Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Trastornos digestivos funcionales Colon irritable
XXVI CURSO DE APARATO DIGESTIVO COLEGIO DE MÉDICOS Santa Cruz de Tenerife 19-23 Marzo 2007 Dr. Carlos Casanova Trujillo Médico Adjunto Servicio de Digestivo del HUC

2
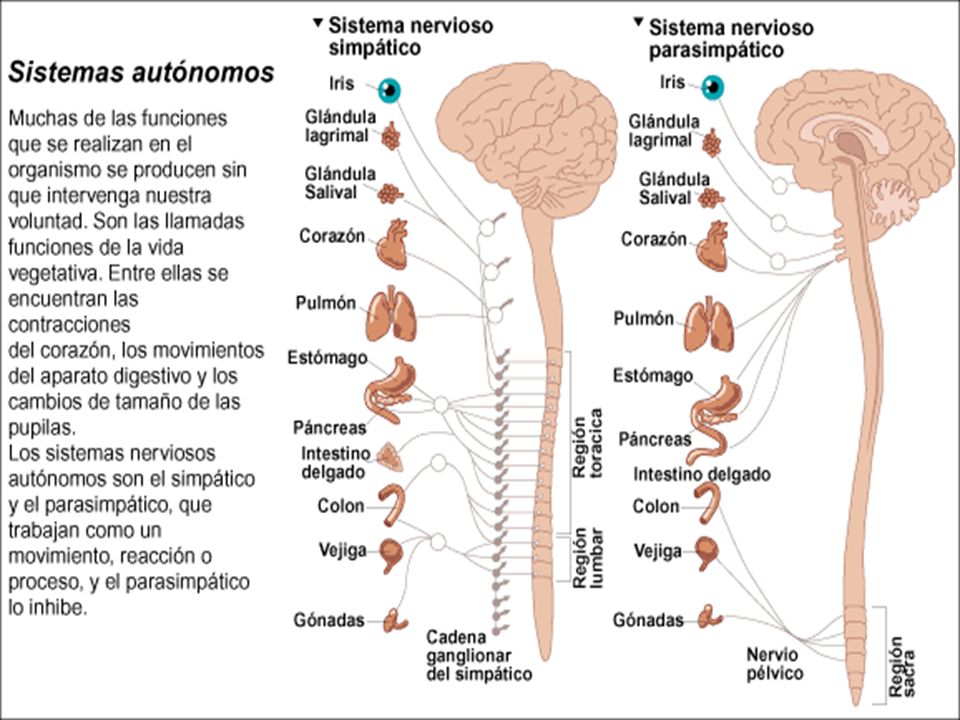
Funciones Aparato Digestivo
F. Motora F. Secretora F. Digestiva F. Absortiva F. Eliminación F. Inmunológica Integradas en respuestas coordinadas Reguladas minuto a minuto Moduladas por múltiples estímulos

4
Percepción Integración Efecto SII - Fisiopatología Conocimiento
Estado afectivo Vista Sonido Olfato Sensib. somática Motilidad Secreción Flujo sang. Inflamación Sensibilidad visceral

