Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Insuficiencia cardiaca

2
DEFINICION “Situación en la cual el corazón es
incapaz de mantener un gasto cardiaco adecuado a los requerimientos metabólicos y al retorno venoso." Definition of Heart Failure. There is no single definition of heart failure. Classically, heart failure is understood as the situation when the heart is incapable of maintaining a cardiac output adequate to accommodate the body’s metabolic requirements and the venous return. This concept is ambiguous and incomplete, however, because heart failure is a composite of clinical symptoms, physical signs, and abnormalities on the hemodynamic, neurohormonal, biochemical, anatomic and cellular levels. In addition, the actual cardiac output, venous return or absolute metabolic requirements are not usually measured in clinical practice. Heart failure is a syndrome characterized by symptoms and physical signs which are secondary to a change in function of the ventricles, valves or load conditions. Braunwald E.: Heart Diseases. W.B. Saunders Co E. Braunwald

3
DEFINICION La insuficiencia cardiaca consiste en un síndrome clínico complejo que puede resultar de cualquier daño estructural o funcional que altere la habilidad del ventrículo para llenarse o expulsar la sangre. Definition of Heart Failure. There is no single definition of heart failure. Classically, heart failure is understood as the situation when the heart is incapable of maintaining a cardiac output adequate to accommodate the body’s metabolic requirements and the venous return. This concept is ambiguous and incomplete, however, because heart failure is a composite of clinical symptoms, physical signs, and abnormalities on the hemodynamic, neurohormonal, biochemical, anatomic and cellular levels. In addition, the actual cardiac output, venous return or absolute metabolic requirements are not usually measured in clinical practice. Heart failure is a syndrome characterized by symptoms and physical signs which are secondary to a change in function of the ventricles, valves or load conditions. Braunwald E.: Heart Diseases. W.B. Saunders Co ACC/AHA 2005 Guideline Update for the Diagnosis and Management of Chronic Heart Failure in the Adult

4
Definición de insuficiencia cardiaca
Síntomas de insuficiencia cardiaca (en reposo o durante el ejercicio), y Evidencia objetiva (preferiblemente por ecocardiografía), de disfunción cardiaca (sistólica y/o diastólica)(en reposo), y (en casos donde el diagnóstico está en duda), Respuesta al tratamiento dirigido a la insuficiencia cardiaca. Los criterios I y II deben cumplirse en todos los casos. Guidelines for the diagnosis and treatment of Chronic Heart Failure (update 2005). European Society of Cardiology
, y. Evidencia objetiva (preferiblemente por ecocardiografía), de disfunción cardiaca (sistólica y/o diastólica)(en reposo), y (en casos donde el diagnóstico está en duda), Respuesta al tratamiento dirigido a la insuficiencia cardiaca. Los criterios I y II deben cumplirse en todos los casos. Guidelines for the diagnosis and treatment of Chronic Heart Failure (update 2005). European Society of Cardiology.")
5
Panorama en U.S.A Prevalencia: aprox. 5 millones de personas
Incidencia: ~ /año Consultas médicas: 12 a 15 millones/año Días hospital: 6.5 millones/año Hospitalizaciones: ~ /año Costo anual: $ 27.9 billones ACC/AHA 2005 Guideline Update for the Diagnosis and Management of Chronic Heart Failure in the Adult

6
Epidemiología En la población europea, la prevalencia de insuficiencia cardiaca sintomática está en el rango del 0.4 al 2% (aprox. 10 millones de pacientes). Esta prevalencia aumenta rápidamente con la edad, con una mediana de 74 años. El pronóstico de esta enfermedad en general es malo. La mitad de los pacientes con un diagnóstico de insuficiencia cardiaca mueren en los próximos 4 años, y en los pacientes con insuficiencia cardiaca severa más del 50% mueren al año. Guidelines for the diagnosis and treatment of Chronic Heart Failure (update 2005). European Society of Cardiology
. Esta prevalencia aumenta rápidamente con la edad, con una mediana de 74 años. El pronóstico de esta enfermedad en general es malo. La mitad de los pacientes con un diagnóstico de insuficiencia cardiaca mueren en los próximos 4 años, y en los pacientes con insuficiencia cardiaca severa más del 50% mueren al año. Guidelines for the diagnosis and treatment of Chronic Heart Failure (update 2005). European Society of Cardiology.")
7
Insuficiencia cardiaca
Es una de las causas más frecuentes de hospitalización Su incidencia aumenta al incrementarse la edad Es la causa más frecuente de hospitalización en el anciano Mortalidad del 50-70% en pacientes clase IV Cardiol Clin 1994;12:1-8

8
Causas de aumento en la frecuencia
Envejecimiento de la población Mejoría en la sobrevida en infarto del miocardio (unidad coronaria y trombolisis) Reducción en la morbimortalidad en HTA debido a un mejor control Aumento en la prevalencia de cardiomiopatía idiopática
 Reducción en la morbimortalidad en HTA debido a un mejor control. Aumento en la prevalencia de cardiomiopatía idiopática.")
9
Factores de riesgo Hipertrofia ventricular izquierda Envejecimiento
Enfermedad coronaria Hipertensión arterial Diabetes Mellitus Obesidad Tabaquismo

10
Incidencia de insuficiencia cardiaca y los factores de riesgo
Riesgo ajustado por edad 35-64 años 65-94 años FR Hombres Mujeres Colesterol 1.2 0.7 0.9 0.8 HTA 4.0** 3.0** 1.9** Diabetes 4.4** 7.7** 2.0** 3.6** HVI-ECG 14.9** 12.8** 4.9** 5.4** Tabaquismo 1.5** 1.1* 1.0 1.3* * p<0.05, ** p<0.001

11
HVI es un factor de riesgo independiente para AVC, insuficiencia cardiaca y EAC
Patients with hypertension have an elevated risk of cardiovascular events compared with normotensive individuals. However, if hypertension is associated with LVH, the overall risk of cardiovascular morbidity and mortality increases even more. Data from the 32-year Framingham Heart Study follow-up of men aged 32–64 years show that the presence of LVH in patients with established hypertension nearly triples the incidence of coronary heart disease and stroke, and increases the incidence of heart failure by about 7-fold.1 1. Kannel WB. Left ventricular hypertrophy as a risk factor in arterial hypertension. Eur Heart J 1992; (Suppl D):82–88. Kannel. Eur Heart J 1992;13 (Suppl D):82–88
:82–88. Kannel. Eur Heart J 1992;13 (Suppl D):82–88.")
12
Etiología Sobrecarga de volumen Sobrecarga de presión
Pérdida de miocardio Disminución en la contractilidad Restricción al llenado

13
Etiología La enfermedad coronaria, la hipertensión y la cardiomiopatía dilatada son las causas más importantes en el mundo occidental. Hasta 30% de los pacientes con una miocardiopatía dilatada tienen una causa genética. La enfermedad valvular cardiaca es otra causa importante de insuficiencia cardiaca.

