Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Curso Anual Modulado SOGIBA 2006
¿Cuándo decimos que estamos frente a un RCIU? Dra. Graciela Scagliotti

2
Epidemiología 3 a 10% de los embarazos
33% del total de RN con BPN (< de 2500 gr.) 20% mortalidad fetal RR de mortalidad perinatal 4 a 8 veces Nivel socio-económico Primera causa en paises pobres: malnutrición materna 50% morbilidad grave o a largo plazo
 20% mortalidad fetal. RR de mortalidad perinatal 4 a 8 veces. Nivel socio-económico. Primera causa en paises pobres: malnutrición materna. 50% morbilidad grave o a largo plazo.")
3
Conceptos actuales acerca de crecimiento fetal
El crecimiento intrauterino es la expresión integrada de las funciones maternas y la información genética fetal, moduladas en la placentación La madre recibe un programa genético fetal constituído por cromosomas maternos y paternos, e intenta cumplirlo a través del funcionamiento placentario. “Puede fallar”…. Respuesta: RCIU

4
Patrón de crecimiento intrauterino normal
Estadío I (Hiperplasia) - 4 a 20 semanas - Mitosis rápidas - Incremento del contenido de ADN Estadío II (Hiperplasia más Hipertrofia) - 20 a 28 semanas - Declinación del n° de mitosis. - Incremento del tamaño de las células.
 - 4 a 20 semanas. - Mitosis rápidas. - Incremento del contenido de ADN. Estadío II (Hiperplasia más Hipertrofia) - 20 a 28 semanas. - Declinación del n° de mitosis. - Incremento del tamaño de las células.")
5
Patrón de crecimiento intrauterino normal
Estadío III ( Hipertrofia) - 28 a 40 semanas - Rápido incremento del tamaño celular. - Rápida acumulación de tejido graso, muscular y conectivo . El 95% de la ganancia del peso fetal ocurre durante las últimas 20 semanas de gestación.
 - 28 a 40 semanas. - Rápido incremento del tamaño celular. - Rápida acumulación de tejido graso, muscular y conectivo . El 95% de la ganancia del peso fetal ocurre durante las últimas 20 semanas de gestación.")
6
Definición de RCIU El RCIU es la consecuencia de la supresión del potencial genético de crecimiento fetal, que ocurre como respuesta a la reducción del aporte de sustratos, o a noxas genéticas, tóxicas o infecciosas. RCIU implica una restricción anormal del crecimiento en el feto que tiene un potencial de desarrollo mayor. Se excluye deliberadamente a aquellos fetos que son pequeños para la edad gestacional (PEG)
")
7
PEG Los PEG son aquellos que crecen en el P10, o por debajo de éste
No todos los fetos que crecen debajo del P10 son patológicos (constitucionalmente pequeños) No todos los fetos que crecen por encima del P10 han podido desarrollar su potencial desarrollo
 No todos los fetos que crecen por encima del P10 han podido desarrollar su potencial desarrollo.")
8
Percentiles ajustados (cm)
Amenorrea (sem) Número de mediciones Percentiles ajustados (cm) 10 50 90 23 26 19 21,5 24,5 24 30 20 22,5 25,25 25 29 20,5 23,5 47 27 57 25,5 28 26,5 29,25 68 27,75 30,25 89 28,75 31,25 31 80 26,25 29,5 32,25 32 64 27,25 30,5 33,25 33 114 34,25 34 101 35 121 29,75 32,75 36 125 33,50 36,75 37 146 37,25 38 115 31,5 37,5 39 34,5 40 51 38,5 41 Fuente: CLAP. 2001
 Número de mediciones. Percentiles ajustados (cm) ,5. 24, ,5. 25, ,5. 23, , ,5. 29, ,75. 30, ,75. 31, ,25. 29,5. 32, ,25. 30,5. 33, , ,75. 32, ,50. 36, , ,5. 37, , , Fuente: CLAP")
9
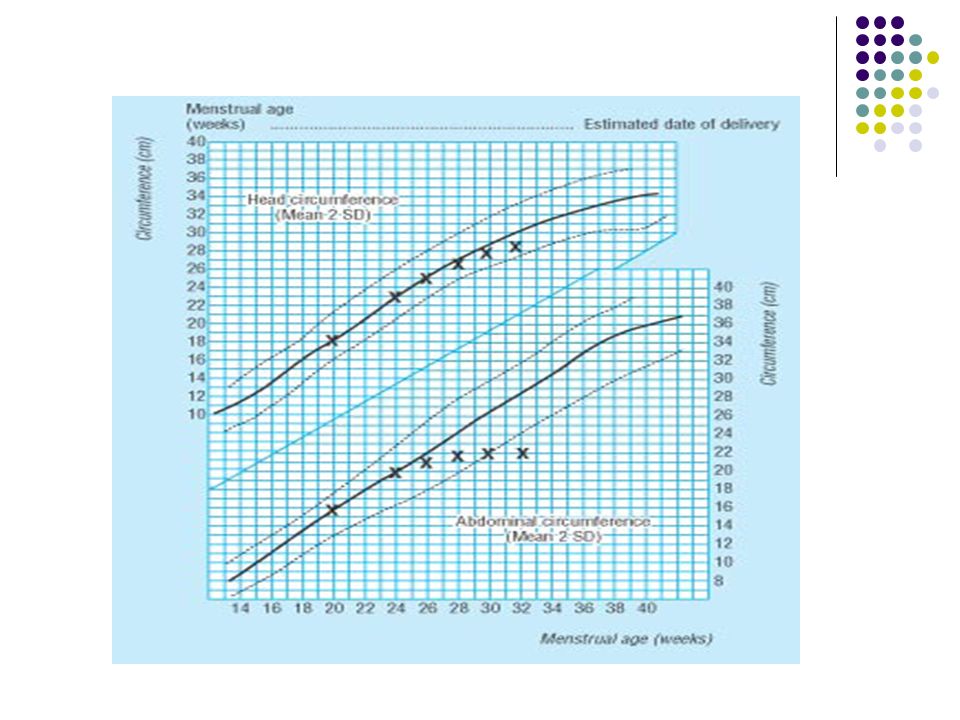
Diagnóstico Pre-requisito conocer la edad gestacional con seguridad.
