Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Curso de actualización en hepatitis virales
Tratamiento de la hepatitis B Curso de actualización en hepatitis virales SoMaMFyC Madrid, de octubre de 2011 Javier García-Samaniego Hospital Carlos III. CIBERehd Madrid

2
Objetivos del tratamiento de la hepatitis B1,2
Supresión sostenida de la replicación del VHB Remisión de la enf. hepática Prevención de la cirrosis Prevención CHC El objetivo último del tratamiento antiviral en la infección crónica por VHB es la seroconversión del HBsAg 1. Lok ASF and McMahon BJ. Hepatology 2007; 45: 2. EASL Guidelines. J Hepatol 2009; 50:

3
End-points of therapy Therapy:
Must reduce HBV DNA to as low a level as possible, ideally below the lower limit of detection of real-time PCR assays (10-15 IU/mL) To ensure a degree of viral suppression that will then lead to biochemical remission, histological improvement and prevention of complications
 To ensure a degree of viral suppression that will then lead to biochemical remission, histological improvement and prevention of complications.")
4
Virological End-points of HBV therapy
HBeAg-positive and negative patients: Sustained HBsAg loss, with or without seroconversion to anti-HBs (ideal end-point) HBeAg-positive patients Durable HBe seroconversion (satisfactory endpoint) HBeAg-positive patients who do not achieve HBe seroconversion and HBeAg-negative patients: Maintained undetectable HBV DNA level with NUCs Sustained undetectable HBV DNA level after IFN therapy
 HBeAg-positive patients. Durable HBe seroconversion (satisfactory endpoint) HBeAg-positive patients who do not achieve HBe seroconversion and HBeAg-negative patients: Maintained undetectable HBV DNA level with NUCs. Sustained undetectable HBV DNA level after IFN therapy.")
5
Advances in the management of chronic hepatitis B (CHB)
Interferon -alfa 2a (IFN-α 2a) EASL HBV Consensus Statement Lamivudine (LAM) Entecavir (ETV) Tenofovir DF (TDF) 1992 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 Adefovir (ADV) Peg-interferon alfa-2a (PEG IFN-α 2a) EASL HBV Guidelines Telbivudine (LdT)