14
Remodelado ventricular posterior a un infarto agudo
Expansión del infarto (horas a días) Infarto inicial Remodelado global (días a meses) Jessup M, Brozena S. Heart Failure. N Engl J Med 2003;348:
 Infarto inicial. Remodelado global (días a meses) Jessup M, Brozena S. Heart Failure. N Engl J Med 2003;348:")
15
Otras etiologías Hipertensión arterial Diabetes Mellitus
Enfermedades tiroideas Acromegalia, feocromocitoma, hiperaldosteronismo, síndrome de Cushing Embarazo (miocardiopatía peripartum) Familiar (10-15%) Abuso de substancias: alcohol. Uso crónico de anfetaminas y/o uso de cocaína
 Familiar (10-15%) Abuso de substancias: alcohol. Uso crónico de anfetaminas y/o uso de cocaína.")
16
Otras etiologías Agentes quimioterapéuticos: doxorrubicina y otras antraciclinas, ciclofosfamida (daño tóxico al miocito). Interleucina 2 (miocarditis eosinofílica) Agentes farmacológicos: Catecolaminas en dosis altas (efecto cardiotóxico) Medicamentos inotrópicos negativos y que ocasionan retención de líquido (exacerbación de una disfunción cardiaca previa)
. Interleucina 2 (miocarditis eosinofílica) Agentes farmacológicos: Catecolaminas en dosis altas (efecto cardiotóxico) Medicamentos inotrópicos negativos y que ocasionan retención de líquido (exacerbación de una disfunción cardiaca previa)")
17
Otras etiologías Toxinas: plomo, arsénico y cobalto
Toxinas endógenas: uremia y sepsis (factor de necrosis tumoral a) Enfermedades del tejido conectivo: LES, esclerodermia, polimiositis Enfermedades granulomatosas: sarcoidosis Enfermedades infiltrativas: amiloidosis Miocarditis: virales, HIV, Chagas y otras.
 Enfermedades del tejido conectivo: LES, esclerodermia, polimiositis. Enfermedades granulomatosas: sarcoidosis. Enfermedades infiltrativas: amiloidosis. Miocarditis: virales, HIV, Chagas y otras.")
18
Otras etiologías Deficiencias metabólicas: Beriberi, deficiencia de carnitina, coenzima Q-10 Hemoglobinopatías: talasemia (sobrecarga de hierro secundario a transfusiones repetitivas), esferocitosis Estados de alto gasto: hipertiroidismo, anemia crónica severa, fístulas AV, enfermedad de Paget y sepsis Enfermedad valvular cardiaca Idiopática (10-20%)
, esferocitosis. Estados de alto gasto: hipertiroidismo, anemia crónica severa, fístulas AV, enfermedad de Paget y sepsis. Enfermedad valvular cardiaca. Idiopática (10-20%)")
19
Insuficiencia cardiaca
Derecha Retrógrada Izquierda Anterógrada Aguda Crónica Alto gasto Bajo gasto Congestiva Diastólica Sistólica

20
Prevalencia de la insuficiencia cardiaca
10 Proporción con función sistólica VI disminuida Proporción con función sistólica VI conservada 9 8.8 8 8.2 7 7.5 Prevalencia (%) 6.7 6 6.4 5 5.1 4.9 4.8 4 4.5 4.2 4.2 3 3.1 2.9 2 2.1 This graph demonstrates that all over the United States and Europe, about half or more of patients with CHF have preserved LV systolic function. In particular, as age increases, patients are more likely to suffer from CHF due to diastolic dysfunction than CHF due to systolic dysfunction. 1.7 1 1.5 USA (CHS) Finland (Helsinki) England (Poole) Sweden (Vasteras) Den. (Copen.) Spain (Asturias) Portugal (EPICA) Nether. (Rotter.) Rango edad Media 66–103 78 75–86 - 70–84 76 75 50 - > 40 60 > 25 68 55–95 65
 This graph demonstrates that all over the United States and Europe, about half or more of patients with CHF have preserved LV systolic function. In particular, as age increases, patients are more likely to suffer from CHF due to diastolic dysfunction than CHF due to systolic dysfunction USA. (CHS) Finland. (Helsinki) England. (Poole) Sweden. (Vasteras) Den. (Copen.) Spain. (Asturias) Portugal. (EPICA) Nether. (Rotter.) Rango edad. Media. 66– – – > > –")
21
EN RIESGO DE INSUFICIENCIA CARDIACA INSUFICIENCIA CARDIACA
Estadíos en el desarrollo de la insuficiencia cardiaca Estadío Descripción Ejemplos A Alto riesgo de insuficiencia cardiaca debido a la presencia de condiciones fuertemente asociadas con el desarrollo de IC, sin cardiopatía estructural o síntomas de insuficiencia cardiaca Hipertensión, Obesidad Enfermedad aterosclerótica Diabetes, Síndrome Metabólico HF de cardiomiopatía, uso de cardiotoxinas B Pacientes con enfermedad cardiaca estructural sin síntomas o signos de insuficiencia cardiaca IM previo Remodelado VI: HVI y FE ↓ Valvulopatía asintomática C Enfermedad cardiaca estructural con síntomas previos o actuales de insuficiencia cardiaca Disnea y fatiga Tolerancia reducida al ejercicio D IC refractaria que requiere intervenciones especializadas Síntomas marcados en reposo a pesar de tratamiento intensivo Hospitalizaciones frecuentes EN RIESGO DE INSUFICIENCIA CARDIACA INSUFICIENCIA CARDIACA ACC/AHA 2005 guideline update for the diagnosis and management of chronic heart failure in the adult

22
Insuficiencia cardiaca
EVOLUCION DE ESTADIOS CLINICOS NORMAL No síntomas Ejercicio normal Fx VI normal Disfunción VI asintomática No síntomas Ejercicio normal Fx VI alterada ICC compensada Important Concepts. Clinical stages in the evolution of heart failure Heart failure is a continuous spectrum of changes, from the subtle loss of normal function to the presence of symptoms refractory to medial therapy. The patient with cardiomyopathy may maintain overall normal ventricular function; the progression of dysfunction may be sudden or gradual. Asymptomatic ventricular dysfunction is characterized by the absence of symptoms or decline in functional capacity, even in the absence of treatment. It may be associated with different changes in cardiac physiology, including ventricular dilatation, regional wall motion abnormalities, and decreases in the LV ejection fraction and of other parameters of ventricular function. The absence of symptoms may be explained by the heart’s functional reserve capacity and by the activation of compensatory mechanisms opposing the deterioration of cardiac function. In compensated heart failure the symptoms are controlled by medical therapy. In decompensated heart failure, symptoms persist despite usual therapy and are refractory to adjustments in drugs and dosages. No síntomas ejercicio Fx VI alterada ICC descompensada Síntomas ejercicio Fx VI alterada ICC refractaria Síntomas no controlados con tratamiento

