Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Anticuerpos Monoclonales contra el EFGR
V Jornada Growing Up Tratamiento dirigido a diana: eficacia y toxicidad Anticuerpos Monoclonales contra el EFGR Dra. María Verónica Pereira Díaz, R4 Tutora: Dra. Laura Vidal Servicio de Oncología Médica Hospital Clínic de Barcelona 22 Enero 2012

2
Outline EGFR signalling pathway Monoclonal antibodies Cetuximab
Panitumumab Indicaciones clínicas EFGR mAB in colorectal cancer EGFR mAB in head and neck cancer Toxicidades y su manejo

4
b-celulina EGF TGFa Amfiregulina HB-EGF Heregulinas -celulina NRG2
Ligandos Heregulinas Dominio extracelular Membrana Dominio Tirosín- kinasa EGFR HER2 HER3 HER4

5
The Development of Monoclonal Antibodies
100% Mouse Protein Mouse ~34% Mouse Protein Chimeric ~10% Mouse Protein Humanized Fully Human 100% Human Protein cetuximab panitumumab (IgG1) (IgG2) Yang XD, et al. Crit Rev Oncol Hematol 2001;38:17-23.
 (IgG2) Yang XD, et al. Crit Rev Oncol Hematol 2001;38:")
6
Panitumumab Inhibits Ligand Binding to EGFR and Dimerization
Inhibition of EGF binding to EGFR EGF, TGFα or other ligands binding to EGFR Panitumumab A fully human lgG2 monoclonal antibody to EGFR High affinity, KD = 5 x M Inhibits ligand-induced EGFR tyrosine phosphorylation This may lead to: Cell proliferation Cell survival Angiogenesis Metastatic spread 1. Yang XD, et al. Crit Rev Oncol Hematol. 2001;38(1): Foon KA, et al. Int J Radiat Oncol Biol Phys. 2004;58(3):
: Foon KA, et al. Int J Radiat Oncol Biol Phys. 2004;58(3):")
11
Potential relationship between KRAS status and response to epidermal growth factor receptor (EGFR) monoclonal antibodies, alone or in combination with irinotecan, in chemotherapy-refractive patients. Wong R , Cunningham D JCO 2008;26: ©2008 by American Society of Clinical Oncology

13
Recent developments with Erbitux: Recurrent and/or metastatic SCCHN
EXTREME study: Erbitux + platinum/5-FU in first line recurrent and/or metastatic SCCHN Primary endpoint (OS) was met Significant improvements in OS, PFS and response rate Addition of Erbitux did not adversely influence QoL Breakthrough advances Erbitux + platinum/5-FU is the first systemic treatment to show an overall benefit over platinum/5-FU alone in recurrent and/or metastatic SCCHN
 was met. Significant improvements in OS, PFS and response rate. Addition of Erbitux did not adversely influence QoL. Breakthrough advances. Erbitux + platinum/5-FU is the first systemic treatment to show an overall benefit over platinum/5-FU alone in recurrent and/or metastatic SCCHN.")
14
EGFR is a potent mediator of radioresistance
Posibles mecanismos1-3: Upregulation of Bcl-2 (down-regulation of apoptotic response induced by RT [or CT]) Upregulation of DNA repair mechanisms (repair of potential lethal damage RT [or CT] induced) Upregulation of cyclin D activating cell proliferation (enlarging proportion of cells in radioresistant phase of cell cycle) Blockade of EGFR signal transduction increases RT activity4 and enhances apoptotic response5 CT, chemotherapy 1 Ke Liang MS, et al. Int J Radiat Oncol Biol Phys 2003;57:246–254;2 Mendelshon J. J Clin Oncol 2002;20:1s–13s; 3 Ochs J. Int J Radiat Oncol Biol Phys 2004;58:941–949 4 Huang S-M, et al. Clin Cancer Res 2000;6:2166–2174; 5 Harari P, et al. Int J Rad Oncol 2001:49;427–433
 Upregulation of DNA repair mechanisms (repair of potential lethal damage RT [or CT] induced) Upregulation of cyclin D activating cell proliferation (enlarging proportion of cells in radioresistant phase of cell cycle) Blockade of EGFR signal transduction increases RT activity4 and enhances apoptotic response5. CT, chemotherapy. 1 Ke Liang MS, et al. Int J Radiat Oncol Biol Phys 2003;57:246–254;2 Mendelshon J. J Clin Oncol 2002;20:1s–13s; 3 Ochs J. Int J Radiat Oncol Biol Phys 2004;58:941– Huang S-M, et al. Clin Cancer Res 2000;6:2166–2174; 5 Harari P, et al. Int J Rad Oncol 2001:49;427–433.")
15
Erbitux + RT in locally advanced SCCHN: Phase III study design
RT (n=213) Stage III and IV non-metastatic SCCHN (n=424) R Erbitux + RT (n=211) Erbitux initial dose (400 mg/m2) 1 week before RT Erbitux (250 mg/m2) + RT (weeks 2–8)b Stratified by KPS Nodal involvement Tumor stage RT regimena Primary endpoint: Duration of locoregional control Secondary endpoints: OS, PFS, RR, and safety aInvestigators’ choice; bUAB regimen: Robert F. J Clin Oncol (2001) Bonner J, et al. N Engl J Med 2006;354:567–578
 Stage III and IV non-metastatic SCCHN. (n=424) R. Erbitux + RT (n=211) Erbitux initial dose (400 mg/m2) 1 week before RT. Erbitux (250 mg/m2) + RT (weeks 2–8)b. Stratified by. KPS. Nodal involvement. Tumor stage. RT regimena. Primary endpoint: Duration of locoregional control. Secondary endpoints: OS, PFS, RR, and safety. aInvestigators’ choice; bUAB regimen: Robert F. J Clin Oncol (2001) Bonner J, et al. N Engl J Med 2006;354:567–578.")
16
Erbitux in locoregionally advanced SCCHN: Efficacy summary
Erbitux + RT demonstrated significant efficacy benefits over RT alone 20-month increase in median survival 26% reduction in risk of death 10-month increase in median locoregional control 32% reduction in locoregional relapse Bonner J, et al. N Engl J Med 2006;354:567–578

