Descargar la presentación
La descarga está en progreso. Por favor, espere

1
INSUFICIENCIA CARDÍACA, ENFERMEDAD RENAL Y ANEMIA VISIÓN CARDIOLÓGICA
Federico Vallés. Córdoba

2
INSUFICIENCIA CARDÍACA, ENFERMEDAD RENAL Y ANEMIA. INTRODUCCIÓN.
Desde hace más de 30 años (Harrison), se consideraba severa anemia ≤ 10 gr de Hb con cardiopatía. Se aplicaba a enfermedad coronaria. No era rutinaria una hematimetría en el enfermo cardiológico, al menos en seguimiento. No estudios de causas de anemia y poco tratamiento.
, se consideraba severa anemia ≤ 10 gr de Hb con cardiopatía. Se aplicaba a enfermedad coronaria. No era rutinaria una hematimetría en el enfermo cardiológico, al menos en seguimiento. No estudios de causas de anemia y poco tratamiento.")
3
CASOS CLÍNICOS Enferma de 45 años, antecedentes isquémicos familiares. Angina típica de esfuerzo. Coronariografía normal en 1981. Enferma de 67 años con lesión mitral e HP. IC grado III. Prótesis metálica en IC grado I. Anemia por pérdidas, IC grado III-IV. Se corrige, IC grado I. Enfermo de 45 años con ER en diálisis. IC grado III con disfunción VI severa en Anemia. EPO en 2004 y hierro, IC grado I.

4
IC, y ANEMIA. IC, ER y ANEMIA ESTADO ACTUAL
En registro de EEUU en 2011 enfermos ambulatorios con IC estable, había anemia en el 29% de los pacientes. Se diagnosticó en el 6% (JACC 2003;41:supplA:157A). EHS en IC: se obtuvo Hb y FG. Nada en tratamiento (EHJ 2003;24:442). Mejoría función tras TR. No se considera la anemia (JACC 2005;45:1051). Guía europea de IC. Se debe evaluar Hb y Cr. En eval riesgo entre 32 factores cita anemia y Cr con dos citas sin comentarios. En tratamiento solo monitorización de Cr con IECA. (EHJ 2005;26:1115).
. EHS en IC: se obtuvo Hb y FG. Nada en tratamiento (EHJ 2003;24:442). Mejoría función tras TR. No se considera la anemia (JACC 2005;45:1051). Guía europea de IC. Se debe evaluar Hb y Cr. En eval riesgo entre 32 factores cita anemia y Cr con dos citas sin comentarios. En tratamiento solo monitorización de Cr con IECA. (EHJ 2005;26:1115).")
5
ANEMIA, INSUFICIENCIA CARDÍACA, ENFERMEDAD RENAL
JACC 2004;44:959

6
IC, y ANEMIA. IC, ER y ANEMIA CUESTIONES PREVIAS
Anemia y función cardíaca. Anemia e insuficiencia cardíaca. Anemia en insuficiencia renal. Anemia en IC y pronóstico Influencia del tratamiento en pronóstico. Conclusiones.

