding on VCE had higher rebleeding rates than those with a high likelihood of bleeding (HR 1.87, 95 %CI 0.94 - 3.37; P = 0.07). Conclusion: Despite long-term remission in most patients, about one-third had rebleeding at 1 year. Independent risk factors for rebleeding were cardiac disease and overt bleeding at original presentation. The lesion characteristics on VCE may be useful to evaluate the bleeding potential of the lesion and may be used for better selection of patients for DBE. Delvaux, M., Fassler, I. & Gay, G. Clinical usefulness of the endoscopic video capsule as the initial intestinal investigation in patients with obscure digestive bleeding: validation of a diagnostic strategy based on the patient outcome after 12 months. Endoscopy 36, 1067–1073 (2004). Milano, A. et al. A prospective evaluation of iron deficiency anemia in the GI endoscopy setting: role of standard endoscopy, videocapsule endoscopy, and CT‑enteroclysis. Gastrointest. Endosc. 73, 1002–1008 (2011). Saperas, E. et al. Capsule endoscopy versus computed tomographic or standard angiography for the diagnosis of obscure gastrointestinal bleeding. Am. J. Gastroenterol. 102, 731–737 (2007). Pasha, S. F. et al. Double-balloon enteroscopy and capsule endoscopy have comparable diagnostic yield in small-bowel disease: a meta-analysis. Clin. Gastroenterol. Hepatol. 6, 671–676 (2008). One study included 100 consecutive patients with obscure bleeding [55]. Patients were categorized into three groups; the diagnostic yield of VCE was highest in the group with ongoing overt bleeding (92 percent), compared with those with previous overt bleeding (13 percent) or guaiac positive stools and iron deficiency anemia (44 percent). The most common findings were angiectasia (29 percent) and Crohn's disease (6 percent). Other factors associated with an increased yield of VCE include older age, male sex, current hospitalization, increasing transfusion requirements, and the presence of connective disuse disease [53,58]. Endoscopy May 15.
. The secondary aim was to assess risk factors for rebleeding. A prospective, multicenter study (15 centers) was conducted, involving patients with obscure gastrointestinal bleeding and SBVL on VCE who were treated during double-balloon enteroscopy (DBE). The likelihood of bleeding was defined according to VCE findings, as high or low. Results: 183 DBE therapy , and 64 (35 %) had rebleeding during the 1 year follow-up period. Cardiac disease (hazard ratio [HR] 2.04, 95 % confidence interval [CI] ; P < 0.01) overt bleeding (HR 1.78, 95 %CI ; P = 0.03) at presentation were associated with the risk of rebleeding. chronic renal failure and the risk of rebleeding was close to statistical significance (HR 1.77, 95 %CI ; P = 0.08). Kaplan-Meier analysis suggested that patients treated during DBE for a lesion with low likelihood of bleeding on VCE had higher rebleeding rates than those with a high likelihood of bleeding (HR 1.87, 95 %CI ; P = 0.07). Conclusion: Despite long-term remission in most patients, about one-third had rebleeding at 1 year. Independent risk factors for rebleeding were cardiac disease and overt bleeding at original presentation. The lesion characteristics on VCE may be useful to evaluate the bleeding potential of the lesion and may be used for better selection of patients for DBE. Delvaux, M., Fassler, I. & Gay, G. Clinical usefulness of the endoscopic video capsule as the initial intestinal investigation in patients with obscure digestive bleeding: validation of a diagnostic strategy based on the patient outcome after 12 months. Endoscopy 36, 1067–1073 (2004). Milano, A. et al. A prospective evaluation of iron deficiency anemia in the GI endoscopy setting: role of standard endoscopy, videocapsule endoscopy, and CT‑enteroclysis. Gastrointest. Endosc. 73, 1002–1008 (2011). Saperas, E. et al. Capsule endoscopy versus computed tomographic or standard angiography for the diagnosis of obscure gastrointestinal bleeding. Am. J. Gastroenterol. 102, 731–737 (2007). Pasha, S. F. et al. Double-balloon enteroscopy and capsule endoscopy have comparable diagnostic yield in small-bowel disease: a meta-analysis. Clin. Gastroenterol. Hepatol. 6, 671–676 (2008). One study included 100 consecutive patients with obscure bleeding [55]. Patients were categorized into three groups; the diagnostic yield of VCE was highest in the group with ongoing overt bleeding (92 percent), compared with those with previous overt bleeding (13 percent) or guaiac positive stools and iron deficiency anemia (44 percent). The most common findings were angiectasia (29 percent) and Crohn s disease (6 percent). Other factors associated with an increased yield of VCE include older age, male sex, current hospitalization, increasing transfusion requirements, and the presence of connective disuse disease [53,58]. Endoscopy May 15.")
