Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Sepsis y Falla Organica Multiple
Jairo Alarcón, MD. Pediatra Intensivista. Universidad del Valle Hospital Universitario del Valle Cali, Colombia

2
Sepsis y Falla Organica Multiple
Objetivos de la charla: Conocer Conceptos tradicionales Aproximación a la fisiopatología. Generalidades del cuadro clínico Perspectivas terapéuticas.

3
Sepsis y Falla Organica Multiple Epidemiologia
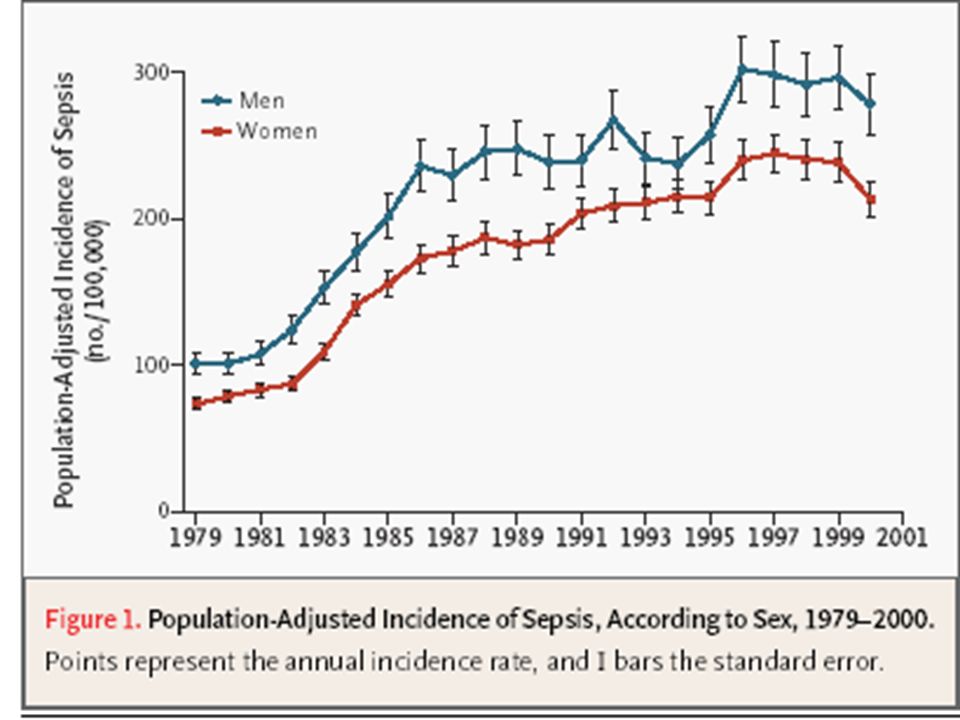
Una de las Principales Causa de Morbi-Mortalidad en todo el mundo. Constituye la treceava ( 13) causa de muerte. La novena causa de muerte en el grupo de cuatro años de edad. Mas de 750,000 casos/año de sepsis severa en USA. Hoy mueren en el mundo mas de 1500 pacientes de sepsis severa diariamente Es la principal causa de muerte en UCI Sepsis is a major worldwide cause of morbidity and mortality. Sands et al described the epidemiology of sepsis in 8 academic medical centers in the United States. They reported that sepsis is the leading cause of death in patients admitted to noncoronary intensive care units. The National Vital Statistics Report indicated that sepsis is the 11th leading cause of death in the United States, based on data for septicemia. Angus et al studied the age-specific incidence and outcomes of sepsis in the United States. Their investigation indicates that there are more than 750,000 cases of severe sepsis (sepsis with organ dysfunction) each year in the United States. Based on data from Angus et al, more than 500 Americans die of severe sepsis daily. Angus DC, Linde-Zwirble WT, Lidicker J, et al. Incidence, cost, outcome of severe sepsis in the United States. Crit Care Med (In Press). Murphy SL. Deaths: final data for National Vital Statistics Reports Web site. Available at: Sands KE, Bates DW, Lanken PN, et al. Epidemiology of sepsis syndrome in 8 academic medical centers. JAMA. 1997;278:
 causa de muerte. La novena causa de muerte en el grupo de cuatro años de edad. Mas de 750,000 casos/año de sepsis severa en USA. Hoy mueren en el mundo mas de 1500 pacientes de sepsis severa diariamente. Es la principal causa de muerte en UCI. Sepsis is a major worldwide cause of morbidity and mortality. Sands et al described the epidemiology of sepsis in 8 academic medical centers in the United States. They reported that sepsis is the leading cause of death in patients admitted to noncoronary intensive care units. The National Vital Statistics Report indicated that sepsis is the 11th leading cause of death in the United States, based on data for septicemia. Angus et al studied the age-specific incidence and outcomes of sepsis in the United States. Their investigation indicates that there are more than 750,000 cases of severe sepsis (sepsis with organ dysfunction) each year in the United States. Based on data from Angus et al, more than 500 Americans die of severe sepsis daily. Angus DC, Linde-Zwirble WT, Lidicker J, et al. Incidence, cost, outcome of severe sepsis in the United States. Crit Care Med (In Press). Murphy SL. Deaths: final data for National Vital Statistics Reports Web site. Available at: Sands KE, Bates DW, Lanken PN, et al. Epidemiology of sepsis syndrome in 8 academic medical centers. JAMA. 1997;278:")
4
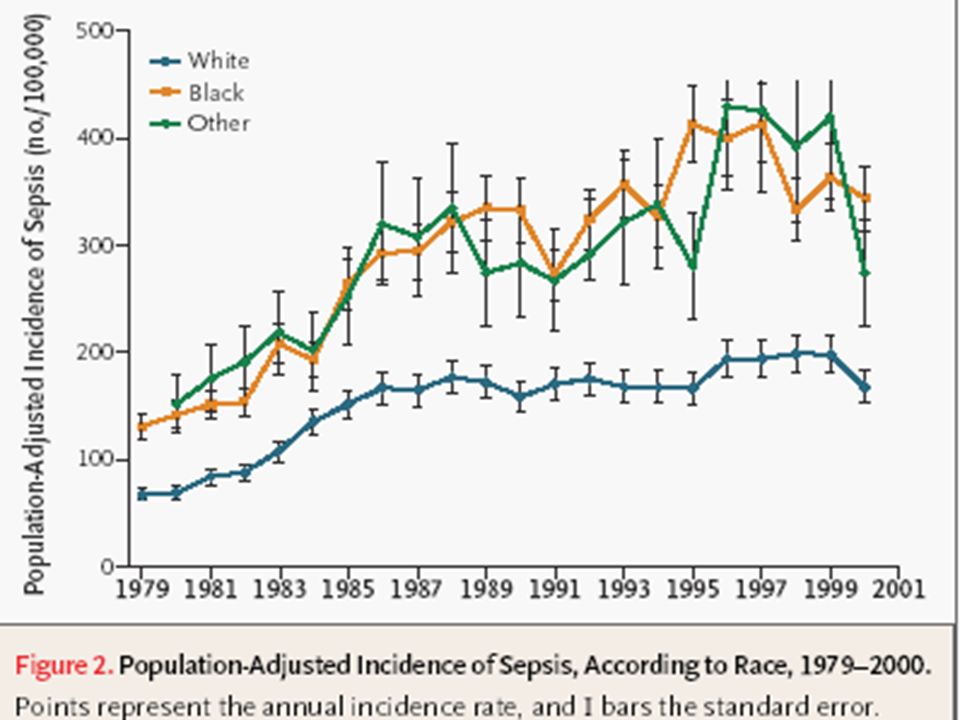
Greg Martin, David mennino,et al.