17
Toxicidad por anti EGFR monoclonal antibodies
Frecuencia Efecto adverso >10% Hipomagnesemia Aumento en los niveles de enzimas hepáticas Reacciones cutáneas Reacciones leves o moderadas en la perfusión 1-10% Deshidratación Hipocalcemia Cefalea Conjuntivitis Diarrea, náuseas, vómitos, anorexia. Reacciones graves relacionadas con la perfusión. Cansancio <1% Blefaritis, queratitis. TVP, TEP.

18
ERUPCIÓN CUTÁNEA ACNEIFORME
Grado Lesión Extensión Síntomas AVD Infección Grado 1 pápulas / pústulas <10% +/- prurito / hiperestesia Grado 2 10-30% Dificulta instrumentales Grado 3 >30% Dificulta básicas Local: atb tópicos Grado 4 cualquiera Extendida: atb iv

19
ERUPCIÓN CUTÁNEA ACNEIFORME
1 2 3

20
RECOMENDACIONES GENERALES
Desde una semana antes y durante el tto: Lavado diario con agua tibia (no caliente). Evitar irritantes: NO jabones, perfumes, desodorantes, lociones con alcohol. SÍ: geles de ducha basados en aceites / avena. Uso diario de cremas hidratantes (prevención sequedad). NO aloe vera. Evitar: Exposiciones al sol (hasta 3 meses después del tto). Afeitado con navaja (maquinilla eléctrica). Tintes de cabello con amoniaco.
. Evitar irritantes: NO jabones, perfumes, desodorantes, lociones con alcohol. SÍ: geles de ducha basados en aceites / avena. Uso diario de cremas hidratantes (prevención sequedad). NO aloe vera. Evitar: Exposiciones al sol (hasta 3 meses después del tto). Afeitado con navaja (maquinilla eléctrica). Tintes de cabello con amoniaco.")
22
MODIFICACIÓN DOSIS