22
Prior Capsule Endoscopy Improves the Diagnostic and Therapeutic Yield of Single-Balloon Enteroscopy.
retrospective analysis of a prospectively collected database at a tertiary-care academic medical center between 2011 and 2013 for all patients referred for SBE. RESULTS: 150 patients 170 SBE indications anemia, overt or occult gastrointestinal bleeding, and suspected mass. CE prior to SBE 113 of 150 patients (75 %). diagnostic yield for small-bowel disease by CE was 62 %. Therapeutic interventions included hemostasis, polypectomy, and foreign body removal. Total diagnostic and therapeutic yield of SBE was 60 and 28 %, respectively. The diagnostic yield of SBE with prior CE was 68 versus 44 % for SBE without prior CE (P 0.002). The therapeutic yield of SBE with prior CE was 35 versus 12 % without prior CE (P 0.001) CONCLUSIONS: SBE appears to be a safe and effective technique for the diagnosis and treatment of small-bowel disease; however, we recommend performing a CE prior to SBE to improve the diagnostic and therapeutic yield of the procedure. Delvaux, M., Fassler, I. & Gay, G. Clinical usefulness of the endoscopic video capsule as the initial intestinal investigation in patients with obscure digestive bleeding: validation of a diagnostic strategy based on the patient outcome after 12 months. Endoscopy 36, 1067–1073 (2004). Milano, A. et al. A prospective evaluation of iron deficiency anemia in the GI endoscopy setting: role of standard endoscopy, videocapsule endoscopy, and CT‑enteroclysis. Gastrointest. Endosc. 73, 1002–1008 (2011). Saperas, E. et al. Capsule endoscopy versus computed tomographic or standard angiography for the diagnosis of obscure gastrointestinal bleeding. Am. J. Gastroenterol. 102, 731–737 (2007). Pasha, S. F. et al. Double-balloon enteroscopy and capsule endoscopy have comparable diagnostic yield in small-bowel disease: a meta-analysis. Clin. Gastroenterol. Hepatol. 6, 671–676 (2008). One study included 100 consecutive patients with obscure bleeding [55]. Patients were categorized into three groups; the diagnostic yield of VCE was highest in the group with ongoing overt bleeding (92 percent), compared with those with previous overt bleeding (13 percent) or guaiac positive stools and iron deficiency anemia (44 percent). The most common findings were angiectasia (29 percent) and Crohn's disease (6 percent). Other factors associated with an increased yield of VCE include older age, male sex, current hospitalization, increasing transfusion requirements, and the presence of connective disuse disease [53,58]. Digetsive disease and science .
. diagnostic yield for small-bowel disease by CE was 62 %. Therapeutic interventions included hemostasis, polypectomy, and foreign body removal. Total diagnostic and therapeutic yield of SBE was 60 and 28 %, respectively. The diagnostic yield of SBE with prior CE was 68 versus 44 % for SBE without prior CE (P 0.002). The therapeutic yield of SBE with prior CE was 35 versus 12 % without prior CE (P 0.001) CONCLUSIONS: SBE appears to be a safe and effective technique for the diagnosis and treatment of small-bowel disease; however, we recommend performing a CE prior to SBE to improve the diagnostic and therapeutic yield of the procedure. Delvaux, M., Fassler, I. & Gay, G. Clinical usefulness of the endoscopic video capsule as the initial intestinal investigation in patients with obscure digestive bleeding: validation of a diagnostic strategy based on the patient outcome after 12 months. Endoscopy 36, 1067–1073 (2004). Milano, A. et al. A prospective evaluation of iron deficiency anemia in the GI endoscopy setting: role of standard endoscopy, videocapsule endoscopy, and CT‑enteroclysis. Gastrointest. Endosc. 73, 1002–1008 (2011). Saperas, E. et al. Capsule endoscopy versus computed tomographic or standard angiography for the diagnosis of obscure gastrointestinal bleeding. Am. J. Gastroenterol. 102, 731–737 (2007). Pasha, S. F. et al. Double-balloon enteroscopy and capsule endoscopy have comparable diagnostic yield in small-bowel disease: a meta-analysis. Clin. Gastroenterol. Hepatol. 6, 671–676 (2008). One study included 100 consecutive patients with obscure bleeding [55]. Patients were categorized into three groups; the diagnostic yield of VCE was highest in the group with ongoing overt bleeding (92 percent), compared with those with previous overt bleeding (13 percent) or guaiac positive stools and iron deficiency anemia (44 percent). The most common findings were angiectasia (29 percent) and Crohn s disease (6 percent). Other factors associated with an increased yield of VCE include older age, male sex, current hospitalization, increasing transfusion requirements, and the presence of connective disuse disease [53,58]. Digetsive disease and science. .")
