Descargar la presentación
La descarga está en progreso. Por favor, espere

1
PERSPECTIVAS DE FUTURO EN EL TRATAMIENTO DE LOS
TRASTORNOS BIPOLARES CURSOS DE FORMACIÓ MÈDICA CONTINUADA PROGRAMA INFORMED DESCENTRALITZAT HOSPITAL UNIVERSITARI SON DURETA Antoni Benabarre Programa de Trastorns Bipolars Institut Clínic de Neurociències Hospital Clínic de Barcelona

3
Programa de Trastornos Bipolares
ASISTENCIA, DOCENCIA, INVESTIGACIÓN, GESTIÓN Clínica Neurobiología Terapéutica Farmacología Psicoeducación Terapia familiar grupo Estudios abiertos Ensayos clínicos Subtipos Suicidio Genética Neuropsicología Comorbilidad Comorbidity Neuromoduladores Neuroimagen

4
Trastorno Bipolar Incidencia del 1.5% al 2% de la población adulta
23/03/2017 Trastorno Bipolar Incidencia del 1.5% al 2% de la población adulta 4ª causa de discapacidad neuropsiquiátrica en todo el mundo Clínica y genéticamente heterogénea La mayoría de pacientes inicialmente mal diagnosticados Aproximadamente del 10% al 15% de los pacientes con Trastorno Bipolar no tratados llevan a cabo el suicidio Bipolar Disorder — Overview Lifetime incidence in EU countries reported to be 1.5% to 2%1 Recognition and definition of bipolar disorder have broadened in recent years—prevalence may be as high as 5% to 7%1,2 Bipolar disorder has a huge negative impact on professional and interpersonal functioning2 Fourth leading cause of neuropsychiatric disability worldwide3 Misdiagnosis is common According to one survey, 69% of bipolar disorder patients were initially misdiagnosed2 The consequences of ineffective recognition and treatment are dire for those who have bipolar disorder4 As many as 25% to 50% of bipolar patients attempt suicide2 Approximately 10% to 15% of bipolar patients commit suicide5 References: 1. Pini S, de Queiroz V, Pagnin D, et al. Prevalence and burden of bipolar disorders in European countries. Eur Neuropsychopharmacol. In press. 2. Glick ID. Undiagnosed bipolar disorder: new syndromes and new treatments. Prim Care Companion J Clin Psychiatry. 2004;6: World Health Organization. The World Health Report 2001—Mental Health: New Understanding, New Hope. Chapter 2: Burden of Mental and Behavioural Disorders. Available at: Accessed February 9, NIMH. Bipolar Disorder Research. Bethesda (MD): National Institute of Mental Health, National Institutes of Health, US Department of Health and Human Services; Available at: 5. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed., Text Revision. Washington, DC: American Psychiatric Association; 2000. Pini S et al. Eur Neuropsychopharmacol. In press. Glick ID. Prim Care Companion J Clin Psychiatry. 2004;6:27-33. World Health Organization NIMH. Bipolar Disorder Research American Psychiatric Association. DSM-IV-TR
: National Institute of Mental Health, National Institutes of Health, US Department of Health and Human Services; Available at: 5. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 4th ed., Text Revision. Washington, DC: American Psychiatric Association; Pini S et al. Eur Neuropsychopharmacol. In press. Glick ID. Prim Care Companion J Clin Psychiatry. 2004;6: World Health Organization NIMH. Bipolar Disorder Research American Psychiatric Association. DSM-IV-TR")
5
Trastorno Bipolar: una enfermedad crónica
23/03/2017 Trastorno Bipolar: una enfermedad crónica El riesgo de recurrencia en 5 años se aproxima al 73% a pesar de la farmacoterapia convencional Los deficits en las funciones psicosociales persisten durante años después de un episodio inicial El 59% de los pacientes muestran alteraciones funcionales 4.5 años después de la hospitalización Una mala función psicosocial predice un menor tiempo de recurrencia Bipolar Disorder Is a Chronic, Recurring Condition The risk of recurrence in bipolar patients has been reported to approach 73% over a follow-up period of 5 years despite treatment with conventional pharmacotherapy.1 Deficits in psychosocial functioning can persist years after an initial bipolar episode despite sustained symptomatic recovery.1-3 In one study, approximately 60% of subjects showed significant impairment in functioning years after hospitalisation3 Poor psychosocial function has been shown to predict shorter time to recurrence4 References: 1. Gitlin MJ, Swendsen J, Heller TL, Hammen C. Relapse and impairment in bipolar disorder. Am J Psychiatry. 1995;152: Coryell W, Scheftner W, Keller M, Endicott J, Maser J, Klerman GL. The enduring psychosocial consequences of mania and depression. Am J Psychiatry. 1993;150: Goldberg JF, Harrow M, Grossman LS. Course and outcome in bipolar affective disorder: a longitudinal follow-up study. Am J Psychiatry. 1995;152: Bauwens F, Pardoen D, Staner L, Dramaix M, Mendlewicz J. Social adjustment and the course of affective illness: a one-year controlled longitudinal study involving bipolar and unipolar outpatients. Depress Anxiety. 1998;8:50-57. Gitlin MJ et al. Am J Psychiatry. 1995;152: Coryell W et al. Am J Psychiatry. 1993;150: Goldberg JF et al. Am J Psychiatry. 1995;152: Bauwens F et al. Depress Anxiety. 1998;8:50-57.