 EASL HBV Consensus Statement. Lamivudine. (LAM) Entecavir. (ETV) Tenofovir DF. (TDF) Adefovir. (ADV) Peg-interferon alfa-2a. (PEG IFN-α 2a) EASL HBV Guidelines. Telbivudine. (LdT)")
6
Undetectable HBV DNA after 1 year of therapy for HBeAg(+) CHB*
100 Treatments LLOQ (copies/ml) Tenofovir (TDF) Entecavir (ETV) Telbivudine (TBV) Lamivudine (LVD) Pegylated interferon (PEG IFN) alpha 2a 400 Adefovir (ADV) Pegylated interferon (PEG IFN) alpha 2b 400 Undetectable HBV DNA (%) 80 76% 67% 60% 60 40 36% 25% 21% 20 10% TDF1 ETV2 TBV3 LVD2 PEG IFN-alpha-2a4 ADV5 PEG IFN alpha-2b6 1. Heathcote J, et al. EASL 2008 2. Chang TT, et al. N Engl J Med. 2006;354: 3. Lai CL, et al. N Engl J Med 2007;357: 4. Lau GKK, et al. N Engl J Med. 2005;352: 5. Marcellin P, et al. N Engl J Med. 2003;348: 6. Janssen H et al. Lancet. 2005;365:123-9. *Collation of currently available data – not from head-to-head studies – using different DNA assays
 Tenofovir (TDF) 400. Entecavir (ETV) 300. Telbivudine (TBV) 300. Lamivudine (LVD) 300. Pegylated interferon (PEG IFN) alpha 2a 400. Adefovir (ADV) 400. Pegylated interferon (PEG IFN) alpha 2b 400. Undetectable HBV DNA (%) % 67% 60% % 25% 21% % TDF1. ETV2. TBV3. LVD2. PEG IFN-alpha-2a4. ADV5. PEG IFN alpha-2b6. 1. Heathcote J, et al. EASL Chang TT, et al. N Engl J Med. 2006;354: Lai CL, et al. N Engl J Med 2007;357: Lau GKK, et al. N Engl J Med. 2005;352: Marcellin P, et al. N Engl J Med. 2003;348: Janssen H et al. Lancet. 2005;365: *Collation of currently available data – not from head-to-head studies. – using different DNA assays.")
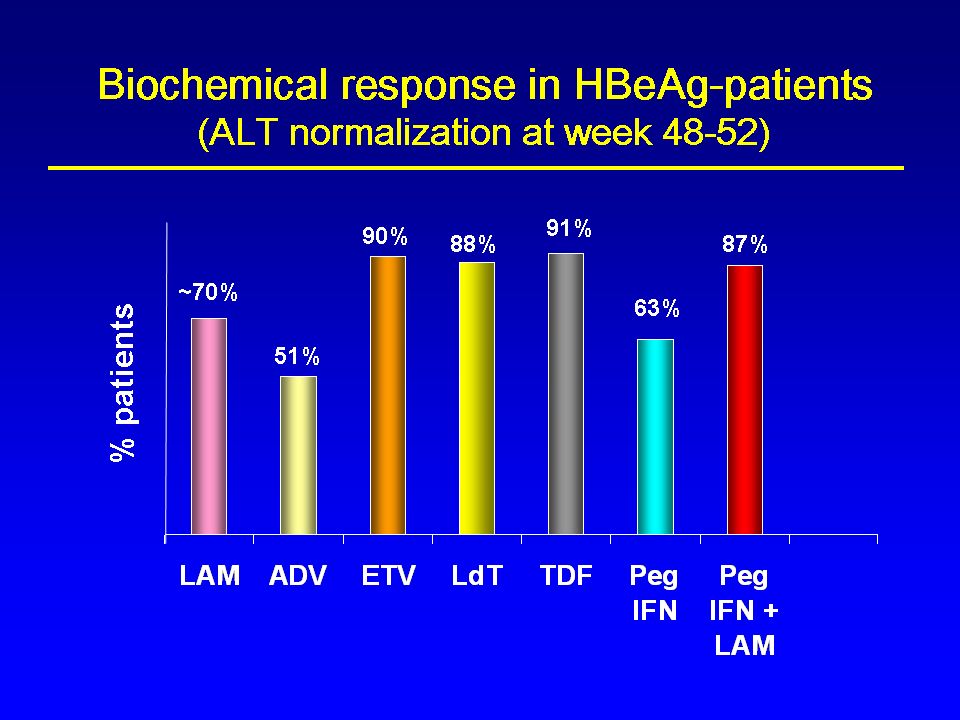
7
Undetectable HBV DNA in HBeAg-Negative Patients at 1 Year
Collation of currently available data: Not from head-to-head studies using different DNA assays undetectable HBV DNA 300–400 cp/mL Marcellin, EASL 2008; Lai et al., N Engl J Med. 2006; Lai et al., N Engl J Med. 2007;