23
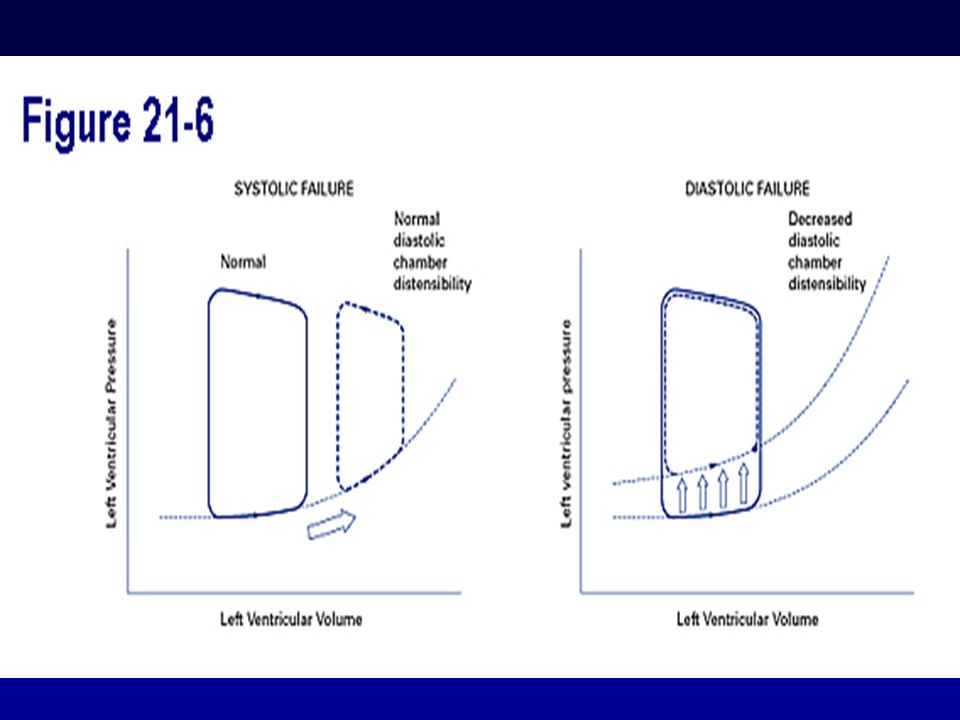
Efectos hemodinámicos
Normal Volumen latido ICC Presión de llenado ventricular