23
Figure 1 | Algorithm for the use of capsule endoscopy to investigate occult, obscure gastrointestinal bleeding. aPerform the investigations in the sequence specified until underlying pathology has been identified. Abbreviations: Ce, capsule endoscopy; D2, second part of duodenum; eGD, esophagogastroduodenoscopy Some, but not all, studies report low rebleeding rates after negative compared with positive VCE findings.47 So-called second-look VCE after initial nondiagnostic testing has been proposed for conditions when haemoglobin levels decrease by >4 g and when obscure bleeding converts to overt haemorrhage Whether VCE improves outcomes is less certain. In one investigation, no differences in diagnostic workups, treatment or symptom resolution were observed in 193 individuals with positive, equivocal or negative VCE findings.52 In a study in which patients with gastrointestinal bleeding were randomly allocated to initial VCE or small bowel barium radiography, no differences were observed in subsequent diagnostic interventions, therapies or hospitalizations over a period of 12 months.53 capsule studies performed with intravenous heparin in controlled settings might unmask occult bleeding sources in selected cases, but should be considered only in centres in which endoscopic, angiographic or surgical support is immediately available in the event of uncontrolled bleeding.49

24
Cápsula en Crohn En Crohn establecido
Detección de más segmentos comprometidos En colitis indiferenciada, 15 % de detección de lesiones en ID En sospecha de Crohn, mejor rendimiento que otras técnicas (E-TAC, ileocolonoscopia, enteroscopia) Si calprotectina (-), muy bajo rendimiento Riesgo de retención de cápsula established Crohn’s disease detects new proximal small bowel lesions in half of patients. Another group noted findings of small bowel Crohn’s disease in 19 of 120 patients (16%) with indeterminate or presumed ulcerative colitis, showing that this technique can clarify the type of IBD present.56 Mehdizadeh, S. et al. Diagnostic yield of capsule endoscopy in ulcerative colitis and inflammatory bowel disease of unclassified type (IBDU). Endoscopy 40, 30–35 (2008). Dionisio, P. M. et al. Capsule endoscopy has a significantly higher diagnostic yield in patients with suspected and established small-bowel Crohn’s disease: a meta-analysis. Am. J. Gastroenterol. 105, 1240–1248 (2010). Koulaouzidis, A., Douglas, S., Rogers, M. A., Arnott, I. D. & Plevris, J. N. Fecal calprotectin: a selection tool for small bowel capsule endoscopy in suspected IBD with prior negative bi-directional endoscopy. Scand. J. Gastroenterol. 46, 561–566 (2011). Endoscopy 2008; 40, 30–35 Am J Gastroenterol. 2010; 105:1240-8 Scand J Gastroenterol. 2011;46:561-6
 Si calprotectina (-), muy bajo rendimiento. Riesgo de retención de cápsula. established Crohn’s disease detects new proximal small bowel lesions in half of patients. Another group noted findings of small bowel Crohn’s disease in 19 of 120 patients (16%) with indeterminate or presumed ulcerative colitis, showing that this technique can clarify the type of IBD present.56. Mehdizadeh, S. et al. Diagnostic yield of capsule endoscopy in ulcerative colitis and inflammatory bowel disease of unclassified type (IBDU). Endoscopy 40, 30–35 (2008). Dionisio, P. M. et al. Capsule endoscopy has a significantly higher diagnostic yield in patients with suspected and established small-bowel Crohn’s disease: a meta-analysis. Am. J. Gastroenterol. 105, 1240–1248 (2010). Koulaouzidis, A., Douglas, S., Rogers, M. A., Arnott, I. D. & Plevris, J. N. Fecal calprotectin: a selection tool for small bowel capsule endoscopy in suspected IBD with prior negative bi-directional endoscopy. Scand. J. Gastroenterol. 46, 561–566 (2011). Endoscopy 2008; 40, 30–35. Am J Gastroenterol. 2010; 105: Scand J Gastroenterol. 2011;46:")
25
Cápsula en Crohn: pros y cons
Small bowel capsule endoscopy • Complete visualization of the small bowel mucosa • Less invasive than conventional endoscopy High diagnostic yield for small mucosal lesions • Scores of severity need further validation in larger cohort of patients No mucosal sampling for histology • Costs • Recent validation of scores of severity (Niv and Lewis) • Bowel preparation • No transmural evaluation • Not widely available established Crohn’s disease detects new proximal small bowel lesions in half of patients. Another group noted findings of small bowel Crohn’s disease in 19 of 120 patients (16%) with indeterminate or presumed ulcerative colitis, showing that this technique can clarify the type of IBD present.56 Mehdizadeh, S. et al. Diagnostic yield of capsule endoscopy in ulcerative colitis and inflammatory bowel disease of unclassified type (IBDU). Endoscopy 40, 30–35 (2008). Dionisio, P. M. et al. Capsule endoscopy has a significantly higher diagnostic yield in patients with suspected and established small-bowel Crohn’s disease: a meta-analysis. Am. J. Gastroenterol. 105, 1240–1248 (2010). Koulaouzidis, A., Douglas, S., Rogers, M. A., Arnott, I. D. & Plevris, J. N. Fecal calprotectin: a selection tool for small bowel capsule endoscopy in suspected IBD with prior negative bi-directional endoscopy. Scand. J. Gastroenterol. 46, 561–566 (2011). Clin Exp Gastroenterol May 20;7: eCollection 2014.