9
Sepsis y Falla Organica Multiple
Una historia de descubrimientos y Logros

10
Sepsis atraves del tiempo:
Historia de Descubrimientos c. 100 BC “small creatures invisible to the eye, fill the atmosphere, and breathed through the nose cause dangerous diseases.” – Marcus Terentius Varro, De re rustica libri III Marcus Terentius Varro, in De re rustica libri III (three books on agriculture), was the first to articulate the notion of contagion. References Lagassé P, ed. The Columbia Encyclopedia. 6th ed. New York, NY: Columbia University Press; 2000. Wilson RF. A brief introduction to sepsis: its importance and some historical notes. Heart Lung ;5:393–396.
, was the first to articulate the notion of contagion. References. Lagassé P, ed. The Columbia Encyclopedia. 6th ed. New York, NY: Columbia University Press; Wilson RF. A brief introduction to sepsis: its importance and some historical notes. Heart Lung. 1976;5:393–396.")
11
Sepsis y Falla Organica Multiple 1864 - 1879
French chemist Louis Pasteur put forth the “germ theory” of disease in a lecture before the French Academy. Louis Pasteur announced to the French Academy that Streptococcus causes puerperal sepsis. References Broad W, Wade N. Betrayers of the Truth: Fraud and Deceit in the Halls of Science. New York, NY: Simon & Schuster Inc; 1982. Classic pages in obstetrics and gynecology: Louis Pasteur. Septicémie puerpérale. Am J Obstet Gynecol ;118:282.