24
Fisiopatología. Mecanismos Compensadores
Mecanismo de Frank-Starling a. En reposo, sin IC b. IC debida a disfunción del VI c. IC avanzada The Frank-Starling mechanism plays an important compensatory role in the early stages of HF, which is demonstrated in this slide. On the graph, there are three points, A, B, and C. Point A is a healthy patient where cardiac performance increases as preload increases (the amount of stretch on the ventricle before contraction due to an increase in volume). Point B represents the same individual after developing LV systolic dysfunction. Since the heart is no longer able to contract as effectively as it did, stroke volume falls. As a result, there is a decrease in LV emptying which leads to an elevation of the end-diastolic volume (preload). Since point B is on the ascending portion of the curve, the increased end-diastolic volume initially serves a compensatory role because it leads to a subsequent increase in stroke volume (i.e., more diastolic stretch, the greater the contractility, and the greater the stroke volume...the Frank-Starling mechanism). This is less than the increase a normal patient would experience. As the patient’s heart failure progresses (represented by point C), which is on the relatively flat portion of the curve, stroke volume only increases slightly relative to further increases in end-diastolic volume (preload). Here the ability of the Frank-Starling mechanism to compensate for worsening LV function is nearly exhausted. In such circumstances, marked elevation of the end-diastolic volume and end-diastolic pressure results in pulmonary congestion, while decreasing cardiac output leads to increasing fatigue and exercise intolerance. Eventually, the curve starts downward due to decompensation of the heart muscle. It is of note that when cardiac resynchronization (discussed later) is implemented, the hope is to put the HF patient back on top of the curve rather than on the downward slope.
. Point B represents the same individual after developing LV systolic dysfunction. Since the heart is no longer able to contract as effectively as it did, stroke volume falls. As a result, there is a decrease in LV emptying which leads to an elevation of the end-diastolic volume (preload). Since point B is on the ascending portion of the curve, the increased end-diastolic volume initially serves a compensatory role because it leads to a subsequent increase in stroke volume (i.e., more diastolic stretch, the greater the contractility, and the greater the stroke volume...the Frank-Starling mechanism). This is less than the increase a normal patient would experience. As the patient’s heart failure progresses (represented by point C), which is on the relatively flat portion of the curve, stroke volume only increases slightly relative to further increases in end-diastolic volume (preload). Here the ability of the Frank-Starling mechanism to compensate for worsening LV function is nearly exhausted. In such circumstances, marked elevation of the end-diastolic volume and end-diastolic pressure results in pulmonary congestion, while decreasing cardiac output leads to increasing fatigue and exercise intolerance. Eventually, the curve starts downward due to decompensation of the heart muscle. It is of note that when cardiac resynchronization (discussed later) is implemented, the hope is to put the HF patient back on top of the curve rather than on the downward slope.")
25
Fisiopatología. Mecanismos Compensadores
Activación Neurohormonal Muchos mecanismos hormonales distintos están comprometidos en mantener una homeostasis cardiovascular normal e incluyen: Sistema Nervioso Simpático (SNS) Sistema Renina-Angiotensina-Aldosterona(SRAA) Vasopresina (hormona antidiurética, HAD) Neurohormonal activation is an important compensatory mechanism involved in maintaining the mean arterial pressure. Hormones and neurohormonal systems play a important role in maintaining normal cardiovascular hemostasis; they also play an important compensatory role in the early stages of heart failure. First, let’s start by defining what a neurohormone is. A hormone is simply a biologically active substance that originates in one tissue and is transported through the bloodstream to another part of the body where it acts to either increase the activity of that tissue or stimulate the release of another hormone. Hormones that are formed by neurosecretory cells and are liberated by nerve stimulation are called neurohormones. In general, activation of the body’s various neurohormonal systems serve to increase systemic vascular resistance, thereby attenuating any fall in blood pressure (recall: Blood Pressure = Cardiac Output x Total Peripheral Vascular Resistance). In addition, many neurohormones encourage salt and water retention, which increases intravascular volume and LV preload so as to maximize stroke volume via the Frank-Starling mechanism. But as was the case with remodeling, too much of a good thing over the long-term eventually becomes detrimental to the failing heart. Because of the importance of neurohormonal activation in the cascade of events that lead to chronic heart failure, and ultimately death, the following slides will review the various neurohormones and neurohormonal systems in detail, starting with their role in maintaining normal cardiovascular hemostasis, and then later their contribution to the progression of heart failure. The acute effects of neurohormonal stimulation are beneficial but the long term or chronic activation of these mechanisms is detrimental.
 Sistema Renina-Angiotensina-Aldosterona(SRAA) Vasopresina (hormona antidiurética, HAD) Neurohormonal activation is an important compensatory mechanism involved in maintaining the mean arterial pressure. Hormones and neurohormonal systems play a important role in maintaining normal cardiovascular hemostasis; they also play an important compensatory role in the early stages of heart failure. First, let’s start by defining what a neurohormone is. A hormone is simply a biologically active substance that originates in one tissue and is transported through the bloodstream to another part of the body where it acts to either increase the activity of that tissue or stimulate the release of another hormone. Hormones that are formed by neurosecretory cells and are liberated by nerve stimulation are called neurohormones. In general, activation of the body’s various neurohormonal systems serve to increase systemic vascular resistance, thereby attenuating any fall in blood pressure (recall: Blood Pressure = Cardiac Output x Total Peripheral Vascular Resistance). In addition, many neurohormones encourage salt and water retention, which increases intravascular volume and LV preload so as to maximize stroke volume via the Frank-Starling mechanism. But as was the case with remodeling, too much of a good thing over the long-term eventually becomes detrimental to the failing heart. Because of the importance of neurohormonal activation in the cascade of events that lead to chronic heart failure, and ultimately death, the following slides will review the various neurohormones and neurohormonal systems in detail, starting with their role in maintaining normal cardiovascular hemostasis, and then later their contribution to the progression of heart failure. The acute effects of neurohormonal stimulation are beneficial but the long term or chronic activation of these mechanisms is detrimental.")
26
Fisiopatología. Activación Simpática en Insuficiencia Cardiaca
Estímulo simpático del SNC Actividad simpática cardiaca Actividad Simpática hacia riñones + vasculatura periférica receptores 1- 2- 1- Activación del SRAA 1- b1- The sympathetic nervous system’s goal is to increase cardiac sympathetic activity. This response is mediated through three receptors: Beta 1, Beta 2, and Alpha 1. In normal situations the Beta 1 receptor increases cardiac sympathetic activity. In heart failure patients, the Beta 1 and Beta 2 receptors are activated. Alpha receptors and their role is yet to be fully delineated. Beta 1, Beta 2, and Alpha 1 receptors lead to myocardial toxicity in the ventricles. Myocardial toxicity leads to decreased ejection fraction, arrhythmias, and tachyarrhythmias caused by sympathetic activation. Increase in sympathetic activity also affects the kidneys and peripheral vasculature through the Beta 1 and Alpha 1 receptors. This mediates activation of the renin-angiotensin system ( discussed on the next slide ), which causes vasoconstriction, sodium retention, and thirst. All of these responses causes the disease to progress. Prolonged neurohormone release also has direct adverse effects on the heart tissue itself. Norepinephrine, for example, is known to be directly cardiotoxic. In fact, studies have established that in patients with heart failure, the probability of survival is markedly worse for those whose plasma norepinephrine levels are >400 pg/ml than for those whose levels are <400 pg/ml. Toxicidad Miocárdica Aumento de arritmias Vasoconstricción Retención Sodio Progreso De la Enfermedad Packer. Progr Cardiovasc Dis. 1998;39(suppl I):39-52.
, which causes vasoconstriction, sodium retention, and thirst. All of these responses causes the disease to progress. Prolonged neurohormone release also has direct adverse effects on the heart tissue itself. Norepinephrine, for example, is known to be directly cardiotoxic. In fact, studies have established that in patients with heart failure, the probability of survival is markedly worse for those whose plasma norepinephrine levels are >400 pg/ml than for those whose levels are <400 pg/ml. Toxicidad Miocárdica. Aumento de arritmias. Vasoconstricción. Retención Sodio. Progreso. De la Enfermedad. Packer. Progr Cardiovasc Dis. 1998;39(suppl I):")
27
Fisiopatología. Mecanismos Compensadores: Sistema Renina-Angiotensina-Aldosterona (SRAA)
Angiotensinógeno Renina Angiotensina I Enzima Convertidora de Angiotensina (IECA) Angiotensina II Receptor AT I The other mechanism in the neurohumoral response to heart failure is the renin-angiotensin-aldosterone system (RAAS). In the RAAS, Renin ( secreted by the kidney ) acts on Angiotensinogen (secreted by the liver) to make Angiotensin I. The Angiotensin converting enzyme (secreted by the lungs) acts on Angiotensin I to make Angiotensin II. Angiotensin II in turn causes vasoconstriction, an increase in aldosterone, facilitates the release of norepinephrine from the SNS, causes sodium reabsorption, stimulates vasopressin secretion from the brain (discussed later), and increases contractility. Subsequently, remodeling of the heart occurs. In a heart failure patient, the effects of Angiotensin II are not beneficial. Why not think about using a medication to block the conversion of Angiotensin I to II? Or, an agent that blocks the Angiotensin I receptor? These blocking agents will be discussed later when we talk about the treatment of heart failure. Vasoconstricción Remodelado Vascular Estrés Oxidativo Remodelado VI Crecimiento Celular Proteinuria
 Angiotensina II. Receptor AT I. The other mechanism in the neurohumoral response to heart failure is the renin-angiotensin-aldosterone system (RAAS). In the RAAS, Renin ( secreted by the kidney ) acts on Angiotensinogen (secreted by the liver) to make Angiotensin I. The Angiotensin converting enzyme (secreted by the lungs) acts on Angiotensin I to make Angiotensin II. Angiotensin II in turn causes vasoconstriction, an increase in aldosterone, facilitates the release of norepinephrine from the SNS, causes sodium reabsorption, stimulates vasopressin secretion from the brain (discussed later), and increases contractility. Subsequently, remodeling of the heart occurs. In a heart failure patient, the effects of Angiotensin II are not beneficial. Why not think about using a medication to block the conversion of Angiotensin I to II Or, an agent that blocks the Angiotensin I receptor These blocking agents will be discussed later when we talk about the treatment of heart failure. Vasoconstricción. Remodelado Vascular. Estrés Oxidativo. Remodelado VI. Crecimiento Celular. Proteinuria.")
