Descargar la presentación
La descarga está en progreso. Por favor, espere

2
Enfermedad Pulmonar Obstructiva Crónica
Dr. Alexis Gutiérrez S. Pneumólogo - FCCP

3
GOLD Website Address

4
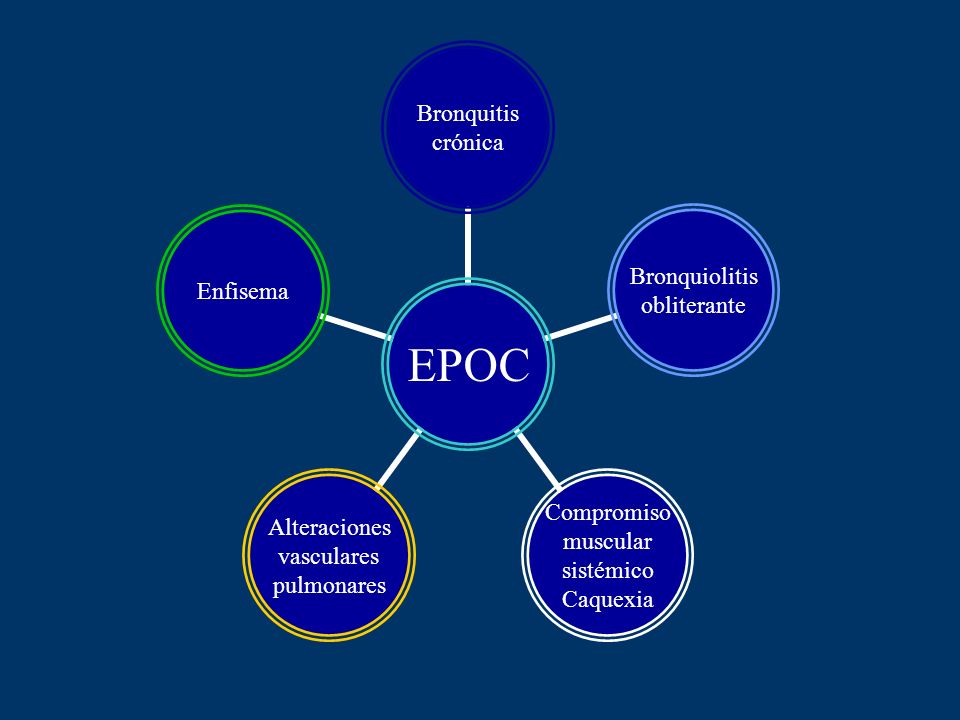
Bronquitis Crónica Enfisema

5
Enfermedad Pulmonar Obstructiva Crónica
Se trata de una enfermedad prevenible y tratable, con efectos extrapulmonares que pueden contribuir a la severidad de la misma Su componente pulmonar se caracteriza por limitación al flujo aéreo que: no es completamente reversible es progresiva está asociada a una respuesta inflamatoria anormal a las partículas nocivas de ciertos gases NHLBI/WHO Global Initiative for Chronic Obstructive Pulmonary Disease (GOLD) 2011
")
7
Prevalencia Estudio NHANES, EUA, 1995
Masculino caucásico 142/1000 fumadores activos Femenino caucásico 136/1000 fumadoras activas Global Burden of Disease Study, Harvard University, 1996 Masculino 9.3/1000 Femenino 7.3/1000 China, Xian SC, 1998 Masculino 4.2/1000 Femenino 1.8/1000 UK diagnosis by General Practitioner, 2000 Masculino 17/1000 Femenino 14/1000

8
Prevalencia Chronic obstructive pulmonary disease in five Latin American cities (the PLATINO study): a prevalence study Lancet 2005;366:

9
PROYECTO LATINOAMERICANO DE INVESTIGACION EN OBSTRUCCION PULMONAR
ALAT PROYECTO LATINOAMERICANO DE INVESTIGACION EN OBSTRUCCION PULMONAR

10
Centros de PLATINO México (Mexico D.F.) Venezuela (Caracas)
Brazil (São Paulo) Chile (Santiago) Uruguay (Montevideo)
 Chile (Santiago) Uruguay (Montevideo)")
11
São Paulo Santiago México DF Montevideo Caracas General 15,8% 16,9% 7,8% 19,7% 12,1% Sexo Masc 18% 23,3% 11,0% 27,1% 15,7% Fem 14% 12,8% 5,6% 14,5% 10,2% Escolaridad 0-2 22,1% 33,3% 11,3% 29,4% 16,2% 3-4 16,3% 21,4% 23,5% 13,7% 5-8 14,4% 17,7% 6,1% 12% ≥ 9 10,4% 13,6% 6,0% 15,2% 10,6%

12
Tasas de mortalidad – Tendencias (ajustado por edad)
Enfermedad Coronaria Otras causas ECV EPOC 2.0 1.5 1.0 0.5 EUA 1966–1998 Proporción de la tasa de 1966 Vital Statistics of the US (NHS)
")
13
Mortalidad Futura Global
Cardiopatía Isquémica Enfermedad Cerebrovascular IVRI Enfermedad Diarreica Trastornos Perinatales EPOC Tuberculosis Sarampión Accidentes de tránsito Cáncer de pulmón 3ro 6to Cáncer gástrico VIH Suicidio Murray & Lopez: Lancet 1997

14
Muertes atribuibles a la EPOC por sexo
Hombres 70 Mujeres 60 50 40 Muertes x1000 habitantes 30 20 Sexo y mortalidad por EPOC Una tendencia notable en los datos de mortalidad por EPOC en EUA es una mayor mortalidad en las mujeres en general. El número total de mujeres que se mueren de EPOC ahora supera el de los hombres. Este aumento en las muertes por EPOC entre las mujeres puede reflejar una mayor prevalencia de fumado.1 Los Centros para el control y prevención de enfermedades (CDC) de los EUA señalaron que, a pesar de que la mortalidad por cualquier causa bajó 32% en hombres y 14% en mujeres en el período 1968–1999, la tasa de mortalidad por EPOC en el mismo período aumentó 382% para las mujeres y 27% para los hombres.1,2 1. Mannino DM & Kiri VA. Int J Chron Obstruct Pulmon Dis 2006;1:219–233. 2. Centros para el control y prevención de enfermedades . MMWR CDC Surveill Summ 2002;51:1–16. 10 1980 1985 1990 1995 2000 Centros De Control Y Prevención De Enfermedades De Los EUA MMWR Surveill Summ 2002;51:1–16.
 de los EUA señalaron que, a pesar de que la mortalidad por cualquier causa bajó 32% en hombres y 14% en mujeres en el período 1968–1999, la tasa de mortalidad por EPOC en el mismo período aumentó 382% para las mujeres y 27% para los hombres.1,2. 1. Mannino DM & Kiri VA. Int J Chron Obstruct Pulmon Dis 2006;1:219– Centros para el control y prevención de enfermedades . MMWR CDC Surveill Summ 2002;51:1– Centros De Control Y Prevención De Enfermedades De Los EUA MMWR Surveill Summ 2002;51:1–16.")
15
mortal Fumar es un placer, genial, sensual,

16
Factores de riesgo para EPOC
Infecciones Genética

17
Patogénesis

18
Patogénesis de la EPOC Insulto Disnea Calidad de vida
Fibrosis peribronquial Destrucción alveolar Hiperplasia glandular Inflamación pulmonar Disnea Inflamación sistémica Capacidad ejercicio Calidad de vida Insulto Exacerbaciones Comorbilidades Explica las diferentes dimensiones de la EPOC e incluye el compromiso sistémico de la enfermedad. Atrofia/Disfunción muscular Pérdida de peso Enfermedad CV Osteoporosis Depresión

