Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Radiografía simple de abdomen
Universidad Autónoma del Estado de Morelos FACULTAD DE MEDICINA Elguea López Aidee Mariana, Aldo Gutierrez Rosales, Erick Eduardo Díaz Díaz, Salvador Padilla Hernández, Samantha Hernández Gurrión

2
Definición Estudio radiológico del abdomen
NO emplea medios de contraste u otras técnicas especiales Puede ser orientada

3
Técnica Miliamperaje elevado Tiempo de exposición corto
Apófisis xifoides – Sínfisis púbica Espiración profunda Proteger las gónadas Intestino preparado (no urgente) Miliamperaje elevado Tiempo de exposición corto
 Miliamperaje elevado. Tiempo de exposición corto.")
4
Planos y posiciones Posición supina Bipedestación (AP, PA)
Decúbito lateral izquierdo Oblicua

5
¿Qué se debe buscar? Estructuras con contenido aéreo/gaseoso
Desplazamiento Calcificaciones Grasa periabdominal

6
5 1 7 8 2 2 3 3 4 4 6 9 Higado 12° costilla Riñón Psoas Estómago
Intestino delgado Ángulo cólico hepático Ángulo cólico esplénico Vejiga 8 2 2 3 3 4 4 6 9

7
Indicaciones Síntomas y signos abdominales: dolor abdominal, abdomen agudo, estreñimiento, distensión, masas palpables, peristaltismo anormal, etc. Síntomas urinarios: dolor renal, dolor urinario, oliguria, polaquiuria, etc. Previo estudio contrastado Dolor lumbar

8
Para interpretar: Identificar estructuras normales
Identificar hallazgos patológicos: Masas anormales Calcificaciones y cuerpos extraños Aire intraluminal anormal Aire extraluminal

9
Masas Presencia de grasa periférica Desplazamiento de otra víscera
Detección durante palpación Paciente de 27 años con enfermedad de Gaucher que presenta masa grande en el cuadrante superior izquierdo, que desplaza el ángulo esplénico del colon hacia abajo y hacia adentro, correspondiente con ESPLENOMEGALIA.

10
Calcificaciones Cartílagos costales Flebolitos Calcificación vascular
Fibromas, leiomiomas uterinos Rx Oblicua: dxd calcificación de cartilagos costales VS calcificación en páncreas, riñon y vesícula. Flebolitos: calcificaciones de venas pélvicas trombosadas. Dxd vs calcificación de uréter distal,

11
Calcificaciones Cálculos en vísceras huecas
Calcificación de tumores o metástasis. Calcificación de pared de un quiste o víscera hueva Rx Oblicua: dxd calcificación de cartilagos costales VS calcificación en páncreas, riñon y vesícula. Flebolitos: calcificaciones de venas pélvicas trombosadas. Dxd vs calcificación de uréter distal,

12
Densidades anormales Cuerpo extraño Lipoma
Dxd lipoma VS teratoma ovárico

13
Obstrucción intestinal
Identificar niveles aéreos Identificar punto de obstrucción: intestino proximal distendido y descompresión del intestino distal

14
Gas intraluminal en otras vísceras
Comunicación con el exterior. Sonda vesical, tubo de nefrostomía, unión de conductos biliares con intestino etc. Fístulas con el intestino o piel. Microorganismos productores de gas: Cistitis enfisematosa, Colecistitis enfisematosa. Pared intestinal: Infección o infarto, preliminar de perforaciones.

15
Rx abdomen: Pielonefritis y cistitis enfisematosa
Rx abdomen: Pielonefritis y cistitis enfisematosa. Se objetiva aire en vías urinarias (flecha) y en la pared de la vejiga (punta de flecha) en paciente portador de catéter doble J bilateral. El aumento de densidad superpuesto a hipocondrio derecho (asterisco) corresponde a una bolsa de colostomía. © Sociedad Española de Radiología Médica, 2010.
 y en la pared de la vejiga (punta de flecha) en paciente portador de catéter doble J bilateral. El aumento de densidad superpuesto a hipocondrio derecho (asterisco) corresponde a una bolsa de colostomía. © Sociedad Española de Radiología Médica,")
16
Más común en px con DM y ancianos
Más común en px con DM y ancianos. Con sospecha de colecistitis, siempre pedir rx de abdomen.