28
Renina-Angiotensina-Aldosterona
Fisiopatología. Mecanismos Compensadores: Sistema Renina-Angiotensina-Aldosterona (SRAA) Descenso de la PAM Renina-Angiotensina-Aldosterona ( perfusión renal) Aumento Simpático Retención Sodio-agua Sed So, when there is a decrease in the mean arterial pressure, there is decreased renal perfusion. Hence, the RAAS is stimulated, and the MAP is increased. Vasoconstricción PAM = (VS x FC) x RTP
 Descenso de la PAM. Renina-Angiotensina-Aldosterona. ( perfusión renal) Aumento. Simpático. Retención Sodio-agua. Sed. So, when there is a decrease in the mean arterial pressure, there is decreased renal perfusion. Hence, the RAAS is stimulated, and the MAP is increased. Vasoconstricción. PAM = (VS x FC) x RTP.")
29
Fisiopatología. Estimulación Compensadora Neurohormonal: Resumen
Gasto Cardiaco Disminuido Sistema Nervioso Simpático Sistema Renina-angiotensina Hormona Antidiurética (vasopresina) Frec. Cardiaca Contractilidad Vasoconstricción Volumen circulante Anteriolar Mantener presión arterial Gasto Cardiaco Volumen Latido + - Venosa Retorno Venoso al corazón ( precarga) Edema Periférico y congestión pulmonar This slide shows a summary of the compensatory neurohormonal mechanisms that occur when there is a decrease in the cardiac output. As you can see, adverse consequences occur (dotted lines) secondary to these activations. Flow chart from Pathophysiology Of Heart Disease, Second Edition, by Leonard S. Lilly, page 205.
 Frec. Cardiaca. Contractilidad. Vasoconstricción. Volumen circulante. Anteriolar. Mantener presión arterial. Gasto. Cardiaco. Volumen. Latido. + - Venosa. Retorno Venoso al corazón ( precarga) Edema Periférico y congestión. pulmonar. This slide shows a summary of the compensatory neurohormonal mechanisms that occur when there is a decrease in the cardiac output. As you can see, adverse consequences occur (dotted lines) secondary to these activations. Flow chart from Pathophysiology Of Heart Disease, Second Edition, by Leonard S. Lilly, page 205.")
30
Fisiopatología. Círculo Vicioso de la Insuficiencia Cardiaca
Disfunción VI Gasto cardiaco disminuido y Presión arterial disminuída Trabajo cardiaco aumentado (ya sea precarga o postcarga) In addition to maintaining normal cardiovascular homeostasis, the hormones and neurohormonal systems described in the last few slides also play an important role in compensating for the diminished cardiac output seen in patients with early heart failure. But it is also known that over time, these same neurohormone systems eventually become detrimental and contribute to the progression of heart failure. Why does this happen? Physiologists now recognize that the neurohormonal mechanisms activated in heart failure are identical to those normally triggered when cardiac output and blood pressure are threatened (e.g., intense physical exercise, hemorrhage), but with an important difference. Under normal circumstances, the release of neurohormones is generally successful in reversing the hemodynamic abnormalities seen in acute low volume/low output states, and consequently, neurohormonal activity eventually subsides. In contrast, neurohormonal activation never “turns off” in the setting of heart failure; rather, is always “on” in an attempt to compensate for the failing heart’s chronic inability to maintain normal cardiovascular homeostasis. Furthermore, the chronic presence of circulating neurohormones tends to exacerbate the hemodynamic abnormalities in heart failure, which only encourages further remodeling and neurohormone release and, thus, further hemodynamic deterioration. Thus, a vicious cycle develops whose end result is progressive ventricular dysfunction and death. Aumento del Gasto Cardiaco (via aumento de contractilidad y frecuencia cardiaca) Aumento de Presión Arterial (via vasoconstricción y aumento de volumen sanguíneo) Mecanismo de Frank-Starling Remodelado Activación Neurohormonal
 In addition to maintaining normal cardiovascular homeostasis, the hormones and neurohormonal systems described in the last few slides also play an important role in compensating for the diminished cardiac output seen in patients with early heart failure. But it is also known that over time, these same neurohormone systems eventually become detrimental and contribute to the progression of heart failure. Why does this happen Physiologists now recognize that the neurohormonal mechanisms activated in heart failure are identical to those normally triggered when cardiac output and blood pressure are threatened (e.g., intense physical exercise, hemorrhage), but with an important difference. Under normal circumstances, the release of neurohormones is generally successful in reversing the hemodynamic abnormalities seen in acute low volume/low output states, and consequently, neurohormonal activity eventually subsides. In contrast, neurohormonal activation never turns off in the setting of heart failure; rather, is always on in an attempt to compensate for the failing heart’s chronic inability to maintain normal cardiovascular homeostasis. Furthermore, the chronic presence of circulating neurohormones tends to exacerbate the hemodynamic abnormalities in heart failure, which only encourages further remodeling and neurohormone release and, thus, further hemodynamic deterioration. Thus, a vicious cycle develops whose end result is progressive ventricular dysfunction and death. Aumento del Gasto Cardiaco (via aumento. de contractilidad y frecuencia cardiaca) Aumento de Presión Arterial (via vasoconstricción y aumento de volumen sanguíneo) Mecanismo de Frank-Starling. Remodelado. Activación Neurohormonal.")
31
Fisiopatología. Mecanismos Compensadores
Remodelado Ventricular Alteraciones en el tamaño, forma, estructura y función del corazón en respuesta a los cambios hemodinámicos crónicos de la insuficiencia cardiaca. Ventricular Remodeling: Heart failure is a progressive disease, and the chronic hemodynamic stresses imparted on the failing heart eventually lead to alterations in the heart’s size, shape, structure, and function. This process is known as remodeling. As the heart remodels, its overall geometry changes; it becomes less elliptical and more spherical. There are also changes in ventricular mass, composition, and volume. Initially, the changes that occur with remodeling can be considered compensatory. For example, the dysfunctioning heart has a compromised stroke volume; thus, from a remodeling perspective, one adaptive mechanism to maintain stroke volume is to enlarge the ventricular volume (ventricular dilatation) so that a greater stroke volume results from a reduced ejection fraction. Remodeling also increases myocardial mass, resulting in increased ventricular wall thickness (hypertrophy). This added wall thickness initially helps reduce ventricular wall stress and improve contractility. It is the progressive nature of remodeling that occurs in the failing heart that eventually becomes detrimental. Continued hypertrophy and dilatation of the ventricle inevitably leads to increasing ventricular wall stress, and ongoing fibrosis of the damaged myocardium increasingly impairs contractility. Thus, the events associated with remodeling eventually become self-propagating and harmful. This remodeling is felt to cause an increase in cell death ( apoptosis). Text from the article: Images were generated by tagged magnetic resonance imaging, which offers a unique noninvasive tool for determining and displaying high-resolution 3D wall motion in patients. Two images are displayed in the Figure: on the left, a normal control patient is seen, and to the right, a patient with severe cardiomyopathy and left bundle branch morphology conduction delay is shown (each image is activated by double clicking over it with the mouse). During systolic contraction, the colors change, reflecting the distribution and timing of regional circumferential strains. Red coding corresponds to the diastolic relaxed state; shortening, by a transition from red to blue; and stretch, by red to yellow. In the normal heart, contraction is synchronous within the myocardium, with a normal symmetric distribution of negative strain (≈-20% by end-systole) across the wall. In contrast, the contraction pattern is markedly dyssynchronous in the heart with dilated cardiomyopathy. Myocardium in the septal region (green dot denotes septum) becomes first blue in early systole and then yellow (i.e., stretching) in late systole. Contraction slowly spreads to the lateral wall as the septum develops positive strains. The temporal magnitude of dyssynchrony is substantial. In this and other such patients, ventricular free wall (or biventricular) pacing with pre-excitation enhances the systolic function of the heart. Curry CW, et al. Mechanical dyssynchrony in dilated cardiomyopathy with intraventricular conduction delay as depicted by 3D tagged magnetic resonance imaging. Circulation 2000 Jan 4;101(1):E2.
 so that a greater stroke volume results from a reduced ejection fraction. Remodeling also increases myocardial mass, resulting in increased ventricular wall thickness (hypertrophy). This added wall thickness initially helps reduce ventricular wall stress and improve contractility. It is the progressive nature of remodeling that occurs in the failing heart that eventually becomes detrimental. Continued hypertrophy and dilatation of the ventricle inevitably leads to increasing ventricular wall stress, and ongoing fibrosis of the damaged myocardium increasingly impairs contractility. Thus, the events associated with remodeling eventually become self-propagating and harmful. This remodeling is felt to cause an increase in cell death ( apoptosis). Text from the article: Images were generated by tagged magnetic resonance imaging, which offers a unique noninvasive tool for determining and displaying high-resolution 3D wall motion in patients. Two images are displayed in the Figure: on the left, a normal control patient is seen, and to the right, a patient with severe cardiomyopathy and left bundle branch morphology conduction delay is shown (each image is activated by double clicking over it with the mouse). During systolic contraction, the colors change, reflecting the distribution and timing of regional circumferential strains. Red coding corresponds to the diastolic relaxed state; shortening, by a transition from red to blue; and stretch, by red to yellow. In the normal heart, contraction is synchronous within the myocardium, with a normal symmetric distribution of negative strain (≈-20% by end-systole) across the wall. In contrast, the contraction pattern is markedly dyssynchronous in the heart with dilated cardiomyopathy. Myocardium in the septal region (green dot denotes septum) becomes first blue in early systole and then yellow (i.e., stretching) in late systole. Contraction slowly spreads to the lateral wall as the septum develops positive strains. The temporal magnitude of dyssynchrony is substantial. In this and other such patients, ventricular free wall (or biventricular) pacing with pre-excitation enhances the systolic function of the heart. Curry CW, et al. Mechanical dyssynchrony in dilated cardiomyopathy with intraventricular conduction delay as depicted by 3D tagged magnetic resonance imaging. Circulation 2000 Jan 4;101(1):E2.")
32
Ley de Laplace P x r T = W T = tensión P = presión r = radio
W= grosor de pared