7
ANEMIA Y FUNCIÓN CARDÍACA
En anemia crónica (Hb < 7 gr/dl), ferropénica: Elevación de VM, Mayor volumen latido y FC. Contractilidad aumentada y no disfunción sistólica ni diastólica (AHJ 1992;124:1516). En niños con anemia más severa (< de 6),había disfunción ventricular, que se corregía con hierro (Pediatr Int 1999;41:13). En anemia falciforme se encontró cardiomegalia por dilatación y en edad adulta algunos presentan disfunción diastólica (Int J Ang 1998;7:185).
, ferropénica: Elevación de VM, Mayor volumen latido y FC. Contractilidad aumentada y no disfunción sistólica ni diastólica (AHJ 1992;124:1516). En niños con anemia más severa (< de 6),había disfunción ventricular, que se corregía con hierro (Pediatr Int 1999;41:13). En anemia falciforme se encontró cardiomegalia por dilatación y en edad adulta algunos presentan disfunción diastólica (Int J Ang 1998;7:185).")
8
CAUSAS DE ANEMIA EN INSUFICIENCIA CARDÍACA
Por hemodilución. Anticoagulantes y antiagregantes. Aumento de TNF-α (inhibe hematopoyesis). Malnutrición. IECA (SOLVD; JACC 2005:45:291) reduce efecto EPO . Déficit absorción Fe y vit B12. Otras: Insuficiencia renal. Anemia del anciano. Todas las posibles causas.
. Malnutrición. IECA (SOLVD; JACC 2005:45:291) reduce efecto EPO . Déficit absorción Fe y vit B12. Otras: Insuficiencia renal. Anemia del anciano. Todas las posibles causas.")
9
PREVALENCIA DE ANEMIA EN INSUFICIENCIA CARDÍACA
Key Point: Prevalence of anemia in heart failure patients varies, ranging from 17% to 48% in studies with the largest sample sizes. References: 1. McClellan WM, Flanders WD, Langston RD, et al. Anemia and renal insufficiency are independent risk factors for death among patients with congestive heart failure admitted to community hospitals: a population- based study. J Am Soc Nephrol. 2002;13: 2. Androne AS, Katz SD, Lund L, et al. Hemodilution is common in patients with advanced heart failure. Circulation. 2003;107: 3. Silverberg DS, Wexler D, Blum M, et al. The use of subcutaneous erythropoietin and intravenous iron for the treatment of the anemia of severe, resistant congestive heart failure improves cardiac and renal function and functional cardiac class, and markedly reduces hospitalizations. J Am Coll Cardiol. 2000;35: 4. Kosiborod M, Smith GL, Radford MJ, et al. The prognostic importance of anemia in patients with heart failure. Am J Med. 2003;114: 5. Horwich TB, Fonarow GC, Hamilton MA, et al. Anemia is associated with worse symptoms, greater impairment in functional capacity and a significant increase in mortality in patients with advanced heart failure. J Am Coll Cardiol. 2002;39: 6. Herzog CA, Li S, Guo H, et al. The prevalence of CHF, chronic kidney disease, anemia, and multiple comorbid conditions in the Medicare population. J Card Fail. 2002;8(suppl):S63. Abstract 228. 7. Al-Ahmad A, Rand WM, Manjunath G, et al. Reduced kidney function and anemia as risk factors for mortality in patients with left ventricular dysfunction. J Am Coll Cardiol. 