Descargar la presentación
La descarga está en progreso. Por favor, espere

1
ANATOMÍA Y FISIOLOGÍA DE TUBO DIGESTIVO
Dra. Ma. Eugenia Icaza

2
INTRODUCCIÓN SISTEMA DIGESTIVO Tracto gastrointestinal Hígado Páncreas
The GI tract, pancreas, and liver are responsible for digestion; absorption of fluids, electrolytes, and nutrients; removal of waste products; and metabolism of medications and other exogenous materials. The epithelial lining of the GI tract is larger than a tennis court. These epithelial cells have a rapid turnover, with a lifespan of 3 to 7 days, and have considerable interaction with endogenous and exogenous materials. The enteric nervous system ( Chapter 138 ), which is composed of a complex array of neurons and ganglia organized around the myenteric (Auerbach) and submucosal (Meissner) plexus located within the wall of the esophagus, stomach, and intestinal tract, contains between 10 and 100 million neurons—equal to the total number in the spinal cord. Although it is an independent nervous system, complex interactions with the autonomic and central nervous systems are necessary for normal function. Recent evidence suggests abnormal interactions among the enteric, autonomic, and central nervous systems in the development and continuation of symptoms in functional bowel disorders such as irritable bowel syndrome ( Chapter 139 ). The immunologic system of the GI tract is the largest immune organ in the body ( Chapter 42 ). It consists of luminal and epithelial barrier defenses, cellular components such as T and B cells, and noncellular inflammatory mediators. It has the overwhelmingly complex task of coexisting with luminal antigens (food), host proteins, and commensal bacteria while simultaneously differentiating these “good” antigens from “bad” antigens such as pathogenic bacterial proteins and transformed epithelial cells. The GI immune system plays a role in systemic autoimmune disorders and immune tolerance. The GI endocrine system is stimulated by the ingestion of food. Secretion of hormones from endocrine cells responds to nutrients and to stimulation from the central nervous system. The motility of the GI tract depends on a complex interaction between smooth muscle and the enteric nervous system. The interstitial cells of Cajal act as pacemakers of the GI tract and are responsible for the smooth, orderly transport of material from the mouth to the anus ( Chapter 138 ). With aging, the GI tract undergoes numerous changes. Epithelial cells interact with the environment and, given the appropriate genetic background, may undergo neoplastic transformation. Colon cancer ( Chapter 203 ) is the second most common malignancy in the United States, and the GI tract collectively has more cancers than any other organ in the body.
, which is composed of a complex array of neurons and ganglia organized around the myenteric (Auerbach) and submucosal (Meissner) plexus located within the wall of the esophagus, stomach, and intestinal tract, contains between 10 and 100 million neurons—equal to the total number in the spinal cord. Although it is an independent nervous system, complex interactions with the autonomic and central nervous systems are necessary for normal function. Recent evidence suggests abnormal interactions among the enteric, autonomic, and central nervous systems in the development and continuation of symptoms in functional bowel disorders such as irritable bowel syndrome ( Chapter 139 ). The immunologic system of the GI tract is the largest immune organ in the body ( Chapter 42 ). It consists of luminal and epithelial barrier defenses, cellular components such as T and B cells, and noncellular inflammatory mediators. It has the overwhelmingly complex task of coexisting with luminal antigens (food), host proteins, and commensal bacteria while simultaneously differentiating these good antigens from bad antigens such as pathogenic bacterial proteins and transformed epithelial cells. The GI immune system plays a role in systemic autoimmune disorders and immune tolerance. The GI endocrine system is stimulated by the ingestion of food. Secretion of hormones from endocrine cells responds to nutrients and to stimulation from the central nervous system. The motility of the GI tract depends on a complex interaction between smooth muscle and the enteric nervous system. The interstitial cells of Cajal act as pacemakers of the GI tract and are responsible for the smooth, orderly transport of material from the mouth to the anus ( Chapter 138 ). With aging, the GI tract undergoes numerous changes. Epithelial cells interact with the environment and, given the appropriate genetic background, may undergo neoplastic transformation. Colon cancer ( Chapter 203 ) is the second most common malignancy in the United States, and the GI tract collectively has more cancers than any other organ in the body.")
3
INTRODUCCIÓN SISTEMA DIGESTIVO: Funciones Digestión
Absorción de líquidos, electrolitos y nutrientes Eliminación de productos de desecho Metabolismo de materiales exógenos y de medicamentos The GI tract, pancreas, and liver are responsible for digestion; absorption of fluids, electrolytes, and nutrients; removal of waste products; and metabolism of medications and other exogenous materials. The epithelial lining of the GI tract is larger than a tennis court. These epithelial cells have a rapid turnover, with a lifespan of 3 to 7 days, and have considerable interaction with endogenous and exogenous materials. The enteric nervous system ( Chapter 138 ), which is composed of a complex array of neurons and ganglia organized around the myenteric (Auerbach) and submucosal (Meissner) plexus located within the wall of the esophagus, stomach, and intestinal tract, contains between 10 and 100 million neurons—equal to the total number in the spinal cord. Although it is an independent nervous system, complex interactions with the autonomic and central nervous systems are necessary for normal function. Recent evidence suggests abnormal interactions among the enteric, autonomic, and central nervous systems in the development and continuation of symptoms in functional bowel disorders such as irritable bowel syndrome ( Chapter 139 ). The immunologic system of the GI tract is the largest immune organ in the body ( Chapter 42 ). It consists of luminal and epithelial barrier defenses, cellular components such as T and B cells, and noncellular inflammatory mediators. It has the overwhelmingly complex task of coexisting with luminal antigens (food), host proteins, and commensal bacteria while simultaneously differentiating these “good” antigens from “bad” antigens such as pathogenic bacterial proteins and transformed epithelial cells. The GI immune system plays a role in systemic autoimmune disorders and immune tolerance. The GI endocrine system is stimulated by the ingestion of food. Secretion of hormones from endocrine cells responds to nutrients and to stimulation from the central nervous system. The motility of the GI tract depends on a complex interaction between smooth muscle and the enteric nervous system. The interstitial cells of Cajal act as pacemakers of the GI tract and are responsible for the smooth, orderly transport of material from the mouth to the anus ( Chapter 138 ). With aging, the GI tract undergoes numerous changes. Epithelial cells interact with the environment and, given the appropriate genetic background, may undergo neoplastic transformation. Colon cancer ( Chapter 203 ) is the second most common malignancy in the United States, and the GI tract collectively has more cancers than any other organ in the body.
, which is composed of a complex array of neurons and ganglia organized around the myenteric (Auerbach) and submucosal (Meissner) plexus located within the wall of the esophagus, stomach, and intestinal tract, contains between 10 and 100 million neurons—equal to the total number in the spinal cord. Although it is an independent nervous system, complex interactions with the autonomic and central nervous systems are necessary for normal function. Recent evidence suggests abnormal interactions among the enteric, autonomic, and central nervous systems in the development and continuation of symptoms in functional bowel disorders such as irritable bowel syndrome ( Chapter 139 ). The immunologic system of the GI tract is the largest immune organ in the body ( Chapter 42 ). It consists of luminal and epithelial barrier defenses, cellular components such as T and B cells, and noncellular inflammatory mediators. It has the overwhelmingly complex task of coexisting with luminal antigens (food), host proteins, and commensal bacteria while simultaneously differentiating these good antigens from bad antigens such as pathogenic bacterial proteins and transformed epithelial cells. The GI immune system plays a role in systemic autoimmune disorders and immune tolerance. The GI endocrine system is stimulated by the ingestion of food. Secretion of hormones from endocrine cells responds to nutrients and to stimulation from the central nervous system. The motility of the GI tract depends on a complex interaction between smooth muscle and the enteric nervous system. The interstitial cells of Cajal act as pacemakers of the GI tract and are responsible for the smooth, orderly transport of material from the mouth to the anus ( Chapter 138 ). With aging, the GI tract undergoes numerous changes. Epithelial cells interact with the environment and, given the appropriate genetic background, may undergo neoplastic transformation. Colon cancer ( Chapter 203 ) is the second most common malignancy in the United States, and the GI tract collectively has more cancers than any other organ in the body.")
4
INTRODUCCIÓN Tracto gastrointestinal Boca Faringe Esófago Estómago
Intestino delgado Intestino grueso (colon) The GI tract, pancreas, and liver are responsible for digestion; absorption of fluids, electrolytes, and nutrients; removal of waste products; and metabolism of medications and other exogenous materials. The epithelial lining of the GI tract is larger than a tennis court. These epithelial cells have a rapid turnover, with a lifespan of 3 to 7 days, and have considerable interaction with endogenous and exogenous materials. The enteric nervous system ( Chapter 138 ), which is composed of a complex array of neurons and ganglia organized around the myenteric (Auerbach) and submucosal (Meissner) plexus located within the wall of the esophagus, stomach, and intestinal tract, contains between 10 and 100 million neurons—equal to the total number in the spinal cord. Although it is an independent nervous system, complex interactions with the autonomic and central nervous systems are necessary for normal function. Recent evidence suggests abnormal interactions among the enteric, autonomic, and central nervous systems in the development and continuation of symptoms in functional bowel disorders such as irritable bowel syndrome ( Chapter 139 ). The immunologic system of the GI tract is the largest immune organ in the body ( Chapter 42 ). It consists of luminal and epithelial barrier defenses, cellular components such as T and B cells, and noncellular inflammatory mediators. It has the overwhelmingly complex task of coexisting with luminal antigens (food), host proteins, and commensal bacteria while simultaneously differentiating these “good” antigens from “bad” antigens such as pathogenic bacterial proteins and transformed epithelial cells. The GI immune system plays a role in systemic autoimmune disorders and immune tolerance. The GI endocrine system is stimulated by the ingestion of food. Secretion of hormones from endocrine cells responds to nutrients and to stimulation from the central nervous system. The motility of the GI tract depends on a complex interaction between smooth muscle and the enteric nervous system. The interstitial cells of Cajal act as pacemakers of the GI tract and are responsible for the smooth, orderly transport of material from the mouth to the anus ( Chapter 138 ). With aging, the GI tract undergoes numerous changes. Epithelial cells interact with the environment and, given the appropriate genetic background, may undergo neoplastic transformation. Colon cancer ( Chapter 203 ) is the second most common malignancy in the United States, and the GI tract collectively has more cancers than any other organ in the body.
 The GI tract, pancreas, and liver are responsible for digestion; absorption of fluids, electrolytes, and nutrients; removal of waste products; and metabolism of medications and other exogenous materials. The epithelial lining of the GI tract is larger than a tennis court. These epithelial cells have a rapid turnover, with a lifespan of 3 to 7 days, and have considerable interaction with endogenous and exogenous materials. The enteric nervous system ( Chapter 138 ), which is composed of a complex array of neurons and ganglia organized around the myenteric (Auerbach) and submucosal (Meissner) plexus located within the wall of the esophagus, stomach, and intestinal tract, contains between 10 and 100 million neurons—equal to the total number in the spinal cord. Although it is an independent nervous system, complex interactions with the autonomic and central nervous systems are necessary for normal function. Recent evidence suggests abnormal interactions among the enteric, autonomic, and central nervous systems in the development and continuation of symptoms in functional bowel disorders such as irritable bowel syndrome ( Chapter 139 ). The immunologic system of the GI tract is the largest immune organ in the body ( Chapter 42 ). It consists of luminal and epithelial barrier defenses, cellular components such as T and B cells, and noncellular inflammatory mediators. It has the overwhelmingly complex task of coexisting with luminal antigens (food), host proteins, and commensal bacteria while simultaneously differentiating these good antigens from bad antigens such as pathogenic bacterial proteins and transformed epithelial cells. The GI immune system plays a role in systemic autoimmune disorders and immune tolerance. The GI endocrine system is stimulated by the ingestion of food. Secretion of hormones from endocrine cells responds to nutrients and to stimulation from the central nervous system. The motility of the GI tract depends on a complex interaction between smooth muscle and the enteric nervous system. The interstitial cells of Cajal act as pacemakers of the GI tract and are responsible for the smooth, orderly transport of material from the mouth to the anus ( Chapter 138 ). With aging, the GI tract undergoes numerous changes. Epithelial cells interact with the environment and, given the appropriate genetic background, may undergo neoplastic transformation. Colon cancer ( Chapter 203 ) is the second most common malignancy in the United States, and the GI tract collectively has more cancers than any other organ in the body.")
5
INTRODUCCIÓN Tracto gastrointestinal