17
Aire extraluminal Rx supina y de pie.
Se puede complementar con Rx simple de tórax para observar diafragma y regiones infradiafragmáticas. Con grandes cantidades de aire se pueden observar bordes externos de estómago, intestino, ligamento falciforme. Perforación visceral.

18
Aire y líquido anormal distiende al estómago y a la trascavidad de los epiplones. Perforación de úlcera.

19
Aire Loculado Absceso intra abdominal: Niveles hidroaereos, contenido semisólido. Más común debajo del diafragma “burbujas dentro de material semisólido”

20
Ascitis Visible en cantidades importantes de líquido. “Vidrio opaco”. Desplazamiento de vísceras. Separación de asas por flotación. Colección de líquido en pelvis. Signo de luna llena: Colección de líquido sobre la vejiga (similar al útero) Colección en correderas parietocólicas.
 Colección en correderas parietocólicas.")
23
ESTUDIOS DE CONTRASTE DE COLON
Enemas de contraste simple y doble contraste

24
1)Sulfato de bario 2)Aire + sulfato de bario ESTUDIOS DE CONTRASTE
Sulfato de bario 2)Aire + sulfato de bario ESTUDIOS DE CONTRASTE")
25
ESTUDIO DE DOBLE CONTRASTE
PROCEDIMIENTO DE DOBLE CONTRASTE DE 2 PASOS PROCEDIMIENTO DE DOBLE CONTRASTE SIMPLE two-stage double-contrast procedure : introduce el bario y al ser evacuado se introduce el gas single-stage doubLe-contrast procedure : se introducen al mismo tiempo

26
¿Qué vamos a observar? Anatomía Tono Anormalidades

27
Medio de Contraste Sulfato de Bario 12-15% 75-95%
Commercially prepared barium sulfate products are generally used for routine ret rograde examinations of the large intestine. Some of these products are referred to as coLLoidal preparations because they have finely divided barium particles that resist precipitation, whereas others are referred to as suspended or floccuLation-resistant cosal pattern. However, when a patient is preparations because they contain some form of suspending or dispersing agent. The newest barium products available are referred to as high-density barium sulfate. These products absorb a greater percentage of radiation, similar to the older "thick" barium products. High density barium is particularly useful for double-contrast studies of the alimentary canal in which uniform coating of the lu men is required. Commercial barium enema prepara tions are available as premixed l iquids that can be poured into the disposable en ema kit bag. Powdered barium is al 0 available in single-contra t disposable kit bags. Water is added, and the solution is mixed by shaking the bag. f warm barium enemas are adminis tered, the temperature should be some what below body temperature-about 85° to 90° F (29° to 30° C). In addition to be ing unpleasant and debilitating, an enema that is too warm is injurious to intestinal tissues and produces so much irritation that it is difficult, if not impossible, for the patient to retain the enema long enough for a satisfactory examination. Cold barium enema suspensions (41° F [5° C]) have been recommended I on the basis that the colder temperature produces less irritation, has a mild anesthetic effect that relaxes the colon, and stimulates tonic contraction of the anal sphincter. These effects result in greater comfort and ease of retention for the patient and permit easier, more rapid filling of the colon. The patient not only has no sensation of chill but also finds the cold suspension soothing and easy to retain. The cold temperature is most easily obtained by preparing the bar ium suspension one day in advance and refrigerating it overnight. Preparaciones coloidales Sulfato de Bario de alta densidad 12-15% % 30ºc, preparaciones calientes y frías
. In addition to be ing unpleasant and debilitating, an enema that is too warm is injurious to intestinal tissues and produces so much irritation that it is difficult, if not impossible, for the patient to retain the enema long enough for a satisfactory examination. Cold barium enema suspensions (41° F [5° C]) have been recommended I on the basis that the colder temperature produces less irritation, has a mild anesthetic effect that relaxes the colon, and stimulates tonic contraction of the anal sphincter. These effects result. in greater comfort and ease of retention for the patient and permit easier, more rapid filling of the colon. The patient not only has no sensation of chill but also finds the cold suspension soothing and easy to retain. The cold temperature is most easily obtained by preparing the bar ium suspension one day in advance and refrigerating it overnight. Preparaciones coloidales. Sulfato de Bario de alta densidad % 75-95% 30ºc, preparaciones calientes y frías.")
28
Medio de Contraste Aire, Dióxido de Carbono Nitrógeno
Air is the gaseous medium usually used in the double-contrast enema study. There fore the procedure is generally called an air-contrast study. Carbon dioxide may also be used because it is more rapidly absorbed than the nitrogen in air when evacuation of the gaseous medium is incomplete. Nitrógeno

