Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Protocolos de Transfusión Masiva Conceptos y controversias
Preparada por: Mónica Isabel Vásquez Arenas Ginecobstetra Nacer, Salud Sexual y Reproductiva Facultad de Medicina Departamento de Obstetricia y Ginecología Universidad de Antioquia Medellin- Colombia

2
Agregar título general

3
Hemorragia masiva Trauma: Conflictos militares y civiles
Eventos obstétricos Cirugía mayor electiva Enfermedad general

4
Pérdidas sanguíneas y reposiciones
Am Coll Surg, ATLS. 1997

5
Hemorragia masiva Pérdida de toda la volemia en 24 horas
Pérdida continua de sangre 150mL/min mL/Kg/min por 20 minutos Pérdida rápida de sangre que produce descompensación y falla circulatoria a pesar de soporte adecuado Erber WN. Transfusion and Apheresis Science.2002; 27: 83–92. Harvey MP y Col. The Medical journal of Australia ; 163: 356–59

6
Transfusión masiva Transfusión de 10 o más unidades de glóbulos rojos en 24 horas 5 U o más en las primeras 4 horas 50 U o más en 48 horas Repine, T. The Use of Fresh Whole Blood in Massive Transfusion. J Trauma. 2006;60:S59 –S69

7
Transfusión masiva Incidencia en trauma: 1-3%
15% Traumas severos (conflictos bélicos) Mortalidad: 20-50% Borgman, M. The Ratio of Blood Products Transfused Affects Mortality in Patients Receiving Massive Transfusions at a Combat Support Hospital. J Trauma. 2007;63:805–813.
 Mortalidad: 20-50% Borgman, M. The Ratio of Blood Products Transfused Affects Mortality in Patients Receiving Massive Transfusions at a Combat Support Hospital. J Trauma. 2007;63:805–813.")
8
Mattox, Kenneth L. et al, Trauma. 6th Edition. McGraw-Hill. 2008
Choque hemorrágico Coagulopatía Acidosis Hipotermia Tríada de la muerte Mattox, Kenneth L. et al, Trauma. 6th Edition. McGraw-Hill. 2008

9
Coagulopatía Presente al ingreso en la mayoría de los casos
Pérdida de factores de coagulación y plaquetas Dilución por infusión de cristaloides Inactivación de factores de coagulación por acidosis Fibrinolisis aumentada Perkins, J. Massive transfusion and nonsurgical hemostatic agents. Crit Care Med 2008; 36:[Suppl.]:S325-S339

10
Hipotermia Hipoperfusión
Pérdidas por conducción, convección, evaporación Termoregulación alterada Disfunción plaquetaria: Reducción activación Factor Von Willlebrand Administración de fluidos y hemocomponentes Perkins, J. Massive transfusion and nonsurgical hemostatic agents. Crit Care Med 2008; 36:[Suppl.]:S325-S339

11
Acidosis Resultante de la producción de lactato por metabolismo anaeróbico en tejidos hipoperfundidos Ph GRE: 7.1 al momento de la recolección Reducción de actividad de factores de la coagulación: Factor VIIa (hasta el 90%) Inhibición de la generación de trombina Activación de anticoagulantes naturales Perkins, J. Massive transfusion and nonsurgical hemostatic agents. Crit Care Med 2008; 36:[Suppl.]:S325-S339
 Inhibición de la generación de trombina. Activación de anticoagulantes naturales. Perkins, J. Massive transfusion and nonsurgical hemostatic agents. Crit Care Med 2008; 36:[Suppl.]:S325-S339.")
12
Metas en el tratamiento
Mantener la perfusión tisular y oxigenación mediante la restauración del volumen y la masa transportadora Controlar el sangrado Uso correcto de hemocomponentes para corrección de coagulopatía Resucitación de control de daño D. Stainsby et al. Guidelines on the management of massive blood loss. British Journal of Haematology, 135, 634–641

13
Protocolo de transfusión masiva
Identificación, soporte y tratamiento del sangrado que amenaza la vida Tratamiento de complicaciones clínicas y bioquímicas Prevención de la coagulopatía que ha demostrado ser superior a su tratamiento No hay un protocolo único Protocolos propuestos por centros de trauma y organizaciones académicas Mitra, B et al. Massive blood transfusion and trauma resuscitation. Injury, Int. J. Care Injured (2007) 38, 1023—1029
 38, 1023—1029.")
14
Protocolo de transfusión masiva
Debe ser conocido, divulgado y probado por médicos, enfermería y personal del banco de sangre Debe ser avalado por el Comité de Transfusiones Definir el papel de cada una de las personas que intervienen Definir quién lo activa, cómo se hace la solicitud de los hemocoponentes Los canales de comunicación con el Banco de Sangre Establecer qué situaciones clínicas lo activan Hemocomponentes requeridos