Superficie mayor a la de una cancha de tenis Alto recambio epitelial con vida media celular de 3 a 7 días Cuenta con sistema nervioso entérico compuesto de una serie de neuronas en la pared del esófago, estómago e intestino Sistema inmunológico mayor del cuerpo: defensas luminales y epiteliales Sistema endócrino propio The GI tract, pancreas, and liver are responsible for digestion; absorption of fluids, electrolytes, and nutrients; removal of waste products; and metabolism of medications and other exogenous materials. The epithelial lining of the GI tract is larger than a tennis court. These epithelial cells have a rapid turnover, with a lifespan of 3 to 7 days, and have considerable interaction with endogenous and exogenous materials. The enteric nervous system ( Chapter 138 ), which is composed of a complex array of neurons and ganglia organized around the myenteric (Auerbach) and submucosal (Meissner) plexus located within the wall of the esophagus, stomach, and intestinal tract, contains between 10 and 100 million neurons—equal to the total number in the spinal cord. Although it is an independent nervous system, complex interactions with the autonomic and central nervous systems are necessary for normal function. Recent evidence suggests abnormal interactions among the enteric, autonomic, and central nervous systems in the development and continuation of symptoms in functional bowel disorders such as irritable bowel syndrome ( Chapter 139 ). The immunologic system of the GI tract is the largest immune organ in the body ( Chapter 42 ). It consists of luminal and epithelial barrier defenses, cellular components such as T and B cells, and noncellular inflammatory mediators. It has the overwhelmingly complex task of coexisting with luminal antigens (food), host proteins, and commensal bacteria while simultaneously differentiating these “good” antigens from “bad” antigens such as pathogenic bacterial proteins and transformed epithelial cells. The GI immune system plays a role in systemic autoimmune disorders and immune tolerance. The GI endocrine system is stimulated by the ingestion of food. Secretion of hormones from endocrine cells responds to nutrients and to stimulation from the central nervous system. The motility of the GI tract depends on a complex interaction between smooth muscle and the enteric nervous system. The interstitial cells of Cajal act as pacemakers of the GI tract and are responsible for the smooth, orderly transport of material from the mouth to the anus ( Chapter 138 ). With aging, the GI tract undergoes numerous changes. Epithelial cells interact with the environment and, given the appropriate genetic background, may undergo neoplastic transformation. Colon cancer ( Chapter 203 ) is the second most common malignancy in the United States, and the GI tract collectively has more cancers than any other organ in the body.
, which is composed of a complex array of neurons and ganglia organized around the myenteric (Auerbach) and submucosal (Meissner) plexus located within the wall of the esophagus, stomach, and intestinal tract, contains between 10 and 100 million neurons—equal to the total number in the spinal cord. Although it is an independent nervous system, complex interactions with the autonomic and central nervous systems are necessary for normal function. Recent evidence suggests abnormal interactions among the enteric, autonomic, and central nervous systems in the development and continuation of symptoms in functional bowel disorders such as irritable bowel syndrome ( Chapter 139 ). The immunologic system of the GI tract is the largest immune organ in the body ( Chapter 42 ). It consists of luminal and epithelial barrier defenses, cellular components such as T and B cells, and noncellular inflammatory mediators. It has the overwhelmingly complex task of coexisting with luminal antigens (food), host proteins, and commensal bacteria while simultaneously differentiating these good antigens from bad antigens such as pathogenic bacterial proteins and transformed epithelial cells. The GI immune system plays a role in systemic autoimmune disorders and immune tolerance. The GI endocrine system is stimulated by the ingestion of food. Secretion of hormones from endocrine cells responds to nutrients and to stimulation from the central nervous system. The motility of the GI tract depends on a complex interaction between smooth muscle and the enteric nervous system. The interstitial cells of Cajal act as pacemakers of the GI tract and are responsible for the smooth, orderly transport of material from the mouth to the anus ( Chapter 138 ). With aging, the GI tract undergoes numerous changes. Epithelial cells interact with the environment and, given the appropriate genetic background, may undergo neoplastic transformation. Colon cancer ( Chapter 203 ) is the second most common malignancy in the United States, and the GI tract collectively has more cancers than any other organ in the body.")
6
INTRODUCCIÓN Páncreas Secreción endócrina: insulina, glucagon
Secreción exócrina: enzimas digestivas Digestión intraluminal del alimento The GI tract, pancreas, and liver are responsible for digestion; absorption of fluids, electrolytes, and nutrients; removal of waste products; and metabolism of medications and other exogenous materials. The epithelial lining of the GI tract is larger than a tennis court. These epithelial cells have a rapid turnover, with a lifespan of 3 to 7 days, and have considerable interaction with endogenous and exogenous materials. The enteric nervous system ( Chapter 138 ), which is composed of a complex array of neurons and ganglia organized around the myenteric (Auerbach) and submucosal (Meissner) plexus located within the wall of the esophagus, stomach, and intestinal tract, contains between 10 and 100 million neurons—equal to the total number in the spinal cord. Although it is an independent nervous system, complex interactions with the autonomic and central nervous systems are necessary for normal function. Recent evidence suggests abnormal interactions among the enteric, autonomic, and central nervous systems in the development and continuation of symptoms in functional bowel disorders such as irritable bowel syndrome ( Chapter 139 ). The immunologic system of the GI tract is the largest immune organ in the body ( Chapter 42 ). It consists of luminal and epithelial barrier defenses, cellular components such as T and B cells, and noncellular inflammatory mediators. It has the overwhelmingly complex task of coexisting with luminal antigens (food), host proteins, and commensal bacteria while simultaneously differentiating these “good” antigens from “bad” antigens such as pathogenic bacterial proteins and transformed epithelial cells. The GI immune system plays a role in systemic autoimmune disorders and immune tolerance. The GI endocrine system is stimulated by the ingestion of food. Secretion of hormones from endocrine cells responds to nutrients and to stimulation from the central nervous system. The motility of the GI tract depends on a complex interaction between smooth muscle and the enteric nervous system. The interstitial cells of Cajal act as pacemakers of the GI tract and are responsible for the smooth, orderly transport of material from the mouth to the anus ( Chapter 138 ). With aging, the GI tract undergoes numerous changes. Epithelial cells interact with the environment and, given the appropriate genetic background, may undergo neoplastic transformation. Colon cancer ( Chapter 203 ) is the second most common malignancy in the United States, and the GI tract collectively has more cancers than any other organ in the body.
, which is composed of a complex array of neurons and ganglia organized around the myenteric (Auerbach) and submucosal (Meissner) plexus located within the wall of the esophagus, stomach, and intestinal tract, contains between 10 and 100 million neurons—equal to the total number in the spinal cord. Although it is an independent nervous system, complex interactions with the autonomic and central nervous systems are necessary for normal function. Recent evidence suggests abnormal interactions among the enteric, autonomic, and central nervous systems in the development and continuation of symptoms in functional bowel disorders such as irritable bowel syndrome ( Chapter 139 ). The immunologic system of the GI tract is the largest immune organ in the body ( Chapter 42 ). It consists of luminal and epithelial barrier defenses, cellular components such as T and B cells, and noncellular inflammatory mediators. It has the overwhelmingly complex task of coexisting with luminal antigens (food), host proteins, and commensal bacteria while simultaneously differentiating these good antigens from bad antigens such as pathogenic bacterial proteins and transformed epithelial cells. The GI immune system plays a role in systemic autoimmune disorders and immune tolerance. The GI endocrine system is stimulated by the ingestion of food. Secretion of hormones from endocrine cells responds to nutrients and to stimulation from the central nervous system. The motility of the GI tract depends on a complex interaction between smooth muscle and the enteric nervous system. The interstitial cells of Cajal act as pacemakers of the GI tract and are responsible for the smooth, orderly transport of material from the mouth to the anus ( Chapter 138 ). With aging, the GI tract undergoes numerous changes. Epithelial cells interact with the environment and, given the appropriate genetic background, may undergo neoplastic transformation. Colon cancer ( Chapter 203 ) is the second most common malignancy in the United States, and the GI tract collectively has more cancers than any other organ in the body.")
7
INTRODUCCIÓN Hígado Metabolismo de sustancias de desecho
Metabolismo de medicamentos Síntesis de proteínas Síntesis de bilis (digestión) Defensa contra antígenos The GI tract, pancreas, and liver are responsible for digestion; absorption of fluids, electrolytes, and nutrients; removal of waste products; and metabolism of medications and other exogenous materials. The epithelial lining of the GI tract is larger than a tennis court. These epithelial cells have a rapid turnover, with a lifespan of 3 to 7 days, and have considerable interaction with endogenous and exogenous materials. The enteric nervous system ( Chapter 138 ), which is composed of a complex array of neurons and ganglia organized around the myenteric (Auerbach) and submucosal (Meissner) plexus located within the wall of the esophagus, stomach, and intestinal tract, contains between 10 and 100 million neurons—equal to the total number in the spinal cord. Although it is an independent nervous system, complex interactions with the autonomic and central nervous systems are necessary for normal function. Recent evidence suggests abnormal interactions among the enteric, autonomic, and central nervous systems in the development and continuation of symptoms in functional bowel disorders such as irritable bowel syndrome ( Chapter 139 ). The immunologic system of the GI tract is the largest immune organ in the body ( Chapter 42 ). It consists of luminal and epithelial barrier defenses, cellular components such as T and B cells, and noncellular inflammatory mediators. It has the overwhelmingly complex task of coexisting with luminal antigens (food), host proteins, and commensal bacteria while simultaneously differentiating these “good” antigens from “bad” antigens such as pathogenic bacterial proteins and transformed epithelial cells. The GI immune system plays a role in systemic autoimmune disorders and immune tolerance. The GI endocrine system is stimulated by the ingestion of food. Secretion of hormones from endocrine cells responds to nutrients and to stimulation from the central nervous system. The motility of the GI tract depends on a complex interaction between smooth muscle and the enteric nervous system. The interstitial cells of Cajal act as pacemakers of the GI tract and are responsible for the smooth, orderly transport of material from the mouth to the anus ( Chapter 138 ). With aging, the GI tract undergoes numerous changes. Epithelial cells interact with the environment and, given the appropriate genetic background, may undergo neoplastic transformation. Colon cancer ( Chapter 203 ) is the second most common malignancy in the United States, and the GI tract collectively has more cancers than any other organ in the body.
 Defensa contra antígenos. The GI tract, pancreas, and liver are responsible for digestion; absorption of fluids, electrolytes, and nutrients; removal of waste products; and metabolism of medications and other exogenous materials. The epithelial lining of the GI tract is larger than a tennis court. These epithelial cells have a rapid turnover, with a lifespan of 3 to 7 days, and have considerable interaction with endogenous and exogenous materials. The enteric nervous system ( Chapter 138 ), which is composed of a complex array of neurons and ganglia organized around the myenteric (Auerbach) and submucosal (Meissner) plexus located within the wall of the esophagus, stomach, and intestinal tract, contains between 10 and 100 million neurons—equal to the total number in the spinal cord. Although it is an independent nervous system, complex interactions with the autonomic and central nervous systems are necessary for normal function. Recent evidence suggests abnormal interactions among the enteric, autonomic, and central nervous systems in the development and continuation of symptoms in functional bowel disorders such as irritable bowel syndrome ( Chapter 139 ). The immunologic system of the GI tract is the largest immune organ in the body ( Chapter 42 ). It consists of luminal and epithelial barrier defenses, cellular components such as T and B cells, and noncellular inflammatory mediators. It has the overwhelmingly complex task of coexisting with luminal antigens (food), host proteins, and commensal bacteria while simultaneously differentiating these good antigens from bad antigens such as pathogenic bacterial proteins and transformed epithelial cells. The GI immune system plays a role in systemic autoimmune disorders and immune tolerance. The GI endocrine system is stimulated by the ingestion of food. Secretion of hormones from endocrine cells responds to nutrients and to stimulation from the central nervous system. The motility of the GI tract depends on a complex interaction between smooth muscle and the enteric nervous system. The interstitial cells of Cajal act as pacemakers of the GI tract and are responsible for the smooth, orderly transport of material from the mouth to the anus ( Chapter 138 ). With aging, the GI tract undergoes numerous changes. Epithelial cells interact with the environment and, given the appropriate genetic background, may undergo neoplastic transformation. Colon cancer ( Chapter 203 ) is the second most common malignancy in the United States, and the GI tract collectively has more cancers than any other organ in the body.")
8
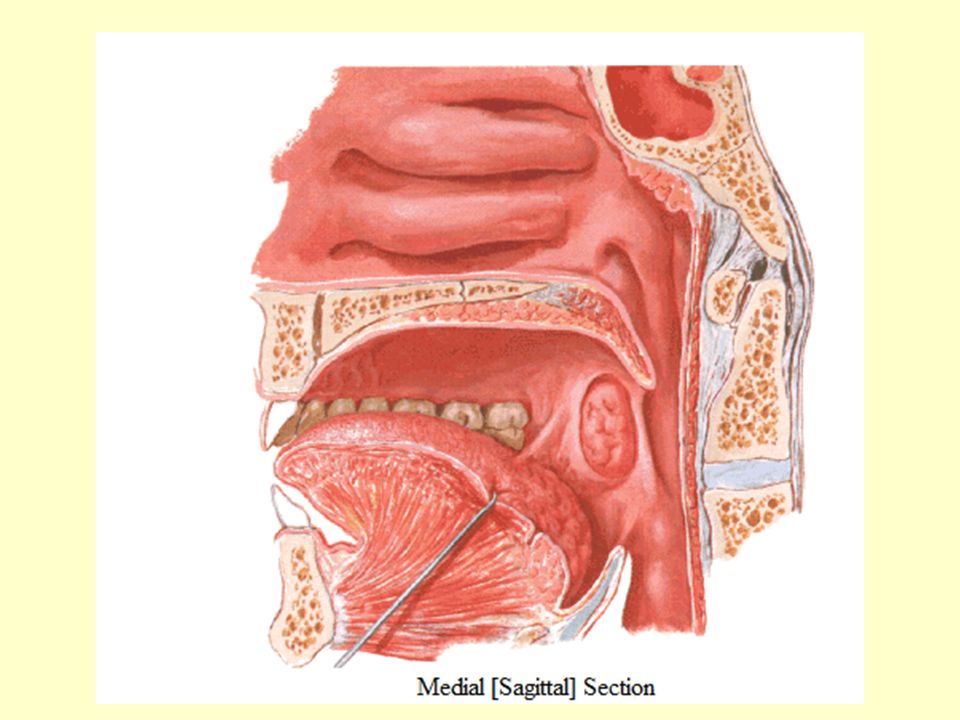
Boca