2001;38: 8. Cleland JG, Swedberg K, Follath F, et al. The EuroHeart Failure survey programme—a survey on the quality of care among patients with heart failure in Europe. Part 1: patient characteristics and diagnosis. Eur Heart J ;24: 9. Mozaffarian D, Nye R, Levy WC. Anemia predicts mortality in severe heart failure: the prospective randomized amlodipine survival evaluation (PRAISE). J Am Coll Cardiol. 2003;41: 10. Anker SD, Sharma R, Francis D, et al. Patients with chronic heart failure (CHF) in the ELITE II trial. Circulation. 2002;106(suppl): 472. Abstract 2335. 11. Ezekowitz JA, McAlister FA, Armstrong PW. Anemia is common in heart failure and is associated with poor outcomes: insights from a cohort of patients with new-onset heart failure. Circulation. 2003;107: 12. Tanner H, Moschovitis G, Kuster GM, et al. The prevalence of anemia in chronic heart failure. Int J Cardiol ;86: 13. Cromie N, et al. Anaemia in chronic heart failure: what is its frequency in the UK and its underlying causes? Heart. 2002;87: 14. Szachniewicz J, Petruk-Kowalczyk J, Majda J, et al. Anaemia is an independent predictor of poor outcome in patients with chronic heart failure. Int J Cardiol Aug;90(2-3):
:S63. Abstract Al-Ahmad A, Rand WM, Manjunath G, et al. Reduced kidney function and anemia as risk factors for mortality in patients with left ventricular dysfunction. J Am Coll Cardiol. 2001;38: Cleland JG, Swedberg K, Follath F, et al. The EuroHeart Failure survey programme—a survey on the quality of care among patients with heart failure in Europe. Part 1: patient characteristics and diagnosis. Eur Heart J. 2003;24: Mozaffarian D, Nye R, Levy WC. Anemia predicts mortality in severe heart failure: the prospective randomized amlodipine survival evaluation (PRAISE). J Am Coll Cardiol. 2003;41: Anker SD, Sharma R, Francis D, et al. Patients with chronic heart failure (CHF) in the ELITE II trial. Circulation. 2002;106(suppl): 472. Abstract Ezekowitz JA, McAlister FA, Armstrong PW. Anemia is common in heart failure and is associated with poor outcomes: insights from a cohort of patients with new-onset heart failure. Circulation. 2003;107: Tanner H, Moschovitis G, Kuster GM, et al. The prevalence of anemia in chronic heart failure. Int J Cardiol. 2002;86: Cromie N, et al. Anaemia in chronic heart failure: what is its frequency in the UK and its underlying causes Heart. 2002;87: Szachniewicz J, Petruk-Kowalczyk J, Majda J, et al. Anaemia is an independent predictor of poor outcome in patients with chronic heart failure. Int J Cardiol Aug;90(2-3):")
10
EUROHEART SURVEY. HEART FAILURE
Enfermos hospitalizados en durante 6 semanas en 115 hospitales de 24 países europeos. Incluyen pacientes con IC sistólica o diastólica. 47 % mujeres Hb < 11: 18% hombres y 23% mujeres. Creatinina >1,5 en el 16% y >2 en 7%. EHS heart failure. EHJ 2003;24:442