19
Desacondicionamiento de Capacidad de Ejercicio
EPOC: Curso clínico Insulto Exacerbaciones Obstrucción Atrapamiento Hiperinsuflación Inactividad Desuso - Miopatía Desacondicionamiento The physiological impairment in COPD is characterized by expiratory flow limitation, air trapping, and hyperinflation. These physiological abnormalities impact patients everyday causing them to become breathless easily when the minute ventilation is increased for example during exercise. Dyspnea in itself is unpleasant, and it also severely limits the amount of activity a patient can undertake. Often patients will avoid situations that demand physical activity. Avoiding activity leads to deconditioning and worsening of the disease and, ultimately, the patient’s health-related quality of life (HRQL) suffers. COPD exacerbations (intermittent worsenings), which occur during the course of the disease, contribute to the deterioration in the patient’s HRQL and may also contribute to the overall progressive decline in lung function. Disnea Disfunción muscular de Capacidad de Ejercicio Depresión Enfermedad CV Osteoporosis Calidad de Vida
 suffers. COPD exacerbations (intermittent worsenings), which occur during the course of the disease, contribute to the deterioration in the patient’s HRQL and may also contribute to the overall progressive decline in lung function. Disnea. Disfunción muscular. de Capacidad de Ejercicio. Depresión. Enfermedad CV. Osteoporosis. Calidad de Vida.")
20
de Capacidad de Ejercicio
Dimensiones de la EPOC Biológica Anatómica Fibrosis peribronquial Destrucción alveolar Hiperplasia glandular Fisiológica VEF1/CVF Tiempo Vol. VEF1 CVF VRI VR VRE VC Clínica Disfunción muscular Calidad de Vida de Capacidad de Ejercicio Disnea Mastocito Macrófago Alveolar Neutrófilos CD8+ T-Linfocito Proteasas Enfisema Hipersecreción Mucoide Irritante inhalado TNF INF Depresión Pérdida de peso Enfermedad CV Osteoporosis La EPOC se entiende hoy como el resultado de una respuesta inflamatoria del parénquima pulmonar al insulto producido por la inhalación de sustancias tóxicas, particularmente de humo de cigarrillo. El proceso inflamatorio puede ser detectado en sangre periférica lo cual permite calificarlo como “sistémico”. Hay evidencia de que la EPOC se acompaña de: niveles elevados de citokinas proinflamatorias (ej Factor de necrosis tumoral [TNF-], interleukina 6 y 8 [IL-6, IL-8]), niveles elevados de reactantes de fase aguda (ej. Proteina C reactiva [CRP]), estrés oxidativo, y activación de varias células inflamatorias (neutrófilos, monocitos y linfocitos). IL-6, IL-8, PCR Medidas de Inflamación Local y Sistémica Estudios Anatómicos o de Imágenes Estudios Fisiológicos Estudios Funcionales
, niveles elevados de reactantes de fase aguda (ej. Proteina C reactiva [CRP]), estrés oxidativo, y. activación de varias células inflamatorias (neutrófilos, monocitos y linfocitos). IL-6, IL-8, PCR. Medidas de Inflamación Local y Sistémica. Estudios Anatómicos o de Imágenes. Estudios Fisiológicos. Estudios Funcionales.")
21
Cuatro Componentes del Manejo de la EPOC
Valorar y monitorizar la enfermedad Reducir los factores de riesgo Manejo de EPOC Estable Educación No-farmacológico Farmacológico Manejo exacerbaciones

22
Metas del manejo de EPOC
Alivio de los síntomas Prevenir la progresión de la enfermedad Mejorar la tolerancia al ejercicio Mejorar el estado general de salud Prevenir y tratar complicaciones Prevenir y tratar exacerbaciones Reducir mortalidad

23
Componentes del Manejo del EPOC
Valorar y monitorizar la enfermedad Reducir los factores de riesgo Manejo del EPOC Estable Educación No-farmacológico Farmacológico

24
Diagnóstico de EPOC è è è ESPIROMETRIA EXPOSICIÓN A FACTORES DE RIESGO
SINTOMAS tos tabaco ocupación esputo contaminación ambiental disnea è è è A diagnosis of COPD should be considered in any patient who has cough, sputum production, or dyspnea and/or a history of exposure to risk factors. The diagnosis is confirmed by spirometry. To help identify individuals earlier in the course of disease, spirometry should be performed for patients who have chronic cough and sputum production even if they do not have dyspnea. Spirometry is the best way to diagnose COPD and to monitor its progression and health care workers to care for COPD patients should have assess to spirometry. ESPIROMETRIA VEF1/CVF < 70% post-broncodilatador VEF1 predicho post-broncodilatador disminuído Poca reversibilidad < 12% Obstrucción progresiva

25
Clasificación de Severidad de EPOC por Espirometría
Fase I: Leve VEF1/CVF < 0.70 VEF1 > 80% predicho Fase II: Moderada VEF1/CVF < 0.70 50% < VEF1 < 80% predicho Fase III: Severa VEF1/CVF < 0.70 30% < VEF1 < 50% predicho Fase IV: Muy Severa VEF1/CVF < 0.70 VEF1 < 30% predicho o VEF1 < 50% predicho más insuficiencia respiratoria crónica

26
Componentes del Manejo del EPOC
Valorar y monitorizar la enfermedad Reducir los factores de riesgo Manejo del EPOC Estable Educación No-farmacológico Farmacológico

27
Reducir Factores de Riesgo
Manejo de EPOC estable Reducir Factores de Riesgo Reducir la exposición a: Humo de tabaco Aerosoles y químicos ocupacionales Contaminantes domiciliares y ambientales La cesación del fumado es la medida aislada más efectiva — y costo efectiva — en la mayor parte de la población para reducir el riesgo de desarrollar EPOC y detener su progresión (Evidencia A).
.")
28
Componentes del Manejo del EPOC
Valorar y monitorizar la enfermedad Reducir los factores de riesgo Abordaje de EPOC Estable Educación No-farmacológico Farmacológico

29
Manejo de EPOC estable La educación a los pacientes con EPOC juega un papel vital en: Cesación de fumado (Evidencia A) Mejoría de habilidades Capacidad para lidiar con la enfermedad Condición de salud

30
Medidas no farmacológicas
Intervenciones directas con el paciente ¡EDUCACIÓN AL PACIENTE! Uso de inhaladores Planes de acción Ejercicios respiratorios Técnicas de relajación Nutrición Apoyo en cesación de fumado Uso adecuado ha demostrado hasta 40% de reducción de internamientos por exacerbación de EPOC. Bourbeau et al. Arch Intern Med. 2003;163:585

31
Medidas farmacológicas

32
Manejo de EPOC estable Ninguno de los medicamentos existentes para EPOC ha demostrado modificar la pérdida a largo plazo de la función pulmonar que caracteriza a la enfermedad (Evidencia A) por lo tanto, la farmacoterapia es usada para disminuir los síntomas y/o complicaciones NHLBI/WHO Global Initiative for Chronic Obstructive Pulmonary Disease (GOLD) 2009
 por lo tanto, la farmacoterapia es usada para disminuir los síntomas y/o complicaciones. NHLBI/WHO Global Initiative for Chronic Obstructive Pulmonary Disease (GOLD)")
33
Broncodilatadores Anti-inflamatorios Acción Corta Acción prolongada
Corticosteroides Beta-agonistas Salbutamol Beta-agonistas Salmeterol Formoterol Oral/Parenteral (uso agudo) Inhalados* Beclometasona Fluticasona Budesonida Mometasona Anti-colinérgicos Ipratropio Anti-colinérgicos Tiotropio Teofilina
 Inhalados* Beclometasona. Fluticasona. Budesonida. Mometasona. Anti-colinérgicos. Ipratropio. Anti-colinérgicos. Tiotropio. Teofilina.")
34
Manejo de EPOC estable Broncodilatadores
Tendrán un papel central para el manejo de los síntomas (Evidencia A). Se indican PRN o en forma regular para prevenir o reducir síntomas y exacerbaciones. El tratamiento regular con broncodilatadores de acción prolongada será más efectivo y conveniente que el tratamiento con broncodilatadores de acción corta (Evidencia A).
. Se indican PRN o en forma regular para prevenir o reducir síntomas y exacerbaciones. El tratamiento regular con broncodilatadores de acción prolongada será más efectivo y conveniente que el tratamiento con broncodilatadores de acción corta (Evidencia A).")
35
Vincken et al, Eur Respir J 2002 Casaburi et al, Eur Respir J 2002