 • Bowel preparation • No transmural evaluation • Not widely available established Crohn’s disease detects new proximal small bowel lesions in half of patients. Another group noted findings of small bowel Crohn’s disease in 19 of 120 patients (16%) with indeterminate or presumed ulcerative colitis, showing that this technique can clarify the type of IBD present.56. Mehdizadeh, S. et al. Diagnostic yield of capsule endoscopy in ulcerative colitis and inflammatory bowel disease of unclassified type (IBDU). Endoscopy 40, 30–35 (2008). Dionisio, P. M. et al. Capsule endoscopy has a significantly higher diagnostic yield in patients with suspected and established small-bowel Crohn’s disease: a meta-analysis. Am. J. Gastroenterol. 105, 1240–1248 (2010). Koulaouzidis, A., Douglas, S., Rogers, M. A., Arnott, I. D. & Plevris, J. N. Fecal calprotectin: a selection tool for small bowel capsule endoscopy in suspected IBD with prior negative bi-directional endoscopy. Scand. J. Gastroenterol. 46, 561–566 (2011). Clin Exp Gastroenterol May 20;7: eCollection")
26
Fecal calprotectin: a selection tool for small bowel capsule endoscopy in suspected IBD with prior negative bi-directional endoscopy Fecal calprotectin (FC) is a non-invasive marker of gastrointestinal inflammation with advocated diagnostic precision in distinguishing inflammatory bowel disease (IBD) from non-IBD diagnoses. To investigate the value of FC as a selection tool for further investigation of the small Scand J Gastroenterol May;46(5): doi: / Epub 2011 Jan 27.
 is a non-invasive marker of gastrointestinal inflammation with advocated diagnostic precision in distinguishing inflammatory bowel disease (IBD) from non-IBD diagnoses. To investigate the value of FC as a selection tool for further investigation of the small. Scand J Gastroenterol May;46(5): doi: / Epub 2011 Jan 27.")
27
23FC (≤ 50 μg/g) and in all those the SBCE was normal.
Patients referred with clinical suspicion of CD and negative bi-directional endoscopies. Only patients with FC results prior to the SBCE test were included; in cases of multiple FC determinations, the value closest to the SBCE date was selected. Medications history including usage of aspirin or non-steroidal anti-inflammatory drugs (NSAIDs) was made available for all patients. SBCE findings were analyzed against final diagnosis and FC values. RESULTS: 72 (53 females, 17 males) 23FC (≤ 50 μg/g) and in all those the SBCE was normal. 44FC >50 μg/g; in this group, 9 51 and 100 μg/g and all had a normal SBCE. 35 >100 μg/g; 15 (42.85%) compatible with FC levels 326 μg/g (range μg/g). A definitive clinical diagnosis of CD, based on subsequent follow-up, was made in 10/35 (28.5%) of patients. These 10 patients were within the subgroup of 15 patients with positive SBCE findings and had median FC levels 368 μg/g (range μg/g). CONCLUSIONS: FC >100 μg/g is good predictor of positive SBCE findings, while FC >200 μg/g was associated with higher SBCE yield (65%) and confirmed CD in 50% of cases. .
 was made available for all patients. SBCE findings were analyzed against final diagnosis and FC values. RESULTS: 72 (53 females, 17 males) 23FC (≤ 50 μg/g) and in all those the SBCE was normal. 44FC >50 μg/g; in this group, 9 51 and 100 μg/g and all had a normal SBCE. 35 >100 μg/g; 15 (42.85%) compatible with FC levels 326 μg/g (range μg/g). A definitive clinical diagnosis of CD, based on subsequent follow-up, was made in 10/35 (28.5%) of patients. These 10 patients were within the subgroup of 15 patients with positive SBCE findings and had median FC levels 368 μg/g (range μg/g). CONCLUSIONS: FC >100 μg/g is good predictor of positive SBCE findings, while. FC >200 μg/g was associated with higher SBCE yield (65%) and confirmed CD in 50% of cases. .")