11
EHS heart failure. EHJ 2003;24:442

12
EHS heart failure. EHJ 2003;24:442

13
PREVALENCIA DE ANEMIA Y EFECTO SOBRE MORTALIDAD EN IC
Recogido de literatura. 26 estudios. pacientes Periodo:1966-agosto 2004 Definición anemia: 2: no definida. 5: Htco menor de 35-41% 19: Hb < g/dl. Prevalencia de anemia: % AHJ 2005;149:391

14
DEFINICIÓN DE ANEMIA EN ESTUDIOS DE IC
OMS: <12 g en mujeres fértiles y < 13 en hombre. Diferentes criterios de hematocrito. National kidney foundation: ≤11 o 12,5 g/dL. Pero en estudios de IC y anemia no se emplea, Código ICD-9: en general menos anemia. No siempre se separa hombres y mujeres. Hay que tener en cuenta la edad, NYHA. Causas corregibles y no renales (vit B12, hierro, sangrado. Empleo de drogas.

15
DEFINICIÓN DE ANEMIA (OMS) Y DISTRIBUCIÓN DE HB EN POBLACIÓN GENERAL
Key Point: Superimposing the World Health Organization (WHO) anemia definition1 over graphs of the distribution of Hb levels by gender2 is revealing: anemia under this definition comprises Hb levels that are significantly lower than mean Hb levels in the population. Although there is no definitive agreement on the definition of anemia, one of the most commonly used definitions is the one used by the World Health Organization. The WHO defines anemia as Hb <13 g/dL in men and <12 g/dL in premenopausal, nonpregnant women. References: 1. World Health Organization. Iron deficiency anaemia assessment, prevention and control: a guide for programme managers. Geneva: World Health Organization; 2001. 2. Dallman PR, Looker AC, Johnson CL, Carroll M. Influence of age on laboratory criteria for the diagnosis of iron deficiency anaemia and iron deficiency in infants and children. In: Hallberg L, Nils-Georg A, eds. Iron Nutrition in Health and Disease. London, UK: John Libbey & Company; 1996:65-74.
 anemia definition1 over graphs of the distribution of Hb levels by gender2 is revealing: anemia under this definition comprises Hb levels that are significantly lower than mean Hb levels in the population. Although there is no definitive agreement on the definition of anemia, one of the most commonly used definitions is the one used by the World Health Organization. The WHO defines anemia as Hb <13 g/dL in men and <12 g/dL in premenopausal, nonpregnant women. References: 1. World Health Organization. Iron deficiency anaemia assessment, prevention and control: a guide for programme managers. Geneva: World Health Organization; Dallman PR, Looker AC, Johnson CL, Carroll M. Influence of age on laboratory criteria for the diagnosis of iron deficiency anaemia and iron deficiency in infants and children. In: Hallberg L, Nils-Georg A, eds. Iron Nutrition in Health and Disease. London, UK: John Libbey & Company; 1996:")
16
PREVALENCIA DE ANEMIA EN RELACIÓN CON LA EDAD
Key Point: Anemia is a health condition that occurs more frequently with advancing age. In this large (N = 53,887) population study conducted in Olmsted County, Minn (Mayo Clinic) by Ania, et al,1 the trend in prevalence increase is noticeable beginning in the age group 60 to 64 years and subsequently increases with advancing age. Using WHO criteria, <10% of the Olmsted residents were anemic, while by age 85, >20% of the females and >40% of the males were anemic. Although prior to age 55 more women than men were anemic, the trend reverses later in life. The same increasing trend with age was noted in patients referred from other areas to Mayo Clinic. Other studies have confirmed the prevalence trend identified in the Olmsted research. In a retrospective study (N = 1784) conducted by Inelmen, et al2 of individuals 65 years, 9.4% of the men and 8.8% of the women were anemic by WHO criteria. Kirkeby, et al,3 who investigated patients 70 years of age (N = 530), found 16% of men and 13% of women with WHO-criteria anemia. Looking at even older patients, Nilsson-Ehle, et al4 reported that 23.8% of men and 10% of women had WHO-criteria anemia at age 88. A recent review of studies of anemia in elderly patients found a wide variation in prevalence, ranging from 2.9% to 61% in men and 3.3% to 41% in women, with the highest rates in the oldest patients and those who were hospitalized.5 References: 1. Anía B, Suman VJ, Fairbanks VF, et al. Prevalence of anemia in medical practice: community versus referral patients. Mayo Clin Proc. 1994;69: 2. Inelmen E, D’Alessio M, Gatto MRA, et al. Descriptive analysis of the prevalence of anemia in a randomly selected sample of elderly people living at home: some results of an Italian multicentric study. Aging Clin Exp Res. 1994;6:81-89. 