Descargar la presentación
La descarga está en progreso. Por favor, espere

1
WFSBP 2011 PRAGA ANDREA MARQUEZ LOPEZ MATO www.ipbi.com.ar

2
ANDREA MARQUEZ LOPEZ MATO Médica Psiquiatra. PNIE. Dolor Prof Psiconeuroinmunoendocrinología (UBA- Barcelo) Presidente electa CAPyN Miembro Honorífica FLAPNIE y AAPNIE Directora Instituto Psiquiatría Biológica Integral (ipbi) Presidente AAPB Presidente electa CANP Secretaria Científica FLAPB y AAPB Secretaria Científica FLAPB y AAPB Vicepresidente SAPNE Secretaria internacional AAP Secretaria adjunta FLAPB Secretaria GENBA LOPEZ MATO EX
 Presidente electa CAPyN Miembro Honorífica FLAPNIE y AAPNIE Directora Instituto Psiquiatría Biológica Integral (ipbi) Presidente AAPB Presidente electa CANP Secretaria Científica FLAPB y AAPB Secretaria Científica FLAPB y AAPB Vicepresidente SAPNE Secretaria internacional AAP Secretaria adjunta FLAPB Secretaria GENBA LOPEZ MATO EX.")
3
Speaker Bureau and/or Consultant AstraZenecaBago Eli LillyBuxton Glaxo SmithKlineGador LundbeckRaffo PfizerRoemmers Roche Sanofi Aventis Servier

5
Terapéutica Quetiapina en depresión Azenapina en psicosis Agomelatina en depresión Zavesca (inhibidor de la glucosilceramida) para Niemman Pick C
 para Niemman Pick C")
6
Neurobiology of Depression Miller et al, 2009

7
Apoptotic and Necrotic Cells Release DAMPS INFLAMMATION

9
GR/Bcl-2 complex doesn’t translocate into the mitochondria -Reduction of mitochondrial function, Bcl-2 -Apoptosis Biphasic Effect of Glucocorticoid on Mitochondria GR complexes with Bcl-2 and translocates to mitochondria -Increases mitochondrial function -Neuroprotection -Adaptation to acute stressful events GCs acute treatment or low doses: GCs chronic treatment or high doses:

10
Neurotrophic factors inhibit apoptosis BDNF NGF NT-3 IGF GDNF VEGF... Cross Talk Between Extrinsic and Intrinsic Apoptotic Pathways

11
Biomarker Approach Metabolomics/ Proteomics Clinical Characterisation Genetics/Genomics Neuroimaging Bioinformatics

12
WFSBP Task Forces

14
Niveles de Evidencia

16
Especificadores Poblaciones especiales Diagnostic subtypes Sex differences Adolescents Elderly Pregnant and puerperium Cardiovascular disease Somatic comorbidity