15
Protocolo de transfusión masiva
The Denver General Health Center Toma de muestra para pruebas cruazadas Procesan inicialmente 10 U GRE Transfusión inicial de 6 U: Inicia PF 2 U Liberación de 4 U GRE por hora grupo compatibles Una vez se ha transfundido el equivalente a una volemia no realizan mas pruebas cruzadas No información sobre plaquetas Universidad de Texas Transfusión inicial de 4 unidades de GRE O- Envío de muestra al banco de sangre Retorno con otras 6 unidades O- y 4 U PF y 1 U aféresis plaquetas, la cual se transfunde cada 10 U GRE Medición de fibrinógeno después de 18 U GRE Metas: Normalizar TP, Plaquetas > , Fibrinógeno >1g/L Universidad de Maryland Objetivo: Minimizar la coagulopatía Hay 12 U GRE grupo O en el servicio de urgencias (2 u GRE O-) Se transfunde 1:1 GRE:PF y una unidad de aféresis de plaquetas por cada 10 U GRE Reanimación guiada por anestesiólogo The protocol of the University of Maryland R Adams Cowley Shock Trauma Center (STC) in Baltimore is designed to minimize the coagulopathy of trauma.12 Red blood cells, plasma, and platelets are used early in the resuscitation of massively bleeding patients, soon after patient arrival at the trauma resuscitation unit (TRU). Infusion of crystalloid has often been started in the field and continues in the TRU with Plasmalyte-A, an isotonic crystalloid similar to Ringer’s solution. Blood is sent immediately to the blood bank for typing and cross-matching. Twelve units of un-cross-matched group O RBC are kept in the TRU blood refrigerator and are available for immediate use. Two of the units are O Rh Neg, and are usually reserved for women of child-bearing age. This un-cross-matched blood is used for immediately lifethreatening hemorrhage until type-compatible or fully crossmatched blood is available. Type-compatible RBC and plasma are generally available within 30–45 minutes. During ongoing massive transfusion, blood is typically ordered in amounts of 10 units of RBC, 10 units of plasma, and an apheresis platelet pack equivalent to 6–11 units. Because RBC are issued on the basis of a computer crossmatch (are type-compatible) and type compatible thawed plasma is maintained in the blood bank, the delay between order and issue is minimal once a blood type has been established. Resuscitation managers, usually anesthesiologists, give the RBC and plasma alternately and the platelets at the end of a 10 RBC unit course. This protocol supports a Debra L. Malone et al. Massive Transfusion Practices Around the Globe and aSuggestion for a Common Massive Transfusion Protocol. J Trauma. 2006;60:S91–S96
 Se transfunde 1:1 GRE:PF y una unidad de aféresis de plaquetas por cada 10 U GRE. Reanimación guiada por anestesiólogo. The protocol of the University of Maryland R Adams. Cowley Shock Trauma Center (STC) in Baltimore is designed. to minimize the coagulopathy of trauma.12 Red blood. cells, plasma, and platelets are used early in the resuscitation. of massively bleeding patients, soon after patient arrival at. the trauma resuscitation unit (TRU). Infusion of crystalloid. has often been started in the field and continues in the TRU. with Plasmalyte-A, an isotonic crystalloid similar to Ringer’s. solution. Blood is sent immediately to the blood bank for. typing and cross-matching. Twelve units of un-cross-matched. group O RBC are kept in the TRU blood refrigerator and are. available for immediate use. Two of the units are O Rh Neg, and are usually reserved for women of child-bearing age. This un-cross-matched blood is used for immediately lifethreatening. hemorrhage until type-compatible or fully crossmatched. blood is available. Type-compatible RBC and. plasma are generally available within 30–45 minutes. During ongoing massive transfusion, blood is typically. ordered in amounts of 10 units of RBC, 10 units of plasma, and an apheresis platelet pack equivalent to 6–11 units. Because RBC are issued on the basis of a computer crossmatch. (are type-compatible) and type compatible thawed. plasma is maintained in the blood bank, the delay between. order and issue is minimal once a blood type has been. established. Resuscitation managers, usually anesthesiologists, give the RBC and plasma alternately and the platelets at. the end of a 10 RBC unit course. This protocol supports a. Debra L. Malone et al. Massive Transfusion Practices Around the Globe and aSuggestion for a Common Massive Transfusion Protocol. J Trauma. 2006;60:S91–S96.")