Altura uterina US precoz Diámetro biparietal Circunferencia abdominal HC/AC Longitud femur Morfología placentaria y líquido amniótico IUGR can be difficult to diagnose and in many cases doctors are not able to make an exact diagnosis until the baby is born. A mother who has had a growth restricted baby is at risk of having another during a later pregnancy. Such mothers are closely monitored during pregnancy. The length in weeks of the pregnancy must be carefully determined so that the doctor will know if development and weight gain are appropriate. Checking the mother's weight and abdomen measurements can help diagnose cases when there are no other risk factors present. Measuring the girth of the abdomen is often used as a tool for diagnosing IUGR. During pregnancy, the healthcare provider will use a tape measure to record the height of the upper portion of the uterus (the uterine fundal height). As the pregnancy continues and the baby grows, the uterus stretches upward in the direction of the mother's head. Between 18 and 30 weeks of gestation, the uterine fundal height (in cm.) equals the weeks of gestation. If the uterine fundal height is more than 2-3 cm below normal, then IUGR is suspected. Ultrasound is used to evaluate the growth of the baby. Usually, IUGR is diagnosed after week 32 of pregnancy. This is during the phase of rapid growth when the baby should be gaining more weight. IUGR caused by genetic factors or infection may sometimes be detected earlier.
. As the pregnancy continues and the baby grows, the uterus stretches upward in the direction of the mother s head. Between 18 and 30 weeks of gestation, the uterine fundal height (in cm.) equals the weeks of gestation. If the uterine fundal height is more than 2-3 cm below normal, then IUGR is suspected. Ultrasound is used to evaluate the growth of the baby. Usually, IUGR is diagnosed after week 32 of pregnancy. This is during the phase of rapid growth when the baby should be gaining more weight. IUGR caused by genetic factors or infection may sometimes be detected earlier.")
11
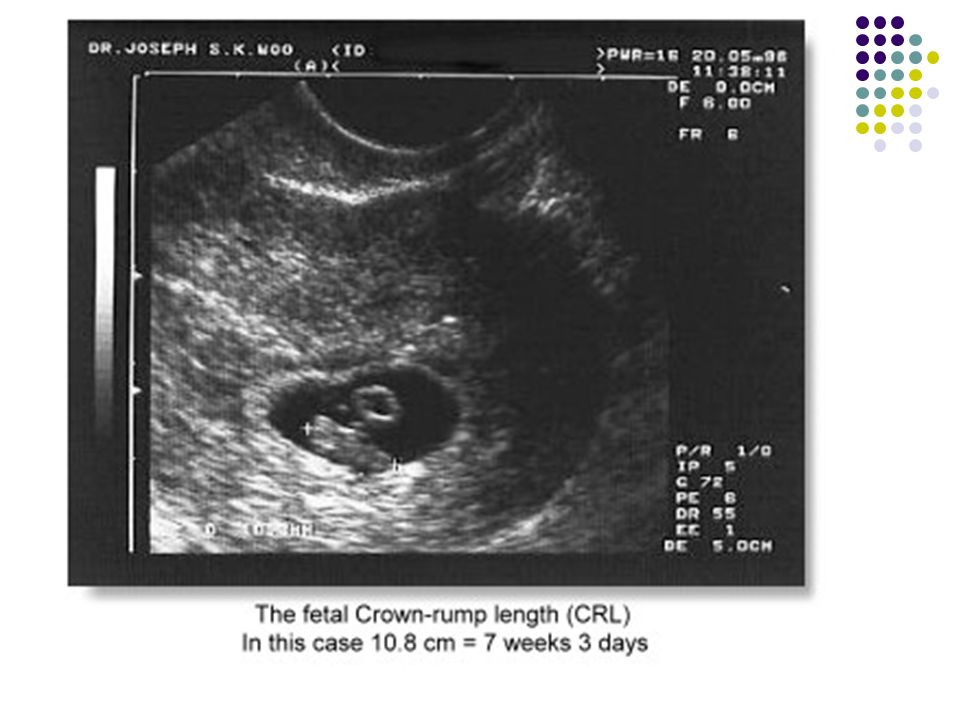
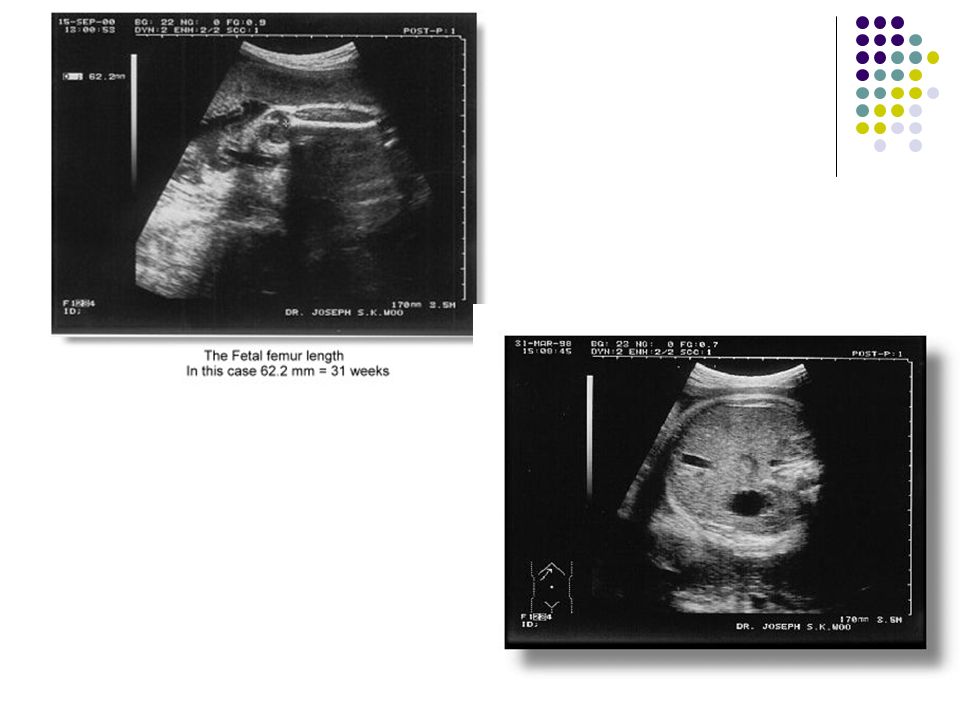
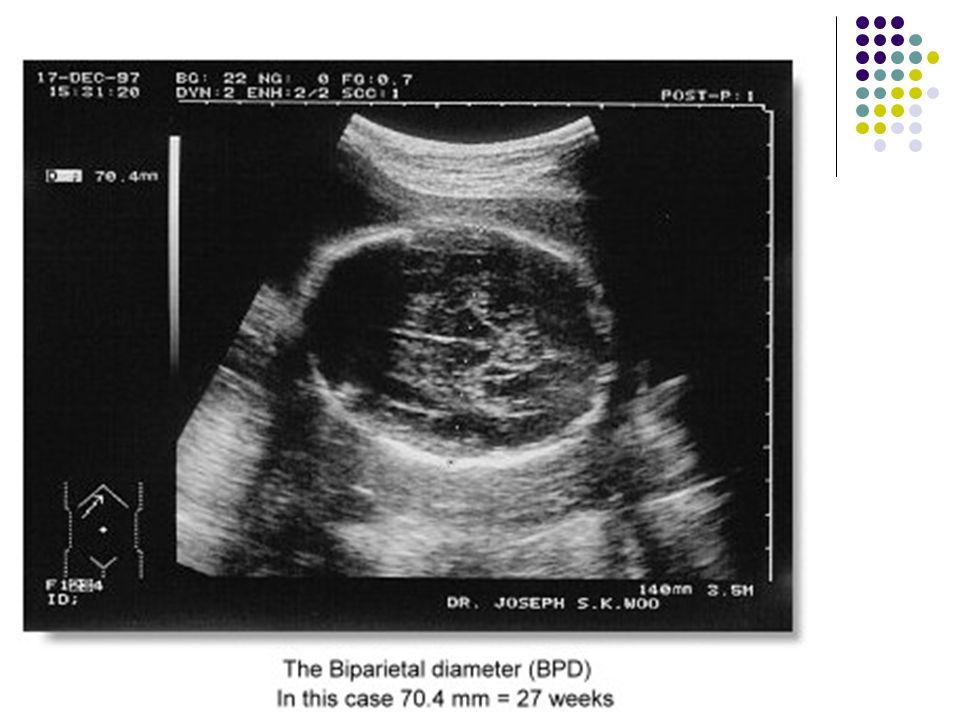
Fidelidad del US Antes de las 14 semanas de gestación la longitud céfalo-caudal tiene un rango de error de 2,7 - 4,7 días. posteriormente, y hasta las 20 semanas, el DBP y fémur tienen un margen de error de 7 días. Entre las 20 y 30 semanas las mismas mediciones ofrecen un margen de 14 días. Entre las 30 y 40 semanas, 21 días.

12
Etiología . In developed countries, cigarette smoking is far and away the most important etiologic determinant, but low gestational weight gain and low pre-pregnancy BMI are also determinants. The etiologic roles of pre-eclampsia, short stature, genetic factors, and alcohol and drug use during pregnancy are well-established but quantitatively less important. Socioeconomic disparities in IUGR risk within developed countries are largely attributable to socioeconomic gradients in smoking, weight gain and maternal stature. In poor urban areas where cocaine abuse is highly prevalent, this may also be important. The etiologic