23
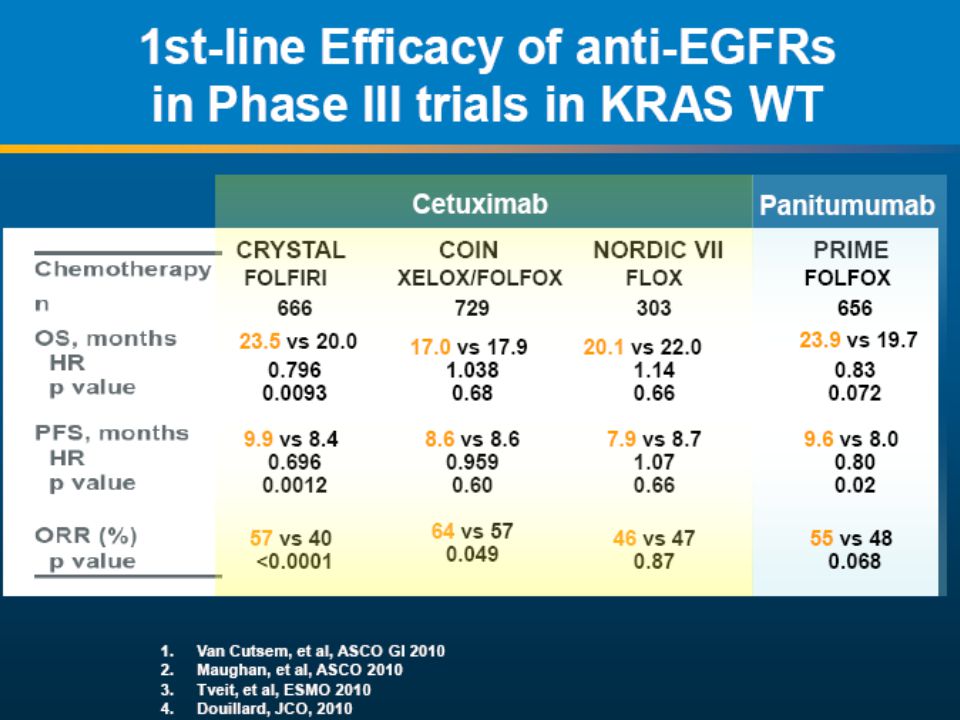
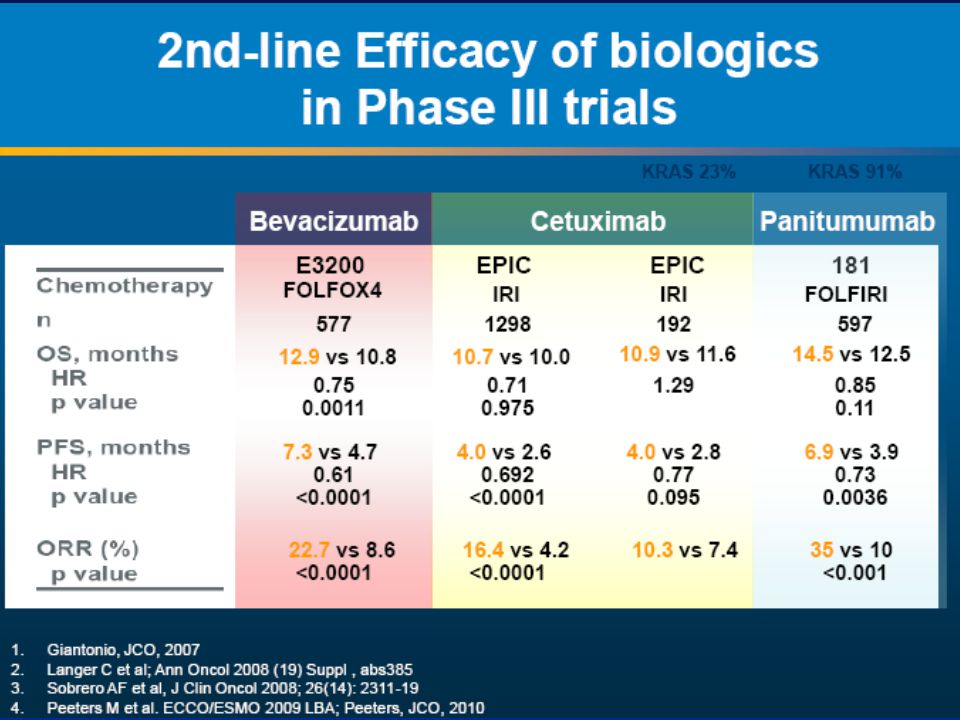
CONCLUSIONES I EGFR juega un papel importante en la regulación de múltiples mecanismos de subsistencia tumoral y su expresión esta asociada con un peor pronóstico. En CCR avanzado se ha demostrado el beneficio de los anticuerpos monoclonales Cetuximab y Panitumumab en pacientes KRAS wt ( factor predictivo). Es de practica clínica habitual la determinación del estado de KRAS en pacientes con CCR avanzado.
. Es de practica clínica habitual la determinación del estado de KRAS en pacientes con CCR avanzado.")
24
CONCLUSIONES II En carcinoma de cabeza y cuello avanzado se ha demostrado la eficacia del Cetuximab en regímes basados en platino. No existe marcador predictivo de respuesta. El rush acneiforme es una toxicidad característica de estoa agentes y en CCR avanzado se asocia a mayor beneficio clínico. Un manejo adecuado de las toxicidades permite menos interrupciones en el tratamiento.

25
MUCHAS GRACIAS!

Presentaciones similares





















 El inhibidor tirosina quinasa multidiana AEE788 ejerce efectos antiproliferativos en células de cáncer de colon mutadas.>")