3. Kirkeby O,Fossum S, Risøe C. Anaemia in elderly patients. Scand J Prim Health Care. 1991;9: 4. Anía B, Suman VJ, Fairbanks VF, et al. Incidence of anemia in older people: an epidemiological study in a well defined population. J Am Geriatr Soc. 1997;45: 5. Nilsson-Ehle H, Jagenburg R, Landahl S, et al. Blood haemoglobin declines in the elderly: implications for reference intervals from age 70 to 88. Eur J Haematol. 2000;65: 6. Zynx Health Incorporated. The Prevalence and Impact of Anemia: A Systematic Review of the Published Literature. Los Angeles, CA: Zynx Health Incorporated;
 population study conducted in Olmsted County, Minn (Mayo Clinic) by Ania, et al,1 the trend in prevalence increase is noticeable beginning in the age group 60 to 64 years and subsequently increases with advancing age. Using WHO criteria, <10% of the Olmsted residents were anemic, while by age 85, >20% of the females and >40% of the males were anemic. Although prior to age 55 more women than men were anemic, the trend reverses later in life. The same increasing trend with age was noted in patients referred from other areas to Mayo Clinic. Other studies have confirmed the prevalence trend identified in the Olmsted research. In a retrospective study (N = 1784) conducted by Inelmen, et al2 of individuals 65 years, 9.4% of the men and 8.8% of the women were anemic by WHO criteria. Kirkeby, et al,3 who investigated patients 70 years of age (N = 530), found 16% of men and 13% of women with WHO-criteria anemia. Looking at even older patients, Nilsson-Ehle, et al4 reported that 23.8% of men and 10% of women had WHO-criteria anemia at age 88. A recent review of studies of anemia in elderly patients found a wide variation in prevalence, ranging from 2.9% to 61% in men and 3.3% to 41% in women, with the highest rates in the oldest patients and those who were hospitalized.5. References: 1. Anía B, Suman VJ, Fairbanks VF, et al. Prevalence of anemia in medical practice: community versus referral patients. Mayo Clin Proc. 1994;69: Inelmen E, D’Alessio M, Gatto MRA, et al. Descriptive analysis of the prevalence of anemia in a randomly selected sample of elderly people living at home: some results of an Italian multicentric study. Aging Clin Exp Res. 1994;6: Kirkeby O,Fossum S, Risøe C. Anaemia in elderly patients. Scand J Prim Health Care. 1991;9: Anía B, Suman VJ, Fairbanks VF, et al. Incidence of anemia in older people: an epidemiological study in a well defined population. J Am Geriatr Soc. 1997;45: Nilsson-Ehle H, Jagenburg R, Landahl S, et al. Blood haemoglobin declines in the elderly: implications for reference intervals from age 70 to 88. Eur J Haematol. 2000;65: Zynx Health Incorporated. The Prevalence and Impact of Anemia: A Systematic Review of the Published Literature. Los Angeles, CA: Zynx Health Incorporated;")
17
ETIOLOGÍA DE LA ANEMIA EN EL ANCIANO
Key Point: Anemia is not an inevitable consequence of aging, as a cause is identified in the majority of patients. In both inpatients and outpatients, chronic disease is the most common identified cause of anemia in the elderly. Iron deficiency is also common in this population. While there is a substantial number of cases in which a cause has not been identified, this may be due in part to inadequate diagnostic evaluation or to absolute or relative erythropoietin deficiency. Failure to evaluate anemia in the elderly could lead to delayed diagnosis of potentially treatable conditions.1 References: 1. Balducci L. Epidemiology of anemia in the elderly: information on diagnostic evaluation. J Am Geriatr Soc. 2003;51(suppl):S2-S9. 2. Joosten E, Pelemans W, Hiele M, et al. Prevalence and causes of anaemia in a geriatric hospitalized population. Gerontology. 1992;38: 3. Anía B, Suman VJ, Fairbanks VF, et al. Incidence of anemia in older people: an epidemiological study in a well defined population. J Am Geriatr Soc. 1997;45:
:S2-S9. 2. Joosten E, Pelemans W, Hiele M, et al. Prevalence and causes of anaemia in a geriatric hospitalized population. Gerontology. 1992;38: Anía B, Suman VJ, Fairbanks VF, et al. Incidence of anemia in older people: an epidemiological study in a well defined population. J Am Geriatr Soc. 1997;45:")
18
AHJ 2005;149:391