19
Panic Disorder

20
GAD

21
Social Phobia Specific Phobia

22
OCD

23
PTSD

27
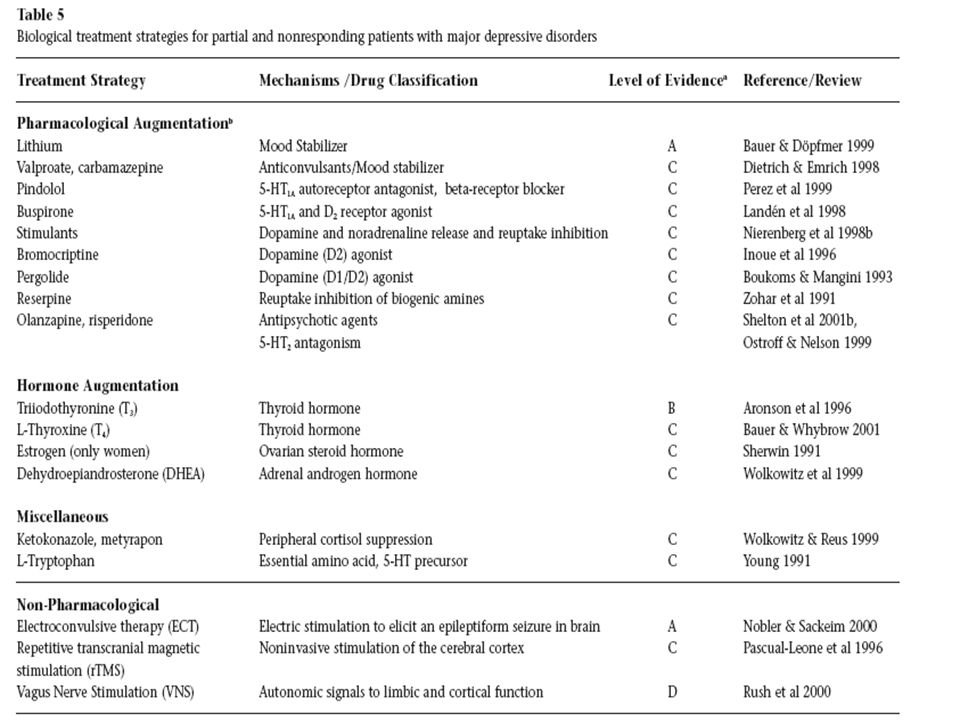
ATD Side Effects

32
Treatment of Personality Disorder

33
BDL Por rasgos: impulsividad, depresión, distorsión, cognitivos Nada para el vacio, el aburrimiento y la soledad Usar med de pocos efectos 2° por poca adherencia (LI, TPR) Avoidant Similar a TA Schizotypic Similar a Ez negativa y cognitiva
 Avoidant Similar a TA Schizotypic Similar a Ez negativa y cognitiva")
35
Acute Side Effects

37
Schizophrenia Long Term Treatment

38
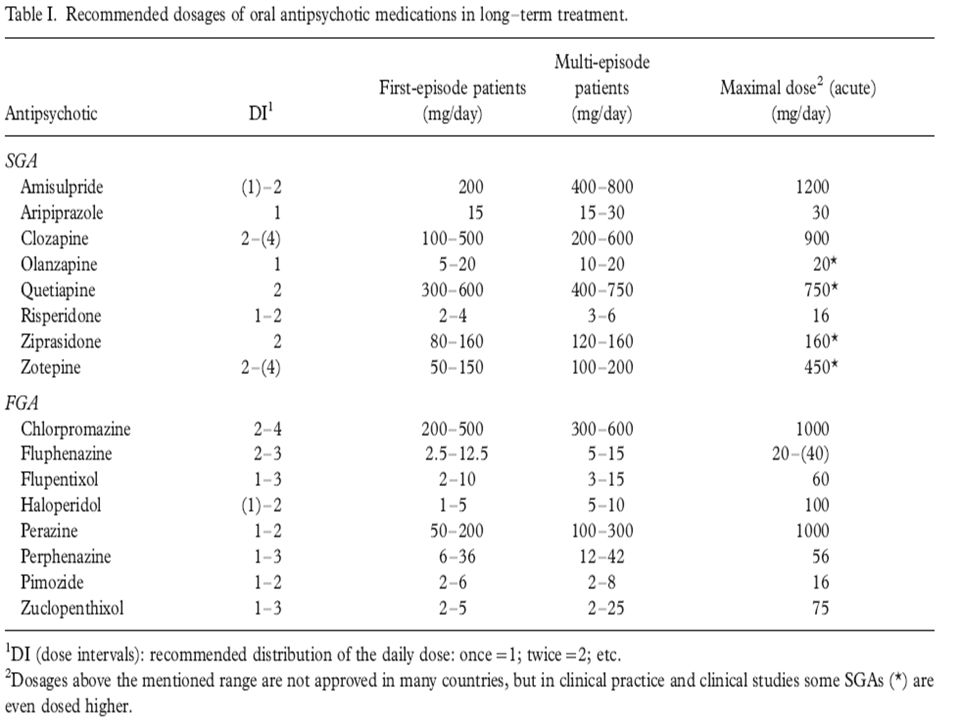
Primer brote 1 o 2 años de tto para evitar recaída 6 meses con misma dosis Resto por lo menos 5 años con full dose o mayor Mejor SGA Técnicas para controlar side effects