28
Cápsula en tumores y pólipos ID
Hallazgo en 2-9% en cápsulas solicitadas por otra causa Estudio multicéntrico 5.129 2.4% tumores (2.2 primarios vs 0.2 metástasis) 32% GIST, 20% adeno Ca, 15% Carcinoides Herramienta útil en detección de pólipos ID en síndromes polipósicos Rondonotti, E. et al. Small-bowel neoplasms in patients undergoing video capsule endoscopy: a multicenter European study. Endoscopy 40, 488–495 (2008). Other small bowel neoplasms detected by VCE include lymphomas, neuroendocrine tumours and sarcomas. Endoscopy. 2008;40(6):
 32% GIST, 20% adeno Ca, 15% Carcinoides. Herramienta útil en detección de pólipos ID en síndromes polipósicos. Rondonotti, E. et al. Small-bowel neoplasms in patients undergoing video capsule endoscopy: a multicenter European study. Endoscopy 40, 488–495 (2008). Other small bowel neoplasms detected by VCE include lymphomas, neuroendocrine tumours and sarcomas. Endoscopy. 2008;40(6):")
29
Cápsula en niños Aprobada en > 10 años
Experiencias reportadas en > de 2 años u 11.5 kg Serie de 70 niños 2 a 10 años, las indicaciones fueron: 25% Crohn, 24% anemia ferropriva, 14% sangrado oculto, 16% Sd polipósicos, 10% GVH Meta análisis 15 estudios, 723 casos < 18 años Indicaciones 54% EII Rendimiento 65% Examen 86% completo, Retención 2.6% Dupont-Lucas, C. et al. Capsule endoscopy in children: which are the best indications? [French] Arch. Pediatrie 17, 1264–1272 (2010). Cohen, S. A. & Klevens, A. I. Use of capsule endoscopy in diagnosis and management of pediatric patients, based on meta-analysis. Clin. Gastroenterol. Hepatol. 9, 490–496 (2011). Clin Gastroenterol Hepatol. 2011;9:490-6.
. Cohen, S. A. & Klevens, A. I. Use of capsule endoscopy in diagnosis and management of pediatric patients, based on meta-analysis. Clin. Gastroenterol. Hepatol. 9, 490–496 (2011). Clin Gastroenterol Hepatol. 2011;9:")
30
Avances Técnicos Ajuste automatizado de luz (uniforme)
Mejor visualización periférica Cromoendoscopia virtual Indicador de sospecha de sangre (detección áreas rojas) Modulación en frecuencia de tomas Imagen en tiempo real light intensity is not modulated in relation to distance to the mucosa, was initially employed and resulted in glare with images of surfaces close to the lens and dim lighting of distant structures. By contrast, adaptive illumination provides automated illumination adjustment, providing uniform lighting regardless of distance to the mucosa. The earliest VCE capsule (the M2A®) included a single element lens that exhibited image distortion at the periphery, a property inherent in wide-angle lenses. Newer capsules (PillCam® SB2, PillCam® ESO2) employ multielement lenses with distortion-free fields of view to >156°.1,2 PillCam® SB2 software permits colour enhancement with a blue mode that removes red light. This capsule also offers an integrated flexible spectral imaging colour enhancement similar to the Fuji Intelligent Colour Enhancement (FICE; Fujinon, Tokyo, Japan) . Olympus Contrast Capsule software (Olympus, Tokyo, Japan) can produce strong contrast images using only the green and blue light to highlight vascular lesions (Figure 2) The latest version of the PillCam software has discontinued the ability to track the location of the capsule within the abdominal cavity because of poor accuracy. The ‘suspected blood indicator’ is a feature of the latest version of the RAPID™ software (Given Imaging, Yoqneam, Israel) developed for automated detection of red mucosal areas. However, the sensitivity of this technique for detection of lesions with bleeding potential is low (37%).10. although the clinical value of this feature is unclear since the sensitivity and specificity are poor The OMOM capsule can vary its frame rate to reduce views of the stomach and increase images in the small bowel
 Modulación en frecuencia de tomas. Imagen en tiempo real. light intensity is not modulated in relation to distance to the mucosa, was initially employed and resulted in glare with images of surfaces close to the lens and dim lighting of distant structures. By contrast, adaptive illumination provides automated illumination adjustment, providing uniform lighting regardless of distance to the mucosa. The earliest VCE capsule (the M2A®) included a single element lens that exhibited image distortion at the periphery, a property inherent in wide-angle lenses. Newer capsules (PillCam® SB2, PillCam® ESO2) employ multielement lenses with distortion-free fields of view to >156°.1,2. PillCam® SB2 software permits colour enhancement with a blue mode that removes red light. This capsule also offers an integrated flexible spectral imaging colour enhancement similar to the Fuji Intelligent Colour Enhancement (FICE; Fujinon, Tokyo, Japan) . Olympus Contrast Capsule software (Olympus, Tokyo, Japan) can produce strong contrast images using only the green and blue light to highlight vascular lesions (Figure 2) The latest version of the PillCam software has discontinued the ability to track the location of the capsule within the abdominal cavity because of poor accuracy. The ‘suspected blood indicator’ is a feature of the latest version of the RAPID™ software (Given Imaging, Yoqneam, Israel) developed for automated detection of red mucosal areas. However, the sensitivity of this technique for detection of lesions with bleeding potential is low (37%).10. although the clinical value of this feature is unclear since the sensitivity and specificity are poor. The OMOM capsule can vary its frame rate to reduce views of the stomach and increase images in the small bowel.")
