Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Departamento de Farmacología, Toxicología y Farmacodependencia Facultad de Farmacia UCR.
AMINOGLICÓSIDOS Dra. Beatriz Badilla II ciclo 2009 1

2
Selman Abrahan Waksman USA
The Nobel Prize in Physiology or Medicine 1952 “for his discovery of streptomycin, obteined from Streptomyces griseus,the first antibiotic effective againts tuberculosis” Selman Abrahan Waksman USA

3
Aminociclitol

4
Estreptomycina 1943 Neomycina 1949

5
GentamYcina (1953) Amikacina (1972) TobramYcina (1970)
 Amikacina (1972) TobramYcina (1970)")
6
Aminoglicósidos y aminociclitoles
6 Farmacóforo un anillo aminociclitol, específicamente 1,3 diamino inositol La mayoría de funciones alcohólicas están sustituidas con enlaces glicosídicos con aminoazúcares característicos “pseudosacáridos” 2-Desoxiestreptamina Estreptamina 2-Desoxiestreptamina Espectinamina 6

7
Agentes específicos Amikacina: derivado acilo de kanamicina A
7 Amikacina: derivado acilo de kanamicina A L-hidroxiamino-buterilamida en N-3 inhiben adenilación y fosforilación. Disminución de la unión a las enzimas codificadas por el factor R Potencia amplia y espectro Compite con Gentamicina para el tx de M. tuberculosis (cepas sensibles) Yersenia tularensis Pseudomona aeruginosa resistentes a otros agentes 7
 Yersenia tularensis. Pseudomona aeruginosa resistentes a otros agentes. 7.")
8
Agentes específicos Tobramicina análogo de kanamicina B sin 3´-OH
8 Tobramicina análogo de kanamicina B sin 3´-OH Fermentación de Micromonospora purpurea Mayor espectro que Kanamicina B (no sensible a fosforilación) IV para infecciones, especialmente Pseudomona aeruginosa resistente a Gentamicina No existe en presentación parenteral en CR, sin embargo se usa en colirios. 8
 IV para infecciones, especialmente Pseudomona aeruginosa resistente a Gentamicina. No existe en presentación parenteral en CR, sin embargo se usa en colirios. 8.")
9
Gentamicina -Sisomicina derivado de gentamicina C1a
9 -Sisomicina derivado de gentamicina C1a -Netilmicina derivado de Sisomicina 9

10
Mecanismo de acción

11
Mecanismo de acción

12
Ingreso de AMG a la célula bacteriana
Tres fases bien definidas Fase de unión iónica superficial Fase I dependiente de energía Fase 2 dependiente de energía Mella S. et al. Aminoglucósidos. Rev Chil. Infect. 2004: 21 (4):
:")
13
Vakulenko S and Mobashery S. Clin Microbiology Reviews. 2003:p435-450
Mecanismo de acción Aminoglycoside Proton motive trnasfer Eflux Outer wall Cytoplasmic membraner Cell wall (G+) or Outer envelope(G-) Reduded or No entry of aminoglycoside Periplasmic space Porin channel Hiperosmolaridad Cationes divalentes Anaerobiosis Reducción de pH Ca++ Mg++ 1 Fase I 2 Fuerza proton motriz Fase 2 3 Mella S. et al. Aminoglucósidos. Rev Chil. Infect. 2004: 21 (4): Vakulenko S and Mobashery S. Clin Microbiology Reviews. 2003:p
 or. Outer envelope(G-) Reduded or. No entry of. aminoglycoside. Periplasmic. space. Porin. channel. Hiperosmolaridad. Cationes divalentes. Anaerobiosis. Reducción de pH. Ca++ Mg++ 1. Fase I. 2. Fuerza proton. motriz. Fase Mella S. et al. Aminoglucósidos. Rev Chil. Infect. 2004: 21 (4): Vakulenko S and Mobashery S. Clin Microbiology Reviews. 2003:p")
14
Inhibition of 30S ribosome-RNAcomplex formation
Inh. Sintesis proteica Lectura errónea del mRNA e incorporación aa incorrectos en la proteína defectuosa