role of micronutrients in IUGR remains to be clarified. The best evidence concerning their importance derives from randomized trials and from systematic overviews of those trials contained in the Cochrane Collaboration Pregnancy and Childbirth database. Unfortunately, there are few supplementation or fortification trials in developing country settings where deficiencies in these micronutrients are prevalent. Trials are required to define the possible etiologic roles of iron, calcium, vitamin D, and vitamin A, especially in developing countries. The evidence concerning folate, magnesium, and zinc also looks sufficiently promising to justify further investigation.

13
Factores maternos RCIU en embarazo previo. Edades extremas de la vida.
Peso y talla materna bajos. Mala nutrición e inadecuada ganancia ponderal durante el embarazo. Bajo nivel socio-económico. Uso de sustancias asociadas a desarrollo anormal o defectos congénitos: narcóticos, alcohol, anticoagulantes, anticonvulsivantes o el hábito de fumar. The physiologic and molecular mechanisms by which nutritional or other determinants affect fetal growth are incompletely understood. Growth is determined not only by substrate availability but also by the integrity of physiologic processes necessary to ensure transfer of nutrients and oxygen to the developing fetus. Expansion of maternal plasma volume, maintenance of uterine blood flow, and development of adequate placentation are key physiologic mechanisms required for optimal fetal growth. All substances used by the fetus are transported by the placenta: some (like oxygen and most other gases) by passive diffusion, others by facilitated transport proteins (e.g., Glut 1 for glucose), and still others (e.g., amino acids) by active energy-dependent transport processes. Insulin-like growth factors (IGFs) are important mediators of substrate incorporation into fetal tissue. IGF1 appears to induce cell differentiation, including (perhaps) oligodendrocyte development in the brain, whereas IGF2 may function to stimulate mitosis. It remains uncertain whether these physiologic and molecular mechanisms are merely the final common pathways for genetic or environmental determinants of IUGR, or whether they themselves vary (favorably or pathologically) independently of those determinants. Fuente: Prof. Dra. Liliana Voto
 by passive diffusion, others by facilitated transport proteins (e.g., Glut 1 for glucose), and still others (e.g., amino acids) by active energy-dependent transport processes. Insulin-like growth factors (IGFs) are important mediators of substrate incorporation into fetal tissue. IGF1 appears to induce cell differentiation, including (perhaps) oligodendrocyte development in the brain, whereas IGF2 may function to stimulate mitosis. It remains uncertain whether these physiologic and molecular mechanisms are merely the final common pathways for genetic or environmental determinants of IUGR, or whether they themselves vary (favorably or pathologically) independently of those determinants. Fuente: Prof. Dra. Liliana Voto.")
14
Factores maternos Embarazo múltiple. Altitud sobre el nivel del mar.