16
Protocolo de transfusión masiva
Ottawa Hospital, University of Ottawa, Canada Bormanis, J. Development of a massive transfusion protocol. Transfusion and Apheresis Science 38 (2008) 57–63
 57–63.")
17
Protocolo de transfusión masiva
Universidad de Nueva Gales del Sur (Sydney) Modelo de rescate Identificar y controlar la fuente de sangrado Transfundir de acuerdo con parámetros de laboratorio: 4 U PF si TP o TTP >1.5 veces el control 10 U crioprecipitado si fibrinógeno <1 g/L 4 U de plaquetas si recuento <75000 10 U GRE Centre Hospitalier Intercommunal (Poissy, Francia) Intenta prevenir coagulopatía No dependiente de parámetros de laboratorio 8 U GRE O- o compatibles de grupo sin pruebas cruzadas PF:GRE : 6-8 6-8: 8 si el sangrado es evidente y no controlado Plaquetas: 1U : 7 Kg Factor VII a Hospital Universitario de Helsinki (Finlandia) Transfusión inicial de 10 U GRE Niveles de Hemoglobina >10 mg/dl Plaquetas >50.000 incorporates treatment intended to prevent coagulopathy and acidosis and includes specific guidelines regarding blood product transfusion.5 This protocol specifies that 8 units of RBC be issued initially, usually group O Rh negative or type-compatible without further testing unless the patient has known antibodies. Serial laboratory testing is performed. Thawed FFP is issued in ratios of 4 FFP/6–8 RBC. Platelets are given at a dose of one unit per 7 kg with a goal of achieving platelet “counts” of 50–70 109/L. With evident bleeding, the FFP/RBC ratio is increased to 6–8 units/8 units of RBC, and cryoprecipitate and rVIIa (60–90 g/kg) are considered as well. A similar protocol was designed by the Massive Transfusion Task Group at the Helsinki University Hospital in Finland.15 Minor differences include the initial and subsequent issue of 10 units of RBC at a time and the issue of RBC to maintain a goal hemoglobin concentration of 10 g/dL and platelets at a concentration of /L Debra L. Malone et al. Massive Transfusion Practices Around the Globe and aSuggestion for a Common Massive Transfusion Protocol. J Trauma. 2006;60:S91–S96
 Modelo de rescate. Identificar y controlar la fuente de sangrado. Transfundir de acuerdo con parámetros de laboratorio: 4 U PF si TP o TTP >1.5 veces el control. 10 U crioprecipitado si fibrinógeno <1 g/L. 4 U de plaquetas si recuento < U GRE. Centre Hospitalier Intercommunal (Poissy, Francia) Intenta prevenir coagulopatía. No dependiente de parámetros de laboratorio. 8 U GRE O- o compatibles de grupo sin pruebas cruzadas. PF:GRE 4 : : 8 si el sangrado es evidente y no controlado. Plaquetas: 1U : 7 Kg. Factor VII a. Hospital Universitario de Helsinki (Finlandia) Transfusión inicial de 10 U GRE. Niveles de Hemoglobina >10 mg/dl. Plaquetas > incorporates treatment intended. to prevent coagulopathy and acidosis and includes specific. guidelines regarding blood product transfusion.5 This. protocol specifies that 8 units of RBC be issued initially, usually. group O Rh negative or type-compatible without further testing. unless the patient has known antibodies. Serial laboratory. testing is performed. Thawed FFP is issued in ratios of 4. FFP/6–8 RBC. Platelets are given at a dose of one unit per 7. kg with a goal of achieving platelet counts of 50– /L. With evident bleeding, the FFP/RBC ratio is increased. to 6–8 units/8 units of RBC, and cryoprecipitate and rVIIa. (60–90 g/kg) are considered as well. A similar protocol was designed by the Massive Transfusion. Task Group at the Helsinki University Hospital in. Finland.15 Minor differences include the initial and subsequent. issue of 10 units of RBC at a time and the issue of RBC. to maintain a goal hemoglobin concentration of 10 g/dL and. platelets at a concentration of /L. Debra L. Malone et al. Massive Transfusion Practices Around the Globe and aSuggestion for a Common Massive Transfusion Protocol. J Trauma. 2006;60:S91–S96.")
18
Preguntas Criterios precisos para activar el protocolo
Hay parámetros de predicción? Transfusión masiva guiada por parámetros de laboratorio? Cuál es la relación adecuada GRE:PFC para evitar y corregir exitosamente la coagulopatía? Por qué hemocomponentes aislados y no sangre total? Diferencias en la transfusión masiva del paciente traumatizado y de la paciente obstétrica