33
Respuesta neurohormonal
Aldosterona Angiotensina II Norepinefrina Respuesta similar a hipovolemia

34
Remodelado ventricular en insuficiencia cardiaca diastólica y sistólica
Corazón normal Hipertrofia ventricular (insuficiencia cardiaca diastólica) Dilatación ventricular (insuficiencia cardiaca sistólica) Jessup M, Brozena S. Heart Failure. N Engl J Med 2003;348:
 Dilatación ventricular. (insuficiencia cardiaca sistólica) Jessup M, Brozena S. Heart Failure. N Engl J Med 2003;348:")
36
Mecanismos de compensación
Efecto beneficioso Consecuencia deletérea Inmediato Retención sodio/agua volumen intravascular con GC y PA estrés parietal, congestión pulmonar y sistémica Vasoconstriccíón periférica retorno venoso, PA estrés parietal, congestión pulmonar frecuencia cardiaca GC MVO2 contractilidad Greenberg BH, Hermann DD. Contemporary Diagnosis and Management of Heart Failure, 2002.

37
Mecanismos de compensación
Efecto beneficioso Consecuencia deletérea Largo plazo Hipertrofia miocárdica generación de fuerza causado por un número de unidades contráctiles (sárcomeros) Normalización del estrés parietal Alteraciones funcionales y estructurales de las proteínas dentro del miocito Desbalance aporte/demanda energía fibrosis Dilatación de cámaras volumen latido estrés parietal, insuficiencia valvular 2a Greenberg BH, Hermann DD. Contemporary Diagnosis and Management of Heart Failure, 2002.
 Normalización del estrés parietal. Alteraciones funcionales y estructurales de las proteínas dentro del miocito. Desbalance aporte/demanda energía. fibrosis. Dilatación de cámaras. volumen latido. estrés parietal, insuficiencia valvular 2a. Greenberg BH, Hermann DD. Contemporary Diagnosis and Management of Heart Failure,")
38
PRECARGA POSTCARGA Volumen telediastólico del ventrículo
Tensión de la pared ventricular durante la sístole

39
Propiedades del corazón
Batmotropismo Excitabilidad Cronotropismo Automatismo Dromotropismo Conductibilidad Inotropismo Contractilidad

40
Mecanismos de Compensación
A largo plazo: Mecanismo de Frank-Starling Activación de los sistemas neurohumorales A corto plazo Remodelación cardiaca : Los ventrículos tratan de compensar la sobrecarga hemodinámica por medio de la hipertrofia.

41
Sobrecarga de presión Aumento de la presión sistólica Aumenta tension sistolica de la pared Adición paralela de miofibrillas Engrosamiento parietal Hipertrofia concéntrica Estos son los tipos de remodelado del ventrículo como respuesta al aumento de la carga de trabajo. La hipertrofia concentrica: Tiene aumento desproporcionado de la masa en relación con el volumen de la cavidad y reduce la tensión sistólica de la pared cuando se eleva la carga de presión.

42
Sobrecarga de volumen Aumento de la presión diastólica Aumento de la tensión diastólica de la pared Adición seriada de nuevos sarcomeros Aumento del tamaño de la cavidad Hipertrofia excéntrica Cuando hay sobre carga de volumen el principal estímulo es la carga diastólica, la relación entre masa y volumen se mantiene .

43
Manejo del paciente pediátrico quemado
Insuficiencia Cardiaca Gasto cardiaco reducido Presión de llenado cardiaca alta Renina Activación del SNS Angiotensina I Vasoconstricción Angiotensina II Retención de sodio y agua Aldosterona Restructuración cardiaca 43

44
Manifestaciones clínicas de insuficiencia cardiaca
Las manifestaciones cardinales de la insuficiencia cardiaca son la disnea y la fatiga, que limitan la tolerancia al ejercicio y la retención de líquido que puede llevar a congestión pulmonar y edema periférico.