5
Serotonina Las células enterocromafines (CE) segregan serotonin
La serotonina se une a receptores en los nervios que modulan las motilidad, secreción y sensibilidad SERT (serotonin reuptake transporter) la introduce en las células epiteliales para su inactivación Gerson MD, Rev Gasterol Dis 2003; 3:S25
 la introduce en las células epiteliales para su inactivación. Gerson MD, Rev Gasterol Dis 2003; 3:S25.")
6
Neurona motora excitatoria
SII - Fisiología Receptores Serotonérgicos 5-HT4 Neurona motora excitatoria Neurona motora Inhibitoria SEROTONIN RECEPTORS AND THEIR ACTION ON INTESTINAL SMOOTH MUSCLE Serotonin in phylogenetically among the oldest of neurotransmitters. Its receptors are widely distributed throughout the brain and the peripheral nervous system including the digestive tract. Fourteen unique serotonergic receptor subtypes and their related genes are recognized currently in mammals. With the exception of the 5-HT5B receptor, all mammalian species appear to have the same set of serotonergic receptor genes. This has allowed development of a consistent molecular nomenclature for the serotonergic receptor subtypes. Thirteen of the serotonergic receptors are metabotropic receptors characterized by 7 transmembrane spanning regions. Pharmacologists used biochemical and physiological results to classify the 13 receptor subtypes into 6 subfamilies denoted as 5-HT1-6. The 5-HT1 subfamily contains 6 subtypes identified as 5-HT1A-F and the 5-HT2 subfamily as 5-HT2A-B. The 5-HT5 subfamily has 2 members and the 5-HT4, 5-HT6 and 5-HT7 subfamilies have only one member. The 14th member of the serotonergic receptor family is an ionotropic receptor identified as the 5-HT3 receptor. The 5-HT3 receptor like the nicotinic receptor for acetylcholine is a receptor-gated cation channel. Binding of 5-HT to this receptor, rather than activating intracellular metabolic pathways, opens an ionic channel that leads to depolarization of the membrane electrical potential. Unlike the other serotonergic receptor subtypes, the 5-HT3 receptor is expressed only by neurons in both the peripheral and central nervous system. The remaining 13 serotonergic receptor subtypes may be expressed by neurons, smooth muscle and other kinds of cells. The 5-HT1, 5-HT4 and 5-HT3 receptors are the main serotonergic receptor subtypes in the digestive tract. All three subtypes are expressed by neurons in the enteric nervous system. Intramural spinal and vagal sensory afferent terminals also express the 5-HT3 receptor subtype. The 5-HT4 receptor subtype is expressed both by enteric neurons and smooth muscles in the digestive tract. Smooth muscle of the esophagus and ileum of animals and of human colon express the 5-HT4 receptor. Stimulation of the various subtypes of 5-HT receptors associated with enteric neurons may lead to activation of excitatory musculomotor neurons and secretomotor neurons or to activation of inhibitory musculomotor neurons. Stimulation of excitatory musculomotor neurons will lead to muscle contraction; stimulation of inhibitory musculomotor neurons will lead to suppression of muscle contraction. Hoyer D, Clarke DE, Fozard JR, Hartig PR, Martin GR, Mylecharane EJ, Saxena PR, Humbhrey PPA. VII. International union of pharmacology classification of receptors for 5-hydroxytryptamine (serotonin). Pharmacol Rev 1994; 46: Humphrey PPA, Bountra C, Clayton N, Kozlowski K. Review article: the therapeutic potential of 5-HT3 receptor antagonists in the treatment of irritable bowel syndrome. Alimen Pharmacol Ther 1999; 13 suppl 2: Peroutka JA, Howell TA. The molecular evolution of G protein-coupled receptors: focus 5-hydroxytryptamine receptors. Neuropharmacology 1994; 33: 5-HT1A 5-HT3 ACh NO, VIP 5-HT1D Contracción Relajación
. Pharmacol Rev 1994; 46: Humphrey PPA, Bountra C, Clayton N, Kozlowski K. Review article: the therapeutic potential of 5-HT3 receptor antagonists in the treatment of irritable bowel syndrome. Alimen Pharmacol Ther 1999; 13 suppl 2: Peroutka JA, Howell TA. The molecular evolution of G protein-coupled receptors: focus 5-hydroxytryptamine receptors. Neuropharmacology 1994; 33: HT1A. 5-HT3. ACh. NO, VIP. 5-HT1D. Contracción. Relajación.")
7
Trastornos digestivo funcionales
Definición: conjunto de molestias atribuibles al aparato digestivo en las que no se demuestra una causa orgánica

8
“Orgánico” “Funcional” Trastorno GI Trastorno GI
Dominio primario Organo/tejido Persona Criterio Patológico Síntomas Medición Histología Motilidad Patología Sensación Endoscopia Percepción Radiología Psicosocial Opciones Trat. Medicación Pro/anti-kineticos Cirugía Analgésicos Antidepresivos Conductual Ejemplos Esofagitis Dolor esofágico Ulcera péptica Dispepsia funcional Enf. Crohn SII Pancr. Cancer Dolor abd. funcional

9
“Espero doctor, que no sea Ud. uno más de esos 20
doctores incompetentes que dicen que no tengo nada y que no me encuentran nada anómalo.”

