Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Dr. Luis Rivera Mejía República Dominicana
Asociación Latinoamericana de Pediatría Dr. Luis Rivera Mejía República Dominicana

2
SINDROME DE DIFICULTAD RESPIRATORIA (SDR)
Dr. Luis Rivera Mejía Jefe Dpto. de Medicina Neonatal-Perinatal Hospital Maternidad Ntra. Sra. de la Altagracia Santo Domingo Hagamos que el milagro de la vida tenga un propósito: Una nueva generación saludable para el bienestar del país!.

3
HOSPITAL MATERNIDAD NTRA. SRA. DE LA ALTAGRACIA

4
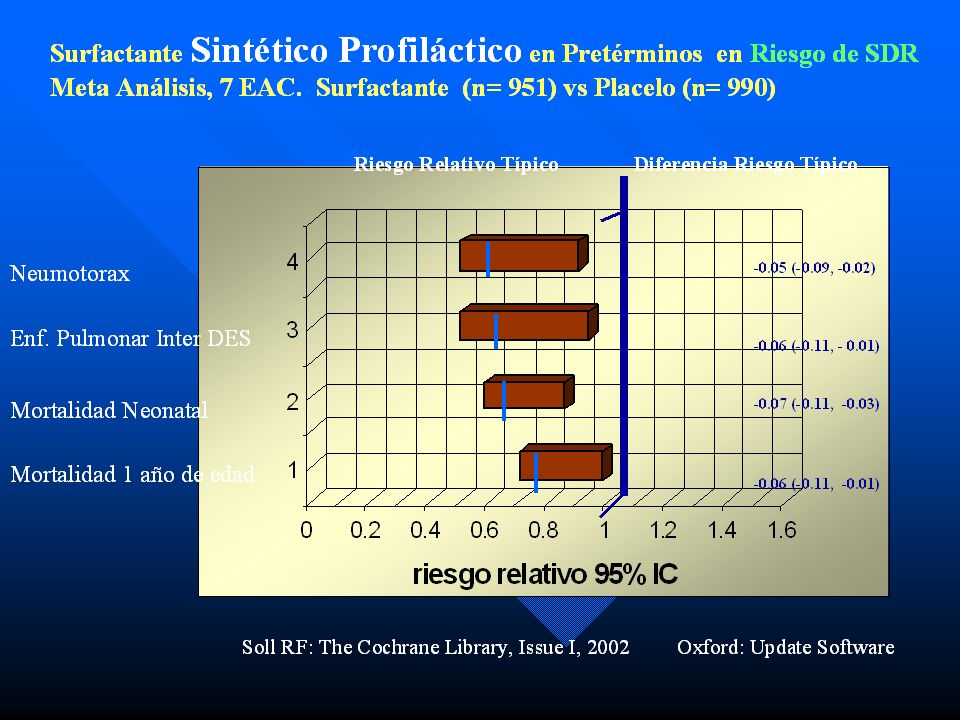
SDR La causa más frecuente de dificultad respiratoria en infantes prematuros 60-80% <28 semanas AG ; 15-30% de semanas AG ; 5% 37 semanas-termino Presentación clásica de quejidos, retracciones, aumento requirimientos O2, patrón reticulo-granular y broncograma aéreo en Rx e inicio < 6horas de edad Incidencia : inversamente proporcional a la edad gestacional. Estrategia de prevencion: Esteroides antenatales y uso de surfactante profilactico

5
Incidencia SDR

6
Laplaces law P = 2t r where: P = pressure T = surface tension
R = radius of the bubble

7
Surface tension Air SURFACE Polar H2O molecules attract liquid

8
Patogénesis Prematuridad Perinatal asphyxia
Reducción síntesis surfactante, almacen, liberación Aumento tension superficie alveolar Atelectasia progresiva gradiente Desigual V/Q Hipoventilación Difusion Hipoxemia retención CO2 Acidosis vasoconstriccion Pulmonar Hipoperfusión Daño endotelio capilar Filtración Plasma Fibrin

