Descargar la presentación
La descarga está en progreso. Por favor, espere

1
UNIDAD HEMATO-ONCOLOGÍA INFANTIL
Dra C. Guerra Becada pediatria HCVB

2
Antecedentes Escolar 8 años 1 mes Antecedentes perinatales: RN sana
Peso al nacer: 3,150Kg, T: 49 cms Lactancia materna hasta los 7 meses Mórbidos: Sin antecedentes de importancia

3
Antecedentes Vacunas según programa vacunación EEUU pendiente 2º dosis hepatitis A Antecedentes Familiares: Madre 33 años, amaurosis bilateral por retinitis pigmentosa congénita Padre 33 años sano Hermanos 5 y 11 años sanos En Estados Unidos (Atlanta) 2004-hasta 24 Mayo por trabajo, en situación ilegal Alimentación: normal, polivitamínico
 2004-hasta 24 Mayo 2009 por trabajo, en situación ilegal. Alimentación: normal, polivitamínico.")
5
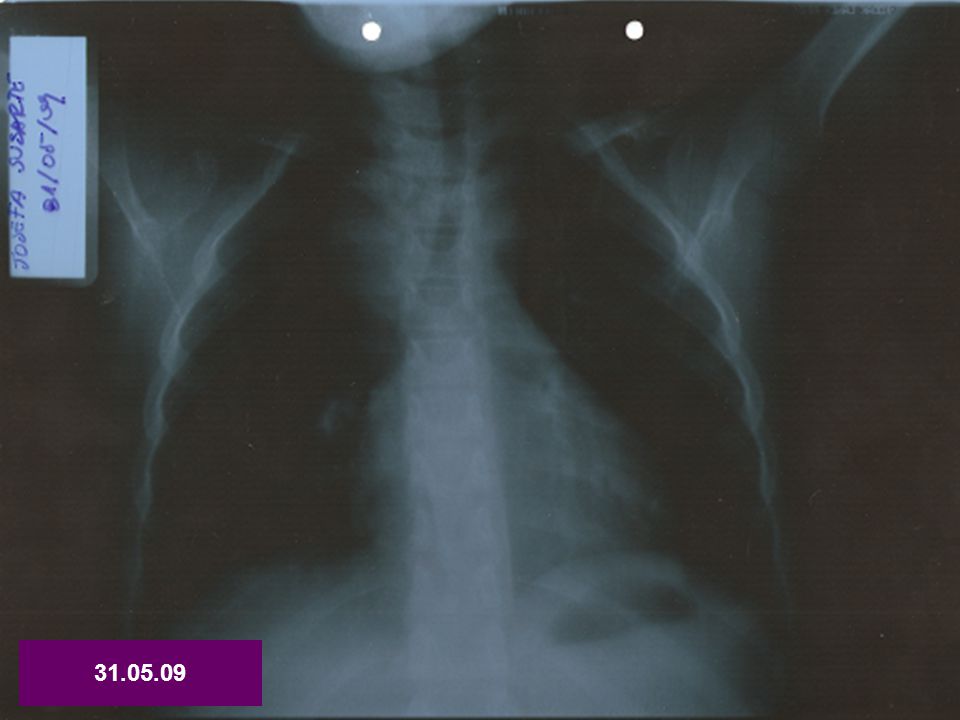
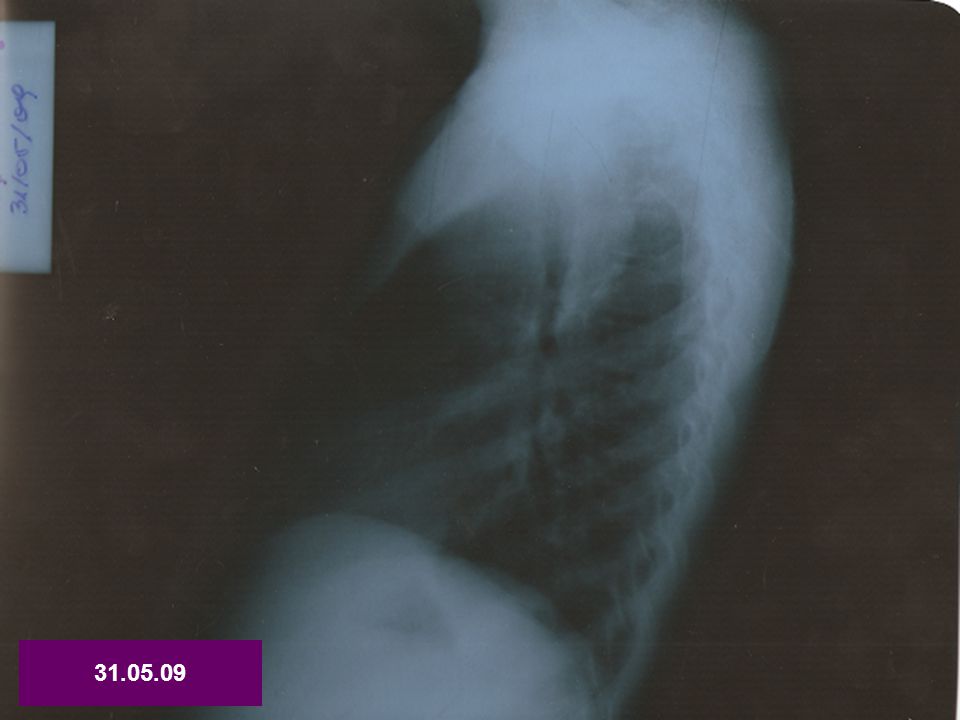
Cuadro de 4 días de evolución con rinorrea, odinofagia y tos, al segundo día se agrega fiebre hasta 39ºC Inicialmente hospitalizada en Quilpué con sospecha influenza A H1N1 en tratamiento con Oseltamivir Se realizan exámenes: Hto 31% Hb 9,5 leucocitos 3900 plqtas PCR 26 mg/dl

8
2Junio 2009: Traslado de Hospital Quilpué a Hospital Gustavo Fricke
Tratamiento penicilina sódica ev Evoluciona sin dificultad respiratoria, febril Se deriva para estudio Diagnósticos: ¿Neumonia redonda? ¿masa mediastínica? Anemia en estudio

9
2 Junio 2009: Hospital Gustavo Fricke
Al examen: pálida febril 38ºC, satura 100% ambiental FR 26/min FC 121/min Tos húmeda Faringe congestiva Pequeñas adenopatías blandas cervicales Tórax: RR2T sin soplo, MP(+) SRA Abdomen: BD sin masas Extremidades: móviles, bien perfundidas
 SRA. Abdomen: BD sin masas. Extremidades: móviles, bien perfundidas.")
10
Indicaciones Mantener penicilina sódica 1 millon U cada 6 hrs ev Oseltamivir 50mg cada 12 hrs vo TAC tórax Repetir IFI viral, exámenes