31
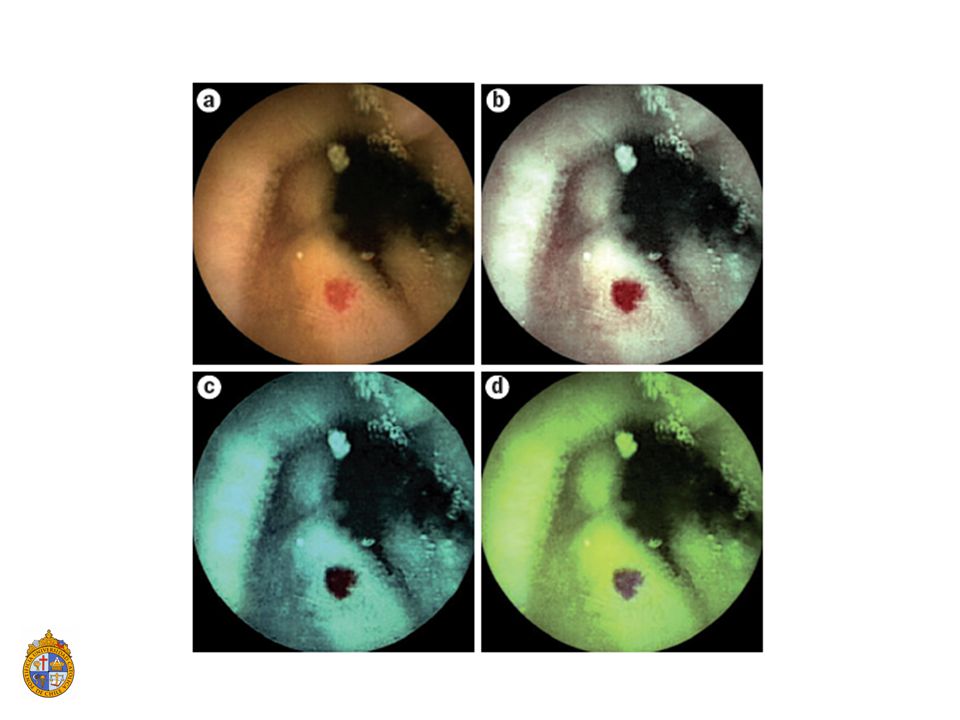
Figure 1 | Example FICE images of a small bowel adenoma
Figure 1 | Example FICE images of a small bowel adenoma. FICE images captured by video capsule endoscopy seen with a | conventional imaging b | FICE setting 1 (red 595 nm; green 540 nm; blue 535 nm), c | FICE setting 2 (red 420 nm; green 520 nm; blue 530 nm), d | FICE setting 3 (red 595 nm; green 570 nm; blue 415 nm). Abbreviation: FICE, Fujinon Intelligent Colour Enhancement.
, c | FICE setting 2 (red 420 nm; green 520 nm; blue 530 nm), d | FICE setting 3 (red 595 nm; green 570 nm; blue 415 nm). Abbreviation: FICE, Fujinon Intelligent Colour Enhancement.")
33
Olympus Contrast Capsule software (Olympus, Tokyo, Japan) can produce strong contrast images using only the green and blue light to highlight vascular lesions (Figure 2) Figure 2 | Enhanced characterization of mucosal vascularity using white-light illumination. Images show white-light illumination across all wavelengths compared with imaging within blue and green spectra. a | Small bowel submucosal vessels seen using white light of conventional imaging. b | The vasculature is distinctly visualized (arrow) in the dark green contrast image. Contrast technology is distinguished from the FICE technique by the postimaging processing, which is carried out on white-light images from a blue-enhanced white light LED rather than from a conventional white-light LED.
 in the dark green contrast image. Contrast technology is distinguished from the FICE technique by the postimaging processing, which is carried out on white-light images from a blue-enhanced white light LED rather than from a conventional white-light LED.")