Enfermedades como -preeclampsia, hipertensión, enfermedad cardiaca cianótica o Gr III y IV, diabetes con lesiones vasculares. Enfermedad crónica renal Infecciones - rubeola, citomegalovirus, varicela, herpes simple, parvo virus B19, tuberculosis, sífilis, malaria. Autoanticuerpos: sindrome de anticuerpos antifosfolípidos, lupus eritematoso sistémico. Hemoglobinopatías. Most of the evidence on etiologic determinants is based on observational studies and systematic overviews or meta-analyses of such studies. In developing countries, the major determinants of IUGR are nutritional: low gestational weight gain (primarily due to inadequate energy intake), low pre-pregnancy BMI (reflecting chronic maternal undernutrition), and short maternal stature (principally due to undernutrition and infection during childhood). Gastroenteritis, intestinal parasitosis, and respiratory infections are prevalent in developing countries and may also have an important impact. Malaria is a major determinant in countries where that disease is endemic. Cigarette smoking is an increasingly important factor in some settings. In developed countries, cigarette smoking is far and away the most important etiologic determinant, but low gestational weight gain and low pre-pregnancy BMI are also determinants. The etiologic roles of pre-eclampsia, short stature, genetic factors, and alcohol and drug use during pregnancy are well-established but quantitatively less important. Socioeconomic disparities in IUGR risk within developed countries are largely attributable to socioeconomic gradients in smoking, weight gain and maternal stature. In poor urban areas where cocaine abuse is highly prevalent, this may also be important. Fuente: Prof. Dra. Liliana Voto
, low pre-pregnancy BMI (reflecting chronic maternal undernutrition), and short maternal stature (principally due to undernutrition and infection during childhood). Gastroenteritis, intestinal parasitosis, and respiratory infections are prevalent in developing countries and may also have an important impact. Malaria is a major determinant in countries where that disease is endemic. Cigarette smoking is an increasingly important factor in some settings. In developed countries, cigarette smoking is far and away the most important etiologic determinant, but low gestational weight gain and low pre-pregnancy BMI are also determinants. The etiologic roles of pre-eclampsia, short stature, genetic factors, and alcohol and drug use during pregnancy are well-established but quantitatively less important. Socioeconomic disparities in IUGR risk within developed countries are largely attributable to socioeconomic gradients in smoking, weight gain and maternal stature. In poor urban areas where cocaine abuse is highly prevalent, this may also be important. Fuente: Prof. Dra. Liliana Voto.")
15
Factores Placentarios
Insuficiencia útero-placentaria- Inadecuada invasión y placentación trofoblástica durante el primer trimestre de la gestación. Reducido flujo sanguíneo materno en el lecho placentario. Insuficiencia feto-placentaria Anormalidades vasculares del cordón y la placenta. Disminución de la funcionalidad de placenta- Mosaico placentario, desprendimiento de placenta, placenta previa, embarazo de post-termino. The etiologic role of micronutrients in IUGR remains to be clarified. The best evidence concerning their importance derives from randomized trials and from systematic overviews of those trials contained in the Cochrane Collaboration Pregnancy and Childbirth database. Unfortunately, there are few supplementation or fortification trials in developing country settings where deficiencies in these micronutrients are prevalent. Trials are required to define the possible etiologic roles of iron, calcium, vitamin D, and vitamin A, especially in developing countries. The evidence concerning folate, magnesium, and zinc also looks sufficiently promising to justify further investigation. The physiologic and molecular mechanisms by which nutritional or other determinants affect fetal growth are incompletely understood. Growth is determined not only by substrate availability but also by the integrity of physiologic processes necessary to ensure transfer of nutrients and oxygen to the developing fetus. Expansion of maternal plasma volume, maintenance of uterine blood flow, and development of adequate placentation are key physiologic mechanisms required for optimal fetal growth. All substances used by the fetus are transported by the placenta: some (like oxygen and most other gases) by passive diffusion, others by facilitated transport proteins (e.g., Glut 1 for glucose), and still others (e.g., amino acids) by active energy-dependent transport processes. Insulin-like growth factors (IGFs) are important mediators of substrate incorporation into fetal tissue. IGF1 appears to induce cell differentiation, including (perhaps) oligodendrocyte development in the brain, whereas IGF2 may function to stimulate mitosis. It remains uncertain whether these physiologic and molecular mechanisms are merely the final common pathways for genetic or environmental determinants of IUGR, or whether they themselves vary (favorably or pathologically) independently of those determinants. Fuente: Prof. Dra. Liliana Voto
 by passive diffusion, others by facilitated transport proteins (e.g., Glut 1 for glucose), and still others (e.g., amino acids) by active energy-dependent transport processes. Insulin-like growth factors (IGFs) are important mediators of substrate incorporation into fetal tissue. IGF1 appears to induce cell differentiation, including (perhaps) oligodendrocyte development in the brain, whereas IGF2 may function to stimulate mitosis. It remains uncertain whether these physiologic and molecular mechanisms are merely the final common pathways for genetic or environmental determinants of IUGR, or whether they themselves vary (favorably or pathologically) independently of those determinants. Fuente: Prof. Dra. Liliana Voto.")