6
23/03/2017 10 causas principales de años vividos con discapacidad (AVD) — Mundialmente, año 2000 Estimado — Personas de 15 a 44 años Ranking Enfermedad o Lesión 1 Depresión Unipolar 2 Abuso de alcohol 3 Esquizofrenia 4 Anemia ferropénica 5 Trastorno Bipolar 6 Pérdida auditiva en adultos 7 VIH/SIDA 8 Enfermedad Pulmonar Obstructiva Crónica 9 Osteoartritis 10 Accidentes de tráfico Bipolar Disorder Is a Leading Cause of Disability1 Mental and behavioural disorders cause massive disruption in the lives of those who are affected and their families. The World Health Organization has developed an assessment of the nonfatal impact of a disease as determined by Years Lived with Disability (YLD): It is estimated that 1 in 4 families worldwide has at least 1 member currently suffering from a mental or behavioural disorder Schizophrenia causes 4.9% of all YLDs, and bipolar disorder causes 4.7% of all YLDs worldwide among persons aged 15 to 44 years Reference: 1. World Health Organization. The World Health Report 2001—Mental Health: New Understanding, New Hope. Chapter 2: Burden of Mental and Behavioural Disorders. Available at: Accessed February 9, 2005. Condiciones neuropsiquiátricas resaltadas. World Health Organization, 2001.
: It is estimated that 1 in 4 families worldwide has at least 1 member currently suffering from a mental or behavioural disorder. Schizophrenia causes 4.9% of all YLDs, and bipolar disorder causes 4.7% of all YLDs worldwide among persons aged 15 to 44 years. Reference: 1. World Health Organization. The World Health Report 2001—Mental Health: New Understanding, New Hope. Chapter 2: Burden of Mental and Behavioural Disorders. Available at: Accessed February 9, Condiciones neuropsiquiátricas resaltadas. World Health Organization,")
7
Circuitos cerebrales de la regulación del estado de ánimo
23/03/2017 Circuitos cerebrales de la regulación del estado de ánimo MDm Mediodorsal Nucleus of the Thalamus MDm Midline Thalamus OMPFC Orbital/Medial Pre-Frontal Cortex OMPFC MV Medullary Velum PB Parabrachial Nucleus PAG Periaqueductal Gray Brain Stem PAG PB MV Ca Acc Nucleus Accumbens Ca Caudate P Putamen VP Ventral Pallidum Striatum Acc P Hippocampus VP CE M CA1 CA1 Field CA3 CA3 Field DG Dentate Gyrus PaS Parasubiculum PrS Presubiculum S Subiculum PAC AB Accessory Basal Nucleus B Basal Nucleus L Lateral Nucleus CE Central Amygdaloid Nucleus M Medial Amygdaloid Nucleus PAC Periamygadaloid Nucleus Hippocampus CA3 PrS PaS Amygdala [Keywords] 629, Soares, global, 03/09/2002, Monte Carlo, Monaco, bipolar, Zyprexa, olanzapine, neuropsychology, imaging, genetics, disease, Kelli Carson, Lilly, Eric Hoefflin, image, diagram### DG S CA1 Amygdala Sheline YI. Biol Psychiatry. 2000;48(8):
:")
8
Anomalías estructurales: Resonancia Magnética
23/03/2017 Anomalías estructurales: Resonancia Magnética [Keywords] 629, Soares, global, 03/09/2002, Monte Carlo, Monaco, bipolar, Zyprexa, olanzapine, neuropsychology, imaging, genetics, disease, Kelli Carson, Lilly, Eric Hoefflin, brain, scan, MRI, image### Benabarre et al, Psychother Psychosom, 2002; 71:

9
Volumen de la amígdala por Resonancia Magnética
23/03/2017 Volumen de la amígdala por Resonancia Magnética Volumen de Amígdala Izquierda 4.0 P=.04 3.5 3.0 2.5 Volumen de Amígdala Izquierda Corregido 2.0 1.5 1.0 [Keywords] 629, Soares, global, 03/09/2002, Monte Carlo, Monaco, bipolar, Zyprexa, olanzapine, neuropsychology, imaging, genetics, disease, Kelli Carson, Lilly, Eric Hoefflin### 0.5 Controles Bipolares Brambilla P, et al. Biol Psychiatry. 2001;49(8):540.
:540.")
10
Lesiones Hiperintensas en Resonancia Magnética (T2)
23/03/2017 [Keywords] 629, Soares, global, 03/09/2002, Monte Carlo, Monaco, bipolar, Zyprexa, olanzapine, neuropsychology, imaging, genetics, disease, Kelli Carson, Lilly, Eric Hoefflin, brain, scan, MRI, image### Altshuler LL, et al. Am J Psychiatry. 1995;152(8): Dupont RM, et al. Biol Psychiatry. 1995;38(7):
: Dupont RM, et al. Biol Psychiatry. 1995;38(7):")
11
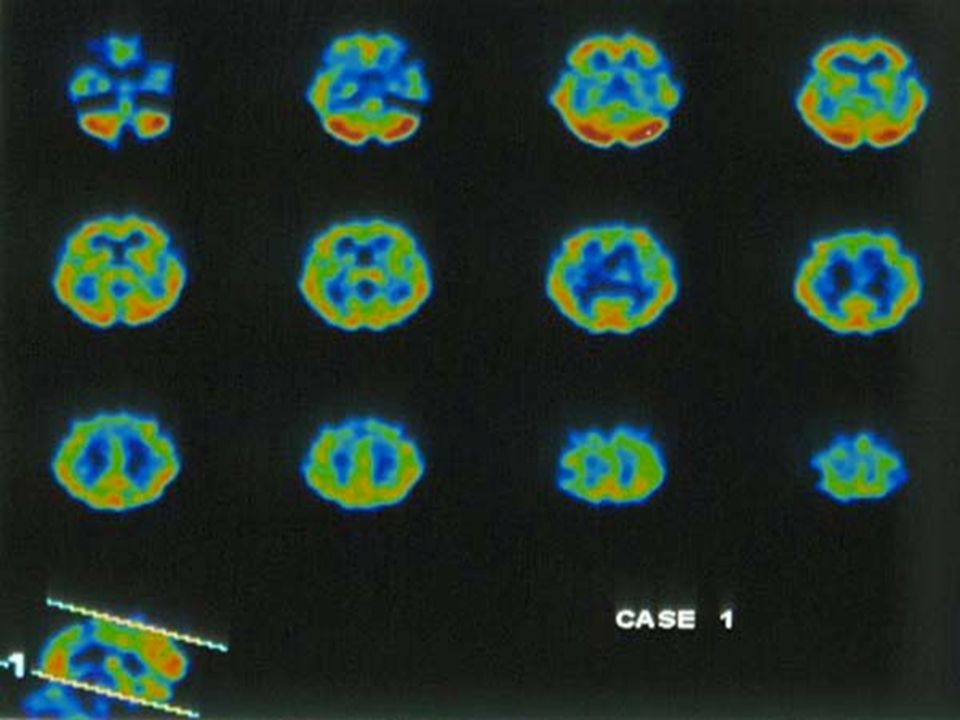
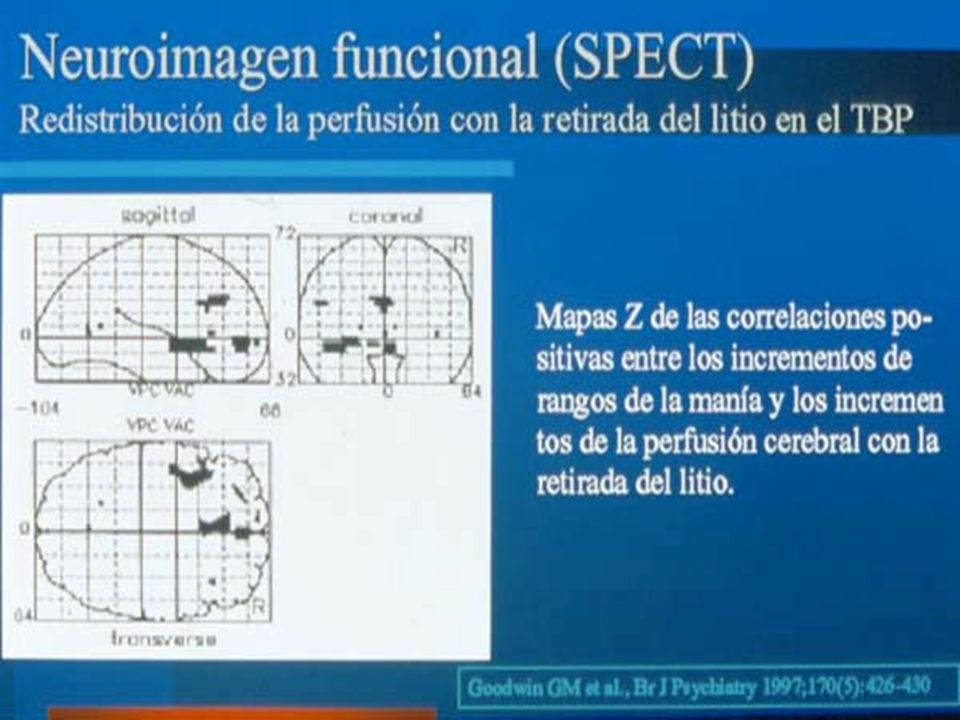
SPECT de perfusión con TC99mHMPAO en la depresión Bipolar
Benabarre et al, J Psychiatry Res (Neuroimag) 2004 Dec 30;132(3):