36
A 4-Year Trial of Tiotropium in Chronic Obstructive Pulmonary Disease
Volume 359: October 9, 2008

37
UPLIFT: estudio multicéntrico, multinacional (37 países),
aleatorizado, doble ciego, controlado con placebo, 5993 pacientes, iniciado en Diciembre de 2002. Europa países Asia países América 4 países África y Medio Oriente 1 país Oceanía 2 países 5,993 pacientes en 37 países

38
UPLIFT® Diseño y método
Pre-inclusión 2- 4 semanas Periodo de tratamiento 4 años (48 meses) Seguimiento de 30 días 1440 días 1470 días Tiotropio 18 µg al día Todos los medicamentos respiratorios prescritos Suspender: Tiotropio Iniciar: Ipratropio Todos los medicamentos respiratorios prescritos, excepto los anticolinérgicos inhalados Se permitieron todos los medicamentos respiratorios previamente prescritos, excepto los anticolinérgicos inhalados Placebo Día 1 Aleatorización Día 30 4 años Fin del estudio Fin del seguimiento Selección Semestral Espirometría Espirometría + CRSJ Espirometría Espirometría + CRSJ Espirometría + CRSJ Espirometría Estado vital CRSJ. Cuestionario respiratorio de San Jorge
 Seguimiento de 30 días días días. Tiotropio 18 µg al día. Todos los medicamentos. respiratorios prescritos. Suspender: Tiotropio. Iniciar: Ipratropio. Todos los medicamentos respiratorios prescritos, excepto los anticolinérgicos inhalados. Se permitieron todos los medicamentos respiratorios previamente prescritos, excepto los anticolinérgicos inhalados. Placebo. Día 1. Aleatorización. Día años. Fin del estudio. Fin del. seguimiento. Selección. Semestral. Espirometría. Espirometría. + CRSJ. Espirometría. Espirometría. + CRSJ. Espirometría. + CRSJ. Espirometría. Estado vital. CRSJ. Cuestionario respiratorio de San Jorge.")
39
Objetivos del estudio Evaluar el cambio en la tasa de declinación de la función pulmonar (VEF1 pre y posbroncodilador), así como la mejoría en las siguientes variables: Función pulmonar Calidad de vida relacionada con la salud Exacerbaciones Hospitalizaciones debidas a exacerbaciones Mortalidad
, así como la mejoría en las siguientes variables: Función pulmonar. Calidad de vida relacionada con la salud. Exacerbaciones. Hospitalizaciones debidas a exacerbaciones. Mortalidad.")
40
Mejora en la función pulmonar
* * * * * * * * * (n=2494) VEF1 pre-broncodilatación = 87 – 103 mL (n=2363) 1 6 12 18 24 30 36 42 48 Día 30 (Estado basal) Mes 40
 VEF1. pre-broncodilatación. = 87 – 103 mL. (n=2363) Día 30. (Estado basal) Mes. 40.")
41
Calificación total CRSJ Valores medios en cada punto del tiempo
Mejora estadísticamente significativa durante los 4 años del estudio 6 12 18 24 30 36 42 48 Mes * *p< vs. placebo Mejoría Basal

42
Reducción de mortalidad con tiotropio
16% de reducción del riesgo de muerte estadísticamente significativa Meses p=0.016

43
Probabilidad de exacerbación o de hospitalización por exacerbación
Reducción de un 14% en exacerbaciones Reducción de un 14% en hospitalizaciones por exacerbaciones

44
Broncodilatadores Anti-inflamatorios Acción Corta Acción prolongada
Corticosteroides Beta-agonistas Salbutamol Beta-agonistas Salmeterol Formoterol Oral/Parenteral (uso agudo) Inhalados Beclometasona Fluticasona Budesonida Mometasona Anti-colinérgicos Ipratropio Anti-colinérgicos Tiotropio Teofilina
 Inhalados. Beclometasona. Fluticasona. Budesonida. Mometasona. Anti-colinérgicos. Ipratropio. Anti-colinérgicos. Tiotropio. Teofilina.")
45
Manejo de EPOC estable Glucocorticoides
El agregar tratamiento regular con esteroides inhalados al tratamiento broncodilatador está indicado en pacientes sintomáticos con un VEF1 < 50% predicho (Fase III: EPOC Severo y Fase IV: EPOC Muy Severo) y con exacerbaciones a repetición (Evidencia A). Pauwels RA, et al. Am J Resp Crit Care Med. 2001:163;1256, ATS-ERS Consensus statement -2004
 y con exacerbaciones a repetición (Evidencia A). Pauwels RA, et al. Am J Resp Crit Care Med. 2001:163;1256, ATS-ERS Consensus statement")
46
Relative Risk of Exacerbations in COPD Patients Treated With ICS: A Meta-analysis
Reference Vestbo et al., 1999 Bourbeau et al., 1998 Burge et al., 2000 Lung Health Study, 2000 Weir et al., 1999 Paggiaro et al., 1998 General Overall relative risk = 0.70 0.5 1.0 1.5 2.0 2.5 3.0 Relative Risk Alsaeedi et al. Am J Med. 2002;113:59-65.

48
Broncodilatadores Anti-inflamatorios Acción Corta Acción prolongada
Corticosteroides Beta-agonistas Salbutamol Beta-agonistas Salmeterol Formoterol Oral/Parenteral (uso agudo) Inhalados Beclometasona Fluticasona Budesonida Mometasona Anti-colinérgicos Ipratropio Anti-colinérgicos Tiotropio Teofilina Combinación ICS + LABA
 Inhalados. Beclometasona. Fluticasona. Budesonida. Mometasona. Anti-colinérgicos. Ipratropio. Anti-colinérgicos. Tiotropio. Teofilina. Combinación ICS + LABA.")
49
La combinación de un esteroide inhalado con un ß2-agonista de acción prolongada (LABA) será más efectiva que los componentes individuales (Evidencia A) Los corticosteroides aumentan la transcripción genética del receptor β2, lo que resulta en una mayor expresión de receptores β2 Los agonistas β2 tienen un efecto positivo en los receptores de glucocorticoides, y mejoran la recolocación, la unión de elementos en respuesta al glucocorticoide, y los efectos antiinflamatorios NHLBI/WHO Global Initiative for Chronic Obstructive Pulmonary Disease (GOLD) 2009 Barnes PJ. Eur Respir J 2002;19:182–191
 Barnes PJ. Eur Respir J 2002;19:182–191.")
50
Szafranski et al. ERJ 2003 Calverley et al. Lancet 2003