11
IFI viral (+) parainfluenza
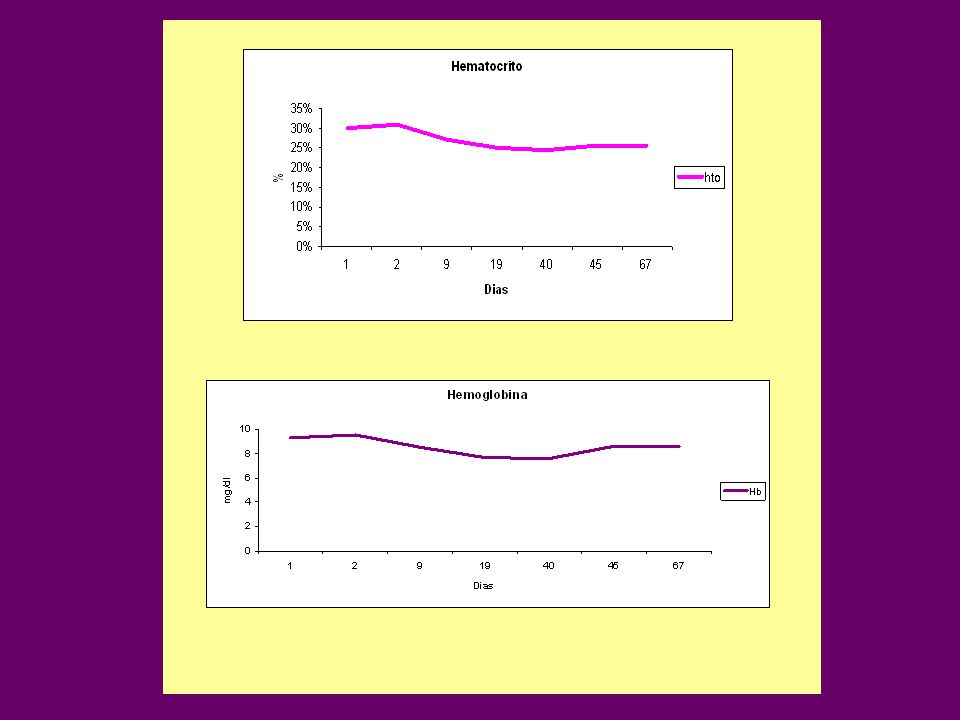
PCR 25,6 mg/dl LDH 356 VHS 119 Hto 26% eritrocitos 4,47mill/mm3 Hb 8,1 VCM 58,1 HCM 18,2 CHCM 31,3

12
Diagnósticos Virosis respiratoria sobreinfectada Obs: influenza H1N1 en tratamiento Masa mediastínica en estudio Anemia microcítica hipocroma en estudio

14
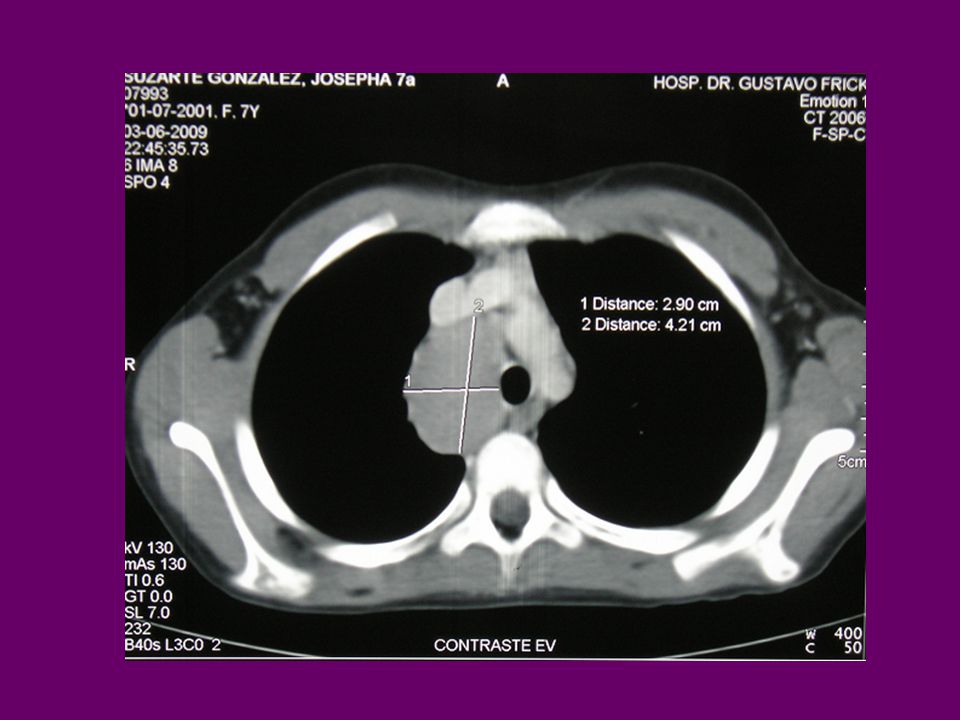
TAC tórax

18
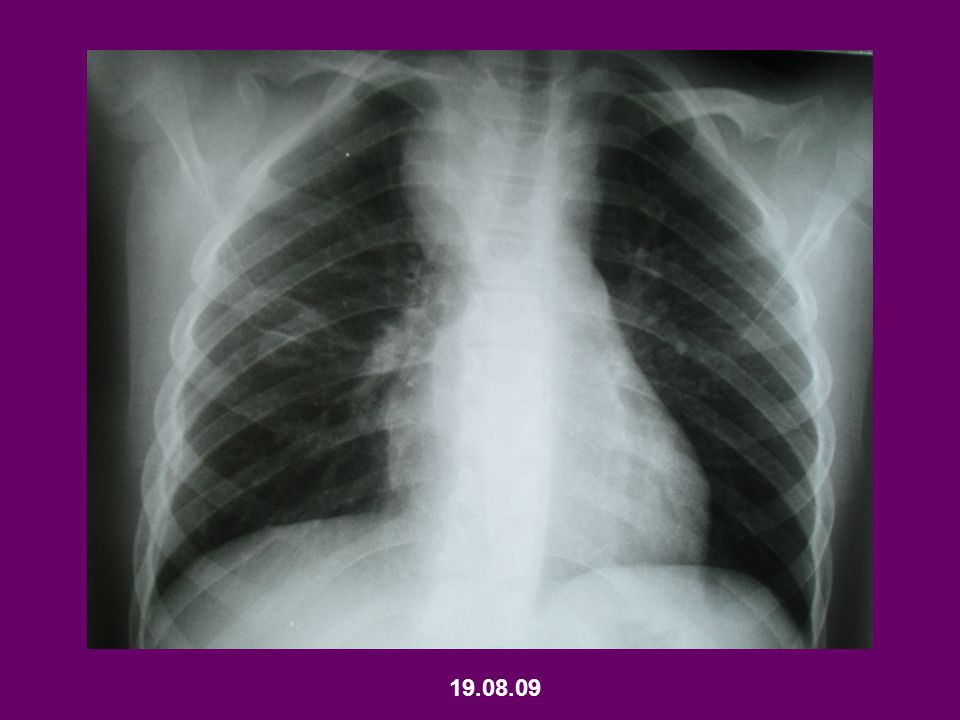
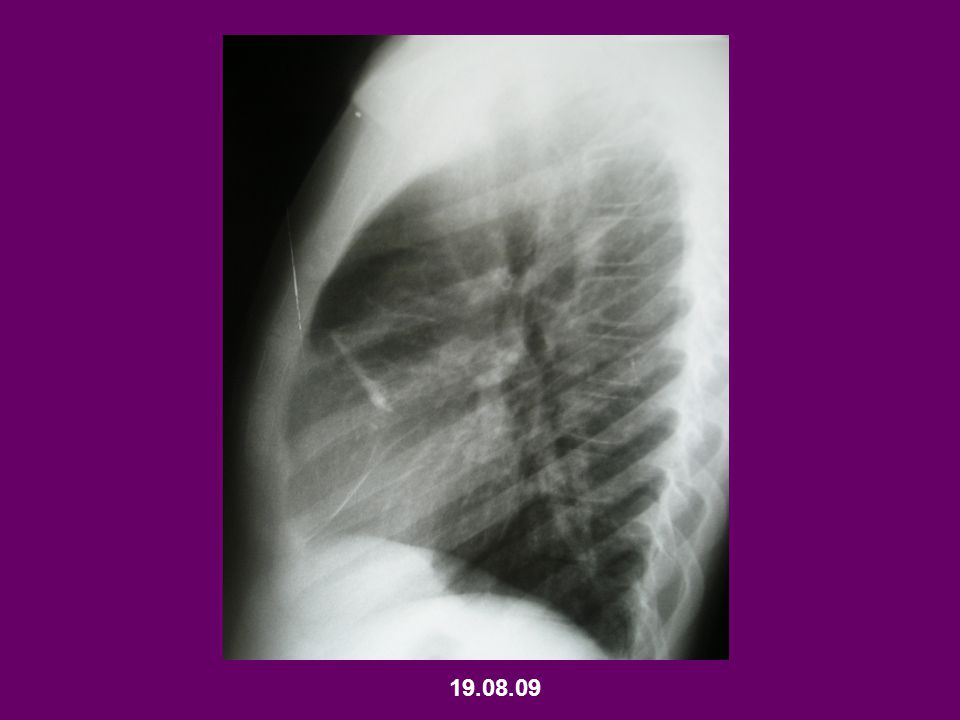
Según esto tenemos una masa de mediatino medio