15
Fourmy et al. Structural basis of Aminoglycoside Action 2001

16
Mecanismos de resistencia de los AMG
Alteración del sitio blanco Mutación de las proteínas ribosomales o del ARN 16S. 2. Reducida acumulación intracelular del AMG Bombas de eflujo Impermeabilidad de la membrana externa Biofilm (Pseudomonas spp). Inactivación por enzimas modificadoras de AMG Acetiltransferasas Adeniltrasferasas Fosfotransferasas 4. Metilación postranscripcional de ARNr *** Mella S. et al. Aminoglucósidos. Rev Chil. Infect. 2004: 21 (4):
. Inactivación por enzimas modificadoras de AMG. Acetiltransferasas. Adeniltrasferasas. Fosfotransferasas. 4. Metilación postranscripcional de ARNr *** Mella S. et al. Aminoglucósidos. Rev Chil. Infect. 2004: 21 (4):")
17
Mecanismos de resistencia a AMG

18
Bacterias anaeróbicas?
R cruzada con todos los AMG Excepto ESTREPTOMICINA AMG → S con Peni y Vanco para Enterococcus faecioun E. faecalis Bacterias anaeróbicas?

19
Características farmacocinéticas de los aminoglicósidos
Antibiótico Tmax (h) Semivida (h) Activo en orina (%) Estreptomicina Gentamicina Tobramicina Netilmicina Amikacina Sisomicina Dibekacina 0.5-1 2-3 2-2.5 50-70 80-90 80-95 70-75 75-85 70-100 Vd= 0.25 L/kg Gilbert D. et al. The Sanford Guide 2009 p179
 Semivida (h) Activo en. orina (%) Estreptomicina. Gentamicina. Tobramicina. Netilmicina. Amikacina. Sisomicina. Dibekacina Vd= 0.25 L/kg. Gilbert D. et al. The Sanford Guide 2009 p179.")
20
Características farmacocinéticas de los aminoglicósidos
Absorción v.o. Categoría en embarazo D

21
Características farmacocinéticas de los aminoglicósidos
“Las concentraciones plasmáticas máximas se alcanzan a los min de la aplicación IM y son semejantes a las observadas 30 min después de concluir el goteo iv de una dosis igual en un lapso de 30 min. G&G .11 Ed. Cap 45.

22
Aminoglycoside Penetration into Various Tissues
(50-90%)* (30%)
* (30%)")
23
Endolinfa y perilinfa de oído interno Alta concentración Corteza renal

24
Factores que afectan el Vd
Obesidad Obesidad mórbida Vd= 0.25 L/kg Fibrosis quística Quemaduras Dism. T ½ ↑eliminación Sanford Guide 39 th ed 2009 p179

25
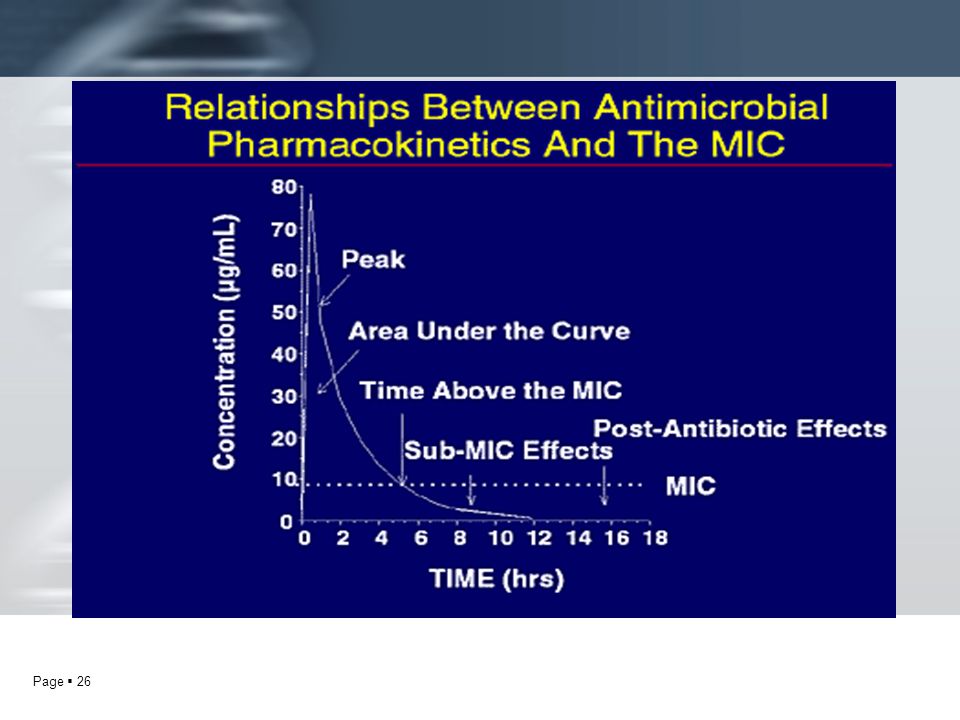
El efecto bactericida y postantibiótico de los AMG es dependiente
de la concentración alcanzada