 2004 Dec 30;132(3):")
16
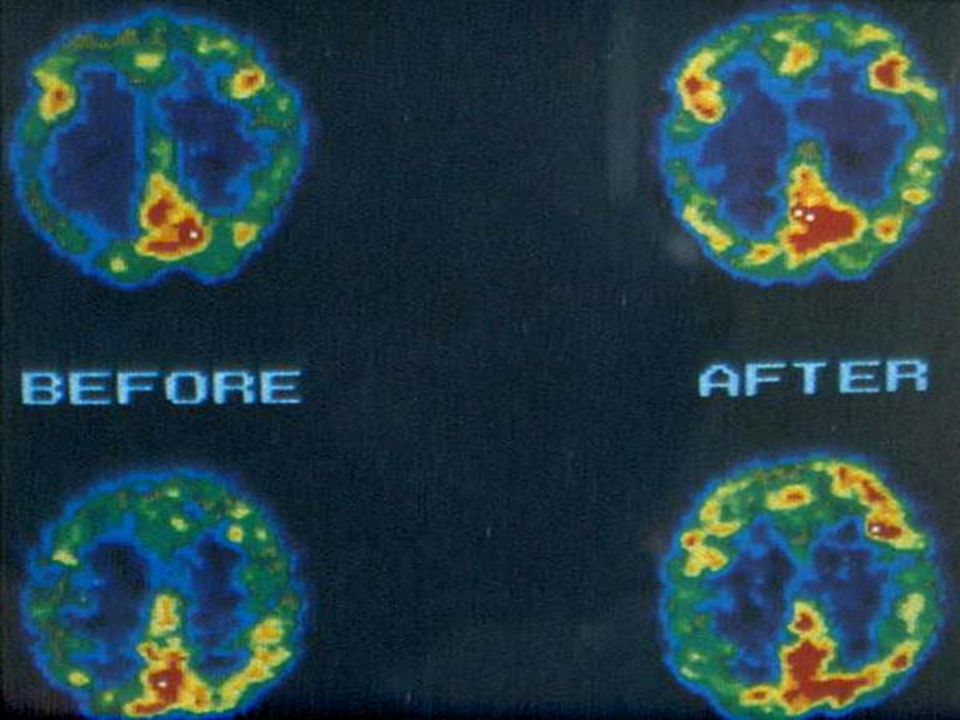
Activación cerebral en la depresión
Drevets WC. Biol Psychiatry. 2000;48(8):
:")
17
RESULTADOS Cohortes del estudio y evaluaciones realizadas
23/03/2017 RESULTADOS Cohortes del estudio y evaluaciones realizadas Casos Controles Total Evaluación SPECT sólo 13 3 16 Evaluación Neuropsicológica sólo 4 1 5 Ambas evaluaciones 26 2 28 Total evaluaciones SPECT (*) 39 44 Total evaluaciones neuropsicológicas 30 33 43 6 49 (*) Detalle de total evaluaciones Spect Casos SPECT fase depresiva 16 SPECT fase hipomaníaca - maníaca 19 SPECT fase eutímica 4
 Total evaluaciones neuropsicológicas (*) Detalle de total evaluaciones Spect. Casos. SPECT fase depresiva. 16. SPECT fase hipomaníaca - maníaca. 19. SPECT fase eutímica. 4.")
18
Pte. en fase depresiva Hipoperfusión frontal ant I cíngulo post I
cerebelo I Hiperperfusión - cerebelo D Asimetría - Cerebelo - Cíngulo post I Diferencias entre ambos hemicerebelos respecto a sujetos control. Benabarre et al., Aust NZ J Psychiatry 2005;39:227-34