29
Preparados iodados solubles en agua
Medio de Contraste Preparados iodados solubles en agua Specifically prepared water-soluble, io dinated contrast agents are administered orally to selected patients when retrograde fillingofthecolonwithbariumisnotpos sible or is contraindicated. A disadvantage of the iodinated solutions is that evacua tion often is insufficient for satisfactory double-contrast visualization of the mu Commercially prepared barium sulfate products are generally used for routine ret rograde examinations of the large intestine. Some of these products are referred to as coLLoidal preparations because they have finely divided barium particles that resist precipitation, whereas others are referred to as suspended or floccuLation-resistant cosal pattern. However, when a patient is preparations because they contain some form of suspending or dispersing agent. The newest barium products available are referred to as high-density barium sulfate. These products absorb a greater percentage of radiation, similar to the older "thick" barium products. High density barium is particularly useful for double-contrast studies of the alimentary canal in which uniform coating of the lu men is required. Air is the gaseous medium usually used in the double-contrast enema study. There fore the procedure is generally called an air-contrast study. Carbon dioxide may also be used because it is more rapidly absorbed than the nitrogen in air when evacuation of the gaseous medium is incomplete. unable to cooperate for a successful en ema study, orally administered iodinated medium allows satisfactory examination of the colon. With these oral agent, transit time from ingestion to colonic filling is fast, averaging 3 to 4 hours. Furthermore, iodinated solutions are practically nonab sorbable from the gastrointestinal mu cosa. As a result, the oral dose reaches and outlines the entire large bowel. Unlike an ingested barium sulfate suspension, this medium is not subject to drying, flaking, and unequal distribution in the colon. Therefore it frequently delineates the in testine almost as well as the barium en ema does. Orales

30
Preparación del tracto intestinal
Vacio the large intestine must be completely emp tied of its contents to render all portions of its inner wall visible for inspection. When coated with a barium sulfate suspension, retained fecal masses are likely to simu late the appearance of polypoid or other small tumor masses The preliminary preparation usually includes dietary re strictions and a laxative. Cleansing ene mas are also used, as are commercially available complete colon cleansing kits designed for easy use by outpatients or hospital nursing personnel.