9
Indications for treatment
(EASL Guidelines) The same for HBeAg-positive and -negative patients HBV DNA level >2,000 IU/mL (>10,000 cp/mL) and/or Serum ALT > ULN and Liver biopsy (or noninvasive markers) shows ≥ A2F2 in Metavir
 The same for HBeAg-positive and -negative patients. HBV DNA level >2,000 IU/mL (>10,000 cp/mL) and/or. Serum ALT > ULN. and. Liver biopsy (or noninvasive markers) shows ≥ A2F2 in Metavir.")
10
Special groups Immunotolerant patients No treatment
Patients with mild chronic hepatitis B Patients with compensated cirrhosis and detectable HBV DNA Treatment Patients with decompensated cirrhosis Urgent treatment

11
Estrategias actuales de tratamiento de la Hepatitis Crónica B
Estrategias de tratamiento Tratamiento finito con interferón pegilado Tratamiento finito con nucleós(t)idos Tratamiento indefinido con nucleós(t)idos EASL guidelines. J Hepatol 2009;50:227–242.
idos. Tratamiento indefinido con nucleós(t)idos. EASL guidelines. J Hepatol 2009;50:227–242.")
12
MECHANISMS OF ACTION OF INTERFERON IN CHRONIC HEPATITIS B
Direct antiviral effect WEAKER vs available NUCs Immunomodulatory effects MUCH STRONGER vs available NUCs Virological/biochemical/histological responses develop differently vs NUCs Enhancement of virus infected cells lysis may occur during therapy with IFN

13
HBeAg seroconversion after 1 year of therapy for HBeAg(+) CHB*
35 32% 30 29% 25 Patients (%) 22% 22% 20 18% 15 12% 10 5 PEG IFN alpha-2a1 PEG IFN-alpha-2b2 TDF3 ETV4 LVD4 ADV5 1. Lau GKK., et al. N Engl J Med 2005; 352: 2. Janssen H, et al. Lancet 2005:365: 3. Heathcote J, et al. EASL 2008 4. Chang TT, et al. N Engl J Med. 2006;354: 5. Marcellin P, et al. N Engl J Med. 2003;348: *Collation of currently available data – not from head-to-head studies
 22% 22% % % PEG IFN alpha-2a1. PEG IFN-alpha-2b2. TDF3. ETV4. LVD4. ADV5. 1. Lau GKK., et al. N Engl J Med 2005; 352: Janssen H, et al. Lancet 2005:365: Heathcote J, et al. EASL Chang TT, et al. N Engl J Med. 2006;354: Marcellin P, et al. N Engl J Med. 2003;348: *Collation of currently available data – not from head-to-head studies.")
14
Treatment of finite duration with Peg-IFN
48 weeks course of Peg-IFN HBeAg-positive patients with the best chance of HBe seroconversion: High baseline ALT (> 3 x ULN) HBV DNA < 2 x106 IU/mL Genotypes A & B
 HBV DNA < 2 x106 IU/mL. Genotypes A & B.")
15
Treatment of finite duration with NUCs
Duration is unpredictable before treatment as it depends on when HBe seroconversion occurs HBe seroconversion more likely in HBeAg-positive patients with: High baseline ALT (> 3 x ULN) HBV DNA < 2 x106 IU/mL Use tenofovir or entecavir to rapidly reduce HBV DNA Prolong therapy 6 to (preferentially) 12 months after HBe seroconversion
 HBV DNA < 2 x106 IU/mL. Use tenofovir or entecavir to rapidly reduce HBV DNA. Prolong therapy 6 to (preferentially) 12 months after HBe seroconversion.")
16
Long-term treatment with NUCs
Indicated in HBeAg-positive patients who did not achieve an HBe seroconversion HBeAg-negative patients The most potent drugs with the optimal resistance profile should be used as first-line monotherapies: Tenofovir Entecavir

17
El desarrollo de nuevos NUC ha cambiado el panorama del tratamiento de la hepatitis crónica B…
Sin embargo, la aparición de cepas resistentes es un problema clínico 17

18
Preexistencia de cepas del VHB con mutaciones resistentes al tratamiento
Poco frecuentes en pacientes no tratados previamente Si estas mutaciones están presentes pueden comprometer significativamente la eficacia del tratamiento antiviral 18

19
La resistencia precede a la reactivación bioquímica y clínica
Breakthrough ALT Virologic Biochemical Viral Breakthrough >1 log10 ADN del VHB Clinical-biochemical effects Límite inferior de detección del ADN del VHB por PCR 6 12 Resistencia genotípica LiPA RLFP Secuenciación directa + - Lok A & McMahon B. J. Hepatol. 2007;45: 19