16
Factores de origen fetal
Exposición a una infección: rubeola, citomegalovirus, herpes simplex, tuberculosis, sífilis, toxoplasmosis, malaria, parvo virus B19. Defectos congénitos: cardiovascular, renal, anencefalia, defecto de los miembros. 19% de los fetos con AC y peso fetal < del percentilo 5 tienen un defecto cromosómico: trisomia 18 (sindrome Edward), 21( sindrome Down), 16, 13, XO (sindrome de Turner) 4p- sindrome, 5p sindrome,13q, 18p, 18q sindromes Enfermedad primaria de hueso o cartílago. Sindrome tanatofórico The etiologic role of micronutrients in IUGR remains to be clarified. The best evidence concerning their importance derives from randomized trials and from systematic overviews of those trials contained in the Cochrane Collaboration Pregnancy and Childbirth database. Unfortunately, there are few supplementation or fortification trials in developing country settings where deficiencies in these micronutrients are prevalent. Trials are required to define the possible etiologic roles of iron, calcium, vitamin D, and vitamin A, especially in developing countries. The evidence concerning folate, magnesium, and zinc also looks sufficiently promising to justify further investigation. The physiologic and molecular mechanisms by which nutritional or other determinants affect fetal growth are incompletely understood. Growth is determined not only by substrate availability but also by the integrity of physiologic processes necessary to ensure transfer of nutrients and oxygen to the developing fetus. Expansion of maternal plasma volume, maintenance of uterine blood flow, and development of adequate placentation are key physiologic mechanisms required for optimal fetal growth. All substances used by the fetus are transported by the placenta: some (like oxygen and most other gases) by passive diffusion, others by facilitated transport proteins (e.g., Glut 1 for glucose), and still others (e.g., amino acids) by active energy-dependent transport processes. Insulin-like growth factors (IGFs) are important mediators of substrate incorporation into fetal tissue. IGF1 appears to induce cell differentiation, including (perhaps) oligodendrocyte development in the brain, whereas IGF2 may function to stimulate mitosis. It remains uncertain whether these physiologic and molecular mechanisms are merely the final common pathways for genetic or environmental determinants of IUGR, or whether they themselves vary (favorably or pathologically) independently of those determinants. modif. Prof. Dra. Liliana Voto
, 21( sindrome Down), 16, 13, XO (sindrome de Turner) 4p- sindrome, 5p sindrome,13q, 18p, 18q sindromes. Enfermedad primaria de hueso o cartílago. Sindrome tanatofórico. The etiologic role of micronutrients in IUGR remains to be clarified. The best evidence concerning their importance derives from randomized trials and from systematic overviews of those trials contained in the Cochrane Collaboration Pregnancy and Childbirth database. Unfortunately, there are few supplementation or fortification trials in developing country settings where deficiencies in these micronutrients are prevalent. Trials are required to define the possible etiologic roles of iron, calcium, vitamin D, and vitamin A, especially in developing countries. The evidence concerning folate, magnesium, and zinc also looks sufficiently promising to justify further investigation. The physiologic and molecular mechanisms by which nutritional or other determinants affect fetal growth are incompletely understood. Growth is determined not only by substrate availability but also by the integrity of physiologic processes necessary to ensure transfer of nutrients and oxygen to the developing fetus. Expansion of maternal plasma volume, maintenance of uterine blood flow, and development of adequate placentation are key physiologic mechanisms required for optimal fetal growth. All substances used by the fetus are transported by the placenta: some (like oxygen and most other gases) by passive diffusion, others by facilitated transport proteins (e.g., Glut 1 for glucose), and still others (e.g., amino acids) by active energy-dependent transport processes. Insulin-like growth factors (IGFs) are important mediators of substrate incorporation into fetal tissue. IGF1 appears to induce cell differentiation, including (perhaps) oligodendrocyte development in the brain, whereas IGF2 may function to stimulate mitosis. It remains uncertain whether these physiologic and molecular mechanisms are merely the final common pathways for genetic or environmental determinants of IUGR, or whether they themselves vary (favorably or pathologically) independently of those determinants. modif. Prof. Dra. Liliana Voto.")
17
Cariotipo Sme. de Edwards

18
Deleción 4p

19
Sindrome tanatofórico
GScagliotti, NGómez y col: SOGIBA 2005

20
Gold Standard (Lejarraga y Capurro)
US en RCIU Gold Standard (Lejarraga y Capurro) U.S RCIU PAEG TOTAL 181 10 191 49 283 332 230 293 523 Fuente: HGAIP. SOGIBA NGómez, GScagliotti y col.
 U.S. RCIU. PAEG. TOTAL Fuente: HGAIP. SOGIBA NGómez, GScagliotti y col.")
21
Valor Predictivo del US
Sensibilidad: 78,7% Especificidad: 96,5% VPPP: 94,7% VPPN: 85,2% Exactitud: 88,7% Fuente: HGAIP. SOGIBA NGómez, GScagliotti y col.

24
Ecografía y Bienestar Fetal
Métodos propuestos (RCOG-nivel de recomendación) Palpación abdominal. (nivel C) Altura uterina embarazadas Sensibilidad 27% Especificidad 88% No mejora los resultados perinatales (nivel B). IUGR can be difficult to diagnose and in many cases doctors are not able to make an exact diagnosis until the baby is born. A mother who has had a growth restricted baby is at risk of having another during a later pregnancy. Such mothers are closely monitored during pregnancy. The length in weeks of the pregnancy must be carefully determined so that the doctor will know if development and weight gain are appropriate. Checking the mother's weight and abdomen measurements can help diagnose cases when there are no other risk factors present. Measuring the girth of the abdomen is often used as a tool for diagnosing IUGR. During pregnancy, the healthcare provider will use a tape measure to record the height of the upper portion of the uterus (the uterine fundal height). As the pregnancy continues and the baby grows, the uterus stretches upward in the direction of the mother's head. Between 18 and 30 weeks of gestation, the uterine fundal height (in cm.) equals the weeks of gestation. If the uterine fundal height is more than 2-3 cm below normal, then IUGR is suspected. Ultrasound is used to evaluate the growth of the baby. Usually, IUGR is diagnosed after week 32 of pregnancy. This is during the phase of rapid growth when the baby should be gaining more weight. IUGR caused by genetic factors or infection may sometimes be detected earlier. Fuente: Prof. Dra. Liliana Voto
 Palpación abdominal. (nivel C) Altura uterina embarazadas. Sensibilidad 27% Especificidad 88% No mejora los resultados perinatales (nivel B). IUGR can be difficult to diagnose and in many cases doctors are not able to make an exact diagnosis until the baby is born. A mother who has had a growth restricted baby is at risk of having another during a later pregnancy. Such mothers are closely monitored during pregnancy. The length in weeks of the pregnancy must be carefully determined so that the doctor will know if development and weight gain are appropriate. Checking the mother s weight and abdomen measurements can help diagnose cases when there are no other risk factors present. Measuring the girth of the abdomen is often used as a tool for diagnosing IUGR. During pregnancy, the healthcare provider will use a tape measure to record the height of the upper portion of the uterus (the uterine fundal height). As the pregnancy continues and the baby grows, the uterus stretches upward in the direction of the mother s head. Between 18 and 30 weeks of gestation, the uterine fundal height (in cm.) equals the weeks of gestation. If the uterine fundal height is more than 2-3 cm below normal, then IUGR is suspected. Ultrasound is used to evaluate the growth of the baby. Usually, IUGR is diagnosed after week 32 of pregnancy. This is during the phase of rapid growth when the baby should be gaining more weight. IUGR caused by genetic factors or infection may sometimes be detected earlier. Fuente: Prof. Dra. Liliana Voto.")