19
POSIBILIDADES DIAGNÓSTICAS
MASA MEDIATINO MEDIO

20
¿LINFOMA? 25%

21
Múltiples adenopatías en espacio paratraqueal derecho
mediastino que forman masa de 4,2 * 2,9 cms Opacidades lineales en lóbulo medio pulmón derecho, de aspecto residual

22
TAC abdomen y pelvis Escasa cantidad de líquido libre en excavación pélvica de carácter inespecífico TAC cráneo,cerebro y cuello Cambios inflamatorios etmoido-maxilares izquierdos. Linfonodos yugulares internos y cadena cervical posterior <1 cm, sin adenopatía de significado patológico

23
09.06.09 Cintigrama óseo Sin hallazgos patológicos
Ig G aumentada 3130 mg/dl, con Ig A e Ig M normales Mielograma: Sin infiltración ,con histofagocitosis ++. No diagnóstico Ferremia 11, ferritina 194 ng/ml, transferrina 218 Completa 3 días con oseltamivir y 8 días con penicilina sódica. Evoluciona afebril con PCR elevada en forma persistente (25-20) En buenas condiciones pero siempre enferma, nunca dolors oseos ni hepatoesplenomegalia
 En buenas condiciones pero siempre enferma, nunca dolors oseos ni hepatoesplenomegalia.")
24
11.06.09 Biopia por videotoracoscopía
Microscopía: Estructura tisular nodular linfática con centros germinales y gran cantidad de macrófagos a nivel centro germinal. Linfocitos pequeños y áreas necróticas periféricas. En uno de los cortes predomina tejido fibroso. No se observan eosinófilos ni células reticulareshistiocitarias CONCLUSION: proceso reaccional linfático. CD68 +++ CD30 (-) CD15 (+) CD20 CD3 ++ CMV Agregar marcadores. Con este estudio IH se descartan linfomas Hospital Luis Calvo Mackenna
 CD15. (+) CD20. CD3. ++ CMV. Agregar marcadores. Con este estudio IH se descartan linfomas. Hospital Luis Calvo Mackenna.")
25
Exámenes al alta transitoria
Evoluciona febril hasta 38, con PCR en aumento (24,8) por lo que se inicia cefotaxima y cloxacilina completando 6 días, se suspenden con hemocultivos, cultivo maki tubo pleural y urocultivo negativos Exámenes al alta transitoria Hto 25,1%, Hb 7,7 g/dl, eritrocitos 3,85 mill/mm3 Alta transitoria VCM 59,9 HCM 18,4 CHCM 30,7 Pqtas PCR 21,4
 por lo que se inicia cefotaxima y cloxacilina completando 6 días, se suspenden con hemocultivos, cultivo maki tubo pleural y urocultivo negativos. Exámenes al alta transitoria. Hto 25,1%, Hb 7,7 g/dl, eritrocitos 3,85 mill/mm3. Alta transitoria. VCM 59,9 HCM 18,4 CHCM 30,7. Pqtas PCR 21,4.")
26
Por persistencia aspecto enfermo, no grave, exs lab alterados y biopsia no diagnostica
No pta fiebre pero persistencia masa y PCR elevada se decide nueva biopsia

27
Exámenes ingreso: Hto 24,3 eritrocitos 4 mill/mm3 Hb 7,6 g/dl VCM 60,6 HCM 19 CHCM 31,2 PCR 18,3

28
10.07.09 Se realiza nueva biopsia masa mediastínica y ganglio linfático de pared
Hallazgos más concordantes con proceso reaccional inflamatorio que con neoplasia mediastínica -Restos estructura linfática con folículos periféricos rodeados por tejido conjuntivo fibroso. Vasos sanguíneos con endotelio hiperplástico, linfocitos pequeños, zona edematosa fibrosa y con reacción inflamatoria, abundantes histiocitos macrofágicos y células plasmáticas Biopsia a masa y gg de la pared

29
Hospital Luis Calvo Mackenna
-Ganglio linfático estructura conservada. Folículos linfáticos periféricos, centros germinales aumentados de tamaño y con numerosos macrófagos con detritus celulares citoplasmáticos. Espacio sinusoidal dilatado, edematosos con linfocitos pequeños histiocitos y polimorfo nucleares. Destaca componente vascular con hiperplasia endotelial. CD68 CD30 CD15 CD20 CD3 CMV Hospital Luis Calvo Mackenna

30
Otros exámenes Cultivo de secreción mediastino (cary Blair), no se observan microorganismos al gram Baciloscopías negativas contenido gástrico y tejido Cultivo Koch (-) hasta ahora VIH negativo
 hasta ahora. VIH negativo.")
31
Al alta persiste anemia microcítica hipocroma
Evoluciona afebril, se decide dar alta y mantener conducta expectante. Se continúa estudio ambulatorio Al alta persiste anemia microcítica hipocroma Hto 25,5%, Hb 8,6, VCM 68,3, HCM 23,1, CHCM 33,7, trombocitosis En controles semanales

34
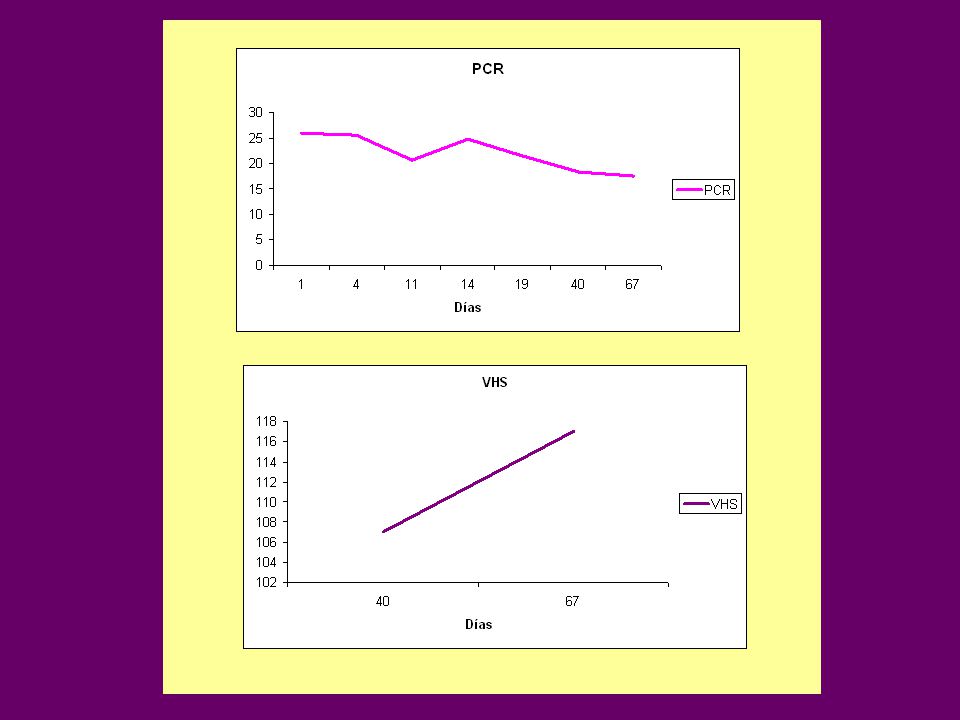
Exámenes actuales 19.08.09 -PCR 30 mg/dl -Ferritina 171
-Parámetros y VHS Eritrocitos 4,69 mill/mm3 Hto 28,6% Hb 9 g/dl Pqtas Leucocitos 9500 RAN 6800