34
Otras indicaciones Cápsula esofágica Cápsula colon
Esofagitis, Barrett, várices Cápsula colon Tamizaje pólipos PillCam™ eso (Given imaging), which is equipped with two cameras—one at each end (Figure 3)—that are capable of acquiring 14 images per second and have a battery life of 20 min -analysis involving nine studies (with a total of 618 patients) estimated that the pooled sensitivity and specificity for diagnosis of Barrett's esophagus were 77 and 86 percent, respectively [95]. The authors concluded that upper endoscopy remains the modality of choice for evaluation of suspected Barrett's esophagus. In addition, two economic analyses concluded that screening for Barrett's esophagus with the PillCam ESO was not cost-effective compared with standard screening with upper endoscopy colonic lumen is much larger than the diameter of PillCam™ sB (Given imaging), this capsule is unlikely to provide views of all the quadrants of the lumen. PillCam™ Colon (Given imaging) capsule (31 × 11 mm) was introduced, which has two cameras—one at each end, each with a frame rate of four images per second and a battery life of 10 h. obtain FDa approval in a dedicated bowel preparation for capsule colono scopy has been developed to ensure a clean colon Ce provided a diagnostic yield of 76% compared with 80% achieved by colonoscopy in the detection of polyps of any size. Guidelines issued by the European Society for Gastrointestinal Endoscopy suggest that colon capsule endoscopy is a reasonable alternative to colonoscopy for colorectal cancer screening in average-risk patients [103]. However, the guidelines do not recommend it for patients at increased risk for colon cancer (eg, those with a family or personal history of colon cancer) or for those with alarm symptoms (eg, anemia, rectal bleeding, weight loss). A study of a newer capsule (PillCam Colon 2) that has a wider angle of view (172 degrees per camera) and an adaptive frame rate that preserves battery life included 109 patients [110]. For detecting polyps that were 6 mm or larger, the capsule had a sensitivity of 84 percent and a specificity of 88 percent. For polyps 10 mm or larger, the sensitivity and specificity were 88 and 95 percent, respectively. Three of the patients had invasive cancer, all of which were detected by the capsule.
, which is equipped with two cameras—one at each end (Figure 3)—that are capable of acquiring 14 images per second and have a battery life of 20 min. -analysis involving nine studies (with a total of 618 patients) estimated that the pooled sensitivity and specificity for diagnosis of Barrett s esophagus were 77 and 86 percent, respectively [95]. The authors concluded that upper endoscopy remains the modality of choice for evaluation of suspected Barrett s esophagus. In addition, two economic analyses concluded that screening for Barrett s esophagus with the PillCam ESO was not cost-effective compared with standard screening with upper endoscopy. colonic lumen is much larger than the diameter of PillCam™ sB (Given imaging), this capsule is unlikely to provide views of all the quadrants of the lumen. PillCam™ Colon (Given imaging) capsule (31 × 11 mm) was introduced, which has two cameras—one at each end, each with a frame rate of four images per second and a battery life of 10 h. obtain FDa approval in a dedicated bowel preparation for capsule colono scopy has been developed to ensure a clean colon. Ce provided a diagnostic yield of 76% compared with 80% achieved by colonoscopy in the detection of polyps of any size. Guidelines issued by the European Society for Gastrointestinal Endoscopy suggest that colon capsule endoscopy is a reasonable alternative to colonoscopy for colorectal cancer screening in average-risk patients [103]. However, the guidelines do not recommend it for patients at increased risk for colon cancer (eg, those with a family or personal history of colon cancer) or for those with alarm symptoms (eg, anemia, rectal bleeding, weight loss). A study of a newer capsule (PillCam Colon 2) that has a wider angle of view (172 degrees per camera) and an adaptive frame rate that preserves battery life included 109 patients [110]. For detecting polyps that were 6 mm or larger, the capsule had a sensitivity of 84 percent and a specificity of 88 percent. For polyps 10 mm or larger, the sensitivity and specificity were 88 and 95 percent, respectively. Three of the patients had invasive cancer, all of which were detected by the capsule.")
35
Riesgos Retención de cápsula Marcapasos, resincronizadores o DAI
F.R: Crohn, cirugías abdominales, radioterapia, AINES Se recomiendan imágenes en pacientes de alto riesgo Cápsula biodegradable Marcapasos, resincronizadores o DAI Malfuncionamiento dispositivo cardiaco (teórico!!!) Deterioro calidad de imagen (raro!!) Falla transmisión imagen (raro!!) VCE is an extremely safe technology. No deaths have been attributed to the device, despite more than a million ingestions the biodegradable capsule of the agile™ Patency system (Given imaging) was developed specifically to identify patients at high risk of capsule retention and impaction. this capsule measures 26 × 11 mm and is composed of lactose and barium that contains a radiofrequency identification tag that can be detected by a scanning device placed on the abdominal wall or by a plain abdominal film. The biodegradable plugs at each end start to dissolve after 30 hours, and fully dissolve 40 to 80 hours after ingestion In ex vivo studies, no interference with cardiac pacemaker or defibrillator function was observed when VCE devices were placed in close proximity.29 Patients with cardiac pacemakers or other implanted electromedical devices are generally considered unsuitable for Ce because of the risks of mutual interference. specifically, three problems have been envisaged in this group of patients: malfunction of the cardiac pacemaker caused by the capsule, impairment of the quality of the image acquired by the capsule and failure to transmit the images collected.