11
Trastornos funcionales intestinales (C)
Rome III Trastornos funcionales intestinales (C) Sindr. intestino irritable (C1) Distensión funcional (C2) Estreñim. funcional (C3) Diarrea funcional (C4) No específico (C5) Slide 83 - Functional Bowel Disorders and Functional Abdominal Pain The functional bowel disorders include: a) irritable bowel syndrome, which is the most common and most extensively studied functional disorder; b) functional abdominal bloating referring to abdominal fullness, bloating or distension unrelated to obvious maldigestion (e.g., lactose intolerance) or excess consumption of poorly digestible but fermentable food stuffs (e.g., sorbitol, beans, wheat bran), in the absence of functional dyspepsia or IBS; c) functional constipation, defined as straining at defecation, a sensation of incomplete evacuation, and the infrequent (two or fewer) passage of lumpy or hard stools in the absence of IBS; and d) functional diarrhea; referring to the frequent (more than three/day) and painless passage of unformed stools associated with a slight increase in stool volume (<500 g/day). Functional abdominal pain is frequently recurrent or continuous pain not associated with physiological events (eating, defecation, menses) and loss of daily function in the absence of organic disease or other functional GI disorders. It is considered a separate category from the functional bowel disorders since there is no evidence for a disturbance of intestinal motility, which typifies the functional bowel disorders. Thompson WG, Longstreth GF, Drossman DA, et. al. C. Functional Bowel Disorders and D. Functional Abdominal Pain. In: Drossman, D. A., Talley, N. J., Thompson, W. G., Whitehead, W. E., and Corazziari, E. Rome II: Functional Gastrointestinal Disorders: Diagnosis, Pathophysiology, and Treatment,2 ed. McLean, VA: Degnon Associates, Inc., 2000: Thompson WG, Longstreth GF, Drossman DA, et. al. Functional Bowel Disorders and Functional Abdominal Pain. Gut 1999; 45:II43-II46. 1786
 Sindr. intestino irritable (C1) Distensión funcional (C2) Estreñim. funcional (C3) Diarrea funcional (C4) No específico (C5) Slide 83 - Functional Bowel Disorders and Functional Abdominal Pain. The functional bowel disorders include: a) irritable bowel syndrome, which is the most common and most extensively studied functional disorder; b) functional abdominal bloating referring to abdominal fullness, bloating or distension unrelated to obvious maldigestion (e.g., lactose intolerance) or excess consumption of poorly digestible but fermentable food stuffs (e.g., sorbitol, beans, wheat bran), in the absence of functional dyspepsia or IBS; c) functional constipation, defined as straining at defecation, a sensation of incomplete evacuation, and the infrequent (two or fewer) passage of lumpy or hard stools in the absence of IBS; and d) functional diarrhea; referring to the frequent (more than three/day) and painless passage of unformed stools associated with a slight increase in stool volume (<500 g/day). Functional abdominal pain is frequently recurrent or continuous pain not associated with physiological events (eating, defecation, menses) and loss of daily function in the absence of organic disease or other functional GI disorders. It is considered a separate category from the functional bowel disorders since there is no evidence for a disturbance of intestinal motility, which typifies the functional bowel disorders. Thompson WG, Longstreth GF, Drossman DA, et. al. C. Functional Bowel Disorders and D. Functional Abdominal Pain. In: Drossman, D. A., Talley, N. J., Thompson, W. G., Whitehead, W. E., and Corazziari, E. Rome II: Functional Gastrointestinal Disorders: Diagnosis, Pathophysiology, and Treatment,2 ed. McLean, VA: Degnon Associates, Inc., 2000: Thompson WG, Longstreth GF, Drossman DA, et. al. Functional Bowel Disorders and Functional Abdominal Pain. Gut 1999; 45:II43-II")
12
Estrés afecta función GI
SII - Fisiología Estrés afecta función GI SNC / SNE Reactividad autonómica Dolor Sensibilidad Contracciones simultáneas Hipersensibilidad visceral SII Post-infeccioso Comidas Dolor / Motilidad 1970 1950 1960 1980 1990 2000 Mecanismos Interacción Cerebro-intestino Motilidad Marcadores mioeléctricos Inflamación Hipersens. visceral

13
1. Alteraciones de motilidad

14
SII - Fisiología Motilidad sigmoidea Minutos Comida SII Normal 2000
1500 1000 Comida Motilidad sigmoidea SII 500 Normal 50 100 130 Minutos Rogers J, Gut 1989;30:634

15
Tono rectal postprandial Hipersensib. rectal Respuesta gastrocólica
SII Fisiopatología Diarrea Estreñimiento Contracciones segm. no propulsivas Contracc. propulsivas Tono rectal postprandial Hipersensib. rectal Respuesta gastrocólica Slide Physiological Correlations of Diarrhea and Constipation Summary of changes in colorectal motor functions in patients with diarrhea- and constipation-predominant irritable bowel syndrome. In general, diarrhea is associated with an increase in propulsive contractions, tone and sensitivity; whereas, constipation is associated with reduced propulsive contractions, tonic response to the meal and a variable effect on rectal sensitivity. Camilleri, Gastroenterology 2001; 120:652 Camilleri, Gastroenterology 2001; 120:652