9
Antes de Surfactante 1 hr after Surfactant

11
Tasa de Mortalidad Infantil de 1915 a 2000. EEUU
Por N.V 120 100 80 60 Rep. Dominicana 2004 (32/1000) 40 20 Tenemos una brecha de 50 años de atraso en la tasa de mortalidad infantil con USA, peor aún, países como cuba, Costa Rica, Chile, las islas del caribe anglosajón y otras nos superan con más de 30 años de brecha de desarrollo en esta área de la salud. A pesar de que somos el país con mayores índices de desarrollo en desde los años de 1960, mostrando un PIB superior en promedio a todos los países de Latino América, no se ha reflejado en la salud, ya que ocupamos uno de los últimos lugares en mortalidad infantil….!Con una destrosa mortalidad neonatal, perinatal y materna!. 1915 1925 1935 1945 1955 1965 1975 1985 1995 2000 2002-3 Agua potable. Leche Pasteuriz. Dispos. Excretas-Basura Mejoria en Educacion Mejoria Nutricion Serv. Salud Materno-Infantil Atimicrobianos Reposicion de liquidos-electrolitos Trasfusion segura Inmunizaciones Causas Perinatales BPN-Pretermino Cuidados Intens. R.N. Regionalizacion Serv. Perinatales Surfact. Artificial Muerte Subita Interrup. Malfor Cirugia y Manejo malformados CDC 1999
 Tenemos una brecha de 50 años de atraso en la tasa de mortalidad infantil con USA, peor aún, países como cuba, Costa Rica, Chile, las islas del caribe anglosajón y otras nos superan con más de 30 años de brecha de desarrollo en esta área de la salud. A pesar de que somos el país con mayores índices de desarrollo en desde los años de 1960, mostrando un PIB superior en promedio a todos los países de Latino América, no se ha reflejado en la salud, ya que ocupamos uno de los últimos lugares en mortalidad infantil….!Con una destrosa mortalidad neonatal, perinatal y materna! Agua potable. Leche Pasteuriz. Dispos. Excretas-Basura. Mejoria en Educacion. Mejoria Nutricion. Serv. Salud Materno-Infantil. Atimicrobianos. Reposicion de liquidos-electrolitos. Trasfusion segura. Inmunizaciones. Causas Perinatales. BPN-Pretermino. Cuidados Intens. R.N. Regionalizacion Serv. Perinatales. Surfact. Artificial. Muerte Subita. Interrup. Malfor. Cirugia y Manejo. malformados. CDC")
12
Mortalidad Infantil Proporción de los componentes para República Dominicana
28 % Pós-neonatal 72 % Neonatal 2,960 muertes 5,040 muertes de 0-28 días 3,024 muertes de 0-7 días (60%) Es increíble esta realidad…aunque la mayoría de las muertes infantiles son de origen neonatal (80%) no existe un plan o programa nacional para la reducción del mismo. El programa de Promese PAUCIN, es el primero en aplicarse desde un organismo gubernamental en toda la historia del país. Fuente: SESPAS, 2003
 Es increíble esta realidad…aunque la mayoría de las muertes infantiles son de origen neonatal (80%) no existe un plan o programa nacional para la reducción del mismo. El programa de Promese PAUCIN, es el primero en aplicarse desde un organismo gubernamental en toda la historia del país. Fuente: SESPAS,")
13
CAUSAS DIRECTAS DE MORTALIDAD NEONATAL EN REPUBLICA DOMINICANA
10% 5% 32 % 24% 29 % Más del 85% de la mortalidad neonatal es prevenible o evitable con un manejo adecuado. Fuente: SESPAS 2003