12
Definiciones-Consenso ACCP/SCCM
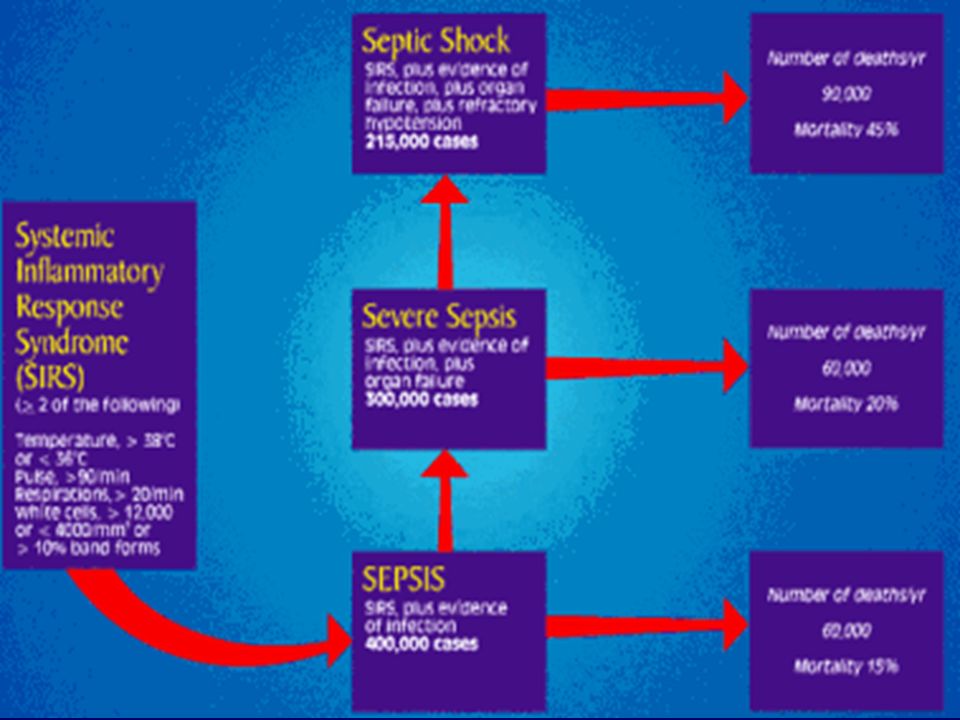
Sepsis Severa Sepsis Disfuncion de organos Shock Septico Hipotension a pesar de resuscitacion con liquidos Sindrome de Disfuncion Multiple de Organos(FDOM) Funcion alterada de organos en un paciente agudamente enfermo Homeostasis no se puede mantener sin soporte. Infeccion Respta inflamatoria a microorganismos,o Invasion de tejidos normalmente esteriles Sindrome de Respuesta inflamatoria sistemica(SIRS) Respuesta sistemica auna amplia variedad de procesos. Sepsis Infeccion mas 2 criterios de SIRS criteria The American College of Chest Physicians (ACCP) and Society of Critical Care Medicine (SCCM) held a consensus conference in August 1991 to agree on a set of definitions that could be applied to patients with sepsis and organ dysfunction. The consensus panel also recommended the use of severity scoring methods to characterize the disease and develop a comprehensive model for the syndrome. This slide provides a brief definition of the various components of the sepsis syndrome. Notably, this is a non-linear process rather than a continuum and the presence of organ dysfunction identifies a population with a significant risk of mortality. Bone RC, Balk RA, Cerra FB, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Chest. 1992;101:
 Funcion alterada de organos en un paciente agudamente enfermo. Homeostasis no se puede mantener sin soporte. Infeccion. Respta inflamatoria a microorganismos,o. Invasion de tejidos normalmente esteriles. Sindrome de Respuesta inflamatoria sistemica(SIRS) Respuesta sistemica auna amplia variedad de procesos. Sepsis. Infeccion mas. 2 criterios de SIRS criteria. The American College of Chest Physicians (ACCP) and Society of Critical Care Medicine (SCCM) held a consensus conference in August 1991 to agree on a set of definitions that could be applied to patients with sepsis and organ dysfunction. The consensus panel also recommended the use of severity scoring methods to characterize the disease and develop a comprehensive model for the syndrome. This slide provides a brief definition of the various components of the sepsis syndrome. Notably, this is a non-linear process rather than a continuum and the presence of organ dysfunction identifies a population with a significant risk of mortality. Bone RC, Balk RA, Cerra FB, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Chest. 1992;101:")
13
SIRS: Mas que solo una respuesta inflamatoria sistemica
Respuesta clinica producto de un insulto no especifico, manifestada por 2 de las siguientes hallazgos: Temperatura 38°C or 36°C FC 90 Lats/min FR 20/min Leucograma 12,000/mL o 4,000/mL o >10% inmaduros The systemic inflammatory response syndrome (SIRS) is a clinical response arising from a nonspecific insult manifested by two or more of the following: Fever or hypothermia Tachycardia Tachypnea Leukocytosis, leukopenia, or a left-shift (increase in immature neutrophilic leukocytes in the blood) Recent evidence indicates that hemostatic changes play a significant role in many SIRS-linked disorders. Bone RC, Balk RA, Cerra FB, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Chest. 1992;101: Opal SM, Thijs L, Cavaillon JM, et al. Relationships between coagulation and inflammatory processes. Crit Care Med. 2000; 28:S81-2. Reciente evidencia indica que existen alteraciones hemostaticas tambien estaninvolucradas. Conllevan a un efecto deletéreo sobre el endotelio y contractibilidad vascular Adapted from: Bone RC et al. Chest. 1992;101: Opal SM et al. Crit Care Med. 2000;28:S81-2.