31
Aparato estándar para el enema de bario
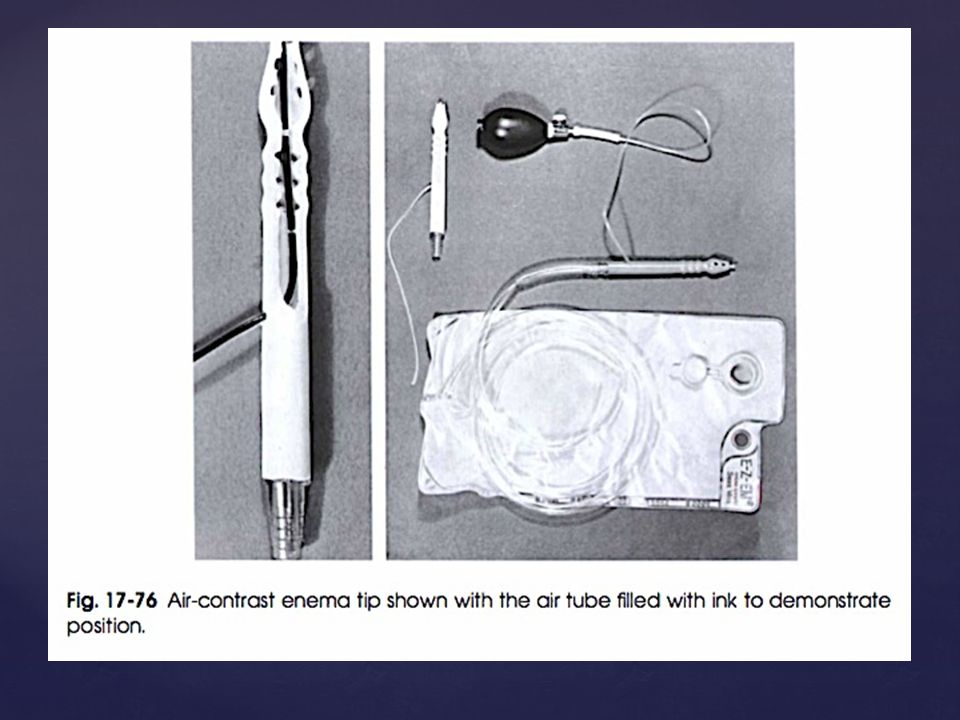
A soft rubber rectal catheter of small caliber should be used in patients who have inflamed hemorrhoids, fissures, a stricture, or other abnormalities of the anus. Disposable rectal retention tips (Fig ) have replaced the older retention catheters such as the Bardex or Foley catheter. The retention tip is a double lumen tube with a thin balloon at its distal end. Because of the danger of intestinal rupture, the retention tip must be inserted with extreme care. The enema retention tip is used in the patient who has a relaxed anal sphi ncter or another condition that makes it difficult or impossible to retain an enema. Some radiologists routinely use retention enema tips and inflate them if necessary. The disposable rectal retention tip has a balloon that fits snugly against the enema nozzle both before and after deflation so that it can be inserted and removed with little discomfort to the patient. A reusable squeeze inflator is recommended to Jjmit the air capacity to approximately 90 ml. One complete squeeze of the inflator pro vides adequate distention of the retention balloon without danger of overinflation. Disposable retention tips are available for both double-contrast and single-contrast enemas. For the safety of the patient, any retention balloon must be inflated with caution, using fluoroscopy, just before the examination. For the performance of a double-con trast barium enema (BE) examination, a special rectal tip is needed to instill air in the colon (Fig ). Alternatively, air can simply be pumped into the colon us ing a sphygmomanometer bulb. Double contrast retention tips are also available. Most enema bags have a capacity of 3 quarts (3000 ml) when fully distended and have graduated quantity markings on the side. A filter may be incorporated within the bag to prevent the passage of any un mixed lumps of barium. The tubing is ap proximately 6 feet long. Catéter de calibre pequeño 3l graduados
 have replaced the older retention catheters such as the Bardex or Foley catheter. The retention tip is a double lumen tube with a thin balloon at its distal end. Because of the danger of intestinal rupture, the retention tip must be inserted with extreme care. The enema retention tip is used in the patient who has a relaxed anal sphi ncter or another condition that makes it difficult or impossible to retain an enema. Some radiologists routinely use. retention enema tips and inflate them if necessary. The disposable rectal retention tip has a balloon that fits snugly against the enema nozzle both before and after deflation so that it can be inserted and removed with little discomfort to the patient. A reusable squeeze inflator is recommended to Jjmit the air capacity to approximately 90 ml. One complete squeeze of the inflator pro vides adequate distention of the retention balloon without danger of overinflation. Disposable retention tips are available for both double-contrast and single-contrast enemas. For the safety of the patient, any retention balloon must be inflated with caution, using fluoroscopy, just before the examination. For the performance of a double-con trast barium enema (BE) examination, a special rectal tip is needed to instill air in the colon (Fig ). Alternatively, air can simply be pumped into the colon us ing a sphygmomanometer bulb. Double contrast retention tips are also available. Most enema bags have a capacity of 3 quarts (3000 ml) when fully distended and have graduated quantity markings on the side. A filter may be incorporated within the bag to prevent the passage of any un mixed lumps of barium. The tubing is ap proximately 6 feet long. Catéter de calibre pequeño. 3l. graduados.")
33
PREPARACION Y CUIDADO DEL PACIENTE
Cooperación Retención del Enema Preparation and care of patient In no radiologic examination is the full cooperation of the patient more essential to success than in the retrograde examina tion of the colon. Few patients who are physically able to retain the enema fail to do so when they understand the procedure and realize that in large measure the suc cess of the examination depends on them. The radiographer should observe the fol lowing guidelines in preparing a patient for retrograde examination of the colon: • Take time to explain the procedural dif ferences between an ordinary cleansing enema and a diagnostic enema: ( I ) with the diagnostic enema the fluoroscopist examines all portions of the bowel as it is being filled with contrast medium un der fluoroscopic observation; (2) this part of the examination involves palpa tion of the abdomen, rotation of the body as required to visualize the differ ent segments of the colon, and the tak ing of spot radiographs without and, when indicated, with compression; (3) a eries o f l arge radiographs are taken before the colon can be evacuated (Fig. 1 7-77). Assure the patient that retention of the diagnostic enema preparation will be comparatively easy because its flow is controlled under fluoroscopic observa tion. Instruct the patient ( l ) to keep the anal sphincter tightly contracted against the tubing to hold it in position and prevent leakage, (2) to relax the abdominal mus cles to prevent intraabdominal pressure, and (3) to concentrate on deep oral breathing to reduce the i ncidence of colonic spasm and resultant cramp . Assure the patient that the flow of the enema will be stopped for the duration of any cramping. PREPARACION Y CUIDADO DEL PACIENTE
 with the diagnostic enema the fluoroscopist examines all portions of the bowel as it is being filled with contrast medium un der fluoroscopic observation; (2) this part of the examination involves palpa tion of the abdomen, rotation of the body as required to visualize the differ ent segments of the colon, and the tak ing of spot radiographs without and, when indicated, with compression; (3) a eries o f l arge radiographs are taken before the colon can be evacuated (Fig ). Assure the patient that retention of the diagnostic enema preparation will be comparatively easy because its flow is controlled under fluoroscopic observa tion. Instruct the patient ( l ) to keep the anal sphincter tightly contracted against the tubing to hold it in position and prevent leakage, (2) to relax the abdominal mus cles to prevent intraabdominal pressure, and (3) to concentrate on deep oral breathing to reduce the i ncidence of colonic spasm and resultant cramp . Assure the patient that the flow of the enema will be stopped for the duration of any cramping. PREPARACION Y CUIDADO DEL PACIENTE.")
34
Indicaciones para el cuidado del paciente
Tomarse el tiempo para explicarle al paciente las diferencias entre el enema ordinario de limpieza y el enema diagnostico. Instruir al paciente a que mantenga el esfínter anal contraído. Relaje los músculos abdominales