37
Diagnósticos sindromáticos:
-Adenopatías medistínicas -Anemia microcítica hipocroma (¿Enfermedad crónica?) -Proceso inflamatorio persistente
 -Proceso inflamatorio persistente.")
39
DIAGNÓSTICO DIFERENCIAL LINFADENOPATÍAS
Enfermedad linfoproliferativa primaria Linfomas (Hodgkin y no Hodgkin) Histiocitosis Maligna Infiltrativas Malignas Metástasis (neuroblastomas/sarcoma) Leucemia No malignas Enf de depósito (Gaucher/NiemannPick) Amiloidosis Carnoma metast neuroblastoma sarcoma Reactivas Infecciosas No infecciosas Cohen & Powderly: Infectious Diseases, 2nd ed.
 Histiocitosis Maligna. Infiltrativas. Malignas. Metástasis (neuroblastomas/sarcoma) Leucemia. No malignas. Enf de depósito (Gaucher/NiemannPick) Amiloidosis. Carnoma metast neuroblastoma sarcoma. Reactivas. Infecciosas. No infecciosas. Cohen & Powderly: Infectious Diseases, 2nd ed.")
40
Infecciosas No Infecciosas
DIAGNÓSTICO DIFERENCIAL LINFADENITIS REACTIVA Infecciosas Virales: Mononucleosis Bacteriana: arañazo gato Micobacterias TBC y atípicas Espiroqueta: sífilis Fúngica: Histoplasmosis Parasitaria: Toxoplasmosis No Infecciosas sarcoidosis Enf tej conectivo LES Enfermedad kikuchi Kawasaki Cohen & Powderly: Infectious Diseases, 2nd ed.

41
LINFADENITIS Inflamación linfonodo
Respuesta inicial: edema e hiperplasia células sinusoidales e infiltración leucocitaria Evolución: progresión a absceso según microorganismo involucrado y respuesta huésped Lymphadenitis ( Table 16.2 ) represents inflammation of the lymph node. The initial response to acute inflammation consists of swelling and hyperplasia of the sinusoidal lining cells and infiltration by leukocytes. The process may progress to abscess formation depending on the micro-organism involved and the host response. Cohen & Powderly: Infectious Diseases, 2nd ed.
 represents inflammation of the lymph node. The initial response to acute inflammation consists of swelling and hyperplasia of the sinusoidal lining cells and infiltration by leukocytes. The process may progress to abscess formation depending on the micro-organism involved and the host response. Cohen & Powderly: Infectious Diseases, 2nd ed.")
42
Histología Enfermedades
ENFERMEDADES QUE CAUSAN LINFADENITIS Histología Linfadenitis supurativa aguda Linfadenitis con necrosis caseosa Linfadenitis granulomatosa necrotizante Linfadenitis granulomatosa no necrotizante Linfadenitis necrotizante no granulomatosa Enfermedades Infecciones piógenas(estrepto, estafilo, yersinia pestis) TBC (mycobacterium Tbc, mycobacter atípicas) Enf arañazo gato(Bartonella), Tularemia (Francisella tularensis) Leishmaniasis (Leishmania Brazilensis) Histoplasmosis, coccidiomicosis, sarcoidosis Sindrome kikuchi, LES Cohen & Powderly: Infectious Diseases, 2nd ed.
 TBC (mycobacterium Tbc, mycobacter atípicas) Enf arañazo gato(Bartonella), Tularemia (Francisella tularensis) Leishmaniasis (Leishmania Brazilensis) Histoplasmosis, coccidiomicosis, sarcoidosis. Sindrome kikuchi, LES. Cohen & Powderly: Infectious Diseases, 2nd ed.")
43
LINFADENITIS MEDIASTÍNICA E HILIAR
Algunas causas Tuberculosis Micosis endémicas Histoplasmosis Coccidiomicosis Sarcoidosis Disfonia por compresio nervio laringeo recurrente, sd vena cava por compresion vena cava sup Cohen & Powderly: Infectious Diseases, 2nd ed.

44
Tuberculosis Linfadenopatía aislada manifestación poco común
Considerar en alto riesgo: VIH, procedentes Asia o Africa Manifestación TBC primaria o como reactividad raro en TBC post primaria Adenopatías hiliares ipsilaterales o mediastínicas típicas en niños (menos en adultos) VIH Linfadenopatia mediastinica o hiliar es una manifestacion poco comun de tbc Isolated mediastinal or hilar lymphadenopathy is an uncommon manifestation of tuberculosis, although tuberculosis should be considered, especially in high-risk patients such as those infected with HIV or people from Asia or Africa. Mediastinal and hilar lymphadenopathy can be a manifestation of primary disease or of reactivation of tuberculosis ( Fig ). Isolated lymphadenopathy is relatively rare in postprimary tuberculosis.[40] Associated ipsilateral hilar or mediastinal adenopathy is almost universal in children who have primary tuberculosis but is less common in adults. In patients infected with HIV, mediastinal or hilar lymphadenopathy are usually present in tuberculosis even in the advanced stages of immunosuppression (see Chapter 129 ). Woodring HJ, Vandiviere M, Lee C: Intrathoracic lymphadenopathy in postprimary tuberculosis. South Med J 1988; 81:
 VIH. Linfadenopatia mediastinica o hiliar es una manifestacion poco comun de tbc. Isolated mediastinal or hilar lymphadenopathy is an uncommon manifestation of tuberculosis, although tuberculosis should be considered, especially in high-risk patients such as those infected with HIV or people from Asia or Africa. Mediastinal and hilar lymphadenopathy can be a manifestation of primary disease or of reactivation of tuberculosis ( Fig ). Isolated lymphadenopathy is relatively rare in postprimary tuberculosis.[40] Associated ipsilateral hilar or mediastinal adenopathy is almost universal in children who have primary tuberculosis but is less common in adults. In patients infected with HIV, mediastinal or hilar lymphadenopathy are usually present in tuberculosis even in the advanced stages of immunosuppression (see Chapter 129 ). Woodring HJ, Vandiviere M, Lee C: Intrathoracic lymphadenopathy in postprimary tuberculosis. South Med J 1988; 81:")
45
Micosis endémicas