 is a clinical response arising from a nonspecific insult manifested by two or more of the following: Fever or hypothermia. Tachycardia. Tachypnea. Leukocytosis, leukopenia, or a left-shift (increase in immature neutrophilic leukocytes in the blood) Recent evidence indicates that hemostatic changes play a significant role in many SIRS-linked disorders. Bone RC, Balk RA, Cerra FB, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Chest. 1992;101: Opal SM, Thijs L, Cavaillon JM, et al. Relationships between coagulation and inflammatory processes. Crit Care Med. 2000; 28:S81-2. Reciente evidencia indica que existen. alteraciones hemostaticas tambien estaninvolucradas. Conllevan a un efecto deletéreo sobre el. endotelio y contractibilidad vascular. Adapted from: Bone RC et al. Chest. 1992;101: Opal SM et al. Crit Care Med. 2000;28:S81-2.")
14
Sepsis: Mas que solo una inflamación
Infeccion conocida o Sospechada mas .... 2 o mas criterios de SIRS. Un significativo vinculo a un desorden de la hemostasis The original ACCP/SCCM criteria for the diagnosis of sepsis required the presence of known or suspected infection plus two or more SIRS criteria. Climbing a flight of stairs can produce two SIRS criteria (tachypnea, tachycardia) in a normal sedentary individual. Thus, clinical studies of sepsis generally require at least three SIRS criteria plus known or suspected infection for entry. Bone RC, Balk RA, Cerra FB, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Chest. 1992;101: Adapted from: Bone RC et al. Chest. 1992;101:
 in a normal sedentary individual. Thus, clinical studies of sepsis generally require at least three SIRS criteria plus known or suspected infection for entry. Bone RC, Balk RA, Cerra FB, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Chest. 1992;101: Adapted from: Bone RC et al. Chest. 1992;101:")
15
Severe Sepsis Definida como sepsis asociada a disfunción orgánica con
hipo perfusión de órganos y/o hipotensión Se define hipo perfusión cuando Acidosis láctica: Lactato venoso>20mg/dl) oliguria(<0.5cc/k/hora) llenado capilar>3seg alteración del estado mental hipotensión. Severe sepsis is sepsis plus signs and symptoms of acute organ dysfunction, hypoperfusion, or hypotension. Hypoperfusion and perfusion abnormalities may include, but are not limited to, lactic acidosis, oliguria, or an acute alteration in mental status. As shown on the next slide, organ dysfunction may involve any of the following alone or in combination: Cardiovascular system Kidney Respiratory system Liver Hematologic (blood, coagulation) Central nervous system Presence of an otherwise unexplained metabolic acidosis Bone RC, Balk RA, Cerra FB, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Chest. 1992;101: Adapted from: Bone RC et al. Chest. 1992;101:
 oliguria(<0.5cc/k/hora) llenado capilar>3seg. alteración del estado mental hipotensión. Severe sepsis is sepsis plus signs and symptoms of acute organ dysfunction, hypoperfusion, or hypotension. Hypoperfusion and perfusion abnormalities may include, but are not limited to, lactic acidosis, oliguria, or an acute alteration in mental status. As shown on the next slide, organ dysfunction may involve any of the following alone or in combination: Cardiovascular system. Kidney. Respiratory system. Liver. Hematologic (blood, coagulation) Central nervous system. Presence of an otherwise unexplained metabolic acidosis. Bone RC, Balk RA, Cerra FB, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Chest. 1992;101: Adapted from: Bone RC et al. Chest. 1992;101:")
16
Sepsis y Falla Organica Multiple
This conceptual framework shows the interrelationships between infection, non-infectious disorders, SIRS, sepsis, and severe sepsis. Components of the process not discussed on the following slides include: Infection: a microbial phenomenon characterized by an inflammatory response to the presence of microorganisms or the invasion of normally sterile host tissue by those organisms Bacteremia: the presence of viable bacteria in the blood stream Septic shock: sepsis-induced hypotension despite adequate fluid resuscitation along with the presence of perfusion abnormalities that may include, but are not limited to, lactic acidosis, oliguria, or an acute alteration in mental status Multiple organ dysfunction syndrome (MODS): presence of altered organ function in an acutely ill patient such that homeostasis cannot be maintained without intervention Inflammation and hemostasis are tightly linked. Therefore, although not shown on this slide, sepsis and severe sepsis lie on a background of disturbed hemostasis. Bone RC, Balk RA, Cerra FB, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Chest. 