19
PRONÓSTICO ANEMIA EN INSUFICIENCIA CARDÍACA

20
AHJ 2005;149:391

21
PRONOSTICO DE ANEMIA EN IC
Al-Alman: (estudio SOLVD). Un 1% de disminución del hematocrito se asocia a riesgo 1,027 mayor de mortalidad global. Mc Clellan: Hematocrito y creatinina se asocian, independientemente a > mortalidad. Horvich: Incluso grados leves de anemia (<12,3) se asocian a deterioro en la situación funcional y en la supervivencia. Ezekowitz: En p. Anemia marcador independiente de mortalidad. JACC2002;39:955; JASN 2002;13:1928. Cir 2003;107:223
. Un 1% de disminución del hematocrito se asocia a riesgo 1,027 mayor de mortalidad global. Mc Clellan: Hematocrito y creatinina se asocian, independientemente a > mortalidad. Horvich: Incluso grados leves de anemia (<12,3) se asocian a deterioro en la situación funcional y en la supervivencia. Ezekowitz: En p. Anemia marcador independiente de mortalidad. JACC2002;39:955; JASN 2002;13:1928. Cir 2003;107:223.")
22
ANEMIA Y MORTALIDAD EN IC
AHJ 2005;

24
STAMINA-HFP. Registro de anemia en población con insuf. Cardíaca
Estudio prospectivo, observacional, con Insuficiencia cardíaca en USA. Resultados, sobre los primeros incluidos: Anemia (Hb < 12g/dl) el 24% I. renal (GFR < 60ml/min/1,73m2) el 61%. Calidad de vida (Cuestionarios Kansas y Minesota): reducida con anemia (variable continua) Supervivencia sobre 198 pacientes (edad media 63 años) 35 fallecimientos en 0,7 años de seguimiento. Anemia aumenta el riesgo en 2,47 RR. Por cada gramo de Hb reducido disminuye 1,39 RR J Cardiac Failure 2004; 10, suppl: S75,S102,S108.
 el 24% I. renal (GFR < 60ml/min/1,73m2) el 61%. Calidad de vida (Cuestionarios Kansas y Minesota): reducida con anemia (variable continua) Supervivencia sobre 198 pacientes (edad media 63 años) 35 fallecimientos en 0,7 años de seguimiento. Anemia aumenta el riesgo en 2,47 RR. Por cada gramo de Hb reducido disminuye 1,39 RR. J Cardiac Failure 2004; 10, suppl: S75,S102,S108.")
25
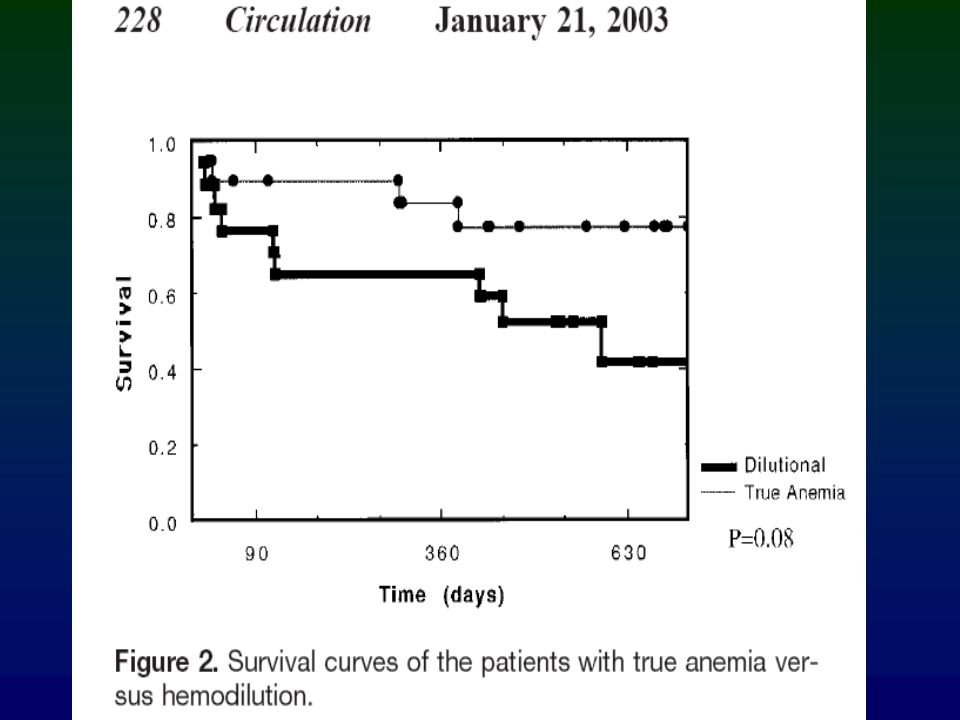
PRESENCIA DE ANEMIA, IC Y ER EN RELACIÓN CON HOSPITALIZACIÓN
Key Point: Medicare patients with heart failure (HF) are at high risk for morbidity. The risk for hospitalization in HF patients significantly increases with the coincidence of CKD and anemia. Based on a survey of the US Medicare population in 1998, Herzog and colleagues estimated that among the 3 million Medicare patients with HF, 850,000 had anemia and 414,000 had CKD; 197,000 HF patients also had both anemia and CKD. Each condition was associated with increased risks of hospitalization, and having 2 or all 3 conditions was associated with correspondingly higher rates of hospitalization. References: 1. Herzog CA, Guo H, Collins AJ. The prevalence of CHF, chronic kidney disease, anemia, and multiple comorbid conditions in the Medicare population [abstract 228]. 6th Annual Scientific Meeting of the Heart Failure Society of America; September 22-25, 2002; Boca Raton, Fla. 2. Herzog CA, Guo H, Collins AJ. Hospitalization rates for CHF patients in the Medicare population: the impact of kidney disease and anemia [abstract 269]. 6th Annual Scientific Meeting of the Heart Failure Society of America; September 22-25, 2002; Boca Raton, Fla.