27
G &G.Las Bases Farmacológicas de la Terapéutica. 11th ed 2006
Concentraciones plasmáticas (ug/ml) después de administrar gentamicina 5.1 mg/kg i.v. G &G.Las Bases Farmacológicas de la Terapéutica. 11th ed 2006
 después de administrar gentamicina 5.1 mg/kg i.v. G &G.Las Bases Farmacológicas de la Terapéutica. 11th ed")
28
Traditional dosing (q 8 hours) Once daily dosing (q 24 hours)
Bates & Nahata. Once Daily Aminoglycosides. Ann. Pharmacother.1994

29
Aberg et al. Infectious Diseases Handbook 6ª ed. p 843

30
The Sanford Guide 39th Ed 2009. pp 96,179
Table 10D Table 17 The Sanford Guide 39th Ed pp 96,179

31
Dosis de carga de aminoglicósidos
Gentamicina Tobramicina Amikacina Fármaco 2 mg/kg 7.5 mg/kg Dosis Dosis mútiple diaria (MDD) Gentamicina Tobramicina Amikacina Fármaco 1.7 mg/kg/8h 7.5 mg/kg/12h Dosis Gilbert D. et al. The Sanford Guide 39Th ed.2009 p96
 Gentamicina. Tobramicina. Amikacina. Fármaco. 1.7 mg/kg/8h. 7.5 mg/kg/12h. Dosis. Gilbert D. et al. The Sanford Guide 39Th ed.2009 p96.")
32
Dosis aminoglicósidos (DMD)
ITU Sinergia Infección severa Gentamicina 1.5 mg/kg/8 h 3 mg/kg 7 mg/kg/dia Dosis Lacy C. et al.Drug Information p749

33
Gentamicina Dosis (mg/kg)/ 24h
Dosis de los aminoglicósidos (OD) Gentamicina Dosis (mg/kg)/ 24h Sandforf 2009 HSJD 5.1 (7 crítico) 240 mg/día Gilbert D. et al. The Sanford Guide 39Th ed.2009 p96
 Gentamicina. Dosis (mg/kg)/ 24h. Sandforf HSJD. 5.1 (7 crítico) 240 mg/día. Gilbert D. et al. The Sanford Guide 39Th ed.2009 p96.")
34
Todos los pacientes requieren DC independientemente
de su función renal Dosis de mantenimiento: % de DC de acuerdo al aclaramiento de creatinina y al intervalo de dosis deseado (DDM)
")
35
Concentraciones séricas deseables
Gentamicina Tobramicina Amikacina 4-10 15-30 < 2. 2-5 Fármaco Pico ( g/ml) Valle ( g/ml) 16-24 56-64 MDD ODD Pacientes >65 a no deben recibir dosis de mantenimiento antes de 12 horas
 Valle ( g/ml) MDD. ODD. Pacientes >65 a no deben recibir dosis de. mantenimiento antes de 12 horas.")
36
SATURABLE TRANSPORT SYSTEM
HIGH CONCENTRATION Traditional/ODD Peak AG Serum Renal Proximal Tubular Cell Bates & Nahata. Once Daily Aminoglycosides. Ann. Pharmacother.1994

37
SATURABLE TRANSPORT SYSTEM
LOW SERUM CONCENTRATION Traditional Trough/Pre AG Serum Renal Proximal Tubular Cell Bates & Nahata. Once.Daily Aminoglycosides. Ann,. Pharmacother.1994