1992;101: Opal SM, Thijs L, Cavaillon JM, et al. Relationships between coagulation and inflammatory processes. Crit Care Med. 2000;28:S81-2. Adapted from: Bone RC et al. Chest. 1992;101: Opal SM et al. Crit Care Med. 2000;28:S81-2.
: presence of altered organ function in an acutely ill patient such that homeostasis cannot be maintained without intervention. Inflammation and hemostasis are tightly linked. Therefore, although not shown on this slide, sepsis and severe sepsis lie on a background of disturbed hemostasis. Bone RC, Balk RA, Cerra FB, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Chest. 1992;101: Opal SM, Thijs L, Cavaillon JM, et al. Relationships between coagulation and inflammatory processes. Crit Care Med. 2000;28:S81-2. Adapted from: Bone RC et al. Chest. 1992;101: Opal SM et al. Crit Care Med. 2000;28:S81-2.")
17
Sepsis y Disfunción Organica Multiple
Estado final disfunción fisiológica progresiva en dos o más sistemas: Cardiovascular. Respiratorio Gastrointestinal Renal Neurológico Hematológico Hepático DOM Severe sepsis is sepsis plus signs and symptoms of acute organ dysfunction, hypoperfusion, or hypotension. Hypoperfusion and perfusion abnormalities may include, but are not limited to, lactic acidosis, oliguria, or an acute alteration in mental status. As shown on the next slide, organ dysfunction may involve any of the following alone or in combination: Cardiovascular system Kidney Respiratory system Liver Hematologic (blood, coagulation) Central nervous system Presence of an otherwise unexplained metabolic acidosis Bone RC, Balk RA, Cerra FB, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Chest. 1992;101: Adapted from: Bone RC et al. Chest. 1992;101:
 Central nervous system. Presence of an otherwise unexplained metabolic acidosis. Bone RC, Balk RA, Cerra FB, et al. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Chest. 1992;101: Adapted from: Bone RC et al. Chest. 1992;101:")
18
Hugonnet, Crit Care Med, Volumen 31(2). February 2003.390-394
CPT-Based Classification of Acute Organ Dysfunction Associated with Sepsis(pic.htm) Hugonnet, Crit Care Med, Volumen 31(2). February
 Hugonnet, Crit Care Med, Volumen 31(2). February")
21
Sepsis: una Cascada de eventos
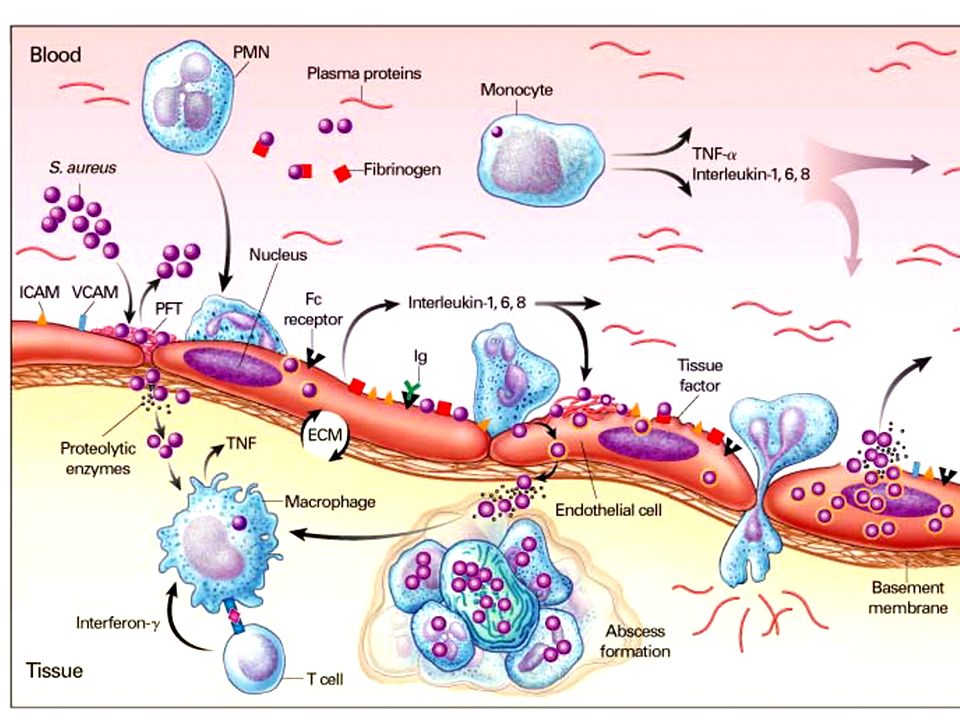
Mediadores Pro-inflamatorios INFLAMACION Activated Protein C T TM Mediadores Anti-Inflamatorios PAI-1 T-PA TAF-1 INFECCION INJURIA ENDOTELIAL TF Severe sepsis is associated with three integrated components: Infection with the systemic activation of inflammation. During progression of sepsis, a wide variety of proinflammatory cytokines is released. Endotoxin induces rapid increases in the levels of tumor necrosis factor (TNF), interleukin-1 (IL-1), and interleukin-6 (IL-6) in experimental models of sepsis. These proinflammatory cytokines are linked to the development of the clinical signs of sepsis. Release of proinflammatory cytokines is associated with endothelial injury and vascular bed-specific changes in the thrombogenicity of the endothelium.These can include increased tissue factor (TF) expression in a subset of endothelial cells and release of plasminogen activator inhibitor-1 (PAI-1). Activation of coagulation. Inflammatory changes trigger the extrinsic pathway of coagulation. Activation of coagulation in patients with sepsis is not always disseminated intravascular coagulation. Instead, in most patients, it is a subclinical activation of the hemostatic system as indicated by changes in commonly measured hemostatic parameters. Experimentally, there are increases in thrombin-antithrombin (TAT) complexes. Clinical laboratory findings include significant increases in D-dimer, a marker of coagulation and associated fibrinolysis. Impairment of fibrinolysis. In patients with sepsis, plasminogen levels fall rapidly while antiplasmin levels remain normal. This decreases the normal fibrinolytic response. Fibrinolysis is further impaired by release of PAI-1 and the generation of increased amounts of thrombin-activatable fibrinolysis inhibitor (TAFI). Although plasminogen/antiplasmin ratio and PAI-1 levels remain abnormal in nonsurviving patients, they tend to normalize in survivors. Kidokoro A, Iba T, Fukunaga M, et al. Alterations in coagulation and fibrinolysis during sepsis. Shock. 1996;5: Levi M, van der Poll T, ten Cate H, et al. The cytokine-mediated imbalance between coagulant and anticoagulant mechanisms in sepsis and endotoxaemia. Eur J Clin Invest. 1997;27:3-9. Lorente JA, Garcia-Frade LJ, Landin L, et al. Time course of hemostatic abnormalities in sepsis and its relation to outcome. Chest. 1993;103: van Deventer SJH, Buller HR, ten Cate JW, et al. Experimental endotoxemia in humans: analysis of cytokine release and coagulation, fibrinolytic, and complement pathways. Blood. 1990;76: Vervloet MG, Thijs LG, Hack CE. Derangements of coagulation and fibrinolysis in critically ill patients with sepsis and septic shock. Semin Thromb Hemost. 1998;24:33-44. COAGULACION Inhibidor fibrinolis is activable Inhibidor activador del plasminogeno FIBRINOLISIS
, interleukin-1 (IL-1), and interleukin-6 (IL-6) in experimental models of sepsis. These proinflammatory cytokines are linked to the development of the clinical signs of sepsis. Release of proinflammatory cytokines is associated with endothelial injury and vascular bed-specific changes in the thrombogenicity of the endothelium.These can include increased tissue factor (TF) expression in a subset of endothelial cells and release of plasminogen activator inhibitor-1 (PAI-1). Activation of coagulation. Inflammatory changes trigger the extrinsic pathway of coagulation. Activation of coagulation in patients with sepsis is not always disseminated intravascular coagulation. Instead, in most patients, it is a subclinical activation of the hemostatic system as indicated by changes in commonly measured hemostatic parameters. Experimentally, there are increases in thrombin-antithrombin (TAT) complexes. Clinical laboratory findings include significant increases in D-dimer, a marker of coagulation and associated fibrinolysis. Impairment of fibrinolysis. In patients with sepsis, plasminogen levels fall rapidly while antiplasmin levels remain normal. This decreases the normal fibrinolytic response. Fibrinolysis is further impaired by release of PAI-1 and the generation of increased amounts of thrombin-activatable fibrinolysis inhibitor (TAFI). Although plasminogen/antiplasmin ratio and PAI-1 levels remain abnormal in nonsurviving patients, they tend to normalize in survivors. Kidokoro A, Iba T, Fukunaga M, et al. Alterations in coagulation and fibrinolysis during sepsis. Shock. 1996;5: Levi M, van der Poll T, ten Cate H, et al. The cytokine-mediated imbalance between coagulant and anticoagulant mechanisms in sepsis and endotoxaemia. Eur J Clin Invest. 1997;27:3-9. Lorente JA, Garcia-Frade LJ, Landin L, et al. Time course of hemostatic abnormalities in sepsis and its relation to outcome. Chest. 1993;103: van Deventer SJH, Buller HR, ten Cate JW, et al. Experimental endotoxemia in humans: analysis of cytokine release and coagulation, fibrinolytic, and complement pathways. Blood. 1990;76: Vervloet MG, Thijs LG, Hack CE. Derangements of coagulation and fibrinolysis in critically ill patients with sepsis and septic shock. Semin Thromb Hemost. 1998;24: COAGULACION. Inhibidor fibrinolis. is activable. Inhibidor activador. del plasminogeno. FIBRINOLISIS.")
23
Sepsis y Falla Organica Multiple
Curso dinámico de la respuesta inflamatoria durante sepsis