14
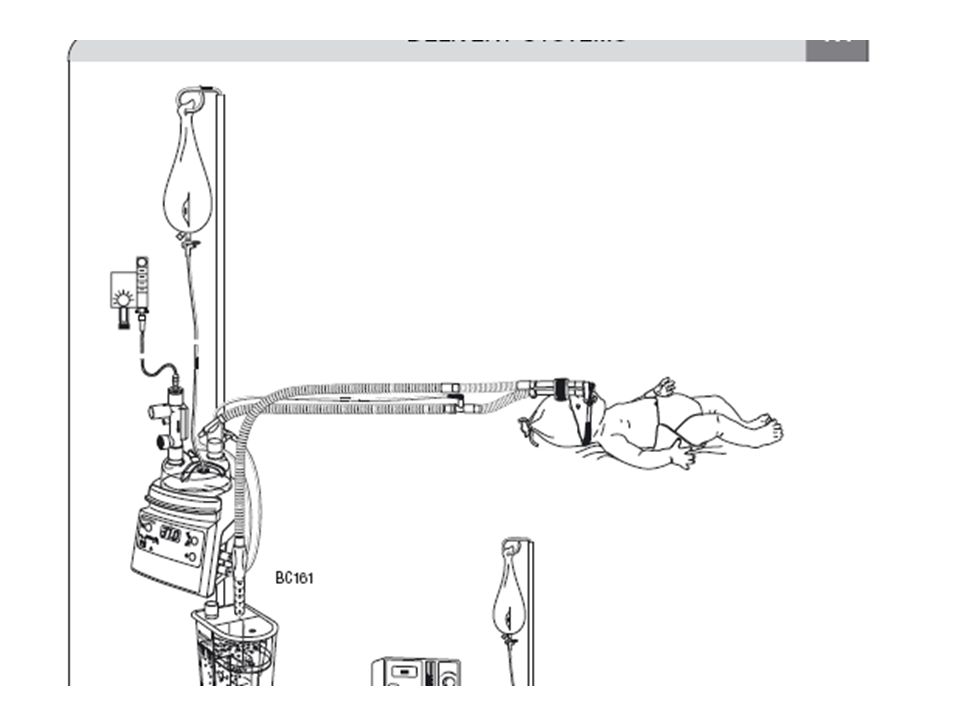
Ventilación Mecánica Modalidades: -CPAP
-Ventilación mandatoria intermitente -Ventilación sincronizada: AC/SIMV -Ventilación de alta frecuencia -Uso de Oxido Nítrico

15
1 Aly, H. Z. Pediatrics 2001;108: Copyright ©2001 American Academy of Pediatrics

21
Predicción de sobrevida según edad gestacional
% sobrevida Semanas de Edad Gestacional FUENTE: Cooper, RL. Am J Obstet Gynecol 168:78, 1993