9
Dientes 20 dientes “de leche” 32 dientes permanentes

10
Dientes definitivos

11
Lengua

12
Lengua

13
Glándulas salivales La saliva es un líquido de la cavidad bucal, producido por las glándulas salivales, transparente, de viscosidad variable, compuesto principalmente por agua, sales minerales y algunas proteínas. Se estima que la boca está humedecida por la producción de entre 1 y 1.5 litros de saliva al día, durante la vida de una persona se generan unos Esta cantidad de saliva es variable ya que va disminuyendo conforme avanzan los años y debido a diferentes tratamientos. La producción de saliva está relacionada con el ciclo circadiano, de tal manera que por la noche se segrega una mínima cantidad de saliva; además, su composición varía en función de los estímulos (como el olor o la visión de la comida) aumentando -por ejemplo- el pH ante estos estímulos (cuando en condiciones normales es de 6.5 a 7.5). Es segregada por las glándulas salivares mayores (parótida, sublingual y submaxilar) y menores. La disminución de saliva se llama hiposalivación, mientras que la sensación de sequedad bucal se denomina xerostomía, la producción excesiva sialorrea. Composición de la saliva [editar] La composición es similar a la del plasma. Está compuesta por: Agua: Representa un 95% de su volumen, en la que se disuelven el 5% restante formado por sales minerales como iones de sodio, potasio, cloruro, bicarbonato y fosfatos. El agua permite que los alimentos se disuelvan y se perciba su sabor en el sentido del gusto. Iones cloruro: Activan la amilasa salival o ptialina. Bicarbonato y fosfato: Neutralizan el pH de los alimentos ácidos y de la corrosión bacteriana. Moco: Lubrica el bolo alimenticio para facilitar la deglución y que pueda avanzar a lo largo del tubo digestivo, sin dañarlo. Lisozima: Es una sustancia antimicrobiana que destruye las bacterias contenidas en los alimentos, protegiendo en parte los dientes de las caries y de las infecciones. Enzimas: Como la ptialina, que es una amilasa que hidroliza el almidón parcialmente en la boca, comenzando la digestión de los hidratos de carbono. Estaterina: Con un extremo aminoterminal muy ácido, que inhibe la precipitación de fosfato cálcico al unirse a los cristales de hidroxiapatita. Además, también tiene función antibacteriana y antifúngica. Otras sustancias: Como inmunoglobulinas específicas, transferrina, lactoferrina. También Calcio: Que le da el "sabor" a la saliva y ayuda a digerir el alimento
 aumentando -por ejemplo- el pH ante estos estímulos (cuando en condiciones normales es de 6.5 a 7.5). Es segregada por las glándulas salivares mayores (parótida, sublingual y submaxilar) y menores. La disminución de saliva se llama hiposalivación, mientras que la sensación de sequedad bucal se denomina xerostomía, la producción excesiva sialorrea. Composición de la saliva [editar] La composición es similar a la del plasma. Está compuesta por: Agua: Representa un 95% de su volumen, en la que se disuelven el 5% restante formado por sales minerales como iones de sodio, potasio, cloruro, bicarbonato y fosfatos. El agua permite que los alimentos se disuelvan y se perciba su sabor en el sentido del gusto. Iones cloruro: Activan la amilasa salival o ptialina. Bicarbonato y fosfato: Neutralizan el pH de los alimentos ácidos y de la corrosión bacteriana. Moco: Lubrica el bolo alimenticio para facilitar la deglución y que pueda avanzar a lo largo del tubo digestivo, sin dañarlo. Lisozima: Es una sustancia antimicrobiana que destruye las bacterias contenidas en los alimentos, protegiendo en parte los dientes de las caries y de las infecciones. Enzimas: Como la ptialina, que es una amilasa que hidroliza el almidón parcialmente en la boca, comenzando la digestión de los hidratos de carbono. Estaterina: Con un extremo aminoterminal muy ácido, que inhibe la precipitación de fosfato cálcico al unirse a los cristales de hidroxiapatita. Además, también tiene función antibacteriana y antifúngica. Otras sustancias: Como inmunoglobulinas específicas, transferrina, lactoferrina. También Calcio: Que le da el sabor a la saliva y ayuda a digerir el alimento.")
14
Glándulas salivales Producen 1 a 1.5 L de saliva al día
Líquido transparente compuesto por agua, sales minerales y algunas proteínas Por la noche se segrega una mínima cantidad de saliva Su composición depende de los estímulos como el olor y la visión de la saliva La saliva es un líquido de la cavidad bucal, producido por las glándulas salivales, transparente, de viscosidad variable, compuesto principalmente por agua, sales minerales y algunas proteínas. Se estima que la boca está humedecida por la producción de entre 1 y 1.5 litros de saliva al día, durante la vida de una persona se generan unos Esta cantidad de saliva es variable ya que va disminuyendo conforme avanzan los años y debido a diferentes tratamientos. La producción de saliva está relacionada con el ciclo circadiano, de tal manera que por la noche se segrega una mínima cantidad de saliva; además, su composición varía en función de los estímulos (como el olor o la visión de la comida) aumentando -por ejemplo- el pH ante estos estímulos (cuando en condiciones normales es de 6.5 a 7.5). Es segregada por las glándulas salivares mayores (parótida, sublingual y submaxilar) y menores. La disminución de saliva se llama hiposalivación, mientras que la sensación de sequedad bucal se denomina xerostomía, la producción excesiva sialorrea. Composición de la saliva [editar] La composición es similar a la del plasma. Está compuesta por: Agua: Representa un 95% de su volumen, en la que se disuelven el 5% restante formado por sales minerales como iones de sodio, potasio, cloruro, bicarbonato y fosfatos. El agua permite que los alimentos se disuelvan y se perciba su sabor en el sentido del gusto. Iones cloruro: Activan la amilasa salival o ptialina. Bicarbonato y fosfato: Neutralizan el pH de los alimentos ácidos y de la corrosión bacteriana. Moco: Lubrica el bolo alimenticio para facilitar la deglución y que pueda avanzar a lo largo del tubo digestivo, sin dañarlo. Lisozima: Es una sustancia antimicrobiana que destruye las bacterias contenidas en los alimentos, protegiendo en parte los dientes de las caries y de las infecciones. Enzimas: Como la ptialina, que es una amilasa que hidroliza el almidón parcialmente en la boca, comenzando la digestión de los hidratos de carbono. Estaterina: Con un extremo aminoterminal muy ácido, que inhibe la precipitación de fosfato cálcico al unirse a los cristales de hidroxiapatita. Además, también tiene función antibacteriana y antifúngica. Otras sustancias: Como inmunoglobulinas específicas, transferrina, lactoferrina. También Calcio: Que le da el "sabor" a la saliva y ayuda a digerir el alimento
 aumentando -por ejemplo- el pH ante estos estímulos (cuando en condiciones normales es de 6.5 a 7.5). Es segregada por las glándulas salivares mayores (parótida, sublingual y submaxilar) y menores. La disminución de saliva se llama hiposalivación, mientras que la sensación de sequedad bucal se denomina xerostomía, la producción excesiva sialorrea. Composición de la saliva [editar] La composición es similar a la del plasma. Está compuesta por: Agua: Representa un 95% de su volumen, en la que se disuelven el 5% restante formado por sales minerales como iones de sodio, potasio, cloruro, bicarbonato y fosfatos. El agua permite que los alimentos se disuelvan y se perciba su sabor en el sentido del gusto. Iones cloruro: Activan la amilasa salival o ptialina. Bicarbonato y fosfato: Neutralizan el pH de los alimentos ácidos y de la corrosión bacteriana. Moco: Lubrica el bolo alimenticio para facilitar la deglución y que pueda avanzar a lo largo del tubo digestivo, sin dañarlo. Lisozima: Es una sustancia antimicrobiana que destruye las bacterias contenidas en los alimentos, protegiendo en parte los dientes de las caries y de las infecciones. Enzimas: Como la ptialina, que es una amilasa que hidroliza el almidón parcialmente en la boca, comenzando la digestión de los hidratos de carbono. Estaterina: Con un extremo aminoterminal muy ácido, que inhibe la precipitación de fosfato cálcico al unirse a los cristales de hidroxiapatita. Además, también tiene función antibacteriana y antifúngica. Otras sustancias: Como inmunoglobulinas específicas, transferrina, lactoferrina. También Calcio: Que le da el sabor a la saliva y ayuda a digerir el alimento.")
15
Glándulas salivales Composición de la saliva Agua 95% Iones cloruro
Bicarbonato Moco Lisozima Ptialina (amilasa) Esteaterina Inmunoglobulinas Calcio Composición de la saliva [editar] La composición es similar a la del plasma. Está compuesta por: Agua: Representa un 95% de su volumen, en la que se disuelven el 5% restante formado por sales minerales como iones de sodio, potasio, cloruro, bicarbonato y fosfatos. El agua permite que los alimentos se disuelvan y se perciba su sabor en el sentido del gusto. Iones cloruro: Activan la amilasa salival o ptialina. Bicarbonato y fosfato: Neutralizan el pH de los alimentos ácidos y de la corrosión bacteriana. Moco: Lubrica el bolo alimenticio para facilitar la deglución y que pueda avanzar a lo largo del tubo digestivo, sin dañarlo. Lisozima: Es una sustancia antimicrobiana que destruye las bacterias contenidas en los alimentos, protegiendo en parte los dientes de las caries y de las infecciones. Enzimas: Como la ptialina, que es una amilasa que hidroliza el almidón parcialmente en la boca, comenzando la digestión de los hidratos de carbono. Estaterina: Con un extremo aminoterminal muy ácido, que inhibe la precipitación de fosfato cálcico al unirse a los cristales de hidroxiapatita. Además, también tiene función antibacteriana y antifúngica. Otras sustancias: Como inmunoglobulinas específicas, transferrina, lactoferrina. También Calcio: Que le da el "sabor" a la saliva y ayuda a digerir el alimento