38
SATURABLE TRANSPORT SYSTEM
AMINOGLICOCID FREE INTERVAL Once-Daily Dosing Trough/Pre AG Serum Renal Proximal Tubular Cell Bates & Nahata. Once.Daily Aminoglycosides. Ann. Pharmacother.1994

39
Desvantajas potenciales
Proposed theoretical benefits and potential disadventages of the once-daily dosing of aminogrycosides Beneficios teóricos Disminución de la toxicidad Mejora de la terapia a traves de la optimización de la pk. Niveles plasmáticos “menores” Ventajas farmacoeconómicas Resitencia adaptativa Desvantajas potenciales Aumento de la toxicidad (?) Pediátricos Neutropénicos geriátricos Disfunción renal (?) Bates & Nahata. Once.Daily Aminoglycosides. Ann,. Pharmacother.1994
 Pediátricos Neutropénicos geriátricos. Disfunción renal ( ) Bates & Nahata. Once.Daily Aminoglycosides. Ann,. Pharmacother")
40
Beneficios del régimen “una vez al dìa” de aminoglósidos
El régimen Dosis única la día es igualmente eficaz y tan seguro como el múltiple. Dosis única al día es más fácil de aplicar y menos costoso en el ambiente hospitalario. Dosis única al día es la indicada excepto en embarazo, neonatos y en pediatría. Bates & Nahata. Once.Daily Aminoglycosides. Ann,. Pharmacother.1994 G &G.Las Bases Farmacológicas de la Terapéutica. 11th ed 2006

41
Eliminación por FG casi completamente. Muy poca reabsorción tubular
Eliminación de los AMG Eliminación por FG casi completamente. Muy poca reabsorción tubular Saturación 30-700h

42
de los aminoglicósidos
Efectos adversos más importantes de los aminoglicósidos

43
“La toxicidad puede considerarse un fenómeno
umbral que tiene mas probabilidades de ocurrir cuando la concentración plasmática excede durante mayor tiempo un limite superior relativamente seguro” Barclay, et al. Clin Pharmacokinet :

44
Endolinfa y perilinfa de oído interno Alta Concentración t 1/2 5-6 v mayores que en plasma

45
Ototoxicidad Hasta 20%. Factores predisponentes 1 2 3 4
El grado de lesión correlaciona con el número irreversible de células sensoriales dañado. Lesión COCLEAR Tinnitus Hipoacusia (frecuencias altas, luego bajas) Pérdida de audición 1 2 3 4 Lesión VESTIBULAR Inicia en laberinto. Nausea, vómito, mareo, pérdida del equilibrio, vértigo, nistagmos. Laberintitis crónica. (persitencia hasta por 2 m). Recuperación m Hasta 20%. Factores predisponentes
 Pérdida de audición Lesión VESTIBULAR. Inicia en laberinto. Nausea, vómito, mareo, pérdida del equilibrio, vértigo, nistagmos. Laberintitis crónica. (persitencia hasta por 2 m). Recuperación m. Hasta 20%. Factores predisponentes.")
46
Figure 1. Drawing of the Outer, Inner, and Middle Ear
Figure 1. Drawing of the Outer, Inner, and Middle Ear. Sound waves are captured by the auricle and conveyed through the external acoustic duct to the tympanic membrane, causing this membrane to vibrate. These vibrations are transmitted through the auditory ossicles of the middle ear to the footplate of the stapes, which is anchored in the oval window of the vestibule of the cochlea. Willems P. N Engl J Med 2000;342:

47
Hotson, J. R. et al. N Engl J Med 1998;339:680-685
Schematic Drawing of the Bony Labyrinth Containing the Vestibular and Auditory Sensory Organs Figure 2. Schematic Drawing of the Bony Labyrinth Containing the Vestibular and Auditory Sensory Organs. The otolithic organs (utricle and saccule) lie in the vestibule. The internal auditory artery divides into the common cochlear artery and the anterior vestibular artery. The anterior vestibular artery provides the blood supply to the anterior and horizontal semicircular canals but not to the cochlea. Isolated occlusion of the anterior vestibular artery may therefore cause acute vestibular syndrome without hearing loss.5,8,16,17 Hotson, J. R. et al. N Engl J Med 1998;339:
 lie in the vestibule. The internal auditory artery divides into the common cochlear artery and the anterior vestibular artery. The anterior vestibular artery provides the blood supply to the anterior and horizontal semicircular canals but not to the cochlea. Isolated occlusion of the anterior vestibular artery may therefore cause acute vestibular syndrome without hearing loss.5,8,16,17. Hotson, J. R. et al. N Engl J Med 1998;339:")
48
The Cochlea Figure 2. The Cochlea. The cochlear duct is embedded in the perilymph. It is filled with endolymph and contains the organ of Corti between the tectorial and the basilar membranes. The relative movement of the two membranes leads to deflection of the stereocilia of the inner hair cells (one row) and the outer hair cells (three rows), which generates the influx of potassium ions through channels at the tip links of the stereocilia. Mutations in the {alpha}-tectorin gene probably impair the function of the tectorial membrane as a resonator. The hair cell is the mechanoelectrical transducer that produces an electrical signal that is transmitted through nerve fibers and the spinal ganglion to the cochlear nerve and the auditory cortex of the brain. The influx of potassium ions from the endolymph activates the hair cells, which leads to stimulation of the underlying nerve cells that convey the auditory signal to the auditory cortex. The potassium ions probably leave the hair cells at their basolateral side through potassium channels formed by the KCNQ4 gene product and enter the supporting cells. The potassium ions then flow through these cells and the cochlear fibrocytes to the stria vascularis by means of connexins. There they are secreted back into the endolymph through another potassium channel formed by the KCNQ1 and KCNE1 gene products. Epithelial supporting cells that express connexin 26 are shown in red. Willems P. N Engl J Med 2000;342:
 and the outer hair cells (three rows), which generates the influx of potassium ions through channels at the tip links of the stereocilia. Mutations in the {alpha}-tectorin gene probably impair the function of the tectorial membrane as a resonator. The hair cell is the mechanoelectrical transducer that produces an electrical signal that is transmitted through nerve fibers and the spinal ganglion to the cochlear nerve and the auditory cortex of the brain. The influx of potassium ions from the endolymph activates the hair cells, which leads to stimulation of the underlying nerve cells that convey the auditory signal to the auditory cortex. The potassium ions probably leave the hair cells at their basolateral side through potassium channels formed by the KCNQ4 gene product and enter the supporting cells. The potassium ions then flow through these cells and the cochlear fibrocytes to the stria vascularis by means of connexins. There they are secreted back into the endolymph through another potassium channel formed by the KCNQ1 and KCNE1 gene products. Epithelial supporting cells that express connexin 26 are shown in red. Willems P. N Engl J Med 2000;342:")
49
Destrucción progresiva de las células
OTOTOXICIDAD Destrucción progresiva de las células sensoriales vestibulares y cocleares que tienen alta sensibilidad a la lesión causada por los AMG

50
OTOTOXICIDAD El mecanismo de ototoxicidad está relacionado con la generación de radicales libres en el oído interno con el subsecuente daño permanente en las células sensoriales y las neuronas resultando en pérdida de la audición. Hasta 25 % Selimoglu E..Aminoglycoside-induced ototoxicity. Curr Pharm Des. 2007; 13(1):119-26
:")
51
Apoptosis ( vía caspasas)
Mecanismos Entrada a través de canales mecano-eléctricos AG-Fe .Reacción con donadores de electrones (AA). ROS ( H2O2). Apoptosis ( vía caspasas) Ototoxicity L P Rybak and V Ramkumar.Kidnmey . Kidney International (2007) 72, 931–935;
. ROS ( H2O2). Apoptosis ( vía caspasas) Ototoxicity. L P Rybak and V Ramkumar.Kidnmey. . Kidney International (2007) 72, 931–935;")
52
Arguedas Q. Aminoglicósidos. 2004 Nº38. AMP
!!! Vancomicina Arguedas Q. Aminoglicósidos Nº38. AMP

53
Causes of Subjective and Objective Tinnitus
Table 1. Causes of Subjective and Objective Tinnitus. Lockwood, A. H. et al. N Engl J Med 2002;347:

54
Oscilopsia Bilateral vestibulopathy occurs when the balance portions of both inner ears are damaged. The symptoms typically include imbalance and visual problems. The imbalance is worse in the dark or in situations where footing is uncertain. Spinning vertigo is unusual. The visual symptoms, called oscillopsia, only occur when the head is moving. The illustration to the right shows what a person with bilateral vestibulopathy may see when driving over a bumpy road. Oscillopsia is often common during walking (Freyss et al, 1988). Quick movements of the head are associated with transient visual blurring. .
. Quick movements of the head are associated with transient visual blurring. .")
55
Typical audiogram of person exposed to gentamicin
Typical audiogram of person exposed to gentamicin. Hearing is commonly normal through 4000 Hz, and then falls off at higher frequencies. Often, persons with significant vestibular damage from gentamicin do not notice any change in their hearing.