22
Prematurity & Low Birthweight, U.S., 2003
< 1,000 grams 0.7% (of live births) Most (99.3%) are preterm 1,000-2,500 grams 7.2% 63.9% are preterm > 2,500 grams % 7.6% are preterm In 2003, about 8 percent of the live births in the U.S. were low-birthweight infants which included both preterm infants and those whose growth has been impaired in utero. An infant who weighs less than the 10th percentile for gestational age is termed “small for gestational age” or “SGA.” An infant weighing less than expected based on gestational age and other growth parameters is said to have experienced intrauterine growth restriction or “IUGR.” Most infants who weigh less than the 5th percentile are growth restricted, and almost all who weigh more than the 10th percentile are not growth restricted. The 10th percentile, the definition of SGA, is therefore often used prenatally as a good screening test to identify fetuses with possible IUGR. The overlap between the categories of infants that are preterm, low birthweight and/or have birth defects is graphically depicted in the next slide. Source: Iams JD, Creasy RK. Preterm labor and delivery, Chapter 34. In: Creasy RK, Resnik R, Iams JD, eds. Maternal-Fetal Medicine: Principles and Practice, 5th ed., 2004. Low birthweight is less than 2,500 grams (5 1/2 pounds). Preterm is less than 37 completed weeks gestation. Source: National Center for Health Statistics, 2003 natality file Prepared by March of Dimes Perinatal Data Center, 2006.
 Most (99.3%) are preterm. 1,000-2,500 grams 7.2% 63.9% are preterm. > 2,500 grams 92.1% 7.6% are preterm. In 2003, about 8 percent of the live births in the U.S. were low-birthweight infants which included both preterm infants and those whose growth has been impaired in utero. An infant who weighs less than the 10th percentile for gestational age is termed small for gestational age or SGA. An infant weighing less than expected based on gestational age and other growth parameters is said to have experienced intrauterine growth restriction or IUGR. Most infants who weigh less than the 5th percentile are growth restricted, and almost all who weigh more than the 10th percentile are not growth restricted. The 10th percentile, the definition of SGA, is therefore often used prenatally as a good screening test to identify fetuses with possible IUGR. The overlap between the categories of infants that are preterm, low birthweight and/or have birth defects is graphically depicted in the next slide. Source: Iams JD, Creasy RK. Preterm labor and delivery, Chapter 34. In: Creasy RK, Resnik R, Iams JD, eds. Maternal-Fetal Medicine: Principles and Practice, 5th ed., Low birthweight is less than 2,500 grams (5 1/2 pounds). Preterm is less than 37 completed weeks gestation. Source: National Center for Health Statistics, 2003 natality file. Prepared by March of Dimes Perinatal Data Center,")
23
Preterm & Very Preterm Births United States, 1993-2003
Preterm is less than 37 completed weeks gestation. Very preterm is less than 32 completed weeks gestation. Source: National Center for Health Statistics, final natality data. Prepared by March of Dimes Perinatal Data Center, 2006. Percent of live births Although the rate of birth before 37 weeks has increased, births before 32 weeks have remained unchanged for more than a decade. However, very preterm births made up 54 percent of infant deaths in 2002. There is a strong relationship between gestational age at birth, neonatal morbidity and mortality, and intrauterine infection and inflammation. These births have therefore been a principal research target. Source: 2002 period-linked birth/infant death data set, prepared by the March of Dimes Perinatal Data Center, 2006. Healthy People Objective

24
Perinatal Mortality & Gestational Age
The likelihood of perinatal death decreases substantially as the gestational age at birth increases, especially between 24 and 28 weeks of gestation. The data in this slide comes from a population-based cohort of 8,523 infants born in in Memphis (Mercer BM, 2003) and is typical of national data. Preterm infants born before 32 weeks have a substantially increased risk of long-term disability and death: 19 percent of infants born before 32 weeks die within the first year of life, compared with 1 percent of infants born at 32–36 weeks, and 0.2 percent of infants delivered at 37–41 weeks (Mathews TJ, MacDorman MF, 2006). Sources: Mercer BM. Preterm premature rupture of the membranes. Obstet Gynecol 2003;101:178-93; Mathews TJ, MacDorman MF. Infant mortality statistics from the 2003 period linked birth/infant death data set. National vital statistics reports; vol 54 no 16. Hyattsville, MD: National Center for Health Statistics, 2006. Source: Mercer BM. Preterm premature rupture of the membranes. Obstet Gynecol 2003;101: Reproduced with permission from Lippincott Williams & Wilkins.
 and is typical of national data. Preterm infants born before 32 weeks have a substantially increased risk of long-term disability and death: 19 percent of infants born before 32 weeks die within the first year of life, compared with 1 percent of infants born at 32–36 weeks, and 0.2 percent of infants delivered at 37–41 weeks (Mathews TJ, MacDorman MF, 2006). Sources: Mercer BM. Preterm premature rupture of the membranes. Obstet Gynecol 2003;101:178-93; Mathews TJ, MacDorman MF. Infant mortality statistics from the 2003 period linked birth/infant death data set. National vital statistics reports; vol 54 no 16. Hyattsville, MD: National Center for Health Statistics, Source: Mercer BM. Preterm premature rupture of the membranes. Obstet Gynecol 2003;101: Reproduced with permission from Lippincott Williams & Wilkins.")
Presentaciones similares