45
Síntomas y signos Disnea Disnea de esfuerzo Ortopnea
Disnea paroxística nocturna Ritmo de galope Crepitantes pulmonares o sibilancias Edema

46
Síntomas y signos Insuficiencia cardiaca congestiva
Disnea (de reposo o esfuerzo) Disnea paroxística nocturna Malestar abdominal o epigástrico Náuseas o anorexia Edema podálico Trastornos del sueño (ansiedad) Ortopnea Tos Ascitis Aumento de peso
 Disnea paroxística nocturna. Malestar abdominal o epigástrico. Náuseas o anorexia. Edema podálico. Trastornos del sueño (ansiedad) Ortopnea. Tos. Ascitis. Aumento de peso.")
47
Síntomas y signos Insuficiencia cardiaca de bajo gasto Fatiga fácil
Náuseas o anorexia Pérdida de peso inexplicada Trastornos de la concentración o la memoria Alteraciones del sueño Desnutrición Tolerancia disminuida al ejercicio Pérdida de masa muscular o debilidad Oliguria durante el día con nicturia

48
Examen físico Inspección venosa
Ingurgitación yugular (especialmente > 15 cm de H2O) Signo de Kussmaul (ausencia de colapso inspiratorio) Ondas v gigantes en el pulso yugular (insuficiencia tricuspídea severa) Reflujo abdominoyugular (sobrecarga de volumen) Hepatomegalia
 Signo de Kussmaul (ausencia de colapso inspiratorio) Ondas v gigantes en el pulso yugular (insuficiencia tricuspídea severa) Reflujo abdominoyugular (sobrecarga de volumen) Hepatomegalia.")
49
Examen físico Inspección arterial
Pulsos carotídeos (estenosis aórtica, cardiomiopatía hipertrófica), soplos (aterosclerosis) Disminución de pulsos periféricos (aterosclerosis) Pulso alternante: implica un bajo gasto cardiaco y disfunción sistólica severa del VI
, soplos (aterosclerosis) Disminución de pulsos periféricos (aterosclerosis) Pulso alternante: implica un bajo gasto cardiaco y disfunción sistólica severa del VI.")
50
Examen físico Perfusión periférica
Extremidades frías o con vasoconstricción, con o sin cianosis leve (GC ¯ y RVS ) Edema: Sin ingurgitación yugular: insuficiencia venosa crónica, trombosis venosa, hipoalbuminemia o hepatopatía Ascitis desproporcionada al edema en MsIs: cardiomiopatía restrictiva/constrictiva o insuficiencia tricuspídea severa
 Edema: Sin ingurgitación yugular: insuficiencia venosa crónica, trombosis venosa, hipoalbuminemia o hepatopatía. Ascitis desproporcionada al edema en MsIs: cardiomiopatía restrictiva/constrictiva o insuficiencia tricuspídea severa.")
51
Examen físico Palpación y percusión del tórax
Latido apexiano: crecimiento cardiaco Latido sostenido con 4R, sugiere HVI Latido paraesternal bajo: HVD Ruido del cierre pulmonar palpable: hipertensión pulmonar Latido apexiano desplazado hacia abajo y hacia fuera: dilatación ventricular Acompañado de un 3R: disfunción sistólica del ventrículo izquierdo

52
Examen físico Palpación y percusión del tórax
Latido apexiano: crecimiento cardiaco Latido sostenido con 4R, sugiere HVI Latido paraesternal bajo: HVD Ruido del cierre pulmonar palpable: hipertensión pulmonar Latido apexiano desplazado hacia abajo y hacia fuera: dilatación ventricular Acompañado de un 3R: disfunción sistólica del ventrículo izquierdo

53
Examen físico Auscultación
Soplos cardiacos: estenosis e insuficiencia aórtica, estenosis e insuficiencia mitral Campos pulmonares: derrame pleural, crepitantes, sibilantess (asma cardiaca) Ritmo de galope
 Ritmo de galope.")
54
Insuficiencia cardiaca izquierda

55
Insuficiencia cardiaca derecha

56
Clasificación funcional New York Heart Association
Clase I. La actividad física acostumbrada no provoca síntomas (fatiga, palpitaciones, disnea, angor). Clase II. La actividad física acostumbrada provoca síntomas. Clase III. La actividad física menor que la acostumbrada provoca síntomas. Clase IV. Síntomas en reposo.
. Clase II. La actividad física acostumbrada provoca síntomas. Clase III. La actividad física menor que la acostumbrada provoca síntomas. Clase IV. Síntomas en reposo.")
57
Estudio Framingham Mortalidad Muerte súbita
62 % en hombres a los 5 años 42% en mujeres a los 5 años 75% después de 9 años del inicio clínico Muerte súbita 25% en hombres, 13% en mujeres

58
Pronóstico Mortalidad anual (%)
Greenberg BH, Hermann DD. Contemporary Diagnosis and Management of Heart Failure, 2002.

59
Diagnóstico diferencial
Disnea con o sin edema Enfermedad parenquimatosa pulmonar, obstructiva crónica o intersticial Enfermedad pulmonar tromboembólica Cor pulmonale Hipertensión pulmonar primaria y secundaria Asma inducida por el ejercicio Anemia severa Estenosis mitral Enfermedad neuromuscular Pericarditis constrictiva Causas metabólicas (acidosis)
")
60
Diagnóstico diferencial
Edema con o sin disnea Síndrome nefrótico Cirrosis Insuficiencia venosa Insuficiencia vascular combinada Linfedema

61
Laboratorio Hemograma completo Orina Sodio, potasio, calcio, magnesio
Nitrógeno ureico, creatinina Glicemia Función hepática TSH

