Descargar la presentación
La descarga está en progreso. Por favor, espere

1
ABORDAJE TERAPÉUTICO EN LAS ENFERMEDADES AUTOINMUNES SISTÉMICAS
Pautas de tratamiento en las formas severas Parte 2 Dr. Lucio Pallarés Ferreres Unitat Malalties Autoimmunes Sistèmiques Servicio de Medicina Interna Hospital Universitario Son Dureta

2
“GOLD STANDARD” en el Tratamiento
Actualmente: Diversas pautas de administración en fase de inducción Nuevos Fármacos Inmunodepresores

3
CORTICOIDES: Pauta de Administración
BOLUS de Metilprednilsona (EV) (Solu-Moderín®) 1 gramo, en 500ml de suero salino Administrar en 4-6 horas Puede repetirse diariamente durante 3-4 días
 (Solu-Moderín®) 1 gramo, en 500ml de suero salino. Administrar en 4-6 horas. Puede repetirse diariamente durante 3-4 días.")
4
CORTICOIDES: Pauta de Administración
BOLUS de Metilprednilsona (EV) Posteriormente, puede seguirse el tratamiento con dosis de corticoides de 0,5mg/Kg. de peso/día. Aunque de forma infrecuente, la administración en bolus de corticoides puede ocasionar problemas cardiovasculares, con aparición de arritmias.
 Posteriormente, puede seguirse el tratamiento con dosis de corticoides de 0,5mg/Kg. de peso/día. Aunque de forma infrecuente, la administración en bolus de corticoides puede ocasionar problemas cardiovasculares, con aparición de arritmias.")
5
CICLOFOSFAMIDA: Pauta de Administración
BOLUS de Ciclofosfamida (EV) (Genoxal®) 0,750 gramos/m2, en 250ml de suero salino Administrar en minutos Mantener hidratación ( ml suero glucosalino) Asociar antiemético: ondansetrón (Zofrán®) 1 ampolla/EV antes del Bolus. Puede repetirse a las 4h y a las 8h post-bolus Periodicidad Mensual
 (Genoxal®) 0,750 gramos/m2, en 250ml de suero salino. Administrar en minutos. Mantener hidratación ( ml suero glucosalino) Asociar antiemético: ondansetrón (Zofrán®) 1 ampolla/EV antes del Bolus. Puede repetirse a las 4h y a las 8h post-bolus. Periodicidad Mensual.")
6
CICLOFOSFAMIDA: Pauta de Administración
BOLUS de Ciclofosfamida (EV) Ajuste dosis mensuales Cada 15 días post-Bolus: Control hematológico <3000 leuc leuc. >5000 leuc. 0,500 gr./m2 0,750 gr./m2 1,000 gr./m2
 Ajuste dosis mensuales. Cada 15 días post-Bolus: Control hematológico. <3000 leuc leuc. >5000 leuc. 0,500 gr./m2 0,750 gr./m2 1,000 gr./m2.")
7
CICLOFOSFAMIDA: Pauta “Clásica”
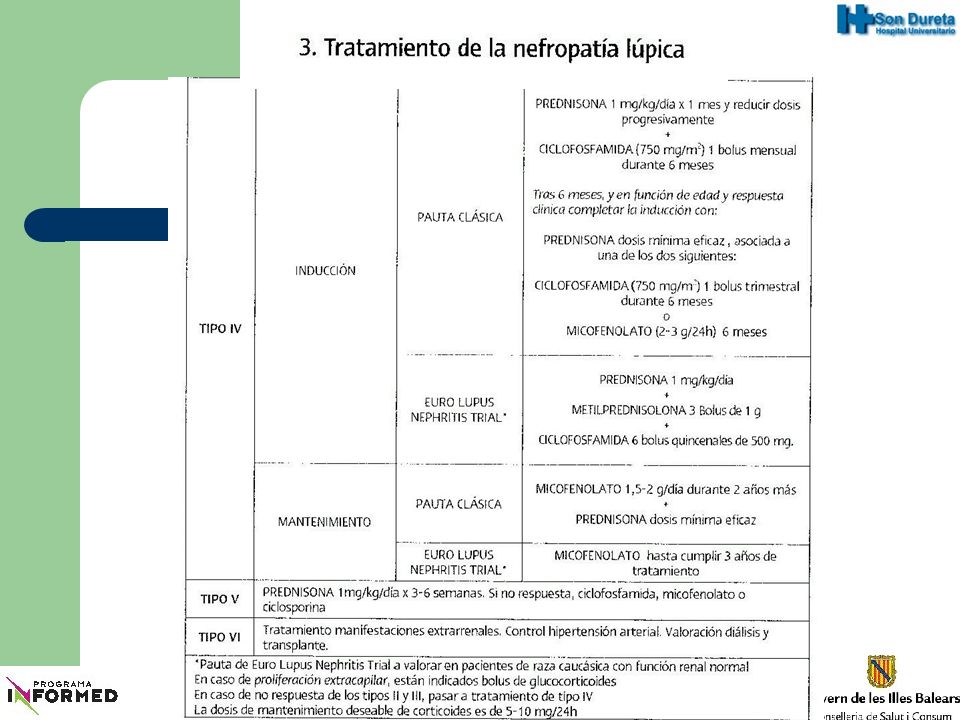
ALTAS DOSIS A LARGO PLAZO Bolus MENSUAL, durante 6 meses (puede prorrogarse) Posteriormente Bolus TRIMESTRAL durante 1-2 años Posteriormente cambiar de Inmunodepresor (Azatioprina)
 Posteriormente Bolus TRIMESTRAL durante 1-2 años. Posteriormente cambiar de Inmunodepresor (Azatioprina)")
8
CICLOFOSFAMIDA: Pauta “Corta”
ALTAS DOSIS A CORTO PLAZO Bolus MENSUAL, máximo 6 meses Posteriormente cambiar de Inmunodepresor (Azatioprina)
")
9
CICLOFOSFAMIDA: Pauta “Bajas Dosis”
BAJAS DOSIS (Pauta St. Thomas’ Hospital) (Genoxal®) 0,500 gramos en 250ml de suero salino Periodicidad QUINCENAL, durante 3 meses (6 Bolus) Posteriormente cambiar de Inmunodepresor (Azatioprina)
 (Genoxal®) 0,500 gramos en 250ml de suero salino. Periodicidad QUINCENAL, durante 3 meses (6 Bolus) Posteriormente cambiar de Inmunodepresor (Azatioprina)")
10
Annals of the Rheumatic Diseases
Volume 56, Number 8 (August 1, 1997) Immunosuppressive treatment in severe connective tissue diseases: effects of low dose intravenous cyclophosphamide Martin-SuarezA1, M. MansoorA2, A.P. FernandesA3, M.A. KhamashtaA4, G.R.V. HughesA5, D. D'CruzA6
 Immunosuppressive treatment in severe connective tissue diseases: effects of low dose intravenous cyclophosphamide. Martin-SuarezA1, M. MansoorA2, A.P. FernandesA3, M.A. KhamashtaA4, G.R.V. HughesA5, D. D CruzA6.")
11
Immunosuppressive treatment in severe connective tissue diseases: effects of low dose intravenous cyclophosphamide Objective To review our experience with low dose intravenous pulse cyclophosphamide in the treatment of patients with severe connective tissue diseases. Patients Ninety patients with severe connective tissue diseases: systemic lupus erythematosus (SLE) (n=43); systemic vasculitides (n=42); idiopathic inflammatory myopathies (n=4); mixed essential cryoglobulinaemic vasculitis (n=1). Median age was 48 (22-76) years with a median disease duration of 94 (18-250) months.
 (n=43); systemic vasculitides (n=42); idiopathic inflammatory myopathies (n=4); mixed essential cryoglobulinaemic vasculitis (n=1). Median age was 48 (22-76) years with a median disease duration of 94 (18-250) months.")
12
Immunosuppressive treatment in severe connective tissue diseases: effects of low dose intravenous cyclophosphamide Results Complete or partial remission was noted in 75.5% after a median follow up of 56 (5-213) months. Vasculitis, Churg-Strauss syndrome, Wegener's granulomatosis, and neuropsychiatric lupus showed the best initial response but 58% of Wegener's patients relapsed. Median corticosteroid doses were significantly reduced. Adverse events: infections (7), neutropenia (5), lymphopenia (18), and haemorrhagic cystitis (3). None of the women had prolonged amenorrhoea. Five patients doubled their serum creatinine and five died from sepsis (2) or severe disease (3).
 months. Vasculitis, Churg-Strauss syndrome, Wegener s granulomatosis, and neuropsychiatric lupus showed the best initial response but 58% of Wegener s patients relapsed. Median corticosteroid doses were significantly reduced. Adverse events: infections (7), neutropenia (5), lymphopenia (18), and haemorrhagic cystitis (3). None of the women had prolonged amenorrhoea. Five patients doubled their serum creatinine and five died from sepsis (2) or severe disease (3).")
13
Immunosuppressive treatment in severe connective tissue diseases: effects of low dose intravenous cyclophosphamide Conclusion Treatment of severe connective tissue diseases with 'low dose' intravenous cyclophosphamide pulses compares in efficacy with the higher monthly doses previously advocated. Treatment was well tolerated with fewer adverse effects and most significantly, there were no cases of premature ovarian failure.