35
INSERCION DE LA PUNTA DEL ENEMA
Colocar al paciente en posición de Sim’s. Expone la región anal Deja salir un poco de bario para eliminar el aire, y se lubrica el tubo rectal con un gel a base de agua. Avisarle al paciente que respire profundo y se relaje. 5. Insertar el tubo rectal suavemente durante la espiración en el orificio anal. Siguiendo el angulo de el canal anal, dirigiendolo anteriormente de 2.5 a 3.5 cm siguiendo la curvatura anal, No introducir mas de 10 cm. 6. No se debe forzar la entrada del tubo rectal. 7. Despues de que la punta del enema a sido insertada, sostenerla en su posición para prevenir que se resbale. Instruct the patient to tum onto the left side, lean forward about 35 to 40 de grees, and rest the flexed right knee on the table, above and in front of the slightly flexed left knee (Sims' posi tion). This position relaxes the abdomi nal muscle , which decreases i ntraab dominal pressure on the rectum and makes relaxation of the anal sphi ncter less difficult. Adjust the IV pole so that the enema contents are no higher than 24 inches (6 1 cm) above the level of the anus. • Adjust the overlapping back of the gown or other draping to expose the anal region only, but keep the patient otherwi e well covered. The anal ori fice is commonly partially obscured by distended hemorrhoids or a fringe of undistended hemorrhoids. Sometimes there is a contraction or other abnor mal ity of the orifice. It is therefore nec essary for the anus to be exposed and sufficiently well lighted for the orifice to be clearly visible so that the enema tip can be inserted without injury or discomfort. • Run a little of the barium mixture into a waste basin to free the tubing of air, and then lubricate the rectal tube well with a water-soluble lubricant. • Advise the patient to relax and take deep breaths so that no discomfort is felt when the tube is inserted. • Push the right buttock laterally to open the gluteal fold. • As the abdominal muscles and anal sphincter are relaxed during the expira tion phase of a deep breath, insert the rectal tube gently and slowly into the anal orifice. Following the angle of the anal canal, direct the tube anteriorly I to I Y; inches (2.5 to 3.8 cm). Then fol lowing the curve of the rectum, direct the tube slightly superiorly. • Insert the tube for a total distance of no more than 3Y; to 4 inches (8.9 to 10 cm). Insertion for a greater distance is not only unnecessary but may injure the rectum. • If the tube does not enter easily, ask the patient to assist if capable. • Never forcibly insert a rectal tube be cause the patient may have distended internal hemorrhoids or another condi tion that makes forced insertion of the tube dangerous. • After the enema tip is inserted, hold it in position to prevent it from slipping while the patient turns to the supine or prone position for fluoroscopy, according to the preference of the fluoroscopist. • Adjust the protective underpadding, and relieve any pressure on the tubing so that the enema mixture will flow freely.
. This position relaxes the abdomi nal muscle , which decreases i ntraab dominal pressure on the rectum and makes relaxation of the anal sphi ncter less difficult. Adjust the IV pole so that the enema contents are no higher than 24 inches (6 1 cm) above the level of the anus. • Adjust the overlapping back of the gown or other draping to expose the anal region only, but keep the patient otherwi e well covered. The anal ori fice is commonly partially obscured by distended hemorrhoids or a fringe of undistended hemorrhoids. Sometimes there is a contraction or other abnor mal ity of the orifice. It is therefore nec essary for the anus to be exposed and sufficiently well lighted for the orifice to be clearly visible so that the enema tip can be inserted without injury or discomfort. • Run a little of the barium mixture into a waste basin to free the tubing of air, and then lubricate the rectal tube well with a water-soluble lubricant. • Advise the patient to relax and take deep breaths so that no discomfort is felt when the tube is inserted. • Push the right buttock laterally to open the gluteal fold. • As the abdominal muscles and anal sphincter are relaxed during the expira tion phase of a deep breath, insert the rectal tube gently and slowly into the anal orifice. Following the angle of the anal canal, direct the tube anteriorly I to I Y; inches (2.5 to 3.8 cm). Then fol lowing the curve of the rectum, direct the tube slightly superiorly. • Insert the tube for a total distance of no more than 3Y; to 4 inches (8.9 to 10 cm). Insertion for a greater distance is not only unnecessary but may injure the rectum. • If the tube does not enter easily, ask the patient to assist if capable. • Never forcibly insert a rectal tube be cause the patient may have distended internal hemorrhoids or another condi tion that makes forced insertion of the tube dangerous. • After the enema tip is inserted, hold it in position to prevent it from slipping while the patient turns to the supine or prone position for fluoroscopy, according to the preference of the fluoroscopist. • Adjust the protective underpadding, and relieve any pressure on the tubing so that the enema mixture will flow freely.")