62
Exámenes de gabinete ECG de 12 derivaciones y radiografía de tórax.
Ecocardiograma bidimensional y doppler. Arteriografía coronaria en pacientes con angina o sospecha de isquemia miocárdica. Una alternativa pueden ser los estudios de imágenes (ecocardiograma con dobutamina, estudio de perfusión miocárdica con sestamibi o Talio), para valorar isquemia y viabilidad.
, para valorar isquemia y viabilidad.")
63
Otros exámenes Tamizaje por hemocromatosis, apnea del sueño o VIH.
Pruebas diagnósticas para enfermedades reumatológicas, amiloidosis o feocromocitoma. Medición del péptido natriurético tipo B (BNP), que puede ser de utilidad en la evaluación de pacientes que se presentan en los servicios de emergencias y en quienes el diagnóstico es incierto.
, que puede ser de utilidad en la evaluación de pacientes que se presentan en los servicios de emergencias y en quienes el diagnóstico es incierto.")
64
Péptidos natriuréticos
1. Neurohormona cardiaca que se segrega en los ventrículos, aunque también un poco en el tejido auricular. 2. Es liberado desde el VI en respuesta a la dilatación volumétrica y a la sobrecarga de presión 3. ANP (Péptidonatriurético atrial) 4. BNP (Péptido natriurético “brain”) En cerebro, y en mayor cantidad en el músculo cardiaco. 5. CNP: en endotelio vascular y riñón. BNP: – Sintetizado como precursor por los miocardiocitos en función de la tensión de la pared. Se transforma en pro-BNP, el cual se escinde en dos partes al liberarse: fragmento N-terminal (76 aminoácidos) y C-terminal (32 aminoácidos) – Aunque la relación molecular de BNP/proBNP es de 1/1, dado que el proBNP tiene una vida media mayor que el BNP (90 min/ 20 min), las concentraciones sanguíneas del proBNP son entre 5-10 veces mayores que el BNP)
 4. BNP (Péptido natriurético brain ) En cerebro, y en mayor cantidad en el músculo cardiaco. 5. CNP: en endotelio vascular y riñón. BNP: – Sintetizado como precursor por los miocardiocitos en función de la tensión de la pared. Se transforma en pro-BNP, el cual se escinde en dos partes al liberarse: fragmento N-terminal (76 aminoácidos) y C-terminal (32 aminoácidos) – Aunque la relación molecular de BNP/proBNP es de 1/1, dado que el proBNP tiene una vida media mayor que el BNP (90 min/ 20 min), las concentraciones sanguíneas del proBNP son entre 5-10 veces mayores que el BNP)")
65
Fisiopatología. Otras Neurohormonas (Péptidos Natriuréticos).
1.- Péptido Natriurético Atrial (ANP) Encontrado en las aurículas (sobrecarga y distension). 2.- Péptido Natriurético Cerebral (hBNP) Encontrado en los ventrículos (dilatación). 3.- Péptido Natriurético tipo C (CNP) Encontrado en el SNC. Propiedades limitadas. Vasodilatadoras (actúan sobre los vasos sanguíneos). - Efectos natriuréticos (excreción de sal) y diuréticos (excreción de agua). - Inhinem la secreción de renina, aldosterona y vasopresina (vasoconstrictivas). Natriuretic Peptides The third neurohormone system on our list includes the natriuretic peptides. The natriuretic peptides—ANP, BNP, and CNP-- are vasodilating neurohormones. As such, they play an important role in counter-regulating the vasoconstricting effects of other neurohormones. These peptides are made and stored in specialized cells in the atria and ventricles, and are released when the atria are stretched (e.g., in volume overload, which distends the atria) or when the ventricles are dilated. The natriuretic peptides act directly on blood vessels to cause vasodilatation. They also have natriuretic (salt excreting) and diuretic (water excreting) effects because of their ability to inhibit the secretion of renin, aldosterone, and vasopressin.
 Encontrado en las aurículas (sobrecarga y distension). 2.- Péptido Natriurético Cerebral (hBNP) Encontrado en los ventrículos (dilatación). 3.- Péptido Natriurético tipo C (CNP) Encontrado en el SNC. Propiedades limitadas. Vasodilatadoras (actúan sobre los vasos sanguíneos). - Efectos natriuréticos (excreción de sal) y diuréticos (excreción de agua). - Inhinem la secreción de renina, aldosterona y vasopresina (vasoconstrictivas). Natriuretic Peptides. The third neurohormone system on our list includes the natriuretic peptides. The natriuretic peptides—ANP, BNP, and CNP-- are vasodilating neurohormones. As such, they play an important role in counter-regulating the vasoconstricting effects of other neurohormones. These peptides are made and stored in specialized cells in the atria and ventricles, and are released when the atria are stretched (e.g., in volume overload, which distends the atria) or when the ventricles are dilated. The natriuretic peptides act directly on blood vessels to cause vasodilatation. They also have natriuretic (salt excreting) and diuretic (water excreting) effects because of their ability to inhibit the secretion of renin, aldosterone, and vasopressin.")
66
Factores que modifican los valores del BNP
El punto de corte (difícil de establecer) para BNP es de 100 pg/ml y de 300 pg/ml para el NT Pro BNP. Obeso disminuye Edad Sexo femenino I Renal Enf pulmonar TEP Sind. Coron. Agudo Hipertiroidismo Cirrosis Glucocorticoides HSA
 para BNP es de 100 pg/ml y de 300. pg/ml para el NT Pro BNP. Obeso disminuye. Edad. Sexo femenino. I Renal. Enf pulmonar. TEP. Sind. Coron. Agudo. Hipertiroidismo. Cirrosis. Glucocorticoides. HSA.")
67
Aplicaciones fundamentales del BNP
1. Diagnóstico de IC – En función del punto de corte y los factores individuales. – Su mayor utilidad radica en su poder predictivo negativo (BNP normal: descarta IC) – Solicitar en situaciones de disnea de diagnóstico dudoso. 2. Evaluación de la gravedad (pronóstico) 3. Monitorización del tratamiento
 – Solicitar en situaciones de disnea de diagnóstico dudoso. 2. Evaluación de la gravedad (pronóstico) 3. Monitorización del tratamiento.")
68
OBJETIVOS DEL TRATAMIENTO
Sobrevida Morbilidad Capacidad ejercicio Calidad de vida Cambios neurohormonales Progresión de ICC Síntomas Treatment of Heart Failure. Objectives The objectives of treatment of the patient with heart failure are many, but they may be summarized in two principles: decrease symptoms and prolong life. In daily practice, the first priority is symptom control and the best plan is to adjust to the individual patient’s particular circumstances over the course of therapy. Nevertheless, the rest of the listed objectives should not be forgotten, as medical therapy now has the potential for decreasing morbidity (hospital admissions, embolism, etc.), increasing exercise capacity (all of the usually prescribed drugs), improve the quality of life, control neurohormonal changes (ACE-I, beta blockers), retard progression (ACEI) and prolong life.
, increasing exercise capacity (all of the usually prescribed drugs), improve the quality of life, control neurohormonal changes (ACE-I, beta blockers), retard progression (ACEI) and prolong life.")
69
Tratamiento no farmacológico
Restricción moderada de sodio Medición diaria del peso (uso de dosis más bajas y seguras de diuréticos) Inmunización con vacunas contra influenza y neumococo Actividad fisica (excepto en periodos de descompensación o en miocarditis)
 Inmunización con vacunas contra influenza y neumococo. Actividad fisica (excepto en periodos de descompensación o en miocarditis)")
70
Corrección de factores agravantes
TRATAMIENTO Corrección de factores agravantes Embarazo Arritmias (FA) Infecciones Hipertiroidismo Tromboembolismo Endocarditis Obesidad Hipertensión Actividad física Excesos en dieta Treatment of Heart Failure. Correction of aggravating factors Often a lack of response to conventional therapy for heart failure is due to the presence of uncorrected aggravating or precipitating factors. It is important to always consider the possibility of such factors, particularly in cases of refractory failure. AF: atrial fibrillation. MEDICACIONES
 Infecciones. Hipertiroidismo. Tromboembolismo. Endocarditis. Obesidad. Hipertensión. Actividad física. Excesos en dieta. Treatment of Heart Failure. Correction of aggravating factors. Often a lack of response to conventional therapy for heart failure is due to the presence of uncorrected aggravating or precipitating factors. It is important to always consider the possibility of such factors, particularly in cases of refractory failure. AF: atrial fibrillation. MEDICACIONES.")
71
TERAPIA FARMACOLOGICA
TRATAMIENTO TERAPIA FARMACOLOGICA DIURETICOS INOTROPICOS VASODILATORES ANTAGONISTAS NEUROHORMONALES OTROS (Ejemplos: Anticoagulantes, antiarrítmicos) Treatment of Heart Failure. Drugs This is a simple and pragmatic classification of the vast numbers and types of medications in the pharmacopoeia for the treatment of heart failure.
 Treatment of Heart Failure. Drugs. This is a simple and pragmatic classification of the vast numbers and types of medications in the pharmacopoeia for the treatment of heart failure.")
Presentaciones similares