19
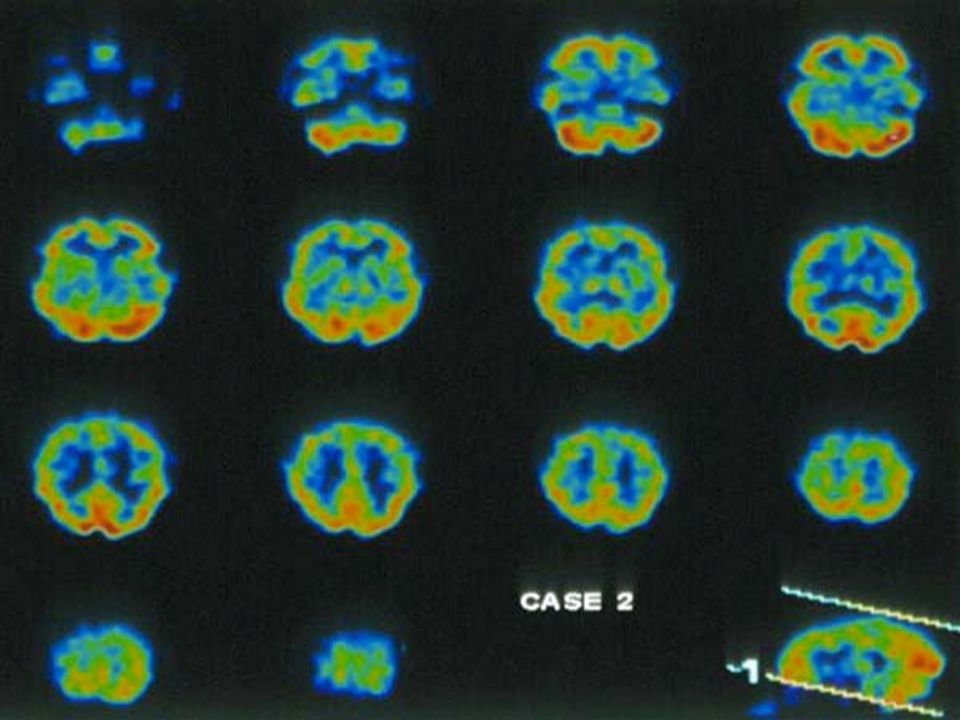
Pte. en fase hipomaniaca
Asimetría - Cíngulo ant Diferencias entre ambos hemicerebelos respecto a sujetos control. Benabarre et al., Aust NZ J Psychiatry 2005;39:227-34