46
Histoplasmosis Histoplasmosis Norteamericana o Fiebre Valle de Ohio
Causa Histoplasma capsulatum MT: Por inhalación esporas Endémica de EEUU, riveras missisipi y Ohio Incidencia áreas endémicas: 1/ casos Foco primario pulmón, con o sin extensión a histoplasmosis crónica o varias formas diseminación Bird and bat (murcielago)excrement Enhance(mejora) the growth of the organism in soil (suelo) by accelerating sporulation. Exposure typically occurs as a result of activities that generate aerosols containing the mycelial phase of the organism (Table 1). In most cases, however, the exact source of exposure is unknown 1/ poara histo pulmonar cronicvsa Histoplasmosis is caused by the fungus Histoplasma capsulatum and characterized by a primary pulmonary focus with occasional progression to chronic pulmonary histoplasmosis (CPH) or various forms of dissemination. Progressive disseminated histoplasmosis (PDH) may present with a diverse clinical spectrum, including adrenal necrosis, pulmonary and mediastinal fibrosis, and ulcerations of the oropharynx and GI tract. In those patients coinfected with the human immunodeficiency virus (HIV), it is a defining disease for acquired immunodeficiency syndrome (AIDS). Histoplasmosis is a fungal infection acquired through inhalation. It is endemic in the USA in the great river valleys of the Mississippi and Ohio. More than 90% of the primary infections are asymptomatic or only mildly symptomatic, although sudden enlargement of the hilar lymph nodes may cause substernal pain. Non-specific systemic symptoms such as fever, headache, malaise and anorexia are common. Most patients recover within 2–6 weeks. Typical findings on chest radiography in symptomatic patients include patchy pneumonic infiltrates. Mediastinal and hilar lymphadenopathy is common in patients with or without parenchymal involvement. At times, extension of the infection from the pulmonary parenchyma to the adjacent mediastinal lymph nodes causes central caseating necrosis and granuloma formation with multinucleated giant cells. Resolution causes fibrosis of the affected nodes, which usually causes no symptoms. Rarely, the fibrotic lymph nodes invade mediastinal structures, resulting in esophageal stricture or compromise to the mediastinal blood or lymph vessels (fibrosing mediastinitis).[41] L. Joseph Wheat, Carol A. Kauffman. Histoplasmosis. Infect Dis Clin N Am 17 (2003) 1–19
excrement. Enhance(mejora) the growth of the organism in soil (suelo) by accelerating sporulation. Exposure typically occurs as a result of activities that generate aerosols containing the mycelial phase of the organism (Table 1). In most cases, however, the exact source of exposure is unknown. 1/ poara histo pulmonar cronicvsa. Histoplasmosis is caused by the fungus Histoplasma capsulatum and characterized by a primary pulmonary focus with occasional progression to chronic pulmonary histoplasmosis (CPH) or various forms of dissemination. Progressive disseminated histoplasmosis (PDH) may present with a diverse clinical spectrum, including adrenal necrosis, pulmonary and mediastinal fibrosis, and ulcerations of the oropharynx and GI tract. In those patients coinfected with the human immunodeficiency virus (HIV), it is a defining disease for acquired immunodeficiency syndrome (AIDS). Histoplasmosis is a fungal infection acquired through inhalation. It is endemic in the USA in the great river valleys of the Mississippi and Ohio. More than 90% of the primary infections are asymptomatic or only mildly symptomatic, although sudden enlargement of the hilar lymph nodes may cause substernal pain. Non-specific systemic symptoms such as fever, headache, malaise and anorexia are common. Most patients recover within 2–6 weeks. Typical findings on chest radiography in symptomatic patients include patchy pneumonic infiltrates. Mediastinal and hilar lymphadenopathy is common in patients with or without parenchymal involvement. At times, extension of the infection from the pulmonary parenchyma to the adjacent mediastinal lymph nodes causes central caseating necrosis and granuloma formation with multinucleated giant cells. Resolution causes fibrosis of the affected nodes, which usually causes no symptoms. Rarely, the fibrotic lymph nodes invade mediastinal structures, resulting in esophageal stricture or compromise to the mediastinal blood or lymph vessels (fibrosing mediastinitis).[41] L. Joseph Wheat, Carol A. Kauffman. Histoplasmosis. Infect Dis Clin N Am 17 (2003) 1–19.")
47
Actividades Microfocos Cuevas/gallineros Aves/ bambu
Patio colegio/prisión Pilas descomposición Árboles muertos Limpieza, demolición, fertilizante excrementos Camping / excavación Corte caña / recreación Limpieza / actividades de rutina Transporte o quema demadera Chimeneas contaminadas Demolición/ remodelación/ limpieza Edificios antiguos/cubierta barcos L. Joseph Wheat, Carol A. Kauffman. Histoplasmosis. Infect Dis Clin N Am 17 (2003) 1–19
 1–19.")
48
Histoplasmosis Patogenia
Inhalación espora----neumonitis localizada o en parche Diseminación hematógena primeras 2 sems antes que se desarrolle respuesta inmune específica 2-3 sems respuesta inmune celular controla la infección (macrófagos fungicidas) Reactivación durante inmunosupresión CD4 lymphocytes activate macrophages to assume fungicidal properties, serving to control the infection in immunocompetent individuals. The interaction of the fungus and the host has been reviewed Recently Reactivation of quiescent infection is postulated to occur during immunosuppression [4]. Evidence for this includes the occurrence of histoplasmosis in persons who were born in the endemic area and who had not returned to that area but years later developed histoplasmosis L. Joseph Wheat, Carol A. Kauffman. Histoplasmosis. Infect Dis Clin N Am 17 (2003) 1–19
 Reactivación durante inmunosupresión. CD4 lymphocytes activate macrophages to assume fungicidal. properties, serving to control the infection in immunocompetent. individuals. The interaction of the fungus and the host has been reviewed. Recently. Reactivation of quiescent infection is postulated to occur during immunosuppression. [4]. Evidence for this includes the occurrence of histoplasmosis. in persons who were born in the endemic area and who had not returned. to that area but years later developed histoplasmosis. L. Joseph Wheat, Carol A. Kauffman. Histoplasmosis. Infect Dis Clin N Am 17 (2003) 1–19.")
49
Histoplasmosis Clínica
90% infección primaria asintomática o síntomas leves dolor por crecimiento linfonodos subesternales Síntomas no específicos: fiebre, cefalea, anorexia, compromiso estado general Asymptomatic infection The magnitude of exposure and the immune status of the host influence the clinical manifestations of histoplasmosis. Infection following low-level exposure of a normal host is typically asymptomatic, but attack rates for clinical disease exceed 75% following heavy exposure in normal hosts. In endemic areas, over half of adults have been infected with H capsulatum, and most remain asymptomatic (Table 2). Histoplasmosis is caused by the fungus Histoplasma capsulatum and characterized by a primary pulmonary focus with occasional progression to chronic pulmonary histoplasmosis (CPH) or various forms of dissemination. Progressive disseminated histoplasmosis (PDH) may present with a diverse clinical spectrum, including adrenal necrosis, pulmonary and mediastinal fibrosis, and ulcerations of the oropharynx and GI tract. In those patients coinfected with the human immunodeficiency virus (HIV), it is a defining disease for acquired immunodeficiency syndrome (AIDS). Histoplasmosis is a fungal infection acquired through inhalation. It is endemic in the USA in the great river valleys of the Mississippi and Ohio. More than 90% of the primary infections are asymptomatic or only mildly symptomatic, although sudden enlargement of the hilar lymph nodes may cause substernal pain. Non-specific systemic symptoms such as fever, headache, malaise and anorexia are common. Most patients recover within 2–6 weeks. Typical findings on chest radiography in symptomatic patients include patchy pneumonic infiltrates. Mediastinal and hilar lymphadenopathy is common in patients with or without parenchymal involvement. At times, extension of the infection from the pulmonary parenchyma to the adjacent mediastinal lymph nodes causes central caseating necrosis and granuloma formation with multinucleated giant cells. Resolution causes fibrosis of the affected nodes, which usually causes no symptoms. Rarely, the fibrotic lymph nodes invade mediastinal structures, resulting in esophageal stricture or compromise to the mediastinal blood or lymph vessels (fibrosing mediastinitis).[41] L. Joseph Wheat, Carol A. Kauffman. Histoplasmosis. Infect Dis Clin N Am 17 (2003) 1–19
. Histoplasmosis is caused by the fungus Histoplasma capsulatum and characterized by a primary pulmonary focus with occasional progression to chronic pulmonary histoplasmosis (CPH) or various forms of dissemination. Progressive disseminated histoplasmosis (PDH) may present with a diverse clinical spectrum, including adrenal necrosis, pulmonary and mediastinal fibrosis, and ulcerations of the oropharynx and GI tract. In those patients coinfected with the human immunodeficiency virus (HIV), it is a defining disease for acquired immunodeficiency syndrome (AIDS). Histoplasmosis is a fungal infection acquired through inhalation. It is endemic in the USA in the great river valleys of the Mississippi and Ohio. More than 90% of the primary infections are asymptomatic or only mildly symptomatic, although sudden enlargement of the hilar lymph nodes may cause substernal pain. Non-specific systemic symptoms such as fever, headache, malaise and anorexia are common. Most patients recover within 2–6 weeks. Typical findings on chest radiography in symptomatic patients include patchy pneumonic infiltrates. Mediastinal and hilar lymphadenopathy is common in patients with or without parenchymal involvement. At times, extension of the infection from the pulmonary parenchyma to the adjacent mediastinal lymph nodes causes central caseating necrosis and granuloma formation with multinucleated giant cells. Resolution causes fibrosis of the affected nodes, which usually causes no symptoms. Rarely, the fibrotic lymph nodes invade mediastinal structures, resulting in esophageal stricture or compromise to the mediastinal blood or lymph vessels (fibrosing mediastinitis).[41] L. Joseph Wheat, Carol A. Kauffman. Histoplasmosis. Infect Dis Clin N Am 17 (2003) 1–19.")