25
Ecografía y Bienestar Fetal
Métodos propuestos (RCOG-nivel de recomendación) Ultrasonido: Circunferencia abdominal. Alto riesgo-Sensibilidad 73-94% especificidad 51-84% ( nivel B) Las curvas usadas deben adaptarse a las poblaciones de estudio (nivel B). Velocidad de crecimiento. Medidas seriadas (mínimo 2 sem.) (nivel B). HC/AC y FL/AC son peores predictores que el peso o la AC sola. El uso rutinario del ultrasonido en embarazos de bajo riesgo luego de las 24 semanas no mejora los resultados perinatales (nivel A). IUGR can be difficult to diagnose and in many cases doctors are not able to make an exact diagnosis until the baby is born. A mother who has had a growth restricted baby is at risk of having another during a later pregnancy. Such mothers are closely monitored during pregnancy. The length in weeks of the pregnancy must be carefully determined so that the doctor will know if development and weight gain are appropriate. Checking the mother's weight and abdomen measurements can help diagnose cases when there are no other risk factors present. Measuring the girth of the abdomen is often used as a tool for diagnosing IUGR. During pregnancy, the healthcare provider will use a tape measure to record the height of the upper portion of the uterus (the uterine fundal height). As the pregnancy continues and the baby grows, the uterus stretches upward in the direction of the mother's head. Between 18 and 30 weeks of gestation, the uterine fundal height (in cm.) equals the weeks of gestation. If the uterine fundal height is more than 2-3 cm below normal, then IUGR is suspected. Ultrasound is used to evaluate the growth of the baby. Usually, IUGR is diagnosed after week 32 of pregnancy. This is during the phase of rapid growth when the baby should be gaining more weight. IUGR caused by genetic factors or infection may sometimes be detected earlier. Fuente: Prof. Dra. Liliana Voto
 Ultrasonido: Circunferencia abdominal. Alto riesgo-Sensibilidad 73-94% especificidad 51-84% ( nivel B) Las curvas usadas deben adaptarse a las poblaciones de estudio (nivel B). Velocidad de crecimiento. Medidas seriadas (mínimo 2 sem.) (nivel B). HC/AC y FL/AC son peores predictores que el peso o la AC sola. El uso rutinario del ultrasonido en embarazos de bajo riesgo luego de las 24 semanas no mejora los resultados perinatales (nivel A). IUGR can be difficult to diagnose and in many cases doctors are not able to make an exact diagnosis until the baby is born. A mother who has had a growth restricted baby is at risk of having another during a later pregnancy. Such mothers are closely monitored during pregnancy. The length in weeks of the pregnancy must be carefully determined so that the doctor will know if development and weight gain are appropriate. Checking the mother s weight and abdomen measurements can help diagnose cases when there are no other risk factors present. Measuring the girth of the abdomen is often used as a tool for diagnosing IUGR. During pregnancy, the healthcare provider will use a tape measure to record the height of the upper portion of the uterus (the uterine fundal height). As the pregnancy continues and the baby grows, the uterus stretches upward in the direction of the mother s head. Between 18 and 30 weeks of gestation, the uterine fundal height (in cm.) equals the weeks of gestation. If the uterine fundal height is more than 2-3 cm below normal, then IUGR is suspected. Ultrasound is used to evaluate the growth of the baby. Usually, IUGR is diagnosed after week 32 of pregnancy. This is during the phase of rapid growth when the baby should be gaining more weight. IUGR caused by genetic factors or infection may sometimes be detected earlier. Fuente: Prof. Dra. Liliana Voto.")
27
Ecografía y Bienestar Fetal
Monitoreo anteparto (NST) No es un predictor temprano del curso de la enfermedad. (nivel A). No mejora los resultados perinatales Los cambios se producen en etapas tardías del RCIU. El intervalo entre un doppler patológico y un NST anormal es de 1 a 26 días. The effectiveness of other interventions has not been demonstrated, but further research is required based on limited, suggestive results from RCTs. 'Packages' of combined interventions and community-based (cluster randomization) approaches should be explored. Potentially adverse effects of these interventions also require careful assessment. Maternal supplementation of iron, zinc, folate, and magnesium should be rigorously evaluated, as these interventions may affect fetal growth, as well as preterm delivery and necrologic outcomes. It is important to target women deficient in the nutrient of interest to maximize the chance of detecting a beneficial effect. In this regard, the possibility of coexisting nutrient deficiencies limiting fetal growth must be considered. Two trials of iron supplementation conducted in developed countries have shown no effect on IUGR; it remains to be seen whether routine iron supplementation affects IUGR in populations with a high prevalence of anemia. A RTC the effect of vitamin A supplementation during pregnancy is currently under way in Nepal. Unlike food fortification with vitamin A, however, supplementation might have adverse safety implications, and caution is required to avoid teratogenic or other adverse effects. In countries where multiple deficiencies and pathologies exist, it may be difficult to demonstrate a significant effect with a single intervention. For example, malaria and other parasitic infections, malnutrition, and anemia coexist in many developing countries. An appropriate combination of anti-anemic (iron-folate) and antimicrobial/antiparasitic agents tested in population-based trials may have a greater chance of showing a reduction in IUGR. Antibiotic treatment of genito-urinary tract infections appears to be a promising area for perinatal research, although the impact may be greater for preterm delivery than for impaired fetal growth. The efficacy and safety of drug treatment remain to be demonstrated. A few older and methodologically weaker trials of abdominal decompression have reported large reductions in IUGR. In selected developed country settings, strategies to improve blood flow to the uterus may merit further testing. Fuente: Prof. Dra. Liliana Voto
 No es un predictor temprano del curso de la enfermedad. (nivel A). No mejora los resultados perinatales. Los cambios se producen en etapas tardías del RCIU. El intervalo entre un doppler patológico y un NST anormal es de 1 a 26 días. The effectiveness of other interventions has not been demonstrated, but further research is required based on limited, suggestive results from RCTs. Packages of combined interventions and community-based (cluster randomization) approaches should be explored. Potentially adverse effects of these interventions also require careful assessment. Maternal supplementation of iron, zinc, folate, and magnesium should be rigorously evaluated, as these interventions may affect fetal growth, as well as preterm delivery and necrologic outcomes. It is important to target women deficient in the nutrient of interest to maximize the chance of detecting a beneficial effect. In this regard, the possibility of coexisting nutrient deficiencies limiting fetal growth must be considered. Two trials of iron supplementation conducted in developed countries have shown no effect on IUGR; it remains to be seen whether routine iron supplementation affects IUGR in populations with a high prevalence of anemia. A RTC the effect of vitamin A supplementation during pregnancy is currently under way in Nepal. Unlike food fortification with vitamin A, however, supplementation might have adverse safety implications, and caution is required to avoid teratogenic or other adverse effects. In countries where multiple deficiencies and pathologies exist, it may be difficult to demonstrate a significant effect with a single intervention. For example, malaria and other parasitic infections, malnutrition, and anemia coexist in many developing countries. An appropriate combination of anti-anemic (iron-folate) and antimicrobial/antiparasitic agents tested in population-based trials may have a greater chance of showing a reduction in IUGR. Antibiotic treatment of genito-urinary tract infections appears to be a promising area for perinatal research, although the impact may be greater for preterm delivery than for impaired fetal growth. The efficacy and safety of drug treatment remain to be demonstrated. A few older and methodologically weaker trials of abdominal decompression have reported large reductions in IUGR. In selected developed country settings, strategies to improve blood flow to the uterus may merit further testing. Fuente: Prof. Dra. Liliana Voto.")