16
2. Alteraciones de la sensibilidad

17
Balón rectosigma. Volumen (ml)
SII - Fisiología 60 SII 40 % Dolor Normal 20 20 60 100 140 180 Balón rectosigma. Volumen (ml) Whitehead et al., Gastroenterology 1990;98:1187
 Whitehead et al., Gastroenterology 1990;98:1187.")
18
Hipersensibilidad visceral
SII - Hipersensibilidad Sensibilidad del órgano SNC Modulación inflamación mucosa Distensión mecánica Cortex Vias Cerebrales Hipersensibilidad visceral Hiperalgesia Alodinia Hiperexitabilidad Medular Sensibilización SII Post-infeccioso ON activación otros Neuropatía 847

19
Alteración en la sensibilidad visceral
SII Alteración en la sensibilidad visceral Estímulos anormales Estimulos repetitivos sobre el intestinol Inflamación aguda Infección ? otros Traumatismo neurológico Operaciones Procedimientos Invasivos Influences on Visceral Sensitization It is now recognized both from animal models and clinical studies that various types of stimuli to the bowel can lead to visceral sensitization. From a clinical perspective, it is therefore possible that sensitization may result from: a) abnormal visceral inputs, for example from chronically increased bowel stimulation or motility, b) acute inflammation related to infection or possibly inflammatory bowel disease and other intestinal inflammatory conditions, or c) neurological trauma related to surgical procedures or invasive procedures including endoscopy. Zighelboim J, Talley NJ, Phillips SF, et. al. Visceral perception in irritable bowel syndrome. Rectal and gastric responses to distension and serotonin type 3 antagonism. Digestive Diseases & Sciences 1995; 40: Drossman DA, et al. Gastroenterology, 2002; in press. Zighelboim J, Dig Dis & Sci 1995; 40:819 Drossman DA et. al., Gastroenterology 2002
 abnormal visceral inputs, for example from chronically increased bowel stimulation or motility, b) acute inflammation related to infection or possibly inflammatory bowel disease and other intestinal inflammatory conditions, or c) neurological trauma related to surgical procedures or invasive procedures including endoscopy. Zighelboim J, Talley NJ, Phillips SF, et. al. Visceral perception in irritable bowel syndrome. Rectal and gastric responses to distension and serotonin type 3 antagonism. Digestive Diseases & Sciences 1995; 40: Drossman DA, et al. Gastroenterology, 2002; in press. Zighelboim J, Dig Dis & Sci 1995; 40:819. Drossman DA et. al., Gastroenterology")
20
Sensibilidad Mecánica aferente EstimulaciónRepetida
SII - Sensibilizacón Sensorial Sensibilidad Mecánica aferente Circuitos medulares sensibilizados CENTRAL SENSORY SENSITIZATION Repeated inflation of a balloon to noxious levels in the recto-sigmoid region leads to lowered perception thresholds for discomfort and pain in IBS patients and possibly in healthy subjects. This phenomenon may be due to centrally mediated hyperalgesia. Centrally mediated hyperalgesia reflects hyperexcitability of second order sensory (spinal or supraspinal) neurons in the dorsal horn of the spinal cord. Under conditions of severe and persistent nociceptive stimulation, small diameter, non-myelinated C fibers fire repetitively and their input progressively increases responses of second order dorsal horn neurons. “Wind-up” of the second order neurons is generated by the release of the neurotransmitter glutamate from the C fibers. Noxious stimulation of the type applied in balloon distension studies in IBS patients can produce long-term changes in the excitability of dorsal horn neurons. This phenomenon is called central sensitization to distinguish it from the sensitization that occurs at the endings of the sensory neurons in the intestinal wall during release of inflammatory mediators. Long-term changes in the excitability of dorsal horn neurons imparts a memory for nociceptive input from C fibers. Peripheral noxious stimulation of C fibers from the skin is known to evoke the induction of early genes that encode transcription factors such as c-fos in dorsal horn neurons. Central sensitization of the spinal dorsal horn neurons is related to post-synaptic activation of NMDA receptors. Basbaum AI, Jessell TM. The perception of pain. In: Principles of science 4th ed. Kandel ER, Schwartz JH, Jessell TM (eds.) New York: McGraw-Hill 2000: Munakata J, Naliboff B, Harraf F, Kodner A, Lembo T, Chang L, Silverman DHS, Mayer EA. Repetitive sigmoid stimulation induces rectal hyperalgesia in patients with irritable bowel syndrome. Gastroenterology 1997;112:55-63. Raiz de ganglio dorsal EstimulaciónRepetida
 neurons in the dorsal horn of the spinal cord. Under conditions of severe and persistent nociceptive stimulation, small diameter, non-myelinated C fibers fire repetitively and their input progressively increases responses of second order dorsal horn neurons. Wind-up of the second order neurons is generated by the release of the neurotransmitter glutamate from the C fibers. Noxious stimulation of the type applied in balloon distension studies in IBS patients can produce long-term changes in the excitability of dorsal horn neurons. This phenomenon is called central sensitization to distinguish it from the sensitization that occurs at the endings of the sensory neurons in the intestinal wall during release of inflammatory mediators. Long-term changes in the excitability of dorsal horn neurons imparts a memory for nociceptive input from C fibers. Peripheral noxious stimulation of C fibers from the skin is known to evoke the induction of early genes that encode transcription factors such as c-fos in dorsal horn neurons. Central sensitization of the spinal dorsal horn neurons is related to post-synaptic activation of NMDA receptors. Basbaum AI, Jessell TM. The perception of pain. In: Principles of science 4th ed. Kandel ER, Schwartz JH, Jessell TM (eds.) New York: McGraw-Hill 2000: Munakata J, Naliboff B, Harraf F, Kodner A, Lembo T, Chang L, Silverman DHS, Mayer EA. Repetitive sigmoid stimulation induces rectal hyperalgesia in patients with irritable bowel syndrome. Gastroenterology 1997;112: Raiz de ganglio dorsal. EstimulaciónRepetida.")
21
La hipersensibilidad dolorosa tiene 2 propiedades:
ALODINIA E HIPERALGESIA La hipersensibilidad dolorosa tiene 2 propiedades: 1º Puede manifestarse como: - Alodinia: un estimulo que normalmente no es doloroso, puede provocar dolor - Hiperalgesia: donde un estimulo doloroso previo induce una respuesta dolorosa exagerada. 2º Se presenta: - no solo en el tejido agredido: alodinia/hiperalgesia 1ª - sino que puede darse en tejidos sanos próximos: alodinia/hiperalgesia 2ª