 Esteaterina. Inmunoglobulinas. Calcio. Composición de la saliva [editar] La composición es similar a la del plasma. Está compuesta por: Agua: Representa un 95% de su volumen, en la que se disuelven el 5% restante formado por sales minerales como iones de sodio, potasio, cloruro, bicarbonato y fosfatos. El agua permite que los alimentos se disuelvan y se perciba su sabor en el sentido del gusto. Iones cloruro: Activan la amilasa salival o ptialina. Bicarbonato y fosfato: Neutralizan el pH de los alimentos ácidos y de la corrosión bacteriana. Moco: Lubrica el bolo alimenticio para facilitar la deglución y que pueda avanzar a lo largo del tubo digestivo, sin dañarlo. Lisozima: Es una sustancia antimicrobiana que destruye las bacterias contenidas en los alimentos, protegiendo en parte los dientes de las caries y de las infecciones. Enzimas: Como la ptialina, que es una amilasa que hidroliza el almidón parcialmente en la boca, comenzando la digestión de los hidratos de carbono. Estaterina: Con un extremo aminoterminal muy ácido, que inhibe la precipitación de fosfato cálcico al unirse a los cristales de hidroxiapatita. Además, también tiene función antibacteriana y antifúngica. Otras sustancias: Como inmunoglobulinas específicas, transferrina, lactoferrina. También Calcio: Que le da el sabor a la saliva y ayuda a digerir el alimento.")
16
Glándulas salivales Orificio de salida de glándula parótida: segundo molar superior

17
Funciones de la saliva Amilasa, mucina y peroxidasa
Anhidrasa carbónica Amortiguador Antibacterial Amilasa, mucina y lipasa Cistatina y mucina Digestión Antiviral Funciones Mineral- ización Antifúngica Cistatinas, histatinas, proteínas ricas en prolina Histatinas Cubierta Lubricación Amilasa, cistatina, mucina, proteínas ricas en prolina Mucinas adapted from M.J. Levine, 1993

18
FARINGE Nasofaringe Orofaringe Hipofaringe

20
CAPAS DEL TUBO DIGESTIVO
Mucosa Submucosa Muscular Circular Longitudinal Serosa

21
ESÓFAGO: ANATOMÍA The muscularis propria is responsible for carrying out the organs' motor function. The upper 5% to 33% is composed exclusively of skeletal muscle, and the distal 33% is composed of smooth muscle. In between is a mixture of both types.[3] Proximally, the esophagus begins where the inferior pharyngeal constrictor merges with the cricopharyngeus, an area of skeletal muscle known functionally as the upper esophageal sphincter (UES) ( Fig. 40-3A ). The UES is contracted at rest and thereby creates a high pressure that prevents inspired air from entering the esophagus. Below the UES, the esophageal wall comprises inner circular and outer longitudinal layers of muscle (see Fig. 40-2A ). The esophageal body lies within the posterior mediastinum behind the trachea and left mainstem bronchus and swings leftward to pass behind the heart and in front of the aorta.[1] At the T10 vertebral level the esophageal body leaves the thorax through a hiatus located within the right crus of the diaphragm (see Fig ). Within the diaphragmatic hiatus the esophageal body ends in a 2- to 4-cm length of asymmetrically thickened circular smooth muscle known as the lower esophageal sphincter (LES) (see Fig. 40-3B ).[4] The phrenoesophageal ligament, which originates from the diaphragm's transversalis fascia and inserts on the lower esophagus, contributes to fixation of the LES within the diaphragmatic hiatus. This positioning is beneficial because it enables diaphragmatic contractions to assist the LES in maintenance of a high-pressure zone during exercise. The LES is contracted at rest, creating a high-pressure zone that prevents gastric contents from entering the esophagus. During swallowing, the LES relaxes to permit the swallowed bolus to be pushed by peristalsis from the esophagus into the stomach.
 ( Fig. 40-3A ). The UES is contracted at rest and thereby creates a high pressure that prevents inspired air from entering the esophagus. Below the UES, the esophageal wall comprises inner circular and outer longitudinal layers of muscle (see Fig. 40-2A ). The esophageal body lies within the posterior mediastinum behind the trachea and left mainstem bronchus and swings leftward to pass behind the heart and in front of the aorta.[1] At the T10 vertebral level the esophageal body leaves the thorax through a hiatus located within the right crus of the diaphragm (see Fig ). Within the diaphragmatic hiatus the esophageal body ends in a 2- to 4-cm length of asymmetrically thickened circular smooth muscle known as the lower esophageal sphincter (LES) (see Fig. 40-3B ).[4] The phrenoesophageal ligament, which originates from the diaphragm s transversalis fascia and inserts on the lower esophagus, contributes to fixation of the LES within the diaphragmatic hiatus. This positioning is beneficial because it enables diaphragmatic contractions to assist the LES in maintenance of a high-pressure zone during exercise. The LES is contracted at rest, creating a high-pressure zone that prevents gastric contents from entering the esophagus. During swallowing, the LES relaxes to permit the swallowed bolus to be pushed by peristalsis from the esophagus into the stomach.")
22
ESÓFAGO Esfínter esofágico superior: permanece cerrado
Músculo esquelético primer tercio Músculo liso dos tercios Hiato esofágico Esfínter esofágico inferior que se relaja al tragar The muscularis propria is responsible for carrying out the organs' motor function. The upper 5% to 33% is composed exclusively of skeletal muscle, and the distal 33% is composed of smooth muscle. In between is a mixture of both types.[3] Proximally, the esophagus begins where the inferior pharyngeal constrictor merges with the cricopharyngeus, an area of skeletal muscle known functionally as the upper esophageal sphincter (UES) ( Fig. 40-3A ). The UES is contracted at rest and thereby creates a high pressure that prevents inspired air from entering the esophagus. Below the UES, the esophageal wall comprises inner circular and outer longitudinal layers of muscle (see Fig. 40-2A ). The esophageal body lies within the posterior mediastinum behind the trachea and left mainstem bronchus and swings leftward to pass behind the heart and in front of the aorta.[1] At the T10 vertebral level the esophageal body leaves the thorax through a hiatus located within the right crus of the diaphragm (see Fig ). Within the diaphragmatic hiatus the esophageal body ends in a 2- to 4-cm length of asymmetrically thickened circular smooth muscle known as the lower esophageal sphincter (LES) (see Fig. 40-3B ).[4] The phrenoesophageal ligament, which originates from the diaphragm's transversalis fascia and inserts on the lower esophagus, contributes to fixation of the LES within the diaphragmatic hiatus. This positioning is beneficial because it enables diaphragmatic contractions to assist the LES in maintenance of a high-pressure zone during exercise. The LES is contracted at rest, creating a high-pressure zone that prevents gastric contents from entering the esophagus. During swallowing, the LES relaxes to permit the swallowed bolus to be pushed by peristalsis from the esophagus into the stomach.
 ( Fig. 40-3A ). The UES is contracted at rest and thereby creates a high pressure that prevents inspired air from entering the esophagus. Below the UES, the esophageal wall comprises inner circular and outer longitudinal layers of muscle (see Fig. 40-2A ). The esophageal body lies within the posterior mediastinum behind the trachea and left mainstem bronchus and swings leftward to pass behind the heart and in front of the aorta.[1] At the T10 vertebral level the esophageal body leaves the thorax through a hiatus located within the right crus of the diaphragm (see Fig ). Within the diaphragmatic hiatus the esophageal body ends in a 2- to 4-cm length of asymmetrically thickened circular smooth muscle known as the lower esophageal sphincter (LES) (see Fig. 40-3B ).[4] The phrenoesophageal ligament, which originates from the diaphragm s transversalis fascia and inserts on the lower esophagus, contributes to fixation of the LES within the diaphragmatic hiatus. This positioning is beneficial because it enables diaphragmatic contractions to assist the LES in maintenance of a high-pressure zone during exercise. The LES is contracted at rest, creating a high-pressure zone that prevents gastric contents from entering the esophagus. During swallowing, the LES relaxes to permit the swallowed bolus to be pushed by peristalsis from the esophagus into the stomach.")
23
Pared esofágica