36
Enema de bario de contraste simple
Administración del medio de contraste La Ámpula rectal se va llenando lentamente. El llenado de bario se detiene cuando la ámpula esta llena. La suspensión saldrá atravez del sigmoides y desciende por el colon. Frecuentemente puede causar simulación de reflejo de defecación. SINGLE-CONTRAST BARIUM ENEMA Administration of contrast medium After preparing the patient for the exami nation, the radiographer observes the fol lowing step : Notify the radiologist as soon as every thing is ready for the examination. If the patient has not been introduced to the radiologist, make the introduction at this time. At the radiologist's request, release the control clip and ensure the enema flow. When occlusion of the enema tip oc curs, displace soft fecal material by withdrawing the rectal tube about 1 inch (2.5 cm). Then before reinserting the tip, temporarily elevate the enema bag to increase fluid pressure. The rectal ampulla fills slowly. Unless the barium flow is stopped for a few sec onds once the rectal ampulla is full, the suspension will flow through the sigmoid and descending portions of the colon at a fairly rapid rate, frequently causing a se vere cramp and acute stimulation of the defecation impUlse. The flow of the bar ium suspension is usually stopped for sev eral seconds at frequent intervals during the fluoroscopically controlled filling of the colon. During the fluoroscopic procedure, the radiologist rotates the patient to inspect all segments of the bowel. The radiologist takes spot radiographs as indicated and determines the positions to be used for subsequent radiographic studies. On com pletion of the fluoroscopic examination, the enema tip is usually removed so that the patient can be maneuvered more eas ily and so that the tip is not accidentally displaced during the imaging procedure. A retention tube is not removed until the patient is placed on a bedpan or the toilet. Durante el estudio el radiólogo rotara en diferentes posiciones al paciente para examinar todas las porciones del colon, por lo que el tubo del enema se retira para que el paciente pueda maniobrar mas facil.
. Then before reinserting the tip, temporarily elevate the enema. bag to increase fluid pressure. The rectal ampulla fills slowly. Unless the barium flow is stopped for a few sec onds once the rectal ampulla is full, the suspension will flow through the sigmoid and descending portions of the colon at a fairly rapid rate, frequently causing a se vere cramp and acute stimulation of the defecation impUlse. The flow of the bar ium suspension is usually stopped for sev eral seconds at frequent intervals during the fluoroscopically controlled filling of the colon. During the fluoroscopic procedure, the radiologist rotates the patient to inspect all segments of the bowel. The radiologist takes spot radiographs as indicated and determines the positions to be used for subsequent radiographic studies. On com pletion of the fluoroscopic examination, the enema tip is usually removed so that the patient can be maneuvered more eas ily and so that the tip is not accidentally displaced during the imaging procedure. A retention tube is not removed until the patient is placed on a bedpan or the toilet. Durante el estudio el radiólogo rotara en diferentes posiciones al paciente para examinar todas las porciones del colon, por lo que el tubo del enema se retira para que el paciente pueda maniobrar mas facil.")
37
Enema de bario de contraste simple
Paciente desecha en el inodoro el bario que sea posible ES TOMADA UNA RADIOGRAFIA POSTEVACUACIÓN. POSICIONES. PA AP PA OBLICUAS AXIALES DEL SIGMOIDES LATERAL (RECTO) After the IRs have been exposed (Fig ), the patient is escorted to a toilet or placed on a bedpan and instructed to expel as much of the barium suspension as pos sible. A postevacuation radiograph is then taken (Fig ). If this radiograph shows evacuation to be inadequate for sat isfactory delineation of the mucosa, the patient may be given a hot beverage (tea or coffee) to stimulate further evacuation. Positioning of opacified colon The most commonly obtained projections for the single-contrast barium enema are the PA or AP, PA obliques, an axial for the sigmoid, and a lateral for demonstration of the rectum.
 After the IRs have been exposed (Fig ), the patient is escorted to a toilet or placed on a bedpan and instructed to expel as much of the barium suspension as pos sible. A postevacuation radiograph is then taken (Fig ). If this radiograph shows evacuation to be inadequate for sat isfactory delineation of the mucosa, the patient may be given a hot beverage (tea. or coffee) to stimulate further evacuation. Positioning of opacified colon. The most commonly obtained projections for the single-contrast barium enema are the PA or AP, PA obliques, an axial for the sigmoid, and a lateral for demonstration of the rectum.")
38
APLICACIÓN DE BARIO Y AIRE
Enema de doble contraste APLICACIÓN DE BARIO Y AIRE MÉTODO EN UN SOLO TIEMPO Colon limpio Bario adecuado Adecuado fluido del bario MÉTODO EN 2 TIEMPOS Llenar colon con bario Aire u otros gases