15
Ninety patients with lupus nephritis were treated with three pulses of intravenous methylprednisolone (IV MP) after which they were allocated to one of two groups The high-dose group received IV CYC 0.5 g/m2 every month for 6 months, increased according to the nadir white cell count. These patients then received two further pulses of IV CYC. The low-dose group received 500 mg IV CYC every 2 weeks for a total of six infusions. Both groups were given azathioprine (2 mg/kg/day) after remission was induced. Follow-up in this study was for a median of 41 months.
 after remission was induced. Follow-up in this study was for a median of 41 months.")
16
Results: Renal remission was seen in 71% of patients in the low-dose group and 54% in the high-dose CYC group. This difference was not statistically significant. Treatment failures in both groups was similar (16%). The ELNT confirms that low-dose IV CYC demonstrates a comparable efficacy to a high-dose treatment regime. There was more infections with high-dose CYC, with twice as many infections occurring in this group. Low incidence of amenorrhoea in the high-dose group (cumulative dose of CYC was lower than in the standard NIH regime).
. The ELNT confirms that low-dose IV CYC demonstrates a comparable efficacy to a high-dose treatment regime. There was more infections with high-dose CYC, with twice as many infections occurring in this group. Low incidence of amenorrhoea in the high-dose group (cumulative dose of CYC was lower than in the standard NIH regime).")
20
The alternative low-dose regime has not been supported by sufficiently long or sufficiently numerous trials to be accepted as an adequate replacement for the NIH platinum standard regime. Further large trials comparing the high-dose and low-dose CYC regimes will be carried out

Presentaciones similares

 European Transfer Credit System (ECTS) Methodology in.>")


