24
Unión esófago-gástrica

26
The stomach, as a J-shaped dilation of the alimentary canal, is continuous with the esophagus proximally and the duodenum distally. It functions primarily as a res-ervoir to store large quantities of recently ingested food, thus allowing intermittent feedings, initiating the digestive process, and releasing its contents in a controlled fashion downstream to accommodate the much smaller capacity of the duodenum. The stomach volume ranges from about 30 mL in a neonate to 1.5 to 2 L in adulthood.

27
Estómago Dilatación en forma de J del canal alimentario
Funciona principalmente como reservorio de la comida permitiendo una alimentación intermitente Inicia el proceso digestivo Permite el paso controlado hacia el duodeno con menor capacidad Volumen entre 30 mL (RN) y 1.5 a 2 L (adulto) The stomach, as a J-shaped dilation of the alimentary canal, is continuous with the esophagus proximally and the duodenum distally. It functions primarily as a res-ervoir to store large quantities of recently ingested food, thus allowing intermittent feedings, initiating the digestive process, and releasing its contents in a controlled fashion downstream to accommodate the much smaller capacity of the duodenum. The stomach volume ranges from about 30 mL in a neonate to 1.5 to 2 L in adulthood.
 y 1.5 a 2 L (adulto) The stomach, as a J-shaped dilation of the alimentary canal, is continuous with the esophagus proximally and the duodenum distally. It functions primarily as a res-ervoir to store large quantities of recently ingested food, thus allowing intermittent feedings, initiating the digestive process, and releasing its contents in a controlled fashion downstream to accommodate the much smaller capacity of the duodenum. The stomach volume ranges from about 30 mL in a neonate to 1.5 to 2 L in adulthood.")
28
ESTÓMAGO The stomach, as a J-shaped dilation of the alimentary canal, is continuous with the esophagus proximally and the duodenum distally. It functions primarily as a res-ervoir to store large quantities of recently ingested food, thus allowing intermittent feedings, initiating the digestive process, and releasing its contents in a controlled fashion downstream to accommodate the much smaller capacity of the duodenum. The stomach volume ranges from about 30 mL in a neonate to 1.5 to 2 L in adulthood. The stomach is divided into four regions, which can be defined by anatomic or histologic landmarks ( Fig ).[2] Anatomically, the cardia is a small, ill-defined area of the stomach immediately adjacent to its junction with the esophagus. This region of the stomach has been the recent focus of intense investigation. Controversy exists as to the nature, location, extent, and even existence of cardiac mucosa. The fundus projects upward, above the cardia and gastroesophageal junction. This dome-shaped area of the stomach is its most superior portion and is in contact above with the left hemidiaphragm and to the left with the spleen. The body, or corpus, the largest portion of the stomach, is located immediately below and continuous with the fundus. The incisura angularis, a fixed, sharp indentation two thirds of the distance down the lesser curvature, marks the caudal aspect of the gastric body ( Fig ). The gastric antrum extends from its indistinct border with the body to the junction of the pylorus with the duodenum. These gross anatomic landmarks correspond roughly with the mucosal histology because antral mucosa (pyloric gland mucosa) actually extends from an area on the lesser curvature somewhat above the incisura. The pylorus (pyloric channel) is a tubular structure joining the duodenum to the stomach and contains the palpable circular muscle, the pyloric sphincter. The pylorus is somewhat mobile owing to its enclosure between the peritoneum of the greater and lesser omenta but is generally located 2 cm to the right of midline at L1. Corresponding motor and secretory functions of these regions of the stomach are discussed in detail in Chapters 46 and 47 .
.[2] Anatomically, the cardia is a small, ill-defined area of the stomach immediately adjacent to its junction with the esophagus. This region of the stomach has been the recent focus of intense investigation. Controversy exists as to the nature, location, extent, and even existence of cardiac mucosa. The fundus projects upward, above the cardia and gastroesophageal junction. This dome-shaped area of the stomach is its most superior portion and is in contact above with the left hemidiaphragm and to the left with the spleen. The body, or corpus, the largest portion of the stomach, is located immediately below and continuous with the fundus. The incisura angularis, a fixed, sharp indentation two thirds of the distance down the lesser curvature, marks the caudal aspect of the gastric body ( Fig ). The gastric antrum extends from its indistinct border with the body to the junction of the pylorus with the duodenum. These gross anatomic landmarks correspond roughly with the mucosal histology because antral mucosa (pyloric gland mucosa) actually extends from an area on the lesser curvature somewhat above the incisura. The pylorus (pyloric channel) is a tubular structure joining the duodenum to the stomach and contains the palpable circular muscle, the pyloric sphincter. The pylorus is somewhat mobile owing to its enclosure between the peritoneum of the greater and lesser omenta but is generally located 2 cm to the right of midline at L1. Corresponding motor and secretory functions of these regions of the stomach are discussed in detail in Chapters 46 and 47 .")
29
CAPAS DEL ESTÓMAGO

30
ESTÓMAGO Pliegues longitudinales que se aplanan con la distensión
La mucosa recubre la luz del estómago, es de apariencia aterciopeada y roja La submucosa es un tejido conectivo denso de colágena y elastina, contiene linfocitos, células plasmáticas, arteriolas, vénulas, linfáticos y el plexo submucoso The luminal surface of the gastric wall forms thick, longitudinally oriented folds or rugae, which flatten with distention. Four layers make up the gastric wall: mucosa, submucosa, muscularis propria, and serosa. Mucosa lines the gastric lumen, appearing as a smooth, velvety, blood-filled lining. The mucosa of the cardia, antrum, and pylorus is somewhat paler than that of the fundus and body. It is within the gastric mucosa that most of the functional secretory elements of the stomach are located (see Chapter 47 ). The submucosa, immediately deep to the mucosa, provides the dense connective tissue skeleton of collagen and elastin fibers. Lymphocytes, plasma cells, arterioles, venules, lymphatics, and the submucosal plexus are also contained within the submucosa. The third tissue layer, the muscularis propria, is a combination of three muscle layers: inner oblique, middle circular, and outer longitudinal. The inner oblique muscle fibers course over the gastric fundus, covering the anterior and posterior aspects of the stomach wall. The middle circular fibers encircle the body of the stomach, thickening distally to become the pyloric sphincter. The outer longitudinal muscle fibers course primarily along the greater and lesser curvatures of the stomach. The final layer of the stomach is the transparent serosa, a continuation of the visceral peritoneum.
. The submucosa, immediately deep to the mucosa, provides the dense connective tissue skeleton of collagen and elastin fibers. Lymphocytes, plasma cells, arterioles, venules, lymphatics, and the submucosal plexus are also contained within the submucosa. The third tissue layer, the muscularis propria, is a combination of three muscle layers: inner oblique, middle circular, and outer longitudinal. The inner oblique muscle fibers course over the gastric fundus, covering the anterior and posterior aspects of the stomach wall. The middle circular fibers encircle the body of the stomach, thickening distally to become the pyloric sphincter. The outer longitudinal muscle fibers course primarily along the greater and lesser curvatures of the stomach. The final layer of the stomach is the transparent serosa, a continuation of the visceral peritoneum.")
31
ESTÓMAGO Muscular propia Serosa: continuación del peritoneo visceral
Oblicua interna Circular media Longitudinal externa Serosa: continuación del peritoneo visceral The submucosa, immediately deep to the mucosa, provides the dense connective tissue skeleton of collagen and elastin fibers. Lymphocytes, plasma cells, arterioles, venules, lymphatics, and the submucosal plexus are also contained within the submucosa. The third tissue layer, the muscularis propria, is a combination of three muscle layers: inner oblique, middle circular, and outer longitudinal. The inner oblique muscle fibers course over the gastric fundus, covering the anterior and posterior aspects of the stomach wall. The middle circular fibers encircle the body of the stomach, thickening distally to become the pyloric sphincter. The outer longitudinal muscle fibers course primarily along the greater and lesser curvatures of the stomach. The final layer of the stomach is the transparent serosa, a continuation of the visceral peritoneum.