28
Ecografía y Bienestar Fetal
Indice de líquido amniotico (nivel B) La profundidad vertical de 4 ventanas de líquido amniótico permiten obtener el indice AFI. Una disminución por debajo del percentilo 5 (≤5cm) se asoció a Apgar bajo y a un aumento de la mortalidad perinatal RCTs aimed at other putative causes of IUGR have been disappointing. For example, efforts to prevent and treat hypertensive disorders have not significantly reduced IUGR. Trials using antiplatelet agents in high-risk women have yielded only modest benefits, while trials of betablockers have suggested a potential for harm. Prenatal care and nutritional education interventions have not heretofore been shown to impact significantly on IUGR, but better approaches are required (e.g., community-wide interventions to promote optimal weight gain and discourage 'eating down'). Future research in the prevention and treatment of IUGR should be based on sound epidemiologic and other scientific evidence. Rigorous randomization procedures (including concealment of treatment allocation) and efforts to minimize losses to follow-up fare required to ensure high methodological quality. Without randomization there is a high risk of bias due to confounding. Sample sizes should be planned with sufficient power to detect significant impacts on IUGR and other fetal/infant outcomes. Study designs should also include practical measures to assess gestational age, as well as potential obstetric complications or other adverse outcomes. Lastly, while systematic reviews of RCTs represent the most objective way to evaluate the effectiveness of health care interventions, the available data are limited. Moreover, there are problems related to the size of the trials, their heterogeneity, settings, and methodologic quality. Findings from observational studies should not be totally discounted, but rather tested in RCTs whenever possible. Fuente: Prof. Dra. Liliana Voto
 La profundidad vertical de 4 ventanas de líquido amniótico permiten obtener el indice AFI. Una disminución por debajo del percentilo 5. (≤5cm) se asoció a Apgar bajo y a un aumento de la mortalidad perinatal. RCTs aimed at other putative causes of IUGR have been disappointing. For example, efforts to prevent and treat hypertensive disorders have not significantly reduced IUGR. Trials using antiplatelet agents in high-risk women have yielded only modest benefits, while trials of betablockers have suggested a potential for harm. Prenatal care and nutritional education interventions have not heretofore been shown to impact significantly on IUGR, but better approaches are required (e.g., community-wide interventions to promote optimal weight gain and discourage eating down ). Future research in the prevention and treatment of IUGR should be based on sound epidemiologic and other scientific evidence. Rigorous randomization procedures (including concealment of treatment allocation) and efforts to minimize losses to follow-up fare required to ensure high methodological quality. Without randomization there is a high risk of bias due to confounding. Sample sizes should be planned with sufficient power to detect significant impacts on IUGR and other fetal/infant outcomes. Study designs should also include practical measures to assess gestational age, as well as potential obstetric complications or other adverse outcomes. Lastly, while systematic reviews of RCTs represent the most objective way to evaluate the effectiveness of health care interventions, the available data are limited. Moreover, there are problems related to the size of the trials, their heterogeneity, settings, and methodologic quality. Findings from observational studies should not be totally discounted, but rather tested in RCTs whenever possible. Fuente: Prof. Dra. Liliana Voto.")
29
AFI Las recomendaciones actuales señalan que si AFI disminuye de 8 después de la semana 35, es oportuna la terminación del embarazo.

30
Pequeños para edad gestacional
Fetos pequeños para edad gestacional-normales- sin anormalidades estructurales, líquido amniótico y doppler de arteria umbilical normal pero… bajo peso. Fetos pequeños-anormales- con anormalidades cromosómicas o malformaciones estructurales. Fetos con crecimiento restringido- debido a mal funcionamiento de la placenta, con o sin patología asociada. Fuente: Prof. Dra. Liliana Voto

31
Clasificación Simétrico Asimétrico
La cabeza y el cuerpo son proporcionadamente pequeños. El cerebro es anormalmente grande comparado con el higado. Application of the international foetal growth reference curve will vary according to its specific clinical and public health uses or purposes. Criteria for diagnosis of foetal growth restriction (e.g., SGA) should be related to evidence of increased risk for perinatal mortality and/or other indices of adverse outcomes. The new reference should provide percentiles [(e.g., 3rd, 5th, 10th, 15th, 25th, 50th (median), 75th, 85th, 90th, 95th, and 97th)] as well as z-scores [(e.g., -3, -2, -1, 0 (mean), 1, 2, and 3 SD)], so that health planners and practitioners can use the most appropriate cut off based on local circumstances. Proportionality at birth may be related to adverse outcomes. Thus there is a need to develop reference data for birth length and head circumference in relation to GA, and for birth weight in relation to birth length. Because the concepts of 'wasting' and 'stunting' have proven useful for categorizing undernourished infants and older children, an attempt should be made to quantify the mortality and morbidity risks associated with 'wasted' and 'stunted' newborns and to develop indicators for their classification. En los niños normales el peso del cerebro es 3 veces mayor que el higado. En el RCIU asimétrico, el cerebro puede pesar 5 o 6 veces más que el higado modif.: Prof. Dra. Liliana Voto
 should be related to evidence of increased risk for perinatal mortality and/or other indices of adverse outcomes. The new reference should provide percentiles [(e.g., 3rd, 5th, 10th, 15th, 25th, 50th (median), 75th, 85th, 90th, 95th, and 97th)] as well as z-scores [(e.g., -3, -2, -1, 0 (mean), 1, 2, and 3 SD)], so that health planners and practitioners can use the most appropriate cut off based on local circumstances. Proportionality at birth may be related to adverse outcomes. Thus there is a need to develop reference data for birth length and head circumference in relation to GA, and for birth weight in relation to birth length. Because the concepts of wasting and stunting have proven useful for categorizing undernourished infants and older children, an attempt should be made to quantify the mortality and morbidity risks associated with wasted and stunted newborns and to develop indicators for their classification. En los niños normales el peso del cerebro es 3 veces mayor que el higado. En el RCIU asimétrico, el cerebro puede pesar 5 o 6 veces más que el higado modif.: Prof. Dra. Liliana Voto.")