51
Tasa de exacerbaciones vs. placebo (%)
Symbicort reduce la tasa de exacerbaciones que requieren intervención médica* *P < 0.05 vs. placebo; P = vs. formoterol; P = NS vs. budesonida Tasa de exacerbaciones vs. placebo (%) –30 –25 –20 –15 –10 –5 Symbicort Budesonida Formoterol –15% –2% –24% * Symbicort® reduce la tasa de exacerbaciones que requieren intervención médica (uso de esteroides orales o antibióticos u hospitalización por síntomas respiratorios) En este estudio a doble ciego, controlado con placebo, de grupos paralelos, por Szafranski et al., pacientes con EPOC (GOLD stage III y IV) fueron asignados aleatoriamente para recibir Symbicort (2 x 160/4.5 mcg b.i.d.), budesonida (2 x 200 mcg b.i.d.), formoterol (2 x 4.5 mcg b.i.d.) o placebo, con terbutalina (0.5 mg) por demanda. Symbicort significativamente redujo la tasa de exacerbaciones graves en 24% comparado con placebo (P < 0.05) y 23% comparado con formoterol (P = 0.043). Szafranski W, et al. Eur Respir J 2003;21:74–81. *intervención médica = use de esteroides orales o antibióticos u hospitalización por síntomas respiratorios Szafranski W, et al. Eur Respir J 2003;21:74–81.
 –30. –25. –20. –15. –10. –5. Symbicort. Budesonida. Formoterol. –15% –2% –24% * Symbicort® reduce la tasa de exacerbaciones que requieren intervención médica (uso de esteroides orales o antibióticos u hospitalización por síntomas respiratorios) En este estudio a doble ciego, controlado con placebo, de grupos paralelos, por Szafranski et al., pacientes con EPOC (GOLD stage III y IV) fueron asignados aleatoriamente para recibir Symbicort (2 x 160/4.5 mcg b.i.d.), budesonida (2 x 200 mcg b.i.d.), formoterol (2 x 4.5 mcg b.i.d.) o placebo, con terbutalina (0.5 mg) por demanda. Symbicort significativamente redujo la tasa de exacerbaciones graves en 24% comparado con placebo (P < 0.05) y 23% comparado con formoterol (P = 0.043). Szafranski W, et al. Eur Respir J 2003;21:74–81. *intervención médica = use de esteroides orales o antibióticos u hospitalización por síntomas respiratorios. Szafranski W, et al. Eur Respir J 2003;21:74–81.")
52
TORCH: TOwards a Revolution in COPD Health

53
Tiempo desde el inicio del tratamiento en días
Análisis Post-hoc ISOLDE: sugiere tendencia de aumento de sobrevida con FP Sobrevida acumulada 1.00 p=0.069 0.90 0.80 FP 0.70 Placebo 0.60 The Global Initiative for Chronic Obstructive Pulmonary Disease (GOLD) guidelines state that none of the existing medications for COPD have been conclusively shown to modify long-term decline in lung function or to significantly impact mortality.1 However, there are some indications from completed clinical trials that inhaled corticosteroids (ICS) may reduce mortality in patients with COPD. In a post-hoc analysis of the Inhaled Steroids in Obstructive Lung Disease in Europe study (ISOLDE) study, researchers followed-up deaths in all randomised patients, including withdrawn patients.2 Date and cause of death were established and patients who withdrew from the trial were found to have a higher death rate from most causes compared with those who remained in the trial. Additionally, patients randomised to fluticasone propionate (FP) appeared to die later than those randomised to placebo (p = 0.069). However, as patients received other medication for their COPD after withdrawal from the study a causal relationship to treatment cannot be confirmed. The TORCH study was powered based on the results of ISOLDE and assumed there would be a placebo death rate of 17% on placebo over 3 years and a 12.7% death rate on SFC. References 1. Pauwels RA, Buist AS, Calverley PM, et al. Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop Summary. Am J Respir Crit Care Med 2001;163:1256–76. 2. Waterhouse JC, Fishwick D, Anderson JA, et al. What caused death in the ISOLDE study? Eur Respir J 1999;14(Suppl. 30): 387s. 0.50 100 200 300 400 500 600 700 800 900 1,000 1,100 1,200 Tiempo desde el inicio del tratamiento en días ISOLDE = Inhaled Steroids in Obstructive Lung Disease in Europe study FP = Propionato de fluticasona Waterhouse et al. Eur Respir J 1999
 guidelines state that none of the existing medications for COPD have been conclusively shown to modify long-term decline in lung function or to significantly impact mortality.1 However, there are some indications from completed clinical trials that inhaled corticosteroids (ICS) may reduce mortality in patients with COPD. In a post-hoc analysis of the Inhaled Steroids in Obstructive Lung Disease in Europe study (ISOLDE) study, researchers followed-up deaths in all randomised patients, including withdrawn patients.2 Date and cause of death were established and patients who withdrew from the trial were found to have a higher death rate from most causes compared with those who remained in the trial. Additionally, patients randomised to fluticasone propionate (FP) appeared to die later than those randomised to placebo (p = 0.069). However, as patients received other medication for their COPD after withdrawal from the study a causal relationship to treatment cannot be confirmed. The TORCH study was powered based on the results of ISOLDE and assumed there would be a placebo death rate of 17% on placebo over 3 years and a 12.7% death rate on SFC. References. 1. Pauwels RA, Buist AS, Calverley PM, et al. Global strategy for the diagnosis, management and prevention of chronic obstructive pulmonary disease. NHLBI/WHO Global Initiative for Chronic Obstructive Lung Disease (GOLD) Workshop Summary. Am J Respir Crit Care Med 2001;163:1256– Waterhouse JC, Fishwick D, Anderson JA, et al. What caused death in the ISOLDE study Eur Respir J 1999;14(Suppl. 30): 387s ,000. 1,100. 1,200. Tiempo desde el inicio del tratamiento en días. ISOLDE = Inhaled Steroids in Obstructive. Lung Disease in Europe study. FP = Propionato de fluticasona. Waterhouse et al. Eur Respir J")
54
TORCH: Participación de 444 centros en 42 países
The TORCH study recruited patients from 444 centres in a total of 42 countries worldwide, including the Americas, Europe, Australasia, Asia and Africa.1 Reference 1. Vestbo J, TORCH Study Group. The TORCH (TOwards a Revolution in COPD Health) survival study protocol. Eur Respir J 2004;24:206–10.
 survival study protocol. Eur Respir J 2004;24:206–10.")
55
Diseño del estudio TORCH
Inducción Asignación aleatoria Tratamiento Seguimiento Salmeterol/fluticasona DPI 50/500 mcg b.i.d. (N=1533) Fluticasona DPI 500 mcg b.i.d. (N=1534) Salmeterol DPI 50 mcg b.i.d. (N=1521) Placebo (N= 1524) El estudio Hacia una Revolución en la Salud en la EPOC (TORCH) El estudio TORCH fue un estudio de 3 años, internacional, multicéntrico, controlado, a doble ciego, aleatorio, de grupos paralelos, conducido pacientes con EPOC moderada a grave. El objetivo primario en TORCH fue la reducción en la mortalidad por cualquier causa entre salmeterol/fluticasona DPI y placebo. Los criterios de inclusión para pacientes en TORCH fueron: edad 40–80 años, historial clínico establecido de EPOC, historia de fumado de ≥ 10 años-paquete, VEF1 basal< 60% del pronóstico normal (prebroncodilatador), < 10% reversibilidad en pronóstico VEF1 y razón VEF1/capacidad vital forzada (CVF) ≤ 70%. Tras 2 semanas de inducción, los pacientes (n = 6112) fueron asignados al azar para recibir salmeterol DPI (50 mcg b.i.d.), fluticasona DPI (500 mcg b.i.d.), salmeterol/fluticasona DPI (50/500 mcg b.i.d.) o placebo, por un periodo de tratamiento de 3 años. Se permitieron medicamentos para condiciones distintas a la EPOC durante el estudio. TORCH fue un estudio de intención de tratamiento, lo que significa que si los pacientes no cumplían bien con su medicamento de estudio, o no lo tomaban, aún contaban en el grupo original al que fueron asignados. Para que un estudio sea realmente aleatorio, se debe asegurar que todos los pacientes se analicen en los grupos en los que fueron asignados al azar, pues de lo contrario algún grupo se vería favorecido sobre el otro en los resultados. Vestbo J, et al. Eur Respir J 2004;24:206–210. Calverley PM, et al. New Engl J Med 2007;356:775–789. Salbutamol disponible como medicamento de rescate para todos los pacientes Mes: –0.5 12 24 36.5 36 Objetivo primario: mortalidad por cualquier causa a los 3 años. N= 6112 Vestbo J, et al. Eur Respir J 2004;24:206–210; Calverley PM, et al. New Engl J Med 2007;356:775–789. .
 Fluticasona DPI 500 mcg b.i.d. (N=1534) Salmeterol DPI 50 mcg b.i.d. (N=1521) Placebo (N= 1524) El estudio Hacia una Revolución en la Salud en la EPOC (TORCH) El estudio TORCH fue un estudio de 3 años, internacional, multicéntrico, controlado, a doble ciego, aleatorio, de grupos paralelos, conducido pacientes con EPOC moderada a grave. El objetivo primario en TORCH fue la reducción en la mortalidad por cualquier causa entre salmeterol/fluticasona DPI y placebo. Los criterios de inclusión para pacientes en TORCH fueron: edad 40–80 años, historial clínico establecido de EPOC, historia de fumado de ≥ 10 años-paquete, VEF1 basal< 60% del pronóstico normal (prebroncodilatador), < 10% reversibilidad en pronóstico VEF1 y razón VEF1/capacidad vital forzada (CVF) ≤ 70%. Tras 2 semanas de inducción, los pacientes (n = 6112) fueron asignados al azar para recibir salmeterol DPI (50 mcg b.i.d.), fluticasona DPI (500 mcg b.i.d.), salmeterol/fluticasona DPI (50/500 mcg b.i.d.) o placebo, por un periodo de tratamiento de 3 años. Se permitieron medicamentos para condiciones distintas a la EPOC durante el estudio. TORCH fue un estudio de intención de tratamiento, lo que significa que si los pacientes no cumplían bien con su medicamento de estudio, o no lo tomaban, aún contaban en el grupo original al que fueron asignados. Para que un estudio sea realmente aleatorio, se debe asegurar que todos los pacientes se analicen en los grupos en los que fueron asignados al azar, pues de lo contrario algún grupo se vería favorecido sobre el otro en los resultados. Vestbo J, et al. Eur Respir J 2004;24:206–210. Calverley PM, et al. New Engl J Med 2007;356:775–789. Salbutamol disponible como medicamento de rescate para todos los pacientes. Mes: – Objetivo primario: mortalidad por cualquier causa a los 3 años. N= Vestbo J, et al. Eur Respir J 2004;24:206–210; Calverley PM, et al. New Engl J Med 2007;356:775–")
56
TORCH: objetivos evaluados
Objetivo primario Efecto de SFC 50/500 mg vs placebo en todas las causas de muerte en tres años de seguimiento de pacientes con EPOC moderado y severo Objetivos secundarios Efecto de SFC 50/500 mg en la tasa de exacerbaciones moderadas y severas Efecto de SFC 50/500 mg en la Calidad de vida (SGRQ) de los pacientes con EPOC The primary endpoint of the TORCH trial1 was the effect of SFC 50/500 µg combination versus placebo on all-cause mortality over 3 years in patients with moderate-to-severe COPD. All-cause mortality was chosen as the primary endpoint as COPD because it is important to ensure that treatment is not reducing mortality from one cause, while increasing mortality from another. This makes all-cause mortality a more robust endpoint than looking for one single cause of death. COPD is a multicomponent disease and patients die from causes other than COPD, including lung cancer, heart disease and stroke.2 Additionally, all-cause mortality is not dependent on coding practice, which can differ between countries, and it can be very difficult to reliably differentiate between death due to COPD specifically and that where COPD was a contributing factor. Lastly, choosing all-cause mortality as the primary endpoint gave us the greatest power for the study because of the likely number of events Patients who withdrew prematurely from the study were also followed-up with regular contact for 3 years from the date of randomisation in order to determine survival status. Secondary endpoints of the TORCH trial were: COPD morbidity as measured by the rate of exacerbations Health-related quality of life (HRQoL) as measured by the St. George’s Respiratory Questionnaire (SGRQ) at 24-weekly intervals. References 1. Vestbo J, TORCH Study Group. The TORCH (TOwards a Revolution in COPD Health) survival study protocol. Eur Respir J 2004;24:206–10. 2. Sin DD, Anthonisen NR, Soriano JB, Agusti AG. Mortality in COPD: role of comorbidities. Eur Respir J 2006; accepted. SGRQ = St. George’s Respiratory Questionnaire Vestbo et al. Eur Respir J 2004
 de los pacientes con EPOC. The primary endpoint of the TORCH trial1 was the effect of SFC 50/500 µg combination versus placebo on all-cause mortality over 3 years in patients with moderate-to-severe COPD. All-cause mortality was chosen as the primary endpoint as COPD because it is important to ensure that treatment is not reducing mortality from one cause, while increasing mortality from another. This makes all-cause mortality a more robust endpoint than looking for one single cause of death. COPD is a multicomponent disease and patients die from causes other than COPD, including lung cancer, heart disease and stroke.2 Additionally, all-cause mortality is not dependent on coding practice, which can differ between countries, and it can be very difficult to reliably differentiate between death due to COPD specifically and that where COPD was a contributing factor. Lastly, choosing all-cause mortality as the primary endpoint gave us the greatest power for the study because of the likely number of events. Patients who withdrew prematurely from the study were also followed-up with regular contact for 3 years from the date of randomisation in order to determine survival status. Secondary endpoints of the TORCH trial were: COPD morbidity as measured by the rate of exacerbations. Health-related quality of life (HRQoL) as measured by the St. George’s Respiratory Questionnaire (SGRQ) at 24-weekly intervals. References. 1. Vestbo J, TORCH Study Group. The TORCH (TOwards a Revolution in COPD Health) survival study protocol. Eur Respir J 2004;24:206– Sin DD, Anthonisen NR, Soriano JB, Agusti AG. Mortality in COPD: role of comorbidities. Eur Respir J 2006; accepted. SGRQ = St. George’s Respiratory Questionnaire. Vestbo et al. Eur Respir J")
57
Resultados: Mortalidad