50
Compromiso pulmonar agudo Mediastinitis fibrosante
Manifestaciones clínicas % Asintomática 50-90 Sintomática 10-50 Sindromes Compromiso pulmonar agudo 60 Reumatológico 10 Pericarditis Compromiso pulmonar crónico Diseminada Histoplasmomas <1 Mediastinitis fibrosante L. Joseph Wheat, Carol A. Kauffman. Histoplasmosis. Infect Dis Clin N Am 17 (2003) 1–19
 1–19.")
51
Histoplasmosis Pulmonar
Post bajo nivel exposición síntomas subagudos similares a influenza: Tos seca, fiebre, fatiga (varias sems post exposición) Rx tórax Crecimiento linfonodos hiliares y mediastínicos e infiltrados en parche (puede ser normal) Mejoría en 2-3 sems a veces fatiga puede persistir Pulmonary histoplasmosis Following the more common low-level exposure, symptomatic pulmonary histoplasmosis is most often a subacute, mild flu-like illness with a dry cough, fever, and fatigue that occurs several weeks after exposure. Chest radiographs usually show enlarged hilar or mediastinal lymph nodes and patchy infiltrates, but may be normal [7]. Improvement in 2 to 3 weeks is characteristic, but in some individuals, fatigue may linger. Following heavy exposure, patients often present with diffuse pulmonary involvement [8]. Symptoms include high fever, chills, fatigue, dyspnea, cough, and chest pain [9]. Respiratory failure and death may ensue [10]. Chest radiographs show diffuse reticulonodular pulmonary infiltrates, sometimes with mediastinal lymphadenopathy [8]. Some patients manifest progressive extrapulmonary dissemination [8]. Although patients can recover from a heavy inoculum exposure without treatment [8], illness often is severe and recovery slow. L. Joseph Wheat, Carol A. Kauffman. Histoplasmosis. Infect Dis Clin N Am 17 (2003) 1–19
 Rx tórax. Crecimiento linfonodos hiliares y mediastínicos e infiltrados en parche (puede ser normal) Mejoría en 2-3 sems a veces fatiga puede persistir. Pulmonary histoplasmosis. Following the more common low-level exposure, symptomatic pulmonary. histoplasmosis is most often a subacute, mild flu-like illness with a dry. cough, fever, and fatigue that occurs several weeks after exposure. Chest. radiographs usually show enlarged hilar or mediastinal lymph nodes and. patchy infiltrates, but may be normal [7]. Improvement in 2 to 3 weeks is. characteristic, but in some individuals, fatigue may linger. Following heavy exposure, patients often present with diffuse pulmonary. involvement [8]. Symptoms include high fever, chills, fatigue, dyspnea, cough, and chest pain [9]. Respiratory failure and death may ensue [10]. Chest radiographs show diffuse reticulonodular pulmonary infiltrates, sometimes. with mediastinal lymphadenopathy [8]. Some patients manifest progressive. extrapulmonary dissemination [8]. Although patients can recover. from a heavy inoculum exposure without treatment [8], illness often is severe. and recovery slow. L. Joseph Wheat, Carol A. Kauffman. Histoplasmosis. Infect Dis Clin N Am 17 (2003) 1–19.")
52
Histoplasmosis Pulmonar
Alto nivel exposición Compromiso pulmonar difuso Fiebre alta, fatiga, disnea, tos y dolor torácico A veces falla respiratoria, muerte Rx tórax Infiltrado reticulonodular difuso Algunos diseminación extrapulmonar progresiva L. Joseph Wheat, Carol A. Kauffman. Histoplasmosis. Infect Dis Clin N Am 17 (2003) 1–19 L. Joseph Wheat, Carol A. Kauffman. Histoplasmosis. Infect Dis Clin N Am 17 (2003) 1–19
 1–19. L. Joseph Wheat, Carol A. Kauffman. Histoplasmosis. Infect Dis Clin N Am 17 (2003) 1–19.")
53
Granuloma mediastínico
Obstruccion vía aérea, vasos pulmonares, vena cava o esófago (<10% con histoplasmosis aguda) Inflamación, necrosis linfonodos puede ser años post infección inicial Riesgo formación fístulas con estructuras mediatínicas Rx tórax Crecimiento linfonodo TAC tórax Compromiso estructuras adyacentes Mediastinal granuloma Enlarged lymph nodes can partially obstruct the airways, pulmonary vessels or vena cava, or the esophagus. This occurs in less than 10% of patients with acute pulmonary histoplasmosis. Such findings, the result of smoldering inflammation and necrosis in the involved lymph nodes, may be delayed for years after the initial infection. Fistulae can form between necrotic nodes and adjacent mediastinal structures. Radiographs show enlarged lymph nodes; CT scans of the chest document the extent of nodal enlargement and help define impingement on adjacent structures. Although enlarged mediastinal nodes usually shrink and symptoms resolve without treatment [11], obstructive syndromes may be severe, and the masses may persist for years [12]. Granulomatous mediastinitis is not thought to progress to fibrosing mediastinitis [13]. L. Joseph Wheat, Carol A. Kauffman. Histoplasmosis. Infect Dis Clin N Am 17 (2003) 1–19
 Inflamación, necrosis linfonodos puede ser años post infección inicial. Riesgo formación fístulas con estructuras mediatínicas. Rx tórax. Crecimiento linfonodo. TAC tórax. Compromiso estructuras adyacentes. Mediastinal granuloma. Enlarged lymph nodes can partially obstruct the airways, pulmonary vessels. or vena cava, or the esophagus. This occurs in less than 10% of patients. with acute pulmonary histoplasmosis. Such findings, the result of smoldering. inflammation and necrosis in the involved lymph nodes, may be delayed. for years after the initial infection. Fistulae can form between necrotic nodes. and adjacent mediastinal structures. Radiographs show enlarged lymph. nodes; CT scans of the chest document the extent of nodal enlargement and help define impingement on adjacent structures. Although enlarged mediastinal. nodes usually shrink and symptoms resolve without treatment [11], obstructive syndromes may be severe, and the masses may persist for years. [12]. Granulomatous mediastinitis is not thought to progress to fibrosing. mediastinitis [13]. L. Joseph Wheat, Carol A. Kauffman. Histoplasmosis. Infect Dis Clin N Am 17 (2003) 1–19.")
54
Granuloma mediastínico
Evolución: Mayoría se retraen, resolución sin tratamiento Riesgo Síndromes obstructivos graves Masas que persisten por años Mediastinal granuloma Enlarged lymph nodes can partially obstruct the airways, pulmonary vessels or vena cava, or the esophagus. This occurs in less than 10% of patients with acute pulmonary histoplasmosis. Such findings, the result of smoldering inflammation and necrosis in the involved lymph nodes, may be delayed for years after the initial infection. Fistulae can form between necrotic nodes and adjacent mediastinal structures. Radiographs show enlarged lymph nodes; CT scans of the chest document the extent of nodal enlargement and help define impingement on adjacent structures. Although enlarged mediastinal nodes usually shrink and symptoms resolve without treatment [11], obstructive syndromes may be severe, and the masses may persist for years [12]. Granulomatous mediastinitis is not thought to progress to fibrosing mediastinitis [13]. L. Joseph Wheat, Carol A. Kauffman. Histoplasmosis. Infect Dis Clin N Am 17 (2003) 1–19
 1–19.")
55
Laboratorio Diagnóstico: Cultivos Tinción para hongo
Detección antígeno Test serológicos A variety of tests, including cultures, fungal stain, antigen detection, and serologic tests for antibodies, are used for the diagnosis of histoplasmosis [37]. The specific role of each test discussed next in different syndromes varies in accordance with host and mycologic factors. For example, the fungal burden is greater in disseminated and diffuse acute pulmonary histoplasmosis, supporting a special role for antigen testing. Serologic tests are highly useful for the subacute and chronic forms of histoplasmosis, but have limitations in immunosuppressed patients with disseminated infection and early in the course of acute pulmonary infection. Cultures Cultures are positive in about 85% of cases with disseminated or chronic pulmonary histoplasmosis (Table 3) [38]. Cultures of lung biopsy or bronchoscopy samples are often positive in patients with acute pulmonary histoplasmosis following a heavy inoculum exposure, but not in the more typical case of subacute, localized pulmonary histoplasmosis. H capsulatum requires several weeks to grow in vitro; culture plates or tubes are held L. Joseph Wheat, Carol A. Kauffman. Histoplasmosis. Infect Dis Clin N Am 17 (2003) 1–19
 [38]. Cultures of lung biopsy or bronchoscopy. samples are often positive in patients with acute pulmonary histoplasmosis. following a heavy inoculum exposure, but not in the more typical. case of subacute, localized pulmonary histoplasmosis. H capsulatum. requires several weeks to grow in vitro; culture plates or tubes are held. L. Joseph Wheat, Carol A. Kauffman. Histoplasmosis. Infect Dis Clin N Am 17 (2003) 1–19.")
56
Sensibilidad Test laboratorio Histoplasmosis: % VP Test Diseminada
Pulmonar crónica Antígeno 92 21 Cultivo 85 Histopatología 43 17 Serología 71 100 A variety of tests, including cultures, fungal stain, antigen detection, and serologic tests for antibodies, are used for the diagnosis of histoplasmosis [37]. The specific role of each test discussed next in different syndromes varies in accordance with host and mycologic factors. For example, the fungal burden is greater in disseminated and diffuse acute pulmonary histoplasmosis, supporting a special role for antigen testing. Serologic tests are highly useful for the subacute and chronic forms of histoplasmosis, but have limitations in immunosuppressed patients with disseminated infection and early in the course of acute pulmonary infection. Cultures Cultures are positive in about 85% of cases with disseminated or chronic pulmonary histoplasmosis (Table 3) [38]. Cultures of lung biopsy or bronchoscopy samples are often positive in patients with acute pulmonary histoplasmosis following a heavy inoculum exposure, but not in the more typical case of subacute, localized pulmonary histoplasmosis. H capsulatum requires several weeks to grow in vitro; culture plates or tubes are held 4 to 6 weeks before they are reported as showing no growth. Multiple specimens must be cultured to achieve the highest yield. The optimal method for processing blood cultures is the Isolator lysis-centrifugation method. Antigen detection Detection of a polysaccharide antigen in the blood, urine, CSF, or bronchoalveolar lavage fluid of infected patients offers a method for rapid diagnosis of disseminated and extensive acute pulmonary histoplasmosis [39,40]. Antigen can be detected in the urine of 90% of patients with disseminated infection and 75% with diffuse acute pulmonary histoplasmosis. The sensitivity for antigen detection