20
La resistencia precede a la reactivación bioquímica y clínica
Rebote ALT Virológico Bioquímico Rebote Viral >1 log10 ADN VHB Efectos Bioquímicos y Clínicos Limite de Detección Inferior del AND VHB por PCR 6 12 Resistencia Genotípica LiPA RLFP Secuenciación Directa + - + + Lok A & McMahon B. J. Hepatol. 2007;45: 20

21
Keeffe EB, et al. Clin Gastroenterol Hepatol. 2006;4:936-962.
Implicaciones del desarrollo de cepas del VHB resistentes al tratamiento Pérdida de beneficios clínicos Incremento en los niveles de ADN del VHB Aumento de ALT y eventual reversión de la mejoría histológica Progresión de la enfermedad hepática: en pacientes con cirrosis riesgo de descompensación Desarrollo de la resistencia a múltiples fármacos Resistencia cruzada Emergencia de nuevas variantes resistentes Transmisión de cepas del VHB con resistencia Keeffe EB, et al. Clin Gastroenterol Hepatol. 2006;4: 21

22
Perfiles de resistencia a los fármacos anti-VHB
Potencia antiviral Barrera a la resistencia Lamivudina ++ Baja Telbivudina +++ Entecavir Alta Adefovir + Tenofovir Tenofovir + FTC

23
Tasas de resistencia durante 6 años entre pacientes no tratados previamente con nucleós(t)idos
72 semanas LVD 23% 46% 55% 71% 80% ADV 0% 3% 11% 18% 29% LdT 5% 25% – – – TDF 0% 0% 0% 0% – ETV <1% <1% 1,2% 1,2% 1,2% 1,2%

24
Incidencia acumulada (%)
La resistencia del VHB a entecavir se ve comprometida por la resistencia previa a lamivudina 100 Entecavir (no tratados previamente): resistencia genotípica Entecavir (resistentes a lamivudina): resistencia genotípica 80 57 60 51 Incidencia acumulada (%) 46 40 36 20 15 6 1,2 0,2 0,5 1,2 1,2 1,2 1 2 3 4 5 6 Año Colonno RJ et al. J Hepatol 2007;46(S1):S294 (abs. 781) . Lai CL, et al. Clin Infect Dis. 2003;36: Lok AS, et al. Gastroenterology. 2003;125: Tenney DJ et al. Hepatol Int 2008; 2 (Suppl. 3): S302-S303 Tenney et al. EASL April 22–26, 2009, Copenhagen, Denmark, Oral Presentation 1761
: resistencia genotípica. Entecavir (resistentes a lamivudina): resistencia genotípica Incidencia acumulada (%) ,2. 0,2. 0,5. 1,2. 1,2. 1, Año. Colonno RJ et al. J Hepatol 2007;46(S1):S294 (abs. 781) . Lai CL, et al. Clin Infect Dis. 2003;36: Lok AS, et al. Gastroenterology. 2003;125: Tenney DJ et al. Hepatol Int 2008; 2 (Suppl. 3): S302-S303. Tenney et al. EASL April 22–26, 2009, Copenhagen, Denmark, Oral Presentation")
25
“Drugs don’t work if people don’t take them” C
“Drugs don’t work if people don’t take them” C. Everett Koop Former US Surgeon General C. Everett Koop

26
Adherencia Estudio longitudinal de adherencia a fármacos antihipertensivos: Pautas de dosificación una vez al día de 4783 pts El 50% de los pacientes interrumpieron la medicación durante el primer año de tratamiento De los que tomaron la medicación durante un año, el 43% “tomó“ vacaciones terapéuticas (mínimo 3 días) Vrijens et al, BMJ 2008;336:1114.
 Vrijens et al, BMJ 2008;336:1114.")
27
El mal cumplimiento puede comprometer seriamente la eficacia del tratamiento antiviral y contribuir a la aparición de resistencias World Health Organization. Adherence to Long-Term Therapies – Evidence for Action Available at: .(Accessed February 2010).
.")
28
“It is a miracle that curiosity survives formal education”
Albert Einstein

Presentaciones similares


















 and numbers are used to tell time. Copyright © 2008 Vista Higher Learning. All rights reserved.>")
.>")