59
Análisis primario: mortalidad a 3 años por todas las causas
Reducción del riesgo: 17.5% p = 0,052 Probabilidad de muerte (%) 18 16 Placebo 15.2% 14 SFC % 12 10 8 Reducción absoluta 2.6% 6 4 The proportions of deaths from any cause at 3 years were 12.6% in the combination therapy group, 15.2% in the placebo group. The absolute risk reduction for death in the combination-therapy group as compared with the placebo group was 2.6%; a reduction in the risk of death at any time in the 3 years was 17.5%, P = 0.052 The survival status of 6111/6112 patients was established. One subject in the SFC arm with survival status unknown at 3 years was treated as censored at 2 years (113 weeks) (the last time point at which survival status was known). The difference in all-cause mortality between SFC and placebo was analysed by the log-rank test (stratified by smoking status) and presented as a Kaplan-Meier plot and calculated hazard ratios. The log-rank test is a popular method for comparing the survival of groups that takes into account the whole follow-up period. It was used to test the null hypothesis that there was no difference between treatment groups in the probability of an event (death) at any time point. The unadjusted hazard ratio for time to all-cause mortality at 3 years between SFC versus placebo was 0.820, p= This p value must be compared to a significance level of p=0.04 because of the interim analyses. The adjusted Hazard Ratio for time to all-cause mortality at 3 years between SFC versus placebo was 0.825, indicating a 17.5% reduction in the risk of death from any cause (p=0.052). The absolute risk reduction with SFC was 2.6% compared with placebo. Although the difference between SFC and placebo was on the edge of the pre-specified p-value of 0.05, it is debatable whether this modest reduction in confidence about the significance of the mortality data invalidates the conclusions. The number of deaths in this 4-limb trial was substantial (875 in the ITT population in total, 193 on SFC and 231 on placebo), although still less than anticipated (the study was powered assuming 440 deaths for SFC and placebo in total, whereas we actually had 424). We powered the study assuming a 17% placebo mortality rate over 3 years whereas our placebo rate was only 15.2%). This, together with the impact of the interim analyses, may explain the observed significance level for the primary outcome. Reference Calverley PMA, Anderson JA, Celli B. for the TORCH investigators. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. NEJM 2007; 356(8): 2 12 24 36 48 60 72 84 96 108 120 132 144 156 Tiempo hasta la muerte (semanas) Pacientes Vivos 1524 1533 1464 1487 1399 1426 1293 1339 Calverley et al. NEJM 2007
 Placebo 15.2% 14. SFC 12.6% Reducción absoluta 2.6% The proportions of deaths from any cause at 3 years were 12.6% in the combination therapy group, 15.2% in the placebo group. The absolute risk reduction for death in the combination-therapy group as compared with the placebo group was 2.6%; a reduction in the risk of death at any time in the 3 years was 17.5%, P = The survival status of 6111/6112 patients was established. One subject in the SFC arm with survival status unknown at 3 years was treated as censored at 2 years (113 weeks) (the last time point at which survival status was known). The difference in all-cause mortality between SFC and placebo was analysed by the log-rank test (stratified by smoking status) and presented as a Kaplan-Meier plot and calculated hazard ratios. The log-rank test is a popular method for comparing the survival of groups that takes into account the whole follow-up period. It was used to test the null hypothesis that there was no difference between treatment groups in the probability of an event (death) at any time point. The unadjusted hazard ratio for time to all-cause mortality at 3 years between SFC versus placebo was 0.820, p= This p value must be compared to a significance level of p=0.04 because of the interim analyses. The adjusted Hazard Ratio for time to all-cause mortality at 3 years between SFC versus placebo was 0.825, indicating a 17.5% reduction in the risk of death from any cause (p=0.052). The absolute risk reduction with SFC was 2.6% compared with placebo. Although the difference between SFC and placebo was on the edge of the pre-specified p-value of 0.05, it is debatable whether this modest reduction in confidence about the significance of the mortality data invalidates the conclusions. The number of deaths in this 4-limb trial was substantial (875 in the ITT population in total, 193 on SFC and 231 on placebo), although still less than anticipated (the study was powered assuming 440 deaths for SFC and placebo in total, whereas we actually had 424). We powered the study assuming a 17% placebo mortality rate over 3 years whereas our placebo rate was only 15.2%). This, together with the impact of the interim analyses, may explain the observed significance level for the primary outcome. Reference. Calverley PMA, Anderson JA, Celli B. for the TORCH investigators. Salmeterol and fluticasone propionate and survival in chronic obstructive pulmonary disease. NEJM 2007; 356(8): Tiempo hasta la muerte (semanas) Pacientes. Vivos Calverley et al. NEJM")
60
Objetivos secundarios del estudio y otros parámetros de eficacia