32
MUCOSA DEL ESTÓMAGO El epitelio se invagina formando glándulas Cardias
Fondo y cuerpo Antro y píloro: glándulas pilóricas con células productoras de gastrina (células G) y células productoras de moco The surface epithelial lining is invaginated by gastric pits, or foveolae, which provide the gastric glands access to the gastric lumen, with a ratio of one pit to four or five gastric glands. The gastric glands of different anatomic regions of the stomach are lined with different types of specialized epithelial cells, allowing for differentiation of these regions by type of gastric gland (see Fig ). The first region, the cardia, is a small transition zone from esophageal squamous epithelium to gastric columnar epithelium. The cardia has been a controversial histologic area of discussion with theories suggesting that its presence is pathologic. However, recent observations concluded that cardiac mucosa develops during gestation and is present at birth.[3] The cardiac glands have a branched and tortuous configuration and are populated by mucous, endocrine, and undifferentiated cells. There is a gradual transition from cardiac glands to the second region, the acid-secreting segment of the stomach. This region encompasses the gastric fundus and body and contains the parietal (or oxyntic or fundic) glands. Parietal, chief (also known as peptic), endocrine, mucous neck, and undifferentiated cells compose the oxyntic glands. The final region, corresponding to the antrum and pylorus, contains the pyloric glands, composed of endocrine cells, including gastrin-producing G cells and mucous cells. By far the most numerous and distinctive gastric glands are the oxyntic glands ( Fig ), responsible for the secretion of acid, intrinsic factor, and most gastric enzymes. These fairly straight and simple tubular glands are closely associated in the areas of gastric fundus and body. A typical gland is subdivided into three areas: the isthmus (where surface mucous cells predominate), the neck (where parietal and mucous neck cells predominate), and the base (where chief cells predominate, along with some parietal and mucous neck cells). Endocrine cells, somatostatin-containing D cells, and histamine-secreting enterochromaffin-like (ECL) cells are scattered throughout the oxyntic epithelium
 y células productoras de moco. The surface epithelial lining is invaginated by gastric pits, or foveolae, which provide the gastric glands access to the gastric lumen, with a ratio of one pit to four or five gastric glands. The gastric glands of different anatomic regions of the stomach are lined with different types of specialized epithelial cells, allowing for differentiation of these regions by type of gastric gland (see Fig ). The first region, the cardia, is a small transition zone from esophageal squamous epithelium to gastric columnar epithelium. The cardia has been a controversial histologic area of discussion with theories suggesting that its presence is pathologic. However, recent observations concluded that cardiac mucosa develops during gestation and is present at birth.[3] The cardiac glands have a branched and tortuous configuration and are populated by mucous, endocrine, and undifferentiated cells. There is a gradual transition from cardiac glands to the second region, the acid-secreting segment of the stomach. This region encompasses the gastric fundus and body and contains the parietal (or oxyntic or fundic) glands. Parietal, chief (also known as peptic), endocrine, mucous neck, and undifferentiated cells compose the oxyntic glands. The final region, corresponding to the antrum and pylorus, contains the pyloric glands, composed of endocrine cells, including gastrin-producing G cells and mucous cells. By far the most numerous and distinctive gastric glands are the oxyntic glands ( Fig ), responsible for the secretion of acid, intrinsic factor, and most gastric enzymes. These fairly straight and simple tubular glands are closely associated in the areas of gastric fundus and body. A typical gland is subdivided into three areas: the isthmus (where surface mucous cells predominate), the neck (where parietal and mucous neck cells predominate), and the base (where chief cells predominate, along with some parietal and mucous neck cells). Endocrine cells, somatostatin-containing D cells, and histamine-secreting enterochromaffin-like (ECL) cells are scattered throughout the oxyntic epithelium.")
33
MUCOSA DEL ESTÓMAGO Cada región tiene distintos tipos de glándulas
Cardias: transición del epitelio escamoso al columnar Fondo y cuerpo: glándulas oxínticas que producen ácido (parietales), factor intrínseco y enzimas (principales o zimogénicas que producen pepsinógeno I y II) Antro: células productoras de moco y células endócrinas productoras de gastrina en respuesta a la distensión gástrica, los aminoácidos y péptidos The surface epithelial lining is invaginated by gastric pits, or foveolae, which provide the gastric glands access to the gastric lumen, with a ratio of one pit to four or five gastric glands. The gastric glands of different anatomic regions of the stomach are lined with different types of specialized epithelial cells, allowing for differentiation of these regions by type of gastric gland (see Fig ). The first region, the cardia, is a small transition zone from esophageal squamous epithelium to gastric columnar epithelium. The cardia has been a controversial histologic area of discussion with theories suggesting that its presence is pathologic. However, recent observations concluded that cardiac mucosa develops during gestation and is present at birth.[3] The cardiac glands have a branched and tortuous configuration and are populated by mucous, endocrine, and undifferentiated cells. There is a gradual transition from cardiac glands to the second region, the acid-secreting segment of the stomach. This region encompasses the gastric fundus and body and contains the parietal (or oxyntic or fundic) glands. Parietal, chief (also known as peptic), endocrine, mucous neck, and undifferentiated cells compose the oxyntic glands. The final region, corresponding to the antrum and pylorus, contains the pyloric glands, composed of endocrine cells, including gastrin-producing G cells and mucous cells. By far the most numerous and distinctive gastric glands are the oxyntic glands ( Fig ), responsible for the secretion of acid, intrinsic factor, and most gastric enzymes. These fairly straight and simple tubular glands are closely associated in the areas of gastric fundus and body. A typical gland is subdivided into three areas: the isthmus (where surface mucous cells predominate), the neck (where parietal and mucous neck cells predominate), and the base (where chief cells predominate, along with some parietal and mucous neck cells). Endocrine cells, somatostatin-containing D cells, and histamine-secreting enterochromaffin-like (ECL) cells are scattered throughout the oxyntic epithelium
, factor intrínseco y enzimas (principales o zimogénicas que producen pepsinógeno I y II) Antro: células productoras de moco y células endócrinas productoras de gastrina en respuesta a la distensión gástrica, los aminoácidos y péptidos. The surface epithelial lining is invaginated by gastric pits, or foveolae, which provide the gastric glands access to the gastric lumen, with a ratio of one pit to four or five gastric glands. The gastric glands of different anatomic regions of the stomach are lined with different types of specialized epithelial cells, allowing for differentiation of these regions by type of gastric gland (see Fig ). The first region, the cardia, is a small transition zone from esophageal squamous epithelium to gastric columnar epithelium. The cardia has been a controversial histologic area of discussion with theories suggesting that its presence is pathologic. However, recent observations concluded that cardiac mucosa develops during gestation and is present at birth.[3] The cardiac glands have a branched and tortuous configuration and are populated by mucous, endocrine, and undifferentiated cells. There is a gradual transition from cardiac glands to the second region, the acid-secreting segment of the stomach. This region encompasses the gastric fundus and body and contains the parietal (or oxyntic or fundic) glands. Parietal, chief (also known as peptic), endocrine, mucous neck, and undifferentiated cells compose the oxyntic glands. The final region, corresponding to the antrum and pylorus, contains the pyloric glands, composed of endocrine cells, including gastrin-producing G cells and mucous cells. By far the most numerous and distinctive gastric glands are the oxyntic glands ( Fig ), responsible for the secretion of acid, intrinsic factor, and most gastric enzymes. These fairly straight and simple tubular glands are closely associated in the areas of gastric fundus and body. A typical gland is subdivided into three areas: the isthmus (where surface mucous cells predominate), the neck (where parietal and mucous neck cells predominate), and the base (where chief cells predominate, along with some parietal and mucous neck cells). Endocrine cells, somatostatin-containing D cells, and histamine-secreting enterochromaffin-like (ECL) cells are scattered throughout the oxyntic epithelium.")
34
Closely associated with parietal cells are mucous neck cells, which appear singly, close to parietal cells or in groups of two or three in the oxyntic gland neck or isthmus. Mucous neck cells differ from their surface counterparts in their synthesis of acidic, sulfated mucus rather than the neutral mucus. Additionally, mucous neck cells have basal nuclei and larger mucous granules around the nucleus rather than apically located granules. Function of the two cell types appears different in that surface mucous cells are cytoprotective, whereas the mucous neck cell functions as a stem cell precursor for surface mucous, parietal, chief, and endocrine cells. Chief cells, also known as zymogen cells, predominate in deeper layers of the oxyntic glands. These pyramid-shaped cells play a role in synthesis and secretion of pepsinogens I and II. The cytoplasm of chief cells has prominent basophilic staining owing to abundance of ribosomes; these ribosomes are either free in cytoplasm or in association with an extensive endoplasmic reticulum system. Zymogen granules lie in the apical cytoplasm; their contents are released into the gastric lumen following fusion of the limiting membrane of the granule with the luminal membrane. Once in the lumen, pepsinogens are converted to pepsin. A variety of endocrine, or enteroendocrine, cells are scattered among the cells of the oxyntic glands. These cells vary in location, being either open or closed relative to the gastric lumen. Open endocrine cells have apical membranes containing receptors; these open cells discharge their contents by basilar exocytosis into the bloodstream, thus exerting an endocrine effect. The closed endocrine cells contain several processes that terminate near its target cells, constituting the so-called paracrine effect. The oxyntic gland model of the closed cell is the D cell, which secretes somatostatin via long processes reaching ECL, parietal, and chief cells. The final region of the stomach encompasses the antrum and pylorus and contains extensively coiled antral glands composed of endocrine and epithelial cells. The epithelial cells are predominantly mucous cells, and there are small numbers of pepsinogen II-secreting oxyntic cells. Although also small in number, gastrin-secreting (G) cells play a vital physiologic role and are the prototype of the open enteroendocrine cell. These cells, which occur either singly or in small clusters in the mid to deep sections of antral glands ( Fig. 45-7A ), contain a basilar cytoplasm densely packed with gastrin-containing secretory granules ( Fig. 45-7B ). Gastrin release is stimulated by gastric distention, vagal stimulation, dietary amino acids, and peptide, with rapid appearance of the hormone into the bloodstream in the postprandial period (see Chapter 47 ). The apical or luminal surface of the G cell is narrowed into small microvilli thought to contain receptors responsible for amino acid and peptide stimulation of gastrin release. Significant quantities of gastrin are also secreted into the gastric lumen; gastrin is a known gastric growth and differentiation factor, mediated through upregulation of heparin-binding epidermal-like growth factor (HB-EGF) in gastric parietal cells. [4] [5]
 cells play a vital physiologic role and are the prototype of the open enteroendocrine cell. These cells, which occur either singly or in small clusters in the mid to deep sections of antral glands ( Fig. 45-7A ), contain a basilar cytoplasm densely packed with gastrin-containing secretory granules ( Fig. 45-7B ). Gastrin release is stimulated by gastric distention, vagal stimulation, dietary amino acids, and peptide, with rapid appearance of the hormone into the bloodstream in the postprandial period (see Chapter 47 ). The apical or luminal surface of the G cell is narrowed into small microvilli thought to contain receptors responsible for amino acid and peptide stimulation of gastrin release. Significant quantities of gastrin are also secreted into the gastric lumen; gastrin is a known gastric growth and differentiation factor, mediated through upregulation of heparin-binding epidermal-like growth factor (HB-EGF) in gastric parietal cells. [4] [5]")
35
Duodeno

37
Corte transversal en L2-L3

38
Intestino delgado

39
Intestino delgado

41
Ciego y apéndice cecal

42
Recto y ano

44
Hígado cara anterior The normal liver occupies the right upper quadrant and extends from the fifth intercostal space in the midclavicular line to the right costal margin. The lower margin of the liver descends below the costal margin during inspiration. The median liver weight is 1800 g in men and 1400 g in women. [5] [6] Transcutaneous liver biopsy specimens are commonly obtained in the midaxillary line through the third interspace below the upper limit of liver dullness during full expiration; this site is usually in the ninth intercostal space. The superior, anterior, and right lateral surfaces of the liver are smooth and convex, fitting against the diaphragm. The posterior surface has indentations from the colon, right kidney, and duodenum on the right lobe and the stomach on the left lobe