24
Sepsis y Falla Organica Multiple
Proteína grupo B1 alta movilidad: HMGB1

25
Sepsis y Falla Organica Multiple
Factor inhibidor migración macrófagos: MIF

26
Sepsis y Disfunción Organica Multiple
1997 Roger Bone. CARS: “sindrome de respuesta antinflamatoria compensatoria”, es un fenómeno que busca proteger el organismo del insulto generado, por el sindrome de respuesta imflamatoria sisatémica. Se caracteriza por la producción de un grupo de citoquinas, que también pueden tener un efecto deletéreo MARS: “sindrome de respuesta antagonista mixta” Se define como un estadio intermedio entre SIRS y el CARS en donde ambas fuerzas se encuentran en equilibriopara regular la homeostasis

27
Concepto del espectro de la respuesta
Inmune en Sepsis Bansal: Curr Opin Clin Nutr Metab Care, Volume 6(2).March
.March")
29
Sepsis y Falla Organica Multiple
Rol en la Sepsis y el Complemento

30
Inflamacion Sistemica Fibrinolisis deficientesis
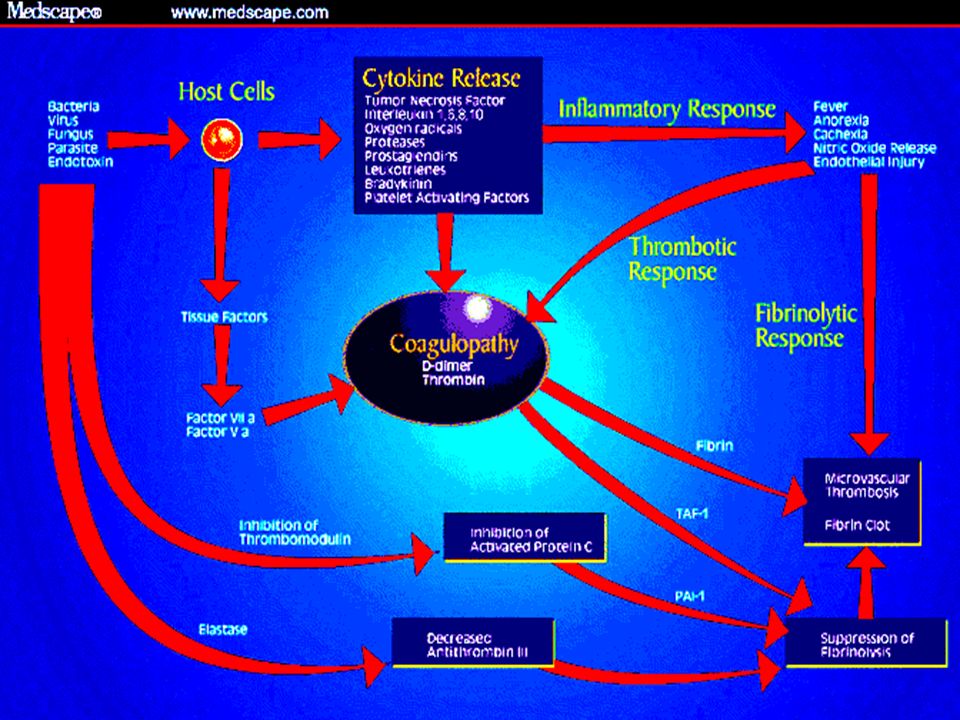
Sepsis y Falla Organica Multiple: Sindrome Clinico Complejo y no Predecible.... Alta Mortalidad 28%-50% Pacientes Heterogeneos Progresion de la enfermedad impredecible Etiologia y Patogenesis no clara Inflamacion Sistemica Coagulacion Severe sepsis is a complex and unpredictable clinical syndrome with mortality ranging from 28% to 50%. The mortality increases with the degree of organ dysfunction. Patients presenting with sepsis are a heterogeneous population varying in: Age Gender Infecting organism Comorbidities Genetic background Immune status, etc. Although the severity of sepsis is related to the degree of organ dysfunction, progression is often unpredictable. Although advances in molecular biology, immunology, and hemostasis have significantly contributed to our understanding of the nature of severe sepsis, there are many points that remain to be clarified concerning its etiology and pathogenesis. Severe sepsis can be thought of as a triad of systemic inflammation, coagulation, and impaired fibrinolysis. Angus DC, Linde-Zwirble WT, Lidicker J, et al. Incidence, cost, outcome of severe sepsis in the United States. Crit Care Med (In Press). Wheeler AP, Bernard GR. Treating patients with severe sepsis. N Engl J Med. 1999;340: Zeni F, Freeman B, Nathanson C. Anti-inflammatory therapies to treat sepsis and septic shock: a reassessment. Crit Care Med. 1997;25: Fibrinolisis deficientesis Angus DC et al. Crit Care Med. 2001; (In Press). Zeni F et al. Crit Care Med. 1997;25: Wheeler AP et al. N Engl J Med. 1999;340:
. Wheeler AP, Bernard GR. Treating patients with severe sepsis. N Engl J Med. 1999;340: Zeni F, Freeman B, Nathanson C. Anti-inflammatory therapies to treat sepsis and septic shock: a reassessment. Crit Care Med. 1997;25: Fibrinolisis deficientesis. Angus DC et al. Crit Care Med. 2001; (In Press). Zeni F et al. Crit Care Med. 1997;25: Wheeler AP et al. N Engl J Med. 1999;340:")
31
FACTORES GENETICOS DEL HOSPEDERO
Factores genéticos determinantes mayores de susceptibilidad muerte. Polimorfismo recptores de FNT – IL1- TLRs. Determina la [ ] de citoquinas inflamatorias y Antinflamatorias diferencian una respuesta a la infección.

32
(TLR) Expresados en las células inmunes.
Interacción entre productos bacterianos(lipopolysaccharide, peptidoglycan, lipoteichoic acid, flagellin) y receptores de reconocimiento(Toll-like receptors (TLR) Expresados en las células inmunes. Pic2.htm
 y receptores de reconocimiento(Toll-like receptors. (TLR) Expresados en las células inmunes. Pic2.htm.")
33
MANIFESTACIONES CLINICAS
Comprometen múltiples órganos y sistemas: Neurológico: “Encefalopatía Séptica”. Cardiovascular: Depresión del miocardio producto de la cascada inflamatoria. Respiratorio: SDRA. Gastrointestinal: disfunción hepática, ulceras de estrés.

34
MANIFESTACIONES CLINICAS
Renal: oliguria, hiperK, aumento de creatinina sérica. Hematológico: CID - trombosis microvas. Metabólico: Gasto energético aumentado, resistencia la insulina periférica. Oxigenación: disminución de la entrega de oxígeno y perdida de habilidad de los tejidos de extraer oxígeno.

35
TERAPIA EN SEPSIS Reconocimiento temprano sepsis clave para un tratamiento exitoso: - cambios en la esfera mental. - conteo de células blancas neutrofilos. - ↑ glicemia. La carencia de una fase de respuesta aguda se asocia con una alta mortalidad.