22
Intensidad del estímulo
SII - Sensibilización Hiperalgesia Sensación Dolor Agresión SENSITIZATION After an injury to superficial tissues (e.g., skin) the site of injury becomes hypersensitive and painful sensations are produced by relatively minor stimuli such as touch, heat and innocuous pin pricks that do not normally produce pain (i.e., allodynia). This phenomenon is called primary hyperalgesia. Increased sensitivity and allodynia are experienced also in areas surrounding the site of injury where no tissue damage has occurred. This phenomenon is called secondary hyperalgesia. Primary hyperalgesia is due to inflammatory substances released at the site of injury that increase the sensitivity of nociceptive primary sensory afferents. Secondary hyperalgesia is attributed to changes in the dorsal horn of the spinal cord. A central origin for secondary hyperalgesia is suggested by experimental findings showing no changes in sensitivity of the receptors in the zone of secondary hyperalgesia in terms of impulse firing in response to stimuli. On the other hand, stimulation of the receptors evokes painful sensations. This implies that application of the same stimulus within the zone of secondary hyperalgesia evokes more ascending impulses in the spinothalamic tracts than occurred when the region was stimulated prior to injury. The neurophysiologic mechanism for secondary hyperalgesia appears not to reside in the periphery, but rather within the synaptic connections between nociceptive afferents and the spinothalamic tracts. Basbaum AI, Jessell TM. The perception of pain. In: Principles of science 4th ed. Kandel ER, Schwartz JH, Jessell TM (eds.) New York: McGraw-Hill 2000: Alodinia Normal Inocuo Nocivo Intensidad del estímulo
 the site of injury becomes hypersensitive and painful sensations are produced by relatively minor stimuli such as touch, heat and innocuous pin pricks that do not normally produce pain (i.e., allodynia). This phenomenon is called primary hyperalgesia. Increased sensitivity and allodynia are experienced also in areas surrounding the site of injury where no tissue damage has occurred. This phenomenon is called secondary hyperalgesia. Primary hyperalgesia is due to inflammatory substances released at the site of injury that increase the sensitivity of nociceptive primary sensory afferents. Secondary hyperalgesia is attributed to changes in the dorsal horn of the spinal cord. A central origin for secondary hyperalgesia is suggested by experimental findings showing no changes in sensitivity of the receptors in the zone of secondary hyperalgesia in terms of impulse firing in response to stimuli. On the other hand, stimulation of the receptors evokes painful sensations. This implies that application of the same stimulus within the zone of secondary hyperalgesia evokes more ascending impulses in the spinothalamic tracts than occurred when the region was stimulated prior to injury. The neurophysiologic mechanism for secondary hyperalgesia appears not to reside in the periphery, but rather within the synaptic connections between nociceptive afferents and the spinothalamic tracts. Basbaum AI, Jessell TM. The perception of pain. In: Principles of science 4th ed. Kandel ER, Schwartz JH, Jessell TM (eds.) New York: McGraw-Hill 2000: Alodinia. Normal. Inocuo. Nocivo. Intensidad del estímulo.")
23
4. Post infección