56
Clasificación de ototoxicidad
Estreptomicina Gentamicina V V-C Tobramicina Kanamicina Amicacina Neomicina Netilmicina menor ototoxicidad C Clínica ?

57
Alta concentración (5-50v) Corteza renal
 Corteza renal")
58
8-26%* NEFROTOXICIDAD Es el resultado de la acumulación del AMG
en las células del túbulo proximal. Aronoff et al Antimicrob.Agents Chemother. *Morales et al. Mecanismos implicados en la nefrotoxicidad producida por AMG. Nefrología XX (5) 2000.
")
59
*Morales et al. Mecanismos implicados en la nefrotoxicidad producida por AMG. Nefrología XX (5) 2000.
")
60
OTOTOXICIDAD Mecanismos Fallo renal
Transporte a través de células en borde de cepillo. Unión a fosfatidil inositol Internalización Acumulación en lisosomas OTOTOXICIDAD Inhibición de PL-C. Activación S-R-A-A Inh. de Na+ /K+/ATPasa Lib Radicales libres Fallo renal 60 60

61
EFECTOS ↓FG ↑Cr plas. ↑BUN ↑ Enzimas tubulares
(alanina aminopeptidasa, beta-D-glucosamina, fosfatasa alcalina) Proteinuria 2 Microglobulina Modificación del sedimento urinario (Cilindruria Leucociuria) ↓FG ↑Cr plas. ↑BUN NAG N-acetil-beta-D-gliocosaminidasa
 Proteinuria. 2 Microglobulina. Modificación del sedimento. urinario. (Cilindruria. Leucociuria) ↓FG ↑Cr plas. ↑BUN. NAG. N-acetil-beta-D-gliocosaminidasa.")
62
Tubular-Cell Injury and Repair in Ischemic Acute Renal Failure
Figure 3. Tubular-Cell Injury and Repair in Ischemic Acute Renal Failure. After ischemia and reperfusion, morphologic changes occur in the proximal tubules, including loss of the brush border, loss of polarity, and redistribution of integrins and Na /K -ATPase to the apical surface. Calcium, reactive oxygen species, purine depletion, and phospholipases probably have a role in these changes in morphology and polarity as well as in the subsequent cell death that occurs as a result of necrosis and apoptosis. There is a sloughing of viable and nonviable cells into the tubular lumen, resulting in the formation of casts and luminal obstruction and contributing to the reduction in the glomerular filtration rate. The severely damaged kidney can completely restore its structure and function. Spreading and dedifferentiation of viable cells occur during recovery from ischemic acute renal failure, which duplicates aspects of normal renal development. A variety of growth factors probably contribute to the restoration of a normal tubular epithelium. Thadhani, R. et al. N Engl J Med 1996;334:

63
Arguedas Q. Aminoglicósidos. 2004 Nº38. AMP

64
Drugs Associated with Acute Renal Failure
Table 1. Drugs Associated with Acute Renal Failure. Thadhani, R. et al. N Engl J Med 1996;334:

65
REVERSIBLE AJUSTE DE DOSIS Cuadro aumentado en:
P.geriátrico I.R. previa Depleción de Na, K Fármacos nefrotóxicos. Mujeres Acidosis metabólica Enfermedad hepática REVERSIBLE AJUSTE DE DOSIS

66
Neomicina Kanamicina Amikacina Gentamicina Tobramicina
BLOQUEO NEUROMUSCULAR Neomicina Kanamicina Amikacina Gentamicina Tobramicina Inhibición de la liberación de Ach presináptica. Reducción de la sensibilidad al neurotransmisor