45
Hígado Cuadrante superior derecho
El márgen inferior del hígado desciende por debajo del margen costal durante la inspiración Pesa entre 1400 gr y 1800 gr The normal liver occupies the right upper quadrant and extends from the fifth intercostal space in the midclavicular line to the right costal margin. The lower margin of the liver descends below the costal margin during inspiration. The median liver weight is 1800 g in men and 1400 g in women. [5] [6] Transcutaneous liver biopsy specimens are commonly obtained in the midaxillary line through the third interspace below the upper limit of liver dullness during full expiration; this site is usually in the ninth intercostal space. The superior, anterior, and right lateral surfaces of the liver are smooth and convex, fitting against the diaphragm. The posterior surface has indentations from the colon, right kidney, and duodenum on the right lobe and the stomach on the left lobe

46
Hígado Tiene una circulación arterial y una circulación portal que recibe la sangre del tracto GI entre el estómago proximal y el recto superior, el bazo, páncreas y vesícula La vena esplénica y la mesentérica superior forman la vena porta The portal vein normally supplies 70% of the blood flow to the hepatic parenchyma. The portal vein receives almost all of the blood flow from the digestive tract between the proximal stomach and upper rectum as well as from the spleen, pancreas, and gallbladder ( Fig ). The splenic and superior mesenteric veins join behind the pancreas to form the portal vein. The splenic vein sits in a groove of the pancreas and receives the short gastric veins, pancreatic veins, left gastroepiploic vein, and inferior mesenteric vein. The portal vein receives the superior pancreaticoduodenal vein and the left gastric (coronary) vein. The superior mesenteric vein receives the inferior pancreaticoduodenal vein and the right gastroepiploic vein. There is some variation in the veins that drain into the portal system.
. The splenic and superior mesenteric veins join behind the pancreas to form the portal vein. The splenic vein sits in a groove of the pancreas and receives the short gastric veins, pancreatic veins, left gastroepiploic vein, and inferior mesenteric vein. The portal vein receives the superior pancreaticoduodenal vein and the left gastric (coronary) vein. The superior mesenteric vein receives the inferior pancreaticoduodenal vein and the right gastroepiploic vein. There is some variation in the veins that drain into the portal system.")
47
The portal vein normally supplies 70% of the blood flow to the hepatic parenchyma. The portal vein receives almost all of the blood flow from the digestive tract between the proximal stomach and upper rectum as well as from the spleen, pancreas, and gallbladder ( Fig ). The splenic and superior mesenteric veins join behind the pancreas to form the portal vein. The splenic vein sits in a groove of the pancreas and receives the short gastric veins, pancreatic veins, left gastroepiploic vein, and inferior mesenteric vein. The portal vein receives the superior pancreaticoduodenal vein and the left gastric (coronary) vein. The superior mesenteric vein receives the inferior pancreaticoduodenal vein and the right gastroepiploic vein. There is some variation in the veins that drain into the portal system.
. The splenic and superior mesenteric veins join behind the pancreas to form the portal vein. The splenic vein sits in a groove of the pancreas and receives the short gastric veins, pancreatic veins, left gastroepiploic vein, and inferior mesenteric vein. The portal vein receives the superior pancreaticoduodenal vein and the left gastric (coronary) vein. The superior mesenteric vein receives the inferior pancreaticoduodenal vein and the right gastroepiploic vein. There is some variation in the veins that drain into the portal system..")
48
HÍGADO Hepatocitos: células polihédricas
Actividad sintética y metabólica Tienen superficie sinusoidal, canalicular y contigua Superficie sinusoidal: espacio de Disse con intercambio entre el plasma y los hepatocitos Hepatocytes are large polyhedral cells approximately 20 to 30 μm in diameter.[2] Consistent with their high synthetic and metabolic activity, hepatocytes are enriched in organelles. About 30% of human hepatocytes are binucleate. Hepatocytes are polarized epithelial cells. Their plasma membranes have three distinct domains—(1) the sinusoidal surface (=37% of the cell surface) that comes in direct contact with plasma through the fenestrae of the specialized hepatic sinusoidal endothelial cells, (2) the canalicular surface (=13% of the cell surface) that encloses the bile canaliculus, and (3) contiguous surfaces. By analogy with glandular epithelia, the sinusoidal, canalicular, and contiguous plasma membrane domains are also called the basolateral, apical, and lateral surfaces, respectively.[3] The sinusoidal and canalicular surfaces contain microvilli, which greatly extend the surface area of these domains. The space between the endothelia and the sinusoidal villi is termed the space of Disse. There is a bidirectional exchange of liquids and solutes between the plasma and hepatocytes at the sinusoidal surface. In many cases, the molecular transfer is augmented by proteins that promote facilitated diffusion or energy-consuming active transport. The canalicular domains of two adjacent hepatocytes are sealed at the periphery by tight junctions (desmosomes), thereby delimiting the bile canaliculus, which is the beginning of the biliary drainage system (see Chapter 59 ). In contrast to the bidirectional flow at the sinusoidal surface, flow from hepatocytes into the bile canaliculi is predominantly unidirectional.
 the sinusoidal surface (=37% of the cell surface) that comes in direct contact with plasma through the fenestrae of the specialized hepatic sinusoidal endothelial cells, (2) the canalicular surface (=13% of the cell surface) that encloses the bile canaliculus, and (3) contiguous surfaces. By analogy with glandular epithelia, the sinusoidal, canalicular, and contiguous plasma membrane domains are also called the basolateral, apical, and lateral surfaces, respectively.[3] The sinusoidal and canalicular surfaces contain microvilli, which greatly extend the surface area of these domains. The space between the endothelia and the sinusoidal villi is termed the space of Disse. There is a bidirectional exchange of liquids and solutes between the plasma and hepatocytes at the sinusoidal surface. In many cases, the molecular transfer is augmented by proteins that promote facilitated diffusion or energy-consuming active transport. The canalicular domains of two adjacent hepatocytes are sealed at the periphery by tight junctions (desmosomes), thereby delimiting the bile canaliculus, which is the beginning of the biliary drainage system (see Chapter 59 ). In contrast to the bidirectional flow at the sinusoidal surface, flow from hepatocytes into the bile canaliculi is predominantly unidirectional.")
49
Hepatocytes are large polyhedral cells approximately 20 to 30 μm in diameter.[2] Consistent with their high synthetic and metabolic activity, hepatocytes are enriched in organelles. About 30% of human hepatocytes are binucleate. Hepatocytes are polarized epithelial cells. Their plasma membranes have three distinct domains—(1) the sinusoidal surface (=37% of the cell surface) that comes in direct contact with plasma through the fenestrae of the specialized hepatic sinusoidal endothelial cells, (2) the canalicular surface (=13% of the cell surface) that encloses the bile canaliculus, and (3) contiguous surfaces. By analogy with glandular epithelia, the sinusoidal, canalicular, and contiguous plasma membrane domains are also called the basolateral, apical, and lateral surfaces, respectively.[3] The sinusoidal and canalicular surfaces contain microvilli, which greatly extend the surface area of these domains. The space between the endothelia and the sinusoidal villi is termed the space of Disse. There is a bidirectional exchange of liquids and solutes between the plasma and hepatocytes at the sinusoidal surface. In many cases, the molecular transfer is augmented by proteins that promote facilitated diffusion or energy-consuming active transport. The canalicular domains of two adjacent hepatocytes are sealed at the periphery by tight junctions (desmosomes), thereby delimiting the bile canaliculus, which is the beginning of the biliary drainage system (see Chapter 59 ). In contrast to the bidirectional flow at the sinusoidal surface, flow from hepatocytes into the bile canaliculi is predominantly unidirectional.
![Hepatocytes are large polyhedral cells approximately 20 to 30 μm in diameter.[2] Consistent with their high synthetic and metabolic activity, hepatocytes are enriched in organelles. About 30% of human hepatocytes are binucleate. Hepatocytes are polarized epithelial cells. Their plasma membranes have three distinct domains—(1) the sinusoidal surface (=37% of the cell surface) that comes in direct contact with plasma through the fenestrae of the specialized hepatic sinusoidal endothelial cells, (2) the canalicular surface (=13% of the cell surface) that encloses the bile canaliculus, and (3) contiguous surfaces. By analogy with glandular epithelia, the sinusoidal, canalicular, and contiguous plasma membrane domains are also called the basolateral, apical, and lateral surfaces, respectively.[3] The sinusoidal and canalicular surfaces contain microvilli, which greatly extend the surface area of these domains.](http://slideplayer.es/slide/1107784/3/images/49/Hepatocytes+are+large+polyhedral+cells+approximately+20+to+30+%CE%BCm+in+diameter.%5B2%5D+Consistent+with+their+high+synthetic+and+metabolic+activity%2C+hepatocytes+are+enriched+in+organelles.+About+30%25+of+human+hepatocytes+are+binucleate.+Hepatocytes+are+polarized+epithelial+cells.+Their+plasma+membranes+have+three+distinct+domains%E2%80%94%281%29+the+sinusoidal+surface+%28%3D37%25+of+the+cell+surface%29+that+comes+in+direct+contact+with+plasma+through+the+fenestrae+of+the+specialized+hepatic+sinusoidal+endothelial+cells%2C+%282%29+the+canalicular+surface+%28%3D13%25+of+the+cell+surface%29+that+encloses+the+bile+canaliculus%2C+and+%283%29+contiguous+surfaces.+By+analogy+with+glandular+epithelia%2C+the+sinusoidal%2C+canalicular%2C+and+contiguous+plasma+membrane+domains+are+also+called+the+basolateral%2C+apical%2C+and+lateral+surfaces%2C+respectively.%5B3%5D+The+sinusoidal+and+canalicular+surfaces+contain+microvilli%2C+which+greatly+extend+the+surface+area+of+these+domains..jpg "The space between the endothelia and the sinusoidal villi is termed the space of Disse. There is a bidirectional exchange of liquids and solutes between the plasma and hepatocytes at the sinusoidal surface. In many cases, the molecular transfer is augmented by proteins that promote facilitated diffusion or energy-consuming active transport. The canalicular domains of two adjacent hepatocytes are sealed at the periphery by tight junctions (desmosomes), thereby delimiting the bile canaliculus, which is the beginning of the biliary drainage system (see Chapter 59 ). In contrast to the bidirectional flow at the sinusoidal surface, flow from hepatocytes into the bile canaliculi is predominantly unidirectional.")
50
Hepatic Sinusoidal Endothelial Cells
Hepatic sinusoidal endothelial cells (HSECs) account for 20% of total liver cells. These cells are distinguished by the fenestrae (pores) in their flat, thin extensions that form sieve plates. Unlike capillary endothelial cells, HSECs do not form intracellular junctions and simply overlap one another (see Fig ). The presence of fenestrae and the absence of a basement membrane permit plasma to enter the space of Disse and come in direct contact with the sinusoidal surfaces of hepatocytes (see Chapter 68 ).[49] Diameters of the fenestrae are controlled actively by the actin-containing components of the cytoskeleton in response to changes in the chemical milieu.[50] Therefore, the specialized endothelial lining of hepatic sinusoids serves as a selective barrier between the blood and the hepatocytes. HSECs can secrete prostaglandins and a wide variety of proteins, including interleukin-1 (IL-1) and IL-6, interferon, tumor necrosis factor-α (TNF-α), and endothelin. Kupffer Cells Kupffer cells are specialized tissue macrophages that account for 80% to 90% of the total population of fixed macrophages in the body. These cells are derived from bone marrow stem cells or monocytes and are highly active in removing particulate matters and toxic or foreign substances that appear in the portal blood from the intestines.[51] Kupffer cells are located in the sinusoidal lumen and are in direct contact with endothelial cells (see Fig ). They possess bristle-coated micropinocytic vesicles, fuzzy-coated vacuoles, and worm-like structures that are special features of cells active in pinocytosis and phagocytosis. An abundance of lysosomes reflects the prominent role of Kupffer cells in degrading substances taken up from the blood stream. Kupffer cells secrete a variety of vasoactive toxic mediators that may be involved in host defense mechanisms and in pathophysiologic processes in some liver diseases. Kupffer cells increase in number and activity in response to chemical, infectious, or immunologic injury to the liver.[52]
 account for 20% of total liver cells. These cells are distinguished by the fenestrae (pores) in their flat, thin extensions that form sieve plates. Unlike capillary endothelial cells, HSECs do not form intracellular junctions and simply overlap one another (see Fig ). The presence of fenestrae and the absence of a basement membrane permit plasma to enter the space of Disse and come in direct contact with the sinusoidal surfaces of hepatocytes (see Chapter 68 ).[49] Diameters of the fenestrae are controlled actively by the actin-containing components of the cytoskeleton in response to changes in the chemical milieu.[50] Therefore, the specialized endothelial lining of hepatic sinusoids serves as a selective barrier between the blood and the hepatocytes. HSECs can secrete prostaglandins and a wide variety of proteins, including interleukin-1 (IL-1) and IL-6, interferon, tumor necrosis factor-α (TNF-α), and endothelin. Kupffer Cells. Kupffer cells are specialized tissue macrophages that account for 80% to 90% of the total population of fixed macrophages in the body. These cells are derived from bone marrow stem cells or monocytes and are highly active in removing particulate matters and toxic or foreign substances that appear in the portal blood from the intestines.[51] Kupffer cells are located in the sinusoidal lumen and are in direct contact with endothelial cells (see Fig ). They possess bristle-coated micropinocytic vesicles, fuzzy-coated vacuoles, and worm-like structures that are special features of cells active in pinocytosis and phagocytosis. An abundance of lysosomes reflects the prominent role of Kupffer cells in degrading substances taken up from the blood stream. Kupffer cells secrete a variety of vasoactive toxic mediators that may be involved in host defense mechanisms and in pathophysiologic processes in some liver diseases. Kupffer cells increase in number and activity in response to chemical, infectious, or immunologic injury to the liver.[52]")
53
Páncreas The pancreas is a soft, elongated, flattened gland 12 to 20 cm in length. [4] [5] [6] The adult gland weighs between 70 and 110 g. The head lies behind the peritoneum of the posterior abdominal wall and has a lobular structure. The pancreas is covered with a fine connective tissue but does not have a true capsule. The head of the pancreas is on the right side and lies within the curvature of the duodenum. The neck, body, and tail of the pancreas lie obliquely in the posterior abdomen, with the tail extending as far as the gastric surface of the spleen ( Fig The second and third duodenum curvatures lie around the head of the pancreas. The anterior surface of the head of the pancreas is adjacent to the pylorus, the first part of the duodenum, and the transverse colon. The posterior surface abuts the hilus and medial border of the right kidney, the inferior vena cava and the right renal vessels, the right gonadal vein, and the right crus of the diaphragm. The uncinate process is a prolongation of pancreatic tissue of variable size and shape. It projects off the lower part of the head of the pancreas, extending upward and to the left. The uncinate process lies anterior to the aorta and inferior vena cava and is covered superiorly by the superior mesenteric vessels that emerge below the neck of the pancreas. There is much variation in the uncinate process, which may even be absent altogether. The neck of the pancreas is a constricted part of the gland extending from the head of the pancreas toward the left, joining the head with the body of the pancreas. It is 1.5 to 2.0 cm long and 3.0 to 4.0 cm wide. Posterior to the neck of the pancreas lies the confluence of the portal vein with the superior mesenteric and splenic veins. Anteriorly it is covered in part by the pylorus and peritoneum of the lesser sac. The neck extends to the right as far as the anterosuperior pancreaticoduodenal artery from the gastroduodenal artery. The body of the pancreas runs toward the left side, anterior to the aorta. It is retroperitoneal and held against the aorta by the peritoneum of the lesser sac. The anterior surface of the body is covered by peritoneum of the omental bursa that separates the stomach from the pancreas. The antrum and body of the stomach and the transverse mesocolon contact the body anteriorly. Posterior to the body of the pancreas are the aorta, the origin of the superior mesenteric artery, the left crus of the diaphragm, the left kidney, the left adrenal gland, and the splenic vein. The midline part of the body overlies the lumbar spine, which makes this area of the pancreas most vulnerable to abdominal trauma. The body passes laterally and merges with the tail of the pancreas without a discernible junction point. The tail is relatively mobile, its tip usually reaching the hilus of the spleen. With the splenic artery and vein, the tail is contained between the two layers of the splenorenal ligament. The splenocolic ligament attaches the splenic flexure of the colon to the spleen and brings it near the tail of the pancreas. The relationship of the pancreas to important structures in the posterior abdomen is seen i