24
Sindrome del intestino irritable postinfeccioso
Fisiopatología. 1. Inflamación de la mucosa gastrointestinal 2. Alteración de la permeabilidad mucosa 3. Alteración de la flora colónica 4. Alteración motora 5. Hipersensibilidad visceral Factores predisponentes. 1. Factores dependientes del agente etiológico 2. Factores dependientes del huésped

25
Sintomas intestinales: 4 Meses Post-infeccion
SII-PI Sintomas intestinales: 4 Meses Post-infeccion 100 SII-PI (n=28) Controles (curados, n=28) 80 Controles sanos (n=34) 60 % 40 20 Pérdidas Urgencia >3 BM/wk Esfuerzo Heces duras Gases Dunlop et al, Gastroenterology 2003;125:1651
 Controles (curados, n=28) 80. Controles sanos (n=34) 60. % Pérdidas. Urgencia. >3 BM/wk. Esfuerzo. Heces duras. Gases. Dunlop et al, Gastroenterology 2003;125:1651.")
26
Prevalencia de Dispepsia y SII Post-Infeccion
Epidemiología SII Prevalencia de Dispepsia y SII Post-Infeccion 3 meses 12 meses 6 meses 4 8 12 16 20 Dispepsia % Pre infeccion SII Post-infección Control Mearin, et al,. Gastroenterology 2005; 129:98

27
Scores psicológicos: 4 Meses Post Infección Limitaciones de actividad
SII-PI Scores psicológicos: 4 Meses Post Infección 25 SII-PI (n=28) Controls (curados, n=28) Controles sanos (n=34) P=0.001 P=0.001 20 15 P=0.001 P=0.01 Score P=0.001 P=0.02 P=0.001 10 P=0.001 5 HAD Ansiedad HAD Depresión QOL Función emocional QOL Limitaciones de actividad Dunlop et al, Gastroenterology 2003;125:1651
 Controls (curados, n=28) Controles sanos (n=34) P= P= P= P=0.01. Score. P= P=0.02. P= P= HAD. Ansiedad. HAD. Depresión. QOL. Función emocional. QOL. Limitaciones de actividad. Dunlop et al, Gastroenterology 2003;125:1651.")
28
Síntomas SII SII Post-infeccioso - Interaccón Cerebro-Intestino
Distres Psicológico Inflamación mucosa Síntomas SII Desencadenante Infección aguda Sensibilidad visceral Slide 1125: Post-infectious IBS – Brain-Gut Interaction Diagram This slide provides a conceptual model to explain the possible relationship between IBS symptoms with psychological distress, mucosal inflammation, dysmotility and visceral hypersensitivity. An acute infection may trigger mucosal inflammation, dysmotility and secretion. Inflammation may also contribute to intestinal dysmotility and secretion. These two factors may then lead to visceral hypersensitivity, which in turn, may produce IBS symptoms. It is noted, however that such gut disturbances do not always lead to symptoms (broken line). In fact, most subjects in the Gwee et al. study did not have symptoms, even though they had intestinal hypersensitivity and dysmotility. Thus, it is likely that high levels of psychological distress may, through central mechanisms, enable the clinical expression of IBS symptoms by amplifying incoming visceral signals. This may occur directly via increased central perception or via its effects on gut inflammation dysmotility, secretion and visceral hypersensitivity. Drossman DA. Mind over matter in the postinfective irritable bowel. Gut 1999; 44: Gwee KA, Leong YL, Graham C, et. al. The role of psychological and biological factors in post- infective gut dysfunction. Gut 1999; 44: Alteración en motilidad secreción Drossman, Gut 1999; 44:306 Gwee et. al., Gut 1999; 44:400
. In fact, most subjects in the Gwee et al. study did not have symptoms, even though they had intestinal hypersensitivity and dysmotility. Thus, it is likely that high levels of psychological distress may, through central mechanisms, enable the clinical expression of IBS symptoms by amplifying incoming visceral signals. This may occur directly via increased central perception or via its effects on gut inflammation dysmotility, secretion and visceral hypersensitivity. Drossman DA. Mind over matter in the postinfective irritable bowel. Gut 1999; 44: Gwee KA, Leong YL, Graham C, et. al. The role of psychological and biological factors in post- infective gut dysfunction. Gut 1999; 44: Alteración en. motilidad. secreción. Drossman, Gut 1999; 44:306. Gwee et. al., Gut 1999; 44:400.")
29
Criterios Rome III– Sindrome Intestino Irritable
Dolor abdominal recurrent or disconfort por lo menos 3 días /mes en los últimos 3 meses asociado con 2 ó más : Mejoría con la defecación Comienzo asociado con cambios en la frecuencia Comianzo asociado a cambios en la forma de las heces y y Longstreth G., Gastroenterology 2006