 are at high risk for morbidity. The risk for hospitalization in HF patients significantly increases with the coincidence of CKD and anemia. Based on a survey of the US Medicare population in 1998, Herzog and colleagues estimated that among the 3 million Medicare patients with HF, 850,000 had anemia and 414,000 had CKD; 197,000 HF patients also had both anemia and CKD. Each condition was associated with increased risks of hospitalization, and having 2 or all 3 conditions was associated with correspondingly higher rates of hospitalization. References: 1. Herzog CA, Guo H, Collins AJ. The prevalence of CHF, chronic kidney disease, anemia, and multiple comorbid conditions in the Medicare population [abstract 228]. 6th Annual Scientific Meeting of the Heart Failure Society of America; September 22-25, 2002; Boca Raton, Fla. 2. Herzog CA, Guo H, Collins AJ. Hospitalization rates for CHF patients in the Medicare population: the impact of kidney disease and anemia [abstract 269]. 6th Annual Scientific Meeting of the Heart Failure Society of America; September 22-25, 2002; Boca Raton, Fla.")
26
ANEMIA FACTOR DE RIESGO MULTIPLICATIVO. MORTALIDAD
Key Point: HF, anemia, and CKD each independently increase the risk of 2-year mortality in Medicare patients, and the coincidence of 2 or all 3 conditions increases the mortality risk correspondingly. In a survey of 1,124,302 Medicare patients (excluding those with ESRD), relative risks of death in a 2-year period ( ) were calculated. The study population was 39% male and 89% Caucasian; 56% were 65 to 74 years of age, and 44% were 75 years of age. Anemia and CKD each confer a twofold increase in the risk of death within 2 years, and HF confers a threefold increase. Combinations of these independent risk factors are associated with correspondingly higher mortality risks. Reference: Herzog CA, Shuling L, Collins AJ. The impact of congestive heart failure (CHF), chronic kidney disease (CKD), and anemia on survival in the Medicare population [abstract 226; S63]. 6th Annual Scientific Meeting of the Heart Failure Society of America; September 22-25, 2002; Boca Raton, Fla.
, relative risks of death in a 2-year period ( ) were calculated. The study population was 39% male and 89% Caucasian; 56% were 65 to 74 years of age, and 44% were 75 years of age. Anemia and CKD each confer a twofold increase in the risk of death within 2 years, and HF confers a threefold increase. Combinations of these independent risk factors are associated with correspondingly higher mortality risks. Reference: Herzog CA, Shuling L, Collins AJ. The impact of congestive heart failure (CHF), chronic kidney disease (CKD), and anemia on survival in the Medicare population [abstract 226; S63]. 6th Annual Scientific Meeting of the Heart Failure Society of America; September 22-25, 2002; Boca Raton, Fla.")
27
ANEMIA FACTOR DE RIESGO MULTIPLICATIVO. MORTALIDAD
Key Point: The presence of anemia compounds the mortality risk of other pathologic conditions, such as CKD, HF, and DM, in the elderly. This analysis, performed by Collins, reviewed claims records of 1.2 million patients in the 5% General Medicare Database identified in a 2-year ( ) entry cohort. Reference: Collins A. Modern approaches to anemia management: current models for clinical and practice success. Presented at ASN Satellite Symposium; December 2002.
 entry cohort. Reference: Collins A. Modern approaches to anemia management: current models for clinical and practice success. Presented at ASN Satellite Symposium; December")
28
PRONÓSTICO EN IC MARC. INFL , NEUROHUM. Y NIVELES EPO
188 pacientes con IC (I-IV), seguidos al menos 24 meses. PCR, NT-pro BNP y nivel sérico de EPO Anemia el 34% e IR 41.4% (no criterios) A los 24 meses fallece el 20,2% y 22.8% ingresados. George J. Arch Int Med 2005;165:1304
, seguidos al menos 24 meses. PCR, NT-pro BNP y nivel sérico de EPO. Anemia el 34% e IR 41.4% (no criterios) A los 24 meses fallece el 20,2% y 22.8% ingresados. George J. Arch Int Med 2005;165:1304.")
29
Arch Int Med 2005;165:1304