54
Páncreas Glándula de 12 a 20 cm de longitud Pesa entre 70 y 110 g
Retroperitoneal Cabeza rodeada por el duodeno Cabeza, cuello, cuerpo y cola The pancreas is a soft, elongated, flattened gland 12 to 20 cm in length. [4] [5] [6] The adult gland weighs between 70 and 110 g. The head lies behind the peritoneum of the posterior abdominal wall and has a lobular structure. The pancreas is covered with a fine connective tissue but does not have a true capsule. The head of the pancreas is on the right side and lies within the curvature of the duodenum. The neck, body, and tail of the pancreas lie obliquely in the posterior abdomen, with the tail extending as far as the gastric surface of the spleen ( Fig The second and third duodenum curvatures lie around the head of the pancreas. The anterior surface of the head of the pancreas is adjacent to the pylorus, the first part of the duodenum, and the transverse colon. The posterior surface abuts the hilus and medial border of the right kidney, the inferior vena cava and the right renal vessels, the right gonadal vein, and the right crus of the diaphragm. The uncinate process is a prolongation of pancreatic tissue of variable size and shape. It projects off the lower part of the head of the pancreas, extending upward and to the left. The uncinate process lies anterior to the aorta and inferior vena cava and is covered superiorly by the superior mesenteric vessels that emerge below the neck of the pancreas. There is much variation in the uncinate process, which may even be absent altogether. The neck of the pancreas is a constricted part of the gland extending from the head of the pancreas toward the left, joining the head with the body of the pancreas. It is 1.5 to 2.0 cm long and 3.0 to 4.0 cm wide. Posterior to the neck of the pancreas lies the confluence of the portal vein with the superior mesenteric and splenic veins. Anteriorly it is covered in part by the pylorus and peritoneum of the lesser sac. The neck extends to the right as far as the anterosuperior pancreaticoduodenal artery from the gastroduodenal artery. The body of the pancreas runs toward the left side, anterior to the aorta. It is retroperitoneal and held against the aorta by the peritoneum of the lesser sac. The anterior surface of the body is covered by peritoneum of the omental bursa that separates the stomach from the pancreas. The antrum and body of the stomach and the transverse mesocolon contact the body anteriorly. Posterior to the body of the pancreas are the aorta, the origin of the superior mesenteric artery, the left crus of the diaphragm, the left kidney, the left adrenal gland, and the splenic vein. The midline part of the body overlies the lumbar spine, which makes this area of the pancreas most vulnerable to abdominal trauma. The body passes laterally and merges with the tail of the pancreas without a discernible junction point. The tail is relatively mobile, its tip usually reaching the hilus of the spleen. With the splenic artery and vein, the tail is contained between the two layers of the splenorenal ligament. The splenocolic ligament attaches the splenic flexure of the colon to the spleen and brings it near the tail of the pancreas. The relationship of the pancreas to important structures in the posterior abdomen is seen i

55
Although the acinar cell secretes several different digestive enzymes in the exocrine pancreas, each cell type in the endocrine pancreas appears to secrete a single hormone. The four major types of cells found are B cells, A cells, D cells, and PP cells. [60] [61] B cells (beta cells), the most numerous (50% to 80%), secrete insulin.[60] A cells or alpha cells (5% to 20%) secrete glucagon. PP (pancreatic polypeptide) cells (10% to 35%) secrete pancreatic polypeptide. D cells (5%) secrete somatostatin. Other rare cell types occur in the islet.[62] In humans, the islets are subdivided into units, each of which exhibits a central aggregation of B cells surrounded by varying numbers of peripherally located cells that secrete the other hormones.
, the most numerous (50% to 80%), secrete insulin.[60] A cells or alpha cells (5% to 20%) secrete glucagon. PP (pancreatic polypeptide) cells (10% to 35%) secrete pancreatic polypeptide. D cells (5%) secrete somatostatin. Other rare cell types occur in the islet.[62] In humans, the islets are subdivided into units, each of which exhibits a central aggregation of B cells surrounded by varying numbers of peripherally located cells that secrete the other hormones..")
56
Islotes y acinos Acinos o exócrino: secretan enximas digestivas: tripsina, quimotripsina, lipasa, amilasa, Endócrino: Células B: insulina Células A: glucagon Células D: somatostatina Células PP: polipéptido pancreático Although the acinar cell secretes several different digestive enzymes in the exocrine pancreas, each cell type in the endocrine pancreas appears to secrete a single hormone. The four major types of cells found are B cells, A cells, D cells, and PP cells. [60] [61] B cells (beta cells), the most numerous (50% to 80%), secrete insulin.[60] A cells or alpha cells (5% to 20%) secrete glucagon. PP (pancreatic polypeptide) cells (10% to 35%) secrete pancreatic polypeptide. D cells (5%) secrete somatostatin. Other rare cell types occur in the islet.[62] In humans, the islets are subdivided into units, each of which exhibits a central aggregation of B cells surrounded by varying numbers of peripherally located cells that secrete the other hormones.
, the most numerous (50% to 80%), secrete insulin.[60] A cells or alpha cells (5% to 20%) secrete glucagon. PP (pancreatic polypeptide) cells (10% to 35%) secrete pancreatic polypeptide. D cells (5%) secrete somatostatin. Other rare cell types occur in the islet.[62] In humans, the islets are subdivided into units, each of which exhibits a central aggregation of B cells surrounded by varying numbers of peripherally located cells that secrete the other hormones.")
Presentaciones similares