61
Tasa de exacerbaciones moderadas y severas a lo largo de tres años
Media de exacerbaciones/año 25% reducción 1.2 1.13 0.97* 1 0.93* 0.85*†‡ 0.8 0.6 0.4 Moderate exacerbaciones are defined as those which require Tratamiento with systemic corticosteroids and/or antibiotics; grave exacerbaciones are defined as those which require hospitalisation. The exacerbation rate was calculated as the total number de moderate and/or grave exacerbaciones experienced by a patient during the Tratamiento period. The number de exacerbaciones was analysed using a generalised linear model, assuming the Negative Binomial distribution, with time on Tratamiento as an offset variable. The model included adjustments for the effects de smoking status, age, gender, baseline FEV1, number de exacerbaciones reported in the 12 months prior to screening, y region. SERETIDE significantly lowered the rate de moderate/grave exacerbaciones compared with placebo (25% reducción, p < 0.001), SALM (12% reducción, p = 0.002) y FP (9% reducción, p = 0.024). SALM y FP also had significantly lower exacerbation rates than placebo (15%, p < y 18%, p < 0.001, respectively). SERETIDE reduced the rate de moderate-to-grave exacerbaciones to a much greater extent than placebo or either de the component monotherapies. exacerbaciones y hospitalisations predict the risk de dying from EPOCover 5 años.1 Reference Soler-Cataluna JJ, Martinez-Garcia MA, Roman Sanchez P, et al. grave acute exacerbaciones y mortalidadin patients with chronic obstructive pulmonary disease. Thorax 2005;60:925–31. 0.2 Placebo SALM FP SFC Tratamiento Calverley et al. NEJM 2007 *p < vs. placebo; †p = vs. SALM; ‡p = vs. FP
, SALM (12% reducción, p = 0.002) y FP (9% reducción, p = 0.024). SALM y FP also had significantly lower exacerbation rates than placebo (15%, p < y 18%, p < 0.001, respectively). SERETIDE reduced the rate de moderate-to-grave exacerbaciones to a much greater extent than placebo or either de the component monotherapies. exacerbaciones y hospitalisations predict the risk de dying from EPOCover 5 años.1. Reference. Soler-Cataluna JJ, Martinez-Garcia MA, Roman Sanchez P, et al. grave acute exacerbaciones y mortalidadin patients with chronic obstructive pulmonary disease. Thorax 2005;60:925– Placebo. SALM. FP. SFC. Tratamiento. Calverley et al. NEJM *p < vs. placebo; †p = vs. SALM; ‡p = vs. FP.")
62
Tasa de exacerbaciones requiriendo corticosteroides sistémicos en tres años
Media de exacerbaciones/año 1.2 1 43% reducción 0.80 0.8 0.64* 0.6 0.52* 0.46*†‡ 0.4 Moderate exacerbaciones are defined as those which require Tratamiento with systemic corticosteroids and/or antibiotics; grave exacerbaciones are defined as those which require hospitalisation. The exacerbation rate was calculated as the total number de moderate and/or grave exacerbaciones experienced by a patient during the Tratamiento period. The number de exacerbaciones was analysed using a generalised linear model, assuming the Negative Binomial distribution, with time on Tratamiento as an offset variable. The model included adjustments for the effects de smoking status, age, gender, baseline FEV1, number de exacerbaciones reported in the 12 months prior to screening, y region. exacerbaciones that require systemic corticosteroids are likely to be thought de by treating physicians as more severe, therefore reducing these exacerbaciones is an important goal de EPOCtherapy. SERETIDE significantly lowered the rate de exacerbaciones requiring systemic corticosteroids compared with placebo (43% reducción, p < 0.001), SALM (29% reducción, p < 0.001) y FP (13% reducción, p = 0.017). SALM y FP also had significantly lower exacerbation rates than placebo (20%, p < y 35%, p < 0.001, respectively). SERETIDE reduced the rate de exacerbaciones requiring systemic corticosteroids to a greater extent than placebo or either de the component monotherapies. exacerbaciones y hospitalisations predict the risk de dying from EPOCover 5 años.2 References Atkinson AC. Plots, transformations y regression. Clarendon Press Soler-Cataluna JJ, Martinez-Garcia MA, Roman Sanchez P, et al. grave acute exacerbaciones y mortalidadin patients with chronic obstructive pulmonary disease. Thorax 2005;60:925–31. 0.2 Placebo SALM FP SFC Tratamiento Calverley et al. NEJM 2007 *p < vs. placebo; †p < vs. SALM; ‡p = vs. FP
, SALM (29% reducción, p < 0.001) y FP (13% reducción, p = 0.017). SALM y FP also had significantly lower exacerbation rates than placebo (20%, p < y 35%, p < 0.001, respectively). SERETIDE reduced the rate de exacerbaciones requiring systemic corticosteroids to a greater extent than placebo or either de the component monotherapies. exacerbaciones y hospitalisations predict the risk de dying from EPOCover. 5 años.2. References. Atkinson AC. Plots, transformations y regression. Clarendon Press Soler-Cataluna JJ, Martinez-Garcia MA, Roman Sanchez P, et al. grave acute exacerbaciones y mortalidadin patients with chronic obstructive pulmonary disease. Thorax 2005;60:925– Placebo. SALM. FP. SFC. Tratamiento. Calverley et al. NEJM *p < vs. placebo; †p < vs. SALM; ‡p = vs. FP.")
63
Tasa de exacerbaciones requiriendo hospitalización en tres años
Media de exacerbaciones/año 0.25 0.2 0.19 0.17 0.16* 0.16† 0.15 0.1 Exacerbations requiring hospitalisation were classed as severe. The number of exacerbations was analysed using a generalised linear model, assuming the Negative Binomial distribution, with time on treatment as an offset variable. The model included adjustments for the effects of smoking status, age, gender, baseline FEV1, number of exacerbations reported in the 12 months prior to screening, and region. Overall, 26% of patients were hospitalised at least once in the 3 years. The annual admission rate was 17% less in those treated with SFC compared with placebo (p = 0.028). Exacerbations and hospitalisations predict the risk of dying from COPD over 5 years.1 Reducing COPD-related hospitalisations is an important target, as this will improve patient quality of life and consequently reduce the economic burden of COPD. Reference Soler-Cataluna JJ, Martinez-Garcia MA, Roman Sanchez P, et al. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax 2005;60:925–31. 0.05 Placebo SALM FP SFC Tratamiento *p = vs placebo; †p = vs placebo Calverley et al. NEJM 2007
. Exacerbations and hospitalisations predict the risk of dying from COPD over 5 years.1. Reducing COPD-related hospitalisations is an important target, as this will improve patient quality of life and consequently reduce the economic burden of COPD. Reference. Soler-Cataluna JJ, Martinez-Garcia MA, Roman Sanchez P, et al. Severe acute exacerbations and mortality in patients with chronic obstructive pulmonary disease. Thorax 2005;60:925– Placebo. SALM. FP. SFC. Tratamiento. *p = vs placebo; †p = vs placebo. Calverley et al. NEJM")
64
Media de cambio de SGRQ (Unidades)
Resultados - SGRQ 3 Plc 2 1 SAL FP SFC Media de cambio de SGRQ (Unidades) -1 -2 -3 SFC statistically significantly better than placebo at 6-months (p=0.001) Adjusted mean change at 3 years SFC= -1.2, FP = -0.2, Sal = 1, Plac = 2.1 Therefore Steroid containing groups prevented expected decline over 3 years -4 -5 24 48 72 96 120 156 Semanas 1149 1148 1155 1133 Número de Sujetos 854 906 942 941 781 844 848 873 726 807 814 675 723 751 773 635 701 686 731 569 634 629 681