30
Arch Int Med 2005;165:1304

31
PRONÓSTICO EN IC MARC. INFL , NEUROHUM. Y NIVELES EPO. CONCLUSIONES
EPO es una hormona que está aumentada en la IC. Aumenta según la gravedad de la IC. Valor pronóstico en términos de mortalidad y hospitalizaciones En la IC hay reducción de la perfusión tisular. La hipoxia podría aumentar la EPO. O bien por producción de radicales libres. ¿Es perjudicial en la IC?: Aumenta agregabilidad, viscosidad, moléculas de adhesión. George J. Arch Int Med 2005;165:1304

32
TRATAMIENTO DE LA ANEMIA EN INSUFICIENCIA CARDÍACA

33
TRATAMIENTO CON EPO EN IRC. EFECTO SOBRE EL CORAZÓN
Wizemann y cols: Nephron 1992;62:161. Tratamiento con EPO reducía la isquemia inducida por ejercicio, disminuía el gasto cardiaco y la sobrecarga del VI. Estudio cruzado y aleatorizado realizado en Australia: NDT 2000;15:1425 Reducción del diámetro telediastólico. HVI significativamente menor. Estudio multicentrico canadiense: Kidney 2000;58;1325. No se pudo demostrar que la normalización de la Hb produjese la regresión de la HVI concéntrica o de la dilatación del VI.

34
EFECTOS ANTIAPOPTÓSICOS DE LA EPO
EPO estimula la proliferación y diferenciación de las células eritroides, evita la muerte celular de los eritroblastos inmaduros. Se une EPO a EPO – R y activan simultaneamente varias vias de señalización. Regulación al alza de genes antiapoptósicos como bcl – 2 y bcl – XL. Mecanismos antiapoptósicos tienen un papel importante en ACV, enfermedades retinianas, IAM e ICC.

35
FUNCIÓN DE LA rh – EPO EN ICC
Silverberg y cols. n = FEVI < 40 % y Hb 10 – 11,5 gr/dl. Objetivo Hb>12,5 g/dl Seguimiento 8,2 ± 2,6 meses. Grupo tratado Grupo no tratado Mejoría 42% CLASE NYHA Empeoramiento 11% Aumento 5,5% FEVI Disminución 5,4% Disminución 79% Días de hospitalización Aumento 57,6% JACC 2001;37:1775

36
FUNCIÓN DE LA rh – EPO EN ICC
Mancini y cols. Circulation 2003:107;204 Evalúa los efectos de rh – EPO sobre la capacidad de ejercicio en 22 pacientes con ICC moderada-grave. En grupo tratado, Hb de 10.9 pasó a 14,3. Conclusiones: EPO mejoraba la capacidad de ejercicio evaluada mediante el consumo máximo de O2. Aumenta la duración del ejercicio y la calidad de vida.

37
TRATAMIENTO CON EPO EN IRC. CONSECUENCIAS CARDÍACAS
CONCLUSIONES: Los efectos de corrección de la anemia son escasos en las ultimas fases de la enfermedad cardiaca en pacientes con IRC cuando se ha desarrollado HVI o dilatación intensa. El tratamiento con rh-EPO tiene efecto favorable sobre la prevención de HVI aunque el numero de pacientes es bajo. Las alteraciones estructurales que aparecen en el corazón, como la fibrosis intersticial, provocan cambios irreversibles y reducen los efectos del tratamiento con rh-EPO. Posibles efectos desfavorables EPO (trombosis, HTA, ↑ act.endotelio…) No obstante, Hay aumento en la clase funcional en IC Mejora la función ventricular Disminuye la necesidad de diuréticos. No efecto sobre mortalidad.
 No obstante, Hay aumento en la clase funcional en IC. Mejora la función ventricular. Disminuye la necesidad de diuréticos. No efecto sobre mortalidad.")
38
JACC 2005;45:1051

40
CONCLUSIONES ANEMIA E IC.- I
Poco caso a la existencia de anemia o no en IC con o sin enfermedad renal. Interés creciente. Disparidad entre datos existentes y preocupación clínica. Difícil valorar síntomas, ya que se mezclan: astenia, aumento disnea, etc.

41
CONCLUSIONES ANEMIA E IC.- II
La anemia es frecuente en IC con enfermedad renal. Es mayor cuanto mayor es el grado NYHA Aumenta con la edad. Aumenta con diabetes. ¿Es causa o consecuencia de IC? Es preciso descartar otras causas de anemia. Decidir el tipo adecuado de tratamiento. ¿Influencia tratamiento?. Estudios aleatorizados.

Presentaciones similares









 Noviembre de 2004.>")