36
Alteraciones clinicas del paciente en shock septico
Irritabilidad Alteracion conciencia Somnolencia Coma Taquicardia Hipotension CVP PAOP Taquipnea PaO2 <70 mm Hg SaO2 <90% PaO2/FiO2 300 Oliguria Anuria Creatinina Following identification of a patient with sepsis, the clinician must assess the patient for the presence of acute organ dysfunction (severe sepsis). The presence of acute organ dysfunction is often recognized clinically by the patient’s presenting signs and symptoms. However, in some instances laboratory data or results of invasive monitoring will confirm the diagnosis of organ dysfunction. The illustration of the patient on this slide has arrows pointing to various organs that might provide clues to the presence of organ dysfunction. Indications of organ dysfunction include: Central nervous system: altered consciousness, confusion, psychosis, delirium Respiratory system: tachypnea, hypoxemia, oxygen saturation <90%, decreased ratio of arterial oxygen vs inspired oxygen Liver: jaundice, increased liver enzymes, hypoalbuminemia, increased prothrombin time Cardiovascular: tachycardia, hypotension, increased central venous pressure, increased pulmonary artery occlusive pressure Kidney: oliguria, anuria, increased creatinine Hematological: thrombocytopenia, abnormal coagulation tests, decreased levels of Protein C, increased D-dimers Ictericia Enzimas Albumina PT Plaquetas PT/APTT Protein C D-dimer
. The presence of acute organ dysfunction is often recognized clinically by the patient’s presenting signs and symptoms. However, in some instances laboratory data or results of invasive monitoring will confirm the diagnosis of organ dysfunction. The illustration of the patient on this slide has arrows pointing to various organs that might provide clues to the presence of organ dysfunction. Indications of organ dysfunction include: Central nervous system: altered consciousness, confusion, psychosis, delirium. Respiratory system: tachypnea, hypoxemia, oxygen saturation <90%, decreased ratio of arterial oxygen vs inspired oxygen. Liver: jaundice, increased liver enzymes, hypoalbuminemia, increased prothrombin time. Cardiovascular: tachycardia, hypotension, increased central venous pressure, increased pulmonary artery occlusive pressure. Kidney: oliguria, anuria, increased creatinine. Hematological: thrombocytopenia, abnormal coagulation tests, decreased levels of Protein C, increased D-dimers. Ictericia. Enzimas. Albumina. PT. Plaquetas. PT/APTT. Protein C. D-dimer.")
37
Terapia en Sepsis Severa Sepsis
Soporte Hemodinamico Control del Foco Antibioticos Ventilacion Mecanica Terapia de Reemplazo Sedacion -Analgesia Adecuada Nutricion Soporte Hematologico Otras medidas de soporte Avances. Standard care of the patient with severe sepsis consists of a number of medical (and sometimes surgical) interventions intended to normalize physiology and eliminate infection. These are divided into: Source control: This term refers to management of the source of the infection. It can consist of surgery to drain an abscess or removal of an infected catheter. Antibiotics: While the initial therapy may be broad-based and empiric, identification of the specific pathogen by microbiologic studies may result in a switch of the antibiotic to those that are the most specific and bacteriocidal. Hemodynamic support: This term refers to volume replenishment therapy followed, when necessary, by appropriate use of drugs such as norepinephrine to maintain blood pressure and organ perfusion. Mechanical ventilation: Respiratory failure is a common manifestation of pulmonary organ dysfunction in patients with severe sepsis. Mechanical ventilation is instituted to increase oxygenation and improve gas exchange. Renal replacement therapy: Impaired renal function is a sign of organ dysfunction in patients with severe sepsis. Renal replacement therapy consists of temporary hemodialysis or ultrafiltration. Sedation and analgesia: Sedation is often required to treat anxiety and agitation in patients with severe sepsis. Because these patients are at risk for pain and physical discomfort, analgesics also are commonly employed. Ensure adequate nutrition: Sepsis is a hypercatabolic state. Therefore, caloric and nitrogen requirements should be met and enteral nutrition provided in a timely fashion. Provide hematological support: Critically ill patients may require packed red blood cells, platelets, and coagulation factors. Other supportive measures: These include measures to prevent deep venous thrombosis, stress ulcer prophylaxis, etc. Wheeler AP, Bernard GR. Treating patients with severe sepsis. N Engl J Med. 1999;340: Wheeler AP, Bernard GR. N Engl J Med. 1999;340:
 interventions intended to normalize physiology and eliminate infection. These are divided into: Source control: This term refers to management of the source of the infection. It can consist of surgery to drain an abscess or removal of an infected catheter. Antibiotics: While the initial therapy may be broad-based and empiric, identification of the specific pathogen by microbiologic studies may result in a switch of the antibiotic to those that are the most specific and bacteriocidal. Hemodynamic support: This term refers to volume replenishment therapy followed, when necessary, by appropriate use of drugs such as norepinephrine to maintain blood pressure and organ perfusion. Mechanical ventilation: Respiratory failure is a common manifestation of pulmonary organ dysfunction in patients with severe sepsis. Mechanical ventilation is instituted to increase oxygenation and improve gas exchange. Renal replacement therapy: Impaired renal function is a sign of organ dysfunction in patients with severe sepsis. Renal replacement therapy consists of temporary hemodialysis or ultrafiltration. Sedation and analgesia: Sedation is often required to treat anxiety and agitation in patients with severe sepsis. Because these patients are at risk for pain and physical discomfort, analgesics also are commonly employed. Ensure adequate nutrition: Sepsis is a hypercatabolic state. Therefore, caloric and nitrogen requirements should be met and enteral nutrition provided in a timely fashion. Provide hematological support: Critically ill patients may require packed red blood cells, platelets, and coagulation factors. Other supportive measures: These include measures to prevent deep venous thrombosis, stress ulcer prophylaxis, etc. Wheeler AP, Bernard GR. Treating patients with severe sepsis. N Engl J Med. 1999;340: Wheeler AP, Bernard GR. N Engl J Med. 1999;340:")
Presentaciones similares


















 es una alteración fisiopatólogica sistémica, trombohemorrágica, que se presenta en algunas situaciones.>")