20
Pte. en fase maniaca Hipoperfusión: cíngulo ant I cíngulo post I
Hiperperfusión: - Temp Ant D Cíngulo post D Asimetría: cíngulo ant estriado Alt. perfusión del Cuerpo estriado Benabarre et al., Aust NZ J Psychiatry 2005;39:227-34

21
Paciente en fase eutímica
Sin alteraciones significativas en las regiones de interés Benabarre et al., Aust NZ J Psychiatry 2005;39:227-34

26
TRATAMIENTO DE LOS TRASTORNOS BIPOLARES: presente y futuro

27
El tratamiento de la manía aguda y de mantenimiento

28
PREMISAS BÁSICAS La edad del paciente.
Los potenciales efectos de una eventual recaída. La conciencia de enfermedad. La gravedad del episodio previo. Los potenciales efectos adversos.

29
23/03/2017

31
23/03/2017

32
TRATAMIENTO DE MANTENIMIENTO: El carbonato de litio
Constituye la principal arma para el tratamiento de mantenimiento de la enfermedad. Se ha demostrado muy eficaz para el tratamiento de la manía, y útil en la prevención y tratamiento de la depresión. Importante en la prevención del suicidio.

33
23/03/2017 [Keywords] 629, Young, global, 03/07/2002, Monte Carlo, Monaco, bipolar, Zyprexa, olanzapine, Kelli Carson, Lilly, Eric Hoefflin###
![23/03/2017 [Keywords] 629, Young, global, 03/07/2002, Monte Carlo, Monaco, bipolar, Zyprexa, olanzapine, Kelli Carson, Lilly, Eric Hoefflin###](http://slideplayer.es/slide/20538/1/images/33/23%2F03%2F2017+%5BKeywords%5D+629%2C+Young%2C+global%2C+03%2F07%2F2002%2C+Monte+Carlo%2C+Monaco%2C+bipolar%2C+Zyprexa%2C+olanzapine%2C+Kelli+Carson%2C+Lilly%2C+Eric+Hoefflin%23%23%23.jpg "23/03/2017 [Keywords] 629, Young, global, 03/07/2002, Monte Carlo, Monaco, bipolar, Zyprexa, olanzapine, Kelli Carson, Lilly, Eric Hoefflin###")
34
TRATAMIENTO DE MANTENIMIENTO: El carbonato de litio
Finalidad de la determinación de los niveles plasmáticos de litio: reducir los riesgos de toxicidad, asegurarnos estar en dosis terapéuticas y comprobar el cumplimiento. Las cifras de mortalidad de los pacientes no cumplidores son muy superiores a las de los cumplidores.

35
TRATAMIENTO DE MANTENIMIENTO: El carbonato de litio
Efectos adversos del litio: Temblor. Síndrome polidipsia-poliuria. Posibilidad de hipotiroidismo subclinico y otras alteraciones tiroideas. Aumento de peso. Toxicidad renal. Riesgo teratogénico.

36
TRATAMIENTO DE MANTENIMIENTO: El carbonato de litio
El tratamiento con litio, controlando la litemia es seguro y eficaz. Situaciones de riesgo para la intoxicación: DIETA SIN SAL. Sudoración muy importante. Uso de diuréticos (como antihipertensivos). Se debe preferir por los bloqueantes de los receptores de la angiotensina II.
. Se debe preferir por los bloqueantes de los receptores de la angiotensina II.")
37
UNIDADES DE PLENUR VENDIDAS (1970-2000)
Millares de unidades

38
TRATAMIENTO DE MANTENIMIENTO: El valproato
Cada vez hay más evidencias de la eficacia de este fármaco. Sobre todo en formas clínicas mixtas, con ciclación rápida o con comorbilidad con el abuso de sustancias. También se determinan sus niveles plasmáticos. Efectos adversos: somnolencia, nauseas, vómitos, molestias intestinales, temblores, alteraciones enzimas hepáticos, trombocitopénia, adelgazamiento de los cabellos.