40
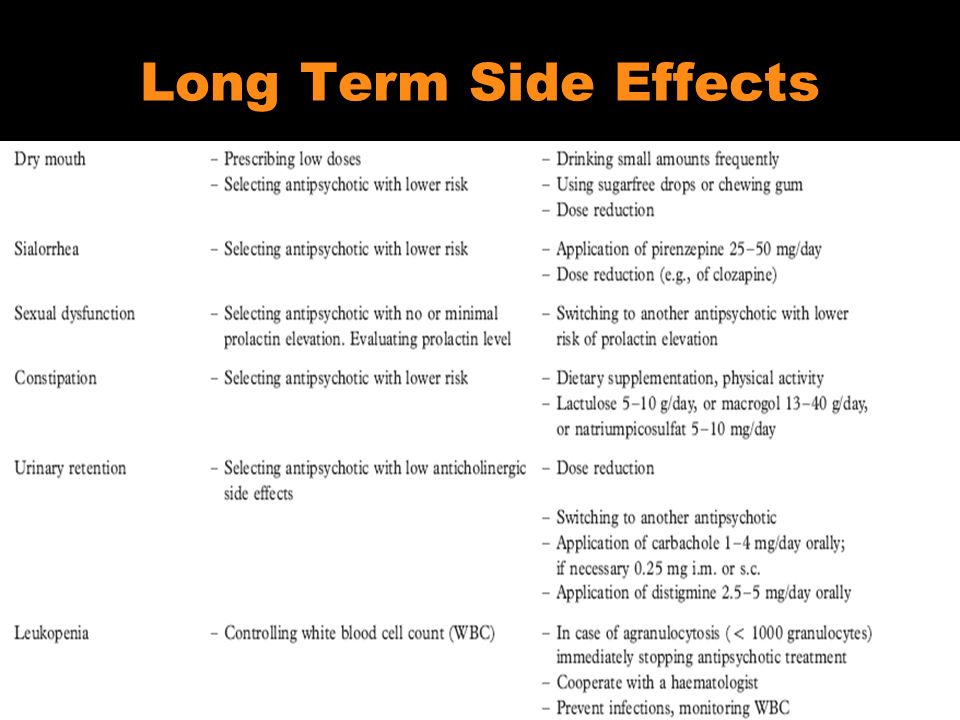
Long Term Side Effects

42
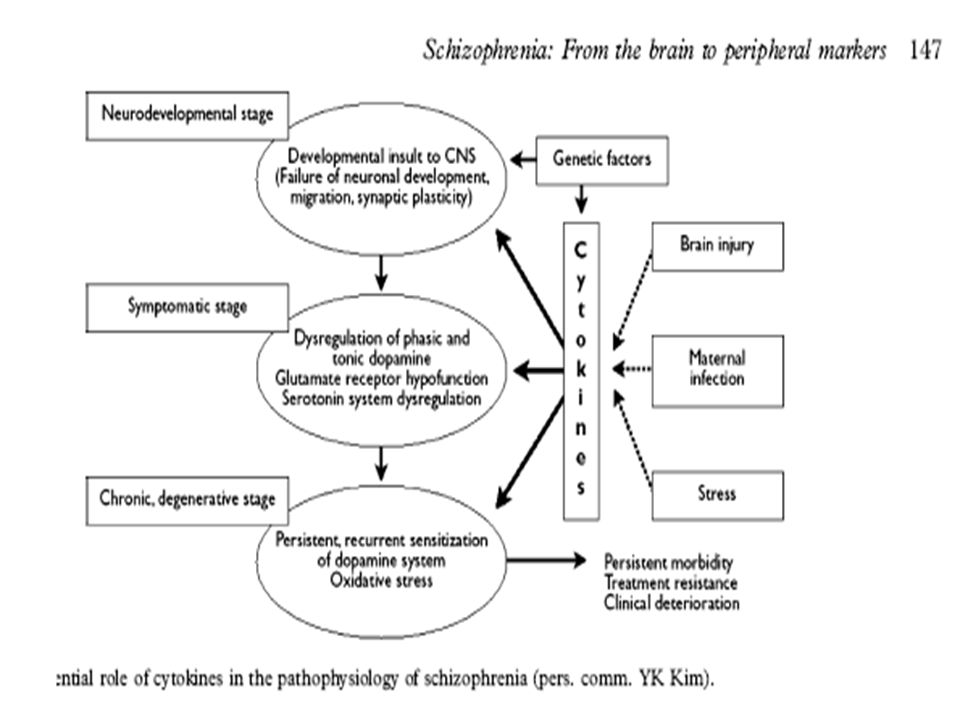
Biological Markers

44
esquizofrenia Marcadores genéticos Neuroimagenes estáticas y funcionales Evaluación neurocognitiva Factores de crecimiento Inmunológicos NMEM?