 Deterioro calidad de imagen (raro!!) Falla transmisión imagen (raro!!) VCE is an extremely safe technology. No deaths have been attributed to the device, despite more than a million ingestions. the biodegradable capsule of the agile™ Patency system (Given imaging) was developed specifically to identify patients at high risk of capsule retention and impaction. this capsule measures 26 × 11 mm and is composed of lactose and barium that contains a radiofrequency identification tag that can be detected by a scanning device placed on the abdominal wall or by a plain abdominal film. The biodegradable plugs at each end start to dissolve after 30 hours, and fully dissolve 40 to 80 hours after ingestion. In ex vivo studies, no interference with cardiac pacemaker or defibrillator function was observed when VCE devices were placed in close proximity.29 Patients with cardiac pacemakers or other implanted electromedical devices are generally considered unsuitable for Ce because of the risks of mutual interference. specifically, three problems have been envisaged in this group of patients: malfunction of the cardiac pacemaker caused by the capsule, impairment of the quality of the image acquired by the capsule and failure to transmit the images collected.")
36
Contraindicaciones (eventuales)
Demencia Estenosis o divertículo esofágico Gastroparesia Obstrucción intestinal Pacientes que rechacen o no sean candidatos a cirugía Embarazo

37
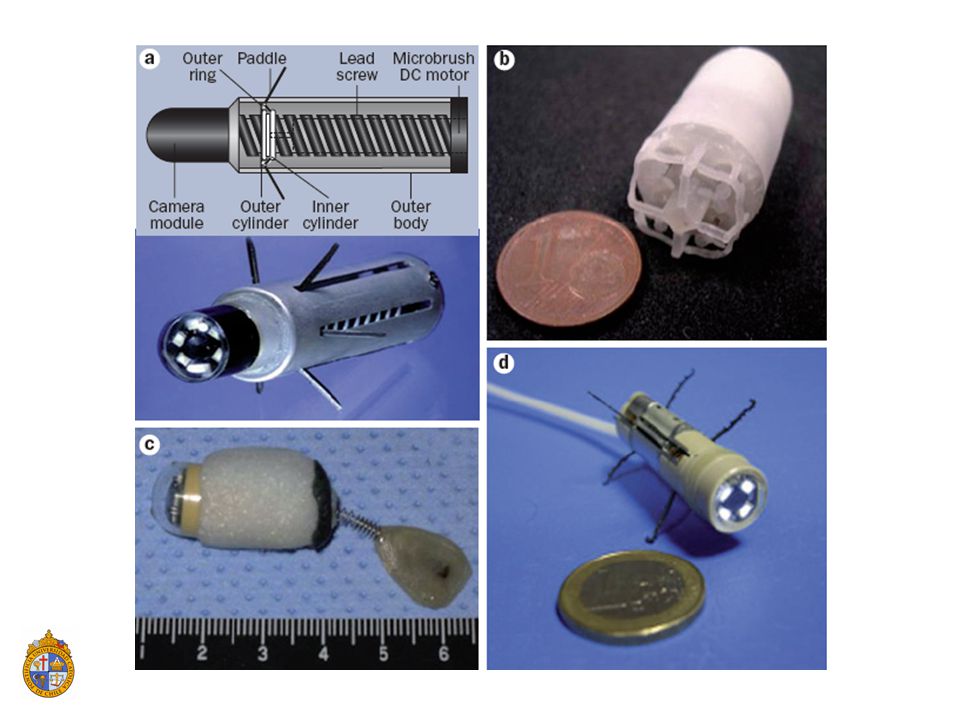
Innovaciones en estudio
Mayor duración de la batería y ahorro de energía Movimiento dirigido Dirección magnética externa Autopropulsión y anclaje Insuflación Marcaje, biopsias, tratamiento lithium batteries can provide longer operating times than silveroxide batteries and carbon nanotubebased systems will not only improve power supply, but they will also reduce required battery space. Power saving, for instance, when the capsule proceeds slowly, the frame collection rate would be reduced. Drawbacks of the current VCE methods include an inability to direct the capsule towards pathology or backwards to revisit mucosal abnormalities. Several prototypes of self-propelled capsules have been devised

Presentaciones similares








 Noviembre de 2004.>")