39
Introducción del enema
Método en un tiempo Introducción del enema Se instila el bario Evacuación del bario

40
Método en un tiempo Ajuste de la cantidad de bario
Reintroducción del bario Inversión de bolsa. Introducción de aire

41
Método de Welin Colon lo más limpio posible
Mucosa de colon preparada para adherencia de bario Regulación de evacuación

42
Método de Welin Primera fase Segunda fase Posición prona
Administración de bario hasta ángulo esplénico. Rx Evacuar bario Introducción de punta de enema Posición prona Dejar que bario recorra sigmoides Decúbito lat. Der. Administrar aire (1800 – 2000 ml)
")
43
Proyecciones PA oblicua der. AP oblicua izq.: Colon ascendente, ángulo hepático, sigmoides PA oblicua izq. AP oblicua der.: Colon descendente, ángulo esplácnico PA, AP: Todo el colon

44
Proyecciones AP oblicua izquierda: Colon asc. Sigmoides y ángulo hepático Lateral: Recto y sigmoides AP: Todo el colon

45
Proyecciones Decúbito lat. Der. AP: Lado medial colon asc. Lado lateral colon desc. Decúbito lat. izq. AP: Lado lateral colon asc. Lado medial colon desc

46
Proyecciones Decúbito ventral lateral: Lado post. Del colon.
Método Chassard Lapiné: Sigmoides, Recto

47
Bibliografia Ballinger & Frank; Merril’s atlas of radiolographic positions & radiologic procedures; 11th edition; 2007 Dr DC Rockey MD, E Paulson MD, D Niedzwiecki PhD, et al.; Analysis of air contrast barium enema, computed tomographic colonography, and colonoscopy: prospective comparison; The Lancet, Volume 365; 2005 Rubesin, Levine, Laufer, Herlinger; Double-Contrast Barium Enema Examination Technique; Radiology; 2000

Presentaciones similares