50
La frutilla del postre… Articulo online de la semana pasada

51
In recent years, however, we have seen the emergence and refinement of a number of different technologies that I predict will, within our professional lifetimes and hopefully within the next 5 years, lead to the incorporation of laboratory-based tests for psychiatric diagnosis. When these will be proved to a satisfactory level of evidence and when they will be reimbursable by third- party payers, we can't know specifically, but I predict this will happen fairly soon. We are seeing the evidence of that even now.

52
What will these diagnostic tests be? The tests that appear to be emerging as the first to be marketed are ones that are based on the proteomic or metabolomic or biochemical analyses of plasma or cerebrospinal fluid. A series of different types of microarray panels have been developed that examine the profile of a series of analytes in plasma, serum, or cerebrospinal fluid. Using these, a certain profile, a biochemical signature if you will, has been found to correspond to specific psychiatric diagnoses. Several companies have developed data, applied for approval from the US Food and Drug Administration, and are beginning to market these tests. Some of these tests] are being used by a few psychiatrists, even though they still have not been accepted as a standard of care

53
A second modality that is likely to be implemented for psychiatric diagnosis is that of imaging techniques; here we're talking about both nuclear medicine imaging with PET and MR imaging with either structural, spectroscopic, or functional imaging applications. These have been used in a variety of disorders. They yield clear differences between diagnostic groups such as schizophrenia or depression and healthy controls or nonaffected individuals on the other. The problem is that the distributions of the values of the control vs patient groups still have too much overlap and are not sufficiently differentiated as to provide high enough positive predictive value at the individual patient or subject level. But I predict that it won't be too long before these are refined, the results will become more robust, and these will contribute to a profile or augment the information that clinicians have to establish their diagnosis..

54
Finally, genetic testing will also come into play. As you probably know, commercial companies already are marketing DNA testing. They provide a "readout" of your genotypes for all of the known coded human genes along with associations with specific diseases in the different organ systems that these correspond to, to the best level of evidence that currently exists. These are not accepted as medically validated and are not used routinely in clinical practice but there is no reason psychiatry cannot begin to use these as other fields of medicine have done. Because all mental disorders will almost certainly prove to be polygenic or multigenic, we will need a gene profile to utilize in term of diagnostic information

55
So, I encourage you to stay tuned, follow this literature, and be thinking about the fact that in the not-too-distant future, psychiatry will have laboratory-based methods to assist in our diagnoses. This should be an enormous benefit to our field in terms of enhancing the validity and precision of our diagnosis as well as elevating the scientific quality of clinical practice for the benefit of our patients. Dr. Jeffrey Lieberman for Medscape, september 2011

56
RESPUESTA ALM A MAIL DE AR Date: Sun, 9 Oct 2011 12:41:20 -0300 Subject: Re: Y me preguntan porque trabajo tanto ??? From: andrealopezmato@gmail.com To: arivetti@hotmail.comandrealopezmato@gmail.com estoy leyendo tu mail mientras preparo charla congreso aapb ayer prepare 2 charlas peru y esta tarde me espera terminar 3 caps para mi libro LA de PNIE todo trabajo con placer eso si, con juan que trabaja en otras cosas pero interrumpimos de tanto en tanto para besitos y algun drink te quiero Que genia ! Yo estoy en lo mismo preparando el de AAPB y otro más. Pero a mí me falta tener al lado "la compañía"... Don't worry...está cerca, lo se ( no alucino, eh ! es una sensación no más...) Un abrazo a los 2, yo también te quiero mucho, Adriana RESPUESTA AR MAIL DE ALM
 Un abrazo a los 2, yo también te quiero mucho, Adriana RESPUESTA AR MAIL DE ALM.")
57
Te quedaste con ganas de más … Busca todo en : – www.aapb.org www.aapb.org – www.wfsbp.org MUCHAS GRACIAS Andrea Marquez Lopez Mato

Presentaciones similares















 –>")
. EXLPANATION GUSTAR is not conjugated like other regular verbs. It is NEVER used in the “yo”, “tú”, or “nosotros” forms. When.>")




 Los Pronombres.>")






>")