32
Clasificación RCIU Asimétrico Simétrico
Longitud, peso y CA proporcionados Noxa temprana: comunmente debido a infecciones congénitas, desórdenes genéticos, o factores extrínsecos Índice ponderal normal Bajo riesgo de asfixia perinatal Bajo riesgo de hipoglicemia Asimétrico Aparición tardía, comunmente debido a Insuficiencia placentaria, Desnutrición materna, hipoxia, o factores extrínsecos Bajo índice ponderal Alto riesgo de asfixia perinatal Alto riesgo de hipoglicemia

33
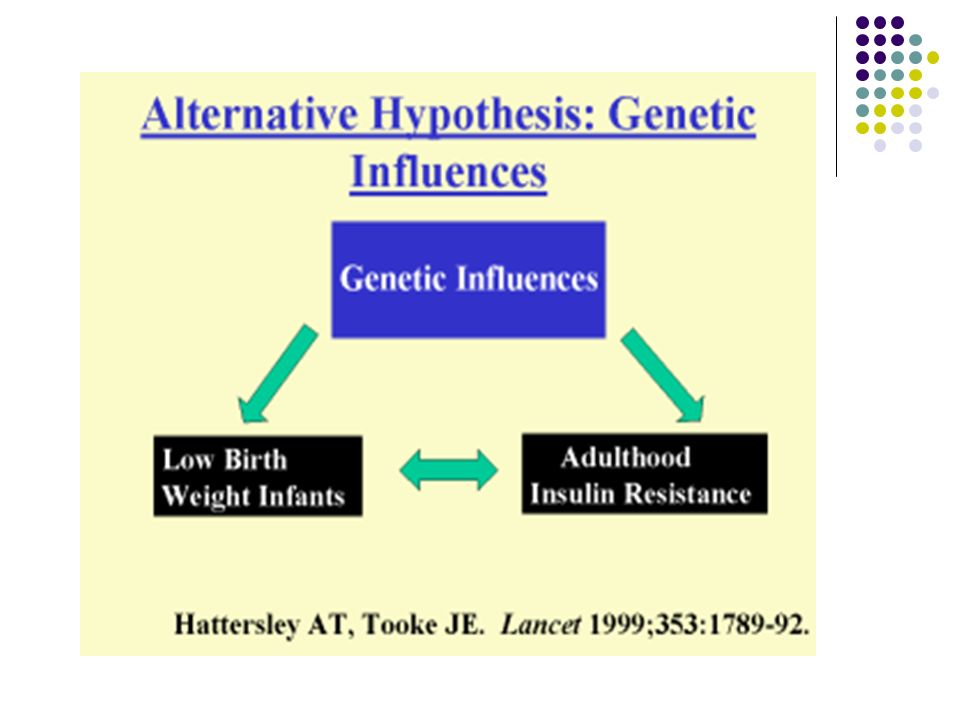
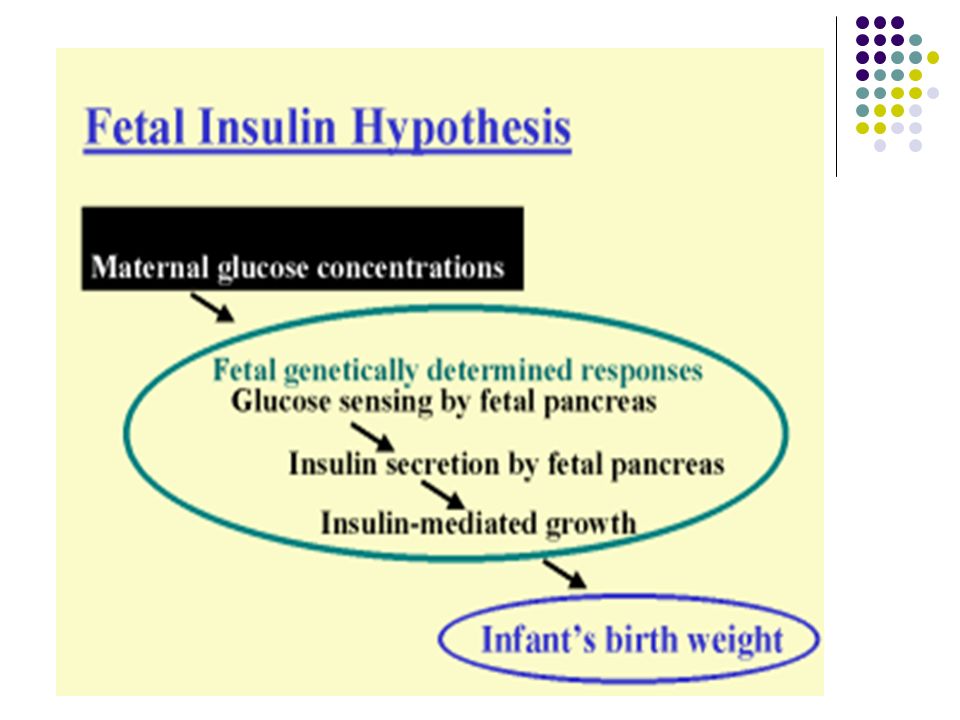
¿Cuál es la hipótesis de las enfermedades de origen fetal?
La suceptibilidad para padecer enfermedades cardiovasculares, DBT tipo II y sindrome de resistencia a la insulina, está programada in utero como respuesta a la desnutrición fetal

36
Cordocentesis Permite la determinación del cariotipo fetal
Evaluación de parámetros bioquímicos en sangre fetal (hipercapnia, acidosis, hiperlactacidemia, hipoglucemia y eritroblastosis Las pacientes que más se benefician: RCIU severo de inicio precoz

Presentaciones similares