 SFC statistically significantly better than placebo at 6-months (p=0.001) Adjusted mean change at 3 years SFC= -1.2, FP = -0.2, Sal = 1, Plac = 2.1. Therefore Steroid containing groups prevented expected decline over 3 years Semanas Número de Sujetos")
65
FEV1 post-broncodilatador
Cambio medio ajustado del FEV1 (mL) –150 –100 –50 50 100 *† SFC SALM FP * Placebo Descriptive statistics de actual FEV1 y change from baseline FEV1 were reported for baseline y all subsequent visits y at withdrawal. Change from baseline FEV1 was compared between Tratamiento groups using a repeated measures ANCOVA. Tratamiento group was fitted as the explanatory variable, y smoking status, age, gender, baseline FEV1 y region were fitted as covariates. Visit was fitted as a categorical variable y the variance-covariance matrix was assumed to be unstructured. Supportive analyses were also performed at each visit. The ANCOVA fitted change in FEV1 as the response variable, Tratamiento group as the predictor variable y also adjusted for smoking status, age, gender, region y baseline FEV1. The adjusted mean change in post-bronchodilator FEV1 was calculated for each Tratamiento group: –62 mL for placebo –21 mL for SALM –15 mL for FP 29 mL for SERETIDE. Tratamiento differences were calculated y the results are as follows: 92 mL for SERETIDE vs. placebo (p < 0.001) 50 mL for SERETIDE vs. SALM (p < 0.001) 44 mL for SERETIDE vs. FP (p < 0.001) 42 mL for SALM vs. placebo (p < 0.001) 47 mL for FP vs. placebo (p < 0.001) In all cases, SERETIDE significantly increased post-bronchodilator FEV1 compared with the other Tratamiento arms. The true Tratamiento effect may be larger, since there was differential drop out with placebo patients more likely to drop out, therefore this biases against the Tratamiento effect de SERETIDE. 24 48 72 96 120 156 Tiempo (semanas) 1524 1521 1534 1533 1248 1317 1346 1375 Número de sujetos 1128 1218 1230 1281 1049 1127 1157 1180 979 1054 1078 1139 906 1012 1006 1073 819 934 908 975 *p < vs. placebo; †p < vs. SALM y FP Calverley et al. NEJM 2007
 –150. –100. – *† SFC. SALM. FP. * Placebo. Descriptive statistics de actual FEV1 y change from baseline FEV1 were reported for baseline y all subsequent visits y at withdrawal. Change from baseline FEV1 was compared between Tratamiento groups using a repeated measures ANCOVA. Tratamiento group was fitted as the explanatory variable, y smoking status, age, gender, baseline FEV1 y region were fitted as covariates. Visit was fitted as a categorical variable y the variance-covariance matrix was assumed to be unstructured. Supportive analyses were also performed at each visit. The ANCOVA fitted change in FEV1 as the response variable, Tratamiento group as the predictor variable y also adjusted for smoking status, age, gender, region y baseline FEV1. The adjusted mean change in post-bronchodilator FEV1 was calculated for each Tratamiento group: –62 mL for placebo. –21 mL for SALM. –15 mL for FP. 29 mL for SERETIDE. Tratamiento differences were calculated y the results are as follows: 92 mL for SERETIDE vs. placebo (p < 0.001) 50 mL for SERETIDE vs. SALM (p < 0.001) 44 mL for SERETIDE vs. FP (p < 0.001) 42 mL for SALM vs. placebo (p < 0.001) 47 mL for FP vs. placebo (p < 0.001) In all cases, SERETIDE significantly increased post-bronchodilator FEV1 compared with the other Tratamiento arms. The true Tratamiento effect may be larger, since there was differential drop out with placebo patients more likely to drop out, therefore this biases against the Tratamiento effect de SERETIDE Tiempo (semanas) Número de. sujetos *p < vs. placebo; †p < vs. SALM y FP. Calverley et al. NEJM")
66
Resumen de eficacia de los resultados
SFC demostró una tendencia al aumento de la supervivencia (p=0,052) Soporte: Disminuyó significativamente las exacerbaciones comparados con placebo o cualquiera de sus componentes Disminuyó significativamente las hospitalizaciones comparados con placebo Mejoría significativa de la calidad de vida comparado con placebo Mejoría significativa de la función pulmonar (VEF1) comparado con placebo The TORCH trial showed that SFC: Improved survival compared with placebo 1 Reduced the rate of exacerbations compared with components and placebo 2,4 Improved health status compared with placebo and components 3 Significantly improved post-bronchodilator FEV1 compared with placebo and components 2,4 References Calverley PMA, Celli B, Anderson JA et al. The TORCH (Towards a Revolution in COPD Health) study: salmeterol/fluticasone propionate (SFC) improves survival in COPD over three years. Eur Respir J 2006; 28(suppl 50): 34S. Celli B, Calverley PMA, Anderson JA et al. The Towards a Revolution in COPD Health (TORCH) study: fluticasone propionate/salmeterol reduces the rate of exacerbations over 3 years. Chest 2006; 130(4 suppl): 177S. Jones PW, Calverley PMA, Celli B et al. The Towards a Revolution in COPD Health (TORCH) study: fluticasone propionate/salmeterol improves and sustains health status in COPD over 3 years. Chest 2006; 130(4 suppl): 177S-178S Celli B, Calverley PMA, Anderson JA et al. The TORCH (Towards a Revolution in COPD Health) study: salmeterol/fluticasone propionate (SFC) improves health status, reduces exacerbations and improves lung function over three years. Eur Respir J 2006; 28(suppl 50): 34S. Calverley et al ERS 2006 Celli et al Chest 2006 Jones et al Chest 2006 Celli et al ERS 2006
 Soporte: Disminuyó significativamente las exacerbaciones comparados con placebo o cualquiera de sus componentes. Disminuyó significativamente las hospitalizaciones comparados con placebo. Mejoría significativa de la calidad de vida comparado con placebo. Mejoría significativa de la función pulmonar (VEF1) comparado con placebo. The TORCH trial showed that SFC: Improved survival compared with placebo 1. Reduced the rate of exacerbations compared with components and placebo 2,4. Improved health status compared with placebo and components 3. Significantly improved post-bronchodilator FEV1 compared with placebo and components 2,4. References. Calverley PMA, Celli B, Anderson JA et al. The TORCH (Towards a Revolution in COPD Health) study: salmeterol/fluticasone propionate (SFC) improves survival in COPD over three years. Eur Respir J 2006; 28(suppl 50): 34S. Celli B, Calverley PMA, Anderson JA et al. The Towards a Revolution in COPD Health (TORCH) study: fluticasone propionate/salmeterol reduces the rate of exacerbations over 3 years. Chest 2006; 130(4 suppl): 177S. Jones PW, Calverley PMA, Celli B et al. The Towards a Revolution in COPD Health (TORCH) study: fluticasone propionate/salmeterol improves and sustains health status in COPD over 3 years. Chest 2006; 130(4 suppl): 177S-178S. Celli B, Calverley PMA, Anderson JA et al. The TORCH (Towards a Revolution in COPD Health) study: salmeterol/fluticasone propionate (SFC) improves health status, reduces exacerbations and improves lung function over three years. Eur Respir J 2006; 28(suppl 50): 34S. Calverley et al ERS Celli et al Chest Jones et al Chest Celli et al ERS")
67
Manejo escalonado del EPOC