is lower in serum than in urine. Cross-reactions occur in patients with penicilliosis, paracoccidioidomycosis, blastomycosis, and African histoplasmosis [41]. The positivity rate ranged from 63% with blastomycosis to 94% with penicilliosis in that study. Of note, however, cross-reactions have not been observed with aspergillosis, candidiasis, cryptococcosis, coccidioidomycosis, and other mycoses. Antigen levels fall with successful therapy, eventually reaching the undetectable range in those who are cured or whose infection is suppressed while receiving chronic maintenance therapy. Persistent antigenuria or antigenemia implies ongoing active infection and supports continued antifungal therapy. Antigen levels rise with relapse [42], supporting use of the test to follow patients after discontinuation of therapy or during chronic maintenance therapy. A rise of greater than or equal to 2 units should trigger studies to exclude relapse, assess antifungal drug levels, and exclude drug-drug interactions leading to decreased activity of the antifungal agent. Testing is available at the Histoplasmosis Reference Laboratory in Indianapolis, Indiana, and results are available at the end of the day that the specimen is received. Fungal stains Silver stain of tissue sections or Wright’s stain of peripheral blood smears permits rapid diagnosis in patients with acute disseminated infection or severe pulmonary infection. Mistakes in identification of Histoplasma organisms are common, however, in laboratories less familiar with the staining characteristics of fungal pathogens. Candida glabrata, Cryptococcus neoformans, Blastomyces dermatitidis, Penicillium marneffei, Pneumocystis carinii, Toxoplasma gondii, Leishmania donovani, and staining artifacts may be misidentified as H capsulatum. Serologic tests The standard serologic tests for antibodies to H capsulatum are the complement fixation (CF) test using both yeast and mycelial antigens and the immunodiffusion (ID) assay. Enzyme immunoassay methods are poorly standardized, difficult to interpret, and complicated by high background positivity, and are not recommended. Serologic tests for antibodies to H capsulatum are positive in greater than 90% of patients with pulmonary histoplasmosis [22,43], and about 80% with disseminated disease [37]. Certain limitations of serologic testing, however, should be recognized. First, 2 to 6 weeks are required for antibody production. Second, serologic tests are less sensitive in immunosuppressed patients and titers are lower [25,38]. Third, positive serologic tests may result from prior infection and incorrectly suggest active histoplasmosis in patients with other diseases. Background rates of seropositivity range from 0.5% by ID to 4% by CF. Finally, antibodies to H capsulatum may be elevated in patients with other fungal infections, most commonly blastomycosis, coccidioidomycosis, and paracoccidioidomycosis [44]. The CF test is more sensitive than the ID test [43]. In acute pulmonary histoplasmosis, the CF test is positive (titers1:8) in 90% of patients, whereas ID reveals M bands in 76% and H bands in only 23% [38,43]. CF assays, however, seem to be less specific than ID assays. Cross-reactions with other fungal infections occur in 5% of cases by ID, 18% by CF, and 49% by radioimmunoassay [45]. Antibody titers decline following self-limited infection, reaching low or undetectable levels in 2 to 5 years [43]. Antibody levels often remain high in those with chronic pulmonary infection [17], progressive disseminated disease [22], or fibrosing mediastinitis L. Joseph Wheat, Carol A. Kauffman. Histoplasmosis. Infect Dis Clin N Am 17 (2003) 1–19
 [38]. Cultures of lung biopsy or bronchoscopy. samples are often positive in patients with acute pulmonary histoplasmosis. following a heavy inoculum exposure, but not in the more typical. case of subacute, localized pulmonary histoplasmosis. H capsulatum. requires several weeks to grow in vitro; culture plates or tubes are held 4 to 6 weeks before they are reported as showing no growth. Multiple specimens. must be cultured to achieve the highest yield. The optimal method for. processing blood cultures is the Isolator lysis-centrifugation method. Antigen detection. Detection of a polysaccharide antigen in the blood, urine, CSF, or bronchoalveolar. lavage fluid of infected patients offers a method for rapid diagnosis. of disseminated and extensive acute pulmonary histoplasmosis [39,40]. Antigen can be detected in the urine of 90% of patients with disseminated. infection and 75% with diffuse acute pulmonary histoplasmosis. The sensitivity. for antigen detection is lower in serum than in urine. Cross-reactions. occur in patients with penicilliosis, paracoccidioidomycosis, blastomycosis, and African histoplasmosis [41]. The positivity rate ranged from 63% with. blastomycosis to 94% with penicilliosis in that study. Of note, however, cross-reactions have not been observed with aspergillosis, candidiasis, cryptococcosis, coccidioidomycosis, and other mycoses. Antigen levels fall with. successful therapy, eventually reaching the undetectable range in those who. are cured or whose infection is suppressed while receiving chronic maintenance. therapy. Persistent antigenuria or antigenemia implies ongoing active. infection and supports continued antifungal therapy. Antigen levels rise. with relapse [42], supporting use of the test to follow patients after discontinuation. of therapy or during chronic maintenance therapy. A rise of. greater than or equal to 2 units should trigger studies to exclude relapse, assess. antifungal drug levels, and exclude drug-drug interactions leading to. decreased activity of the antifungal agent. Testing is available at the Histoplasmosis. Reference Laboratory in Indianapolis, Indiana, and results are. available at the end of the day that the specimen is received. Fungal stains. Silver stain of tissue sections or Wright’s stain of peripheral blood smears. permits rapid diagnosis in patients with acute disseminated infection or severe pulmonary infection. Mistakes in identification of Histoplasma. organisms are common, however, in laboratories less familiar with the staining. characteristics of fungal pathogens. Candida glabrata, Cryptococcus. neoformans, Blastomyces dermatitidis, Penicillium marneffei, Pneumocystis. carinii, Toxoplasma gondii, Leishmania donovani, and staining artifacts may. be misidentified as H capsulatum. Serologic tests. The standard serologic tests for antibodies to H capsulatum are the complement. fixation (CF) test using both yeast and mycelial antigens and the. immunodiffusion (ID) assay. Enzyme immunoassay methods are poorly. standardized, difficult to interpret, and complicated by high background. positivity, and are not recommended. Serologic tests for antibodies to H. capsulatum are positive in greater than 90% of patients with pulmonary histoplasmosis. [22,43], and about 80% with disseminated disease [37]. Certain. limitations of serologic testing, however, should be recognized. First, 2 to 6. weeks are required for antibody production. Second, serologic tests are less. sensitive in immunosuppressed patients and titers are lower [25,38]. Third, positive serologic tests may result from prior infection and incorrectly suggest. active histoplasmosis in patients with other diseases. Background rates. of seropositivity range from 0.5% by ID to 4% by CF. Finally, antibodies to. H capsulatum may be elevated in patients with other fungal infections, most. commonly blastomycosis, coccidioidomycosis, and paracoccidioidomycosis. [44]. The CF test is more sensitive than the ID test [43]. In acute pulmonary. histoplasmosis, the CF test is positive (titers1:8) in 90% of patients, whereas. ID reveals M bands in 76% and H bands in only 23% [38,43]. CF assays, however, seem to be less specific than ID assays. Cross-reactions with other. fungal infections occur in 5% of cases by ID, 18% by CF, and 49% by radioimmunoassay. [45]. Antibody titers decline following self-limited infection, reaching low or undetectable levels in 2 to 5 years [43]. Antibody levels often. remain high in those with chronic pulmonary infection [17], progressive. disseminated disease [22], or fibrosing mediastinitis. L. Joseph Wheat, Carol A. Kauffman. Histoplasmosis. Infect Dis Clin N Am 17 (2003) 1–19.")
57
Laboratorio diseminación: Anemia leucopenia trombocitopenia
Aumento enzimas hepáticas y bilirrubina Aumento LDH y ferritina Hipercalcemia Laboratory findings suggestive of disseminated histoplasmosis Laboratory evidence for disseminated disease includes anemia, leukopenia, thrombocytopenia, and elevations of hepatic enzymes and bilirubin. Marked lactate dehydrogenase [30] and ferritin elevations [31] have been reported but these findings are not specific for histoplasmosis. Hypercalcemia also has been reported and can be complicated by renal failure. L. Joseph Wheat, Carol A. Kauffman. Histoplasmosis. Infect Dis Clin N Am 17 (2003) 1–19
 1–19.")
58
Tratamiento Mayoría asintomáticos, con resolución espontánea
Tratamiento antifúngico infección crónica pulmonar y diseminada Treatment Most cases of histoplasmosis are asymptomatic or clinically self-limited and do not require treatment with antifungal agents. Patients who have chronic pulmonary or disseminated infection, however, require treatment with antifungal agents (Table 4). Some of the recommendations in this and other reviews [46–48] are based on opinion and experience rather than clinical investigation (Table 5). Guidelines from the Infectious Diseases Society of America for the treatment of histoplasmosis recently have been published [48]. L. Joseph Wheat, Carol A. Kauffman. Histoplasmosis. Infect Dis Clin N Am 17 (2003) 1–19
. Some of the recommendations in this and. other reviews [46–48] are based on opinion and experience rather than. clinical investigation (Table 5). Guidelines from the Infectious Diseases. Society of America for the treatment of histoplasmosis recently have been. published [48]. L. Joseph Wheat, Carol A. Kauffman. Histoplasmosis. Infect Dis Clin N Am 17 (2003) 1–19.")
59
Coccidiomicosis Endémica Sudeste Estados Unidos, México y Susamérica y centroamérica Linfonodos hiliares y mediastínicos principalmente comprometidos Coccidioidomycosis is endemic in the south west USA, Mexico and Central and South America. The lymph nodes most commonly involved are the mediastinal and hilar lymph nodes. When there is involvement of the scalene or supraclavicular nodes, the organism can be isolated from these sites