39
Litio vs. Valproato vs. Placebo en la Manía aguda
Divalproato Litio 28 26 24 22 20 18 16 Puntuación * * * * Basal Días *p<0.05 vs placebo Bowden et al, 1994

40
Respuesta terapéutica en función del número de episodios previos
Placebo (n=63) Litio (n=29) Divalproato (n=62) 10 8 6 4 2 Mejoría en síntomas maníacos de la SADS Número de episodios previos Swann AC et al. Am J Psychiatry 1999;156:1264–6
 Litio (n=29) Divalproato (n=62) Mejoría en síntomas. maníacos de la SADS Número de episodios previos. Swann AC et al. Am J Psychiatry 1999;156:1264–6.")
41
TRATAMIENTO DE MANTENIMIENTO CON VALPROATO, LITIO O PLACEBO (1 AÑO)
% 40 39 35 33 30 25 24 22 23 20 18 17 15 10 10 6 5 Depresión Manía Depresión o manía Placebo Litio Valproato Bowden et al, Arch Gen Psychiatry 2000

42
TRATAMIENTO DE MANTENIMIENTO: La carbamacepina
Existen estudios que avalan su efectividad en el mantenimiento del trastorno bipolar. Muy buena experiencia con la combinación del carbonato de litio y la carbamacepina. También se determinan sus niveles plasmáticos. Efectos adversos: leucopenia, somnolencia, diplopia, temblor, aumento de peso, alteración de los enzimas hepáticos, hiponatrémia, Sd. Stevens-Johnson,

43
Respuesta Diferencial al litio y la carbamacepina
23/03/2017 Respuesta Diferencial al litio y la carbamacepina Classical Nonclassical BP I, no mood-incongruent delusions/comorbidity BP II, BP NOS, mood-incongruent delusions, comorbidity 20 30 40 50 60 70 80 90 100 10 20 30 40 50 60 70 80 90 100 10 Carbamazepine Lithium Lithium Patients Remaining Well (%) Carbamazepine Slide 63 The role of carbamazepine in maintenance treatment is still undefined. Results of clinical studies have been equivocal, with some favoring carbamazepine over lithium but most finding the 2 equivalent or lithium to be superior. Conclusive evidence from placebo-controlled, blinded trials is lacking, but in the studies that have been done no more than 25% of patients maintained euthymia on carbamazepine monotherapy by 1 year. In a randomized, prospective, multicenter, long-term evaluation of the differential efficacy of lithium and carbamazepine in maintenance treatment of bipolar disorder (N=171), mean serum drug concentrations were 0.63±0.12 mmol/L for lithium and 6.14±1.5 g/mL for carbamazepine. Differential efficacy was assessed by dividing patients into 2 groups based on the presence of “classical” features (bipolar I without mood-incongruent delusions; n=67) or “nonclassical” features (all others, including bipolar II, bipolar disorder not otherwise specified, comorbidity, mood-incongruent delusions; n=104). Classical bipolar patients were hospitalized less frequently with lithium than with carbamazepine (P<0.006). Nonclassical bipolar patients appeared to have a better response to carbamazepine than lithium (P<0.08). For patients taking lithium, there was a significant (P=0.035) correlation between the number of nonclassical features present and risk of hospitalization. The researchers concluded that patients with nonclassical features of bipolar disorder might benefit more from carbamazepine than lithium treatment. P<0.006 n=67 P<0.08 n=104 6 12 18 24 30 6 12 18 24 30 Months Months BP I=bipolar I disorder; BP II=bipolar II disorder; BP NOS=bipolar disorder not otherwise specified. Greil et al. J Clin Psychopharmacol. 1998;18: Greil W, Kleindienst N, Erazo N, Muller-Oerlinghausen B. Differential response to lithium and carbamazepine in the prophylaxis of bipolar disorder. J Clin Psychopharmacol. 1998;18: Hirschfeld RMA, Bowden CL, Gitlin MJ, et al, for the Work Group on Bipolar Disorder. Practice Guideline for the Treatment of Patients With Bipolar Disorder (Revision). Am J Psychiatry. 2002;159(suppl):1-50. Keck PE Jr, McElroy SL. Carbamazepine and valproate in the maintenance treatment of bipolar disorder. J Clin Psychiatry. 2002;63(suppl 10):13-17.
 Carbamazepine. Slide 63. The role of carbamazepine in maintenance treatment is still undefined. Results of clinical studies have been equivocal, with some favoring carbamazepine over lithium but most finding the 2 equivalent or lithium to be superior. Conclusive evidence from placebo-controlled, blinded trials is lacking, but in the studies that have been done no more than 25% of patients maintained euthymia on carbamazepine monotherapy by 1 year. In a randomized, prospective, multicenter, long-term evaluation of the differential efficacy of lithium and carbamazepine in maintenance treatment of bipolar disorder (N=171), mean serum drug concentrations were 0.63±0.12 mmol/L for lithium and 6.14±1.5 g/mL for carbamazepine. Differential efficacy was assessed by dividing patients into 2 groups based on the presence of classical features (bipolar I without mood-incongruent delusions; n=67) or nonclassical features (all others, including bipolar II, bipolar disorder not otherwise specified, comorbidity, mood-incongruent delusions; n=104). Classical bipolar patients were hospitalized less frequently with lithium than with carbamazepine (P<0.006). Nonclassical bipolar patients appeared to have a better response to carbamazepine than lithium (P<0.08). For patients taking lithium, there was a significant (P=0.035) correlation between the number of nonclassical features present and risk of hospitalization. The researchers concluded that patients with nonclassical features of bipolar disorder might benefit more from carbamazepine than lithium treatment. P< n=67. P<0.08. n= Months. Months. BP I=bipolar I disorder; BP II=bipolar II disorder; BP NOS=bipolar disorder not otherwise specified. Greil et al. J Clin Psychopharmacol. 1998;18: Greil W, Kleindienst N, Erazo N, Muller-Oerlinghausen B. Differential response to lithium and carbamazepine in the prophylaxis of bipolar disorder. J Clin Psychopharmacol. 1998;18: Hirschfeld RMA, Bowden CL, Gitlin MJ, et al, for the Work Group on Bipolar Disorder. Practice Guideline for the Treatment of Patients With Bipolar Disorder (Revision). Am J Psychiatry. 2002;159(suppl):1-50. Keck PE Jr, McElroy SL. Carbamazepine and valproate in the maintenance treatment of bipolar disorder. J Clin Psychiatry. 2002;63(suppl 10):")
44
NUEVOS EUTIMIZANTES ANTIEPILEPTICOS Lamotrigina Gabapentina Topiramato
Tiagabina Oxcarbacepina Levetiracetam Pregabalina Retigabina