68
Terapia por cada fase de EPOC
I: Leve II: Moderada III: Severa IV: Muy Severa VEF1/CVF < 70% VEF1 < 30% predicho o VEF1 < 50% predicho más insuficiencia respiratoria crónica VEF1/CVF < 70% 30% < VEF1 < 50% predicho VEF1/CVF < 70% 50% < VEF1 < 80% predicho VEF1/CVF < 70% VEF1 > 80% predicho Reducción activa de los factores de riesgo; vacunación contra influenza Agregar broncodilatador de acción corta (PRN) This provides a summary of the recommended treatment at each stage of COPD. Agregar tratamiento regular con uno o más broncodilatadores de acción prolongada (de ser necesario);Agregar rehabilitación Agregar glucocorticosteroides inhalados con exacerbaciones a repetición Agregar oxígeno a largo plazo si hay IR crónica. Considerar tratamiento quirúrgico
 This provides a summary of the recommended treatment at each stage of COPD. Agregar tratamiento regular con uno o más broncodilatadores de acción prolongada (de ser necesario);Agregar rehabilitación. Agregar glucocorticosteroides inhalados con exacerbaciones a repetición. Agregar oxígeno a largo plazo si hay IR crónica. Considerar tratamiento quirúrgico.")
69
Algoritmo Clínico para el tratamiento de la EPOC
Terapia No farmacológica Inhaloterapia Fase Clínica Fase GOLD Cesación de fumado Evitar exposición Síntomas Intermitentes I Broncodilatador de acción corta PRN ( Ipratropio, Salbutamol, o combinación) Vacunación (influenza, neumococo) Síntomas Persistentes‡ II Tiotropio + Salbutamol Salmeterol o Formoterol + Ipratropio, Salbutamol, o combinación Rehabilitación Pulmonar (Prescripción Ejercicio) The proposed 3-step algorithm for mild, moderate, and severe COPD is shown in the slide. Alternatively, the right-hand pathway (arrows) could be selected at this stage. A short-acting bronchodilator can be used as a rescue medication. ICS are indicated if repeated exacerbations require treatment with antibiotics or oral glucocorticosteroids; or if there is favorable response (decreased symptoms, increased lung function, and/or decreased healthcare utilization). Low-dose methylxanthines can be prescribed if the response to inhaled bronchodilator therapy is insufficient. The first column represents 2 alternative pathways for the staged introduction of long-acting bronchodilator therapy with increasing COPD severity. Both pathways lead from as-needed, short-acting bronchodilators alone in mild disease (stage I) to a single long-acting bronchodilator plus an as-needed, short-acting agent in moderate disease (stage II), to the combination of long-acting anticholinergic and LABA therapy with progression of disease severity with or without the addition of ICS for patients with frequent exacerbations or inadequate symptom control despite optimal treatment with bronchodilators alone (stage III/IV). Tiotropio + Salmeterol o Formoterol Salmeterol o Formoterol + Tiotropio Exacerbaciones Frecuentes III Tiotropio + Salmeterol o Formoterol + Corticosteroide Inhalado Insfuficiencia Respiratoria IV Oxígeno Suplementario Cirugía de reducción de volumen Transplante pulmonar Cooper CB et al. BMJ. 2005;330; Tashkin DP, Cooper CB. The role of long-acting bronchodilators in the management of stable COPD. Chest. 2004;125: Global Initiative for Chronic Obstructive Lung Disease: Executive Summary Updated Global Strategies for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. Available at: Accessed February 21, 2005.
 Vacunación (influenza, neumococo) Síntomas. Persistentes‡ II. Tiotropio + Salbutamol. Salmeterol o Formoterol + Ipratropio, Salbutamol, o combinación. Rehabilitación Pulmonar (Prescripción Ejercicio) The proposed 3-step algorithm for mild, moderate, and severe COPD is shown in the slide. Alternatively, the right-hand pathway (arrows) could be selected at this stage. A short-acting bronchodilator can be used as a rescue medication. ICS are indicated if repeated exacerbations require treatment with antibiotics or oral glucocorticosteroids; or if there is favorable response (decreased symptoms, increased lung function, and/or decreased healthcare utilization). Low-dose methylxanthines can be prescribed if the response to inhaled bronchodilator therapy is insufficient. The first column represents 2 alternative pathways for the staged introduction of long-acting bronchodilator therapy with increasing COPD severity. Both pathways lead from as-needed, short-acting bronchodilators alone in mild disease (stage I) to a single long-acting bronchodilator plus an as-needed, short-acting agent in moderate disease (stage II), to the combination of long-acting anticholinergic and LABA therapy with progression of disease severity with or without the addition of ICS for patients with frequent exacerbations or inadequate symptom control despite optimal treatment with bronchodilators alone (stage III/IV). Tiotropio + Salmeterol o Formoterol. Salmeterol o Formoterol + Tiotropio. Exacerbaciones. Frecuentes. III. Tiotropio + Salmeterol o Formoterol + Corticosteroide Inhalado. Insfuficiencia. Respiratoria. IV. Oxígeno Suplementario. Cirugía de reducción de volumen. Transplante pulmonar. Cooper CB et al. BMJ. 2005;330; Tashkin DP, Cooper CB. The role of long-acting bronchodilators in the management of stable COPD. Chest. 2004;125: Global Initiative for Chronic Obstructive Lung Disease: Executive Summary Updated Global Strategies for the Diagnosis, Management, and Prevention of Chronic Obstructive Pulmonary Disease. Available at: Accessed February 21,")
Presentaciones similares


 Concepción Díaz Sánchez H. Cabueñes.Gijón.>")

>")











 2000-2003.>")