60
Sarcoidosis

61
Enfermedad granulomatosa multisistémica Causa desconocida
Típico linfadenopatías hiliares simétricas bilaterales, usualmente adenopatías paratraqueales Raro linfadenopatías periféricas Forma leve hallazgo radiológico asintomático TAC detecta linfonodo mediatino anterior y subcarinal, no detectados por Rx tórax Biopsia tejido pulmonar más específico que linfonodo (generalmente sin granuloma específico) Sarcoidosis is a multisystem granulomatous disease of unknown etiology. Bilateral symmetric hilar lymphadenopathy, usually with paratracheal adenopathy, is characteristic. Peripheral lymphadenopathy is rare. In the mild form of the disease (radiologic grading stage 1) mediastinal or hilar lymphadenopathy is usually discovered inadvertently in asymptomatic persons undergoing a chest radiography for an unrelated cause. Computerized tomography scanning can detect anterior mediastinal and subcarinal lymph nodes that are undetected by chest radiography. Biopsy of lung tissue, even without radiologic findings, is superior for histopathologic diagnosis to lymph node biopsy because it has a higher specificity. The lymph node often shows only non-specific granuloma and therefore has a low diagnostic yield.[44]
 Sarcoidosis is a multisystem granulomatous disease of unknown etiology. Bilateral symmetric hilar lymphadenopathy, usually with paratracheal adenopathy, is characteristic. Peripheral lymphadenopathy is rare. In the mild form of the disease (radiologic grading stage 1) mediastinal or hilar lymphadenopathy is usually discovered inadvertently in asymptomatic persons undergoing a chest radiography for an unrelated cause. Computerized tomography scanning can detect anterior mediastinal and subcarinal lymph nodes that are undetected by chest radiography. Biopsy of lung tissue, even without radiologic findings, is superior for histopathologic diagnosis to lymph node biopsy because it has a higher specificity. The lymph node often shows only non-specific granuloma and therefore has a low diagnostic yield.[44]")
62
Exámenes pendientes Muestra en estudio micología
Tinción Warthin-Starry Bartonella Cultivo Koch Serología Bartonella Hensellae (por evaluar) Estudio Enf autoinmunes ¿SUGIEREN ALGO NUEVO?
 Estudio Enf autoinmunes. ¿SUGIEREN ALGO NUEVO")
63
FIN Eco cardiaca Exs pendientes cultivo koch (+) hasta ahora exs inmunologicos
 hasta ahora exs inmunologicos")
Presentaciones similares