30
Evaluación Diagnóstica Rome III
SII - Diagnóstico Evaluación Diagnóstica Rome III Examen heces Sangre oculta Leucocitos Parásitos Sigmoidoscopia o Colonoscopia (>50 años) Examen Físico Hemograma Test aliento lactulosa Est. funcionales Otros estudios si se estima que son necesarios
 Examen Físico. Hemograma. Test aliento lactulosa. Est. funcionales. Otros estudios si se estima que son necesarios.")
31
Tratamiento

32
Tasa de respuesta a placebo
SII - Tratamiento Tasa de respuesta a placebo Autor Fármaco Respuesta placebo (%) p<.05 Piai ‘81 Prifinium 33 yes Milo ‘80 Domperidona (Motilium) 34 yes Page ‘81 Diciclomina (Colchimax) 54 yes Heefner ‘78 Desipramina 60 + Myren ‘82 Trimiprimine 67 no Longs ‘81 Metamucil 71 no Fielding ‘81 Timolol 73 no Fielding ‘80 Trimebutine (Polibutin) 88 no
 p<.05. Piai ‘81. Prifinium. 33. yes. Milo ‘80. Domperidona (Motilium) 34. yes. Page ‘81. Diciclomina (Colchimax) 54. yes. Heefner ‘78. Desipramina Myren ‘82. Trimiprimine. 67. no. Longs ‘81. Metamucil. 71. no. Fielding ‘81. Timolol. 73. no. Fielding ‘80. Trimebutine (Polibutin) 88. no.")
33
Sindrome del intestino irritable Tratamiento
Abordaje individualizado Predominio estreñimiento Predominio diarrea Dolor abdominal - Increm. de bolo - Medidas dietéticas - Laxantes - Espasmolíticos - Loperamida - Espasmolíticos - Antidepresivos Manejo de los factores estresantes asociados Antidepresivos Explicar correctamente al paciente su enfermedad

34
Esquema Severo Moderado Leve Todos SII - Tratamiento Metas realistas
Antidepresivos Tratamiento del dolor Severo Moderado Fármacos sobre la (motilidad/sensibilidad) Tratamiento Psicológico Leve Modificación de dieta y estilo de vida Buena relación / Tratamiento continuado Educación / Revaloración Todos 667
 Tratamiento. Psicológico. Leve. Modificación de dieta y estilo de vida. Buena relación / Tratamiento continuado. Educación / Revaloración. Todos")
36
y después...

38
- Colon irritable desde hace 15 años
- Tengo gases en la barriga que me comprimen el pecho - Me parece que tengo una depresión senil por que estoy disgustado y tengo malestar abdominal, - Desde hace 3m a raiz de problemas famimliares tengo molestias abdominales que alivian al defecar y expulsar gases REEVALUACION CONTINUA DEL PACIENTE FUNCIONAL

Presentaciones similares




















>")