67
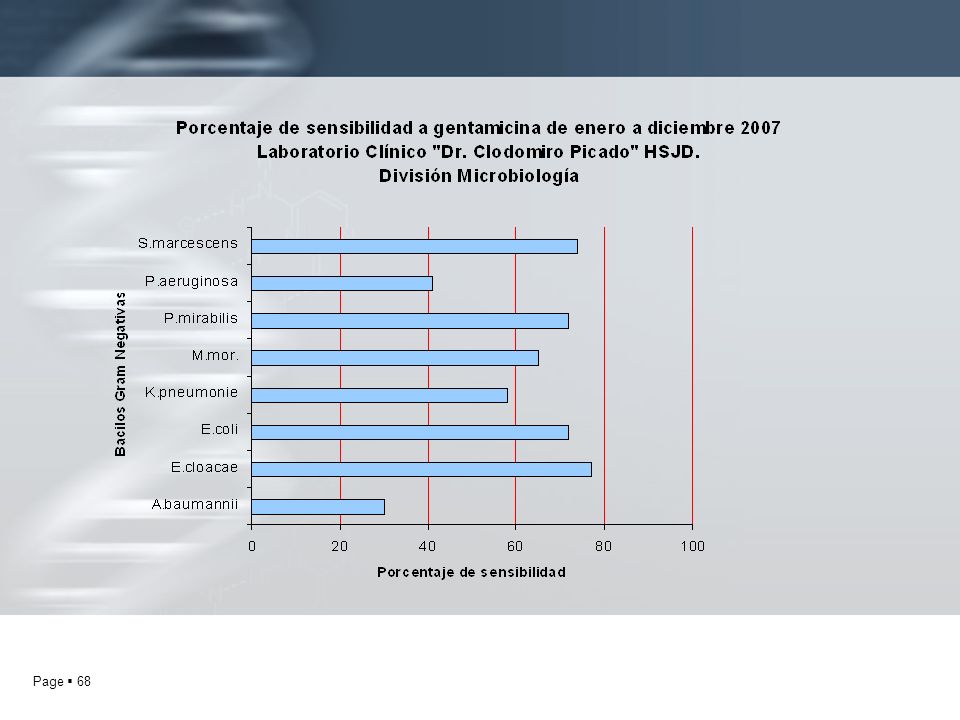
Gilbert D. et al. The Sanford Guide 39 th Ed. 2009. p71
Espectro de actividad Gram (-) Moraxella catharralis H. influenzae E. coli Klebsiella pneunonie Enterobacter sp Shigella Proteus mirabilis Pseudomona aeruginosa Francisella tularensis (E) Vibrio cholerae Pausterella pestis Mycobacterium tuberculosis Cocos Gram (+) Staph aureus MS Enterococcus S L. monocytogenes Gilbert D. et al. The Sanford Guide 39 th Ed p71
 Moraxella catharralis. H. influenzae. E. coli. Klebsiella pneunonie. Enterobacter sp. Shigella. Proteus mirabilis. Pseudomona aeruginosa. Francisella tularensis (E) Vibrio cholerae. Pausterella pestis. Mycobacterium tuberculosis. Cocos Gram (+) Staph aureus MS. Enterococcus S. L. monocytogenes. Gilbert D. et al. The Sanford Guide 39 th Ed p71.")
70
Do we still need the aminoglycosides?
Int J Antimicrob Agents. 2009; 33(3):201-5 Aminoglycoside-induced ototoxicity. Curr Pharm Des. 2007; 13(1):119-26 Selimoglu E
: Aminoglycoside-induced ototoxicity. Curr Pharm Des. 2007; 13(1): Selimoglu E.")
71
Infecciones serias por Gram (-) Endocarditis enterocóccica
USO CLÍNICO Infecciones por Enterococcus faecium o faecalis Peni + AMG Vanco+ AMG Infecciones por Enterobacterias Infecciones serias por Gram (-) Endocarditis enterocóccica
 Endocarditis enterocóccica.")
72
ITU Infecciones crónicas Neumonía Septicemia Peritonitis
USO CLÍNICO ITU Infecciones crónicas Neumonía Septicemia Peritonitis Tularemia Francisella tularensis E GENTA 5 mg/kg/día x 10 d.

Presentaciones similares









 Noviembre de 2004.>")