45
Ácido g-aminobutírico (GABA)
GABAPENTINA COOH H2N CH2 H2N COOH Ácido g-aminobutírico (GABA) Gabapentina Aminoácido Estructuralmente relacionado con el GABA
 Gabapentina. Aminoácido. Estructuralmente relacionado con el GABA.")
46
Gabapentina vs. placebo añadidos a litio en la manía
23/03/2017 Gabapentina vs. placebo añadidos a litio en la manía Puntuaciones en la YMRS Semanas Pande et al, 1999

47
Gabapentina como tratamiento coadyuvante en T. Bipolar resistente
23/03/2017 Gabapentina como tratamiento coadyuvante en T. Bipolar resistente LOCF p<0.05 * Dosis media: 1310 mg/d Vieta et al, Eur Psychiatry 2000

48
Gabapentina en bipolares con mala respuesta a otros estabilizadores
23/03/2017 Gabapentina en bipolares con mala respuesta a otros estabilizadores Porcentaje de pacientes 80 70 60 50 40 30 20 10 Ansiedad Irritabilidad Sueño Estabilidad Sociabilidad Concentración Mejor Igual Peor Vieta et al, Eur Psychiatry 2000

49
Gabapentin in the prophylactic add-on treatment of bipolar disorder
23/03/2017 One-year, double-blind, randomized, placebo-controlled trial P=0,004 Improvement in CGI-BP-M for BD Vieta et al, J Clin Psychiatry, 2006 N=13 N=12

50
sulfamato de 2,3:4,5-bis-0- (1-metiletilideno)-b-D-fructopiranosa
TOPIRAMATO CH2OSO2NH2 sulfamato de 2,3:4,5-bis-0- (1-metiletilideno)-b-D-fructopiranosa
-b-D-fructopiranosa.")
Presentaciones similares