19
Parámetros de predicción
Edad Género Mecanismo de trauma INR TP TTP Hb Recuento de plaquetas Índices de severidad Schreiber, M. Early Predictors of Massive Transfusion in Combat Casualties. J Am Coll Surg 2007;205:541–545

20
2 Hospitales de trauma en Irak 558 pacientes incluidos
Estudio cohorte 2 Hospitales de trauma en Irak 558 pacientes incluidos 247 pacientes transfusión masiva 311 no la requirieron J Am Coll Surg 2007;205:541–545

21
Paraclínicos Inicio de transfusión masiva “a ciegas” Consumo de Tiempo
Resultados poco precisos Estáticos Pueden solicitarse para controlar la reposición de hemocomponentes c/4-6 U GRE Tromboelastografía CBC platelets, INR, PTT, TT and repeat after 4- 6 units Why these tests? They should be always available 24/7. Some hospitals have point of care coagulation testing, the INR being most common and more consistently useful than the PTT. The INR is a surrogate marker for the degree of dilutionalcoagulopathy. Once the INR is >1.5 then the level of clotting factors is approaching 20%. In patients with exsanguinating injuries, urgent transfusion of blood products is needed to restore oxygen transport, perfusion and coagulation. In contrast to the clinical situation of massive blood loss during elective operations, massive transfusion in exsanguinating trauma is performed ‘blindly’ i.e. not guided by laboratory tests. During these hectic circumstances, massive transfusion protocols are vital to assure proper treatment. If not, coagulation factors and plateletswill not be administered timely and/or in enough quantities and coagulopathy is further promoted.42,47,68 Blood component therapy itself, as well as sound logistic procedures regarding automatic delivery of products in packages (containing Packed Red Blood Cells (PRBC), Fresh Frozen Plasma (FFP) and platelets) to the shock room or operating theatre, has to be well defined in those protocols.93 Massive transfusion protocols exist at a relatively small number of large and well-organised trauma centres. Standard coagulation tests in exsanguinating trauma, such as PTT, PT and platelets may not reflect the actual coagulation status in the patient. The tests are time consuming and do not test coagulation function. However, the role of thromboelastography TEG (or thromboelastometry TEM) as a point-of-care test for the coagulation status in massive blood loss is emerging, providing information about actual clot formation and stability, shortly (10 min) after the blood sample is taken.39,65 Thus, therapy can be directed by the test results allowing for administration of specific coagulation factors, e.g. fibrinogen and/or PCC that may be depleted despite administration with FFP during massive transfusion of blood components L.M.G. Geeraedts et al.Exsanguination in trauma: A review of diagnostics and treatment options. Injury, Int. J. Care Injured 40 (2009) 11–20
, Fresh Frozen Plasma (FFP) and platelets) to the shock room or operating theatre, has to be well defined in. those protocols.93 Massive transfusion protocols exist at a. relatively small number of large and well-organised trauma. centres. Standard coagulation. tests in exsanguinating trauma, such as PTT, PT and platelets. may not reflect the actual coagulation status in the patient. The. tests are time consuming and do not test coagulation function. However, the role of thromboelastography TEG (or thromboelastometry. TEM) as a point-of-care test for the coagulation status. in massive blood loss is emerging, providing information about. actual clot formation and stability, shortly (10 min) after the. blood sample is taken.39,65 Thus, therapy can be directed by the. test results allowing for administration of specific coagulation. factors, e.g. fibrinogen and/or PCC that may be depleted despite. administration with FFP during massive transfusion of blood. components. L.M.G. Geeraedts et al.Exsanguination in trauma: A review of diagnostics and treatment options. Injury, Int. J. Care Injured 40 (2009) 11–20.")
22
Tromboelastografía Medición in vitro de la función hemostática global de una muestra de sangre Transmisión de oscilaciones producidas por la sangre durante la coagulación Oscilación---Señal eléctrica---Amplificación---Reporte gráfico Mide la velocidad de formación y estabilidad del coágulo y lo expresa en una gráfica Maia, P y col. Tromboelastógrafo en Cirugía Cardíaca: Estado Actual. Rev Bras Anestesiol. 2006; 56: 1:

23
Tromboelastograma Maia, P y col. Tromboelastógrafo en Cirugía Cardíaca: Estado Actual. Rev Bras Anestesiol. 2006; 56: 1:

24
Relación GRE : PF Objeto de debate
Composición del paquete de transfusión debe ser comparable a la composición de la sangre total Múltiples esquemas 1:8, 1:4, 1:1 Últimamente se ha planteado relación 1:1 con buenos resultados en cuanto a mortalidad, FOM y estancia hospitalaria The fixed ratio between the amounts of packed red blood cells, FFP and platelets within a transfusion package is subject to debate. Nevertheless, the composition of a transfusion package must be comparable to the composition of whole blood regarding total volume and the total amount of coagulation factors and platelets. Malone et al. have suggested that the use of a simple ratio of 1:1:1 for PRBC:FFP:platelets may result in the administration of higher plasma and platelets doses and may improve outcome. Numerous strategies in regards to the use of fresh frozen plasma (FFP) in critically injured patients exist, which include 1 unit of FFP for every 4 to 10 U of PRBCs transfused and a minimum of 2 U of FFP if the PT is greater than or equal to 1.8 times contro Most recently, Borgman et al7 reported a retrospective study of patients with combat-related trauma who required massive transfusion. A high plasma to RBC ratio (1:1.4 U) was independently associated with improved survival to hospital discharge, primarily by decreasing death from hemorrhage. The adaptation of an early and aggressive transfusion practice that mandates a 1:1 ratio of FFP to PRBCs would clearly impact blood bank resources across the country L.M.G. Geeraedts et al.Exsanguination in trauma: A review of diagnostics and treatment options. Injury, Int. J. Care Injured 40 (2009) 11–20
 in critically injured patients exist, which include 1 unit. of FFP for every 4 to 10 U of PRBCs transfused and a. minimum of 2 U of FFP if the PT is greater than or equal to. 1.8 times contro. Most recently, Borgman et al7 reported a retrospective. study of patients with combat-related trauma who. required massive transfusion. A high plasma to RBC ratio. (1:1.4 U) was independently associated with improved survival. to hospital discharge, primarily by decreasing death. from hemorrhage. The adaptation of an early and aggressive transfusion. practice that mandates a 1:1 ratio of FFP to PRBCs would. clearly impact blood bank resources across the country. L.M.G. Geeraedts et al.Exsanguination in trauma: A review of diagnostics and treatment options. Injury, Int. J. Care Injured 40 (2009) 11–20.")
25
The American Journal of Surgery (2008) 196, 948–960
Estudio de cohorte prospectivo 383 pacientes hemorragia masiva 16 meses hasta feb/06 Pacientes pertenecientes al grupo 1 (muerte temprana) GRE: 26.4 PF: 6.5 12% no recibieron The American Journal of Surgery (2008) 196, 948–960
 GRE: PF: % no recibieron. The American Journal of Surgery (2008) 196, 948–960.")
26
Estudio de cohorte prospectivo
R Adams Cowley Shock Trauma Center (Maryland) Julio Noviembre 2006 Trauma en civiles No se encontró efecto protector en la transfusión de hemocomponentes PF:GRE 1:1 R Adams Cowley Shock Trauma Center, the Primary Adult Resource Center (PARC) for the State of Maryland This prospective cohort study (July 2004–November 2006 Again, the presence of a 1:1 ratio was not associated with any protective effect against mortality when controlling for other significant predictors of death Ann Surg 2008;248: 578–584
 Julio Noviembre Trauma en civiles. No se encontró efecto protector en la transfusión de hemocomponentes PF:GRE 1:1. R Adams Cowley Shock Trauma Center, the Primary Adult. Resource Center (PARC) for the State of Maryland. This prospective cohort study. (July 2004–November Again, the presence of a 1:1 ratio was not. associated with any protective effect against mortality when. controlling for other significant predictors of death. Ann Surg 2008;248: 578–584.")
27
Estudio retrospectivo
Pacientes admitidos en hospital de soporte de combate en Irak Noviembre 2003-septiembre 2005 5293 pacientes admitidos 246 (4.6%) recibió transfusión masiva Relación plasma: GRE we performed a retrospective analysis of data for trauma patients admitted to a combat support hospital (CSH) in Iraq between November 2003 and September 2005. 5,293 patients were admitted to the CSH in Baghdad. The JTTR identified 246 (4.6%) patients who received massive transfusion J Trauma. 2007;63:805–813
 recibió transfusión masiva. Relación plasma: GRE. we performed a retrospective. analysis of data for trauma patients admitted to a combat. support hospital (CSH) in Iraq between November 2003 and. September ,293. patients were admitted to the CSH in Baghdad. The JTTR. identified 246 (4.6%) patients who received massive transfusion. J Trauma. 2007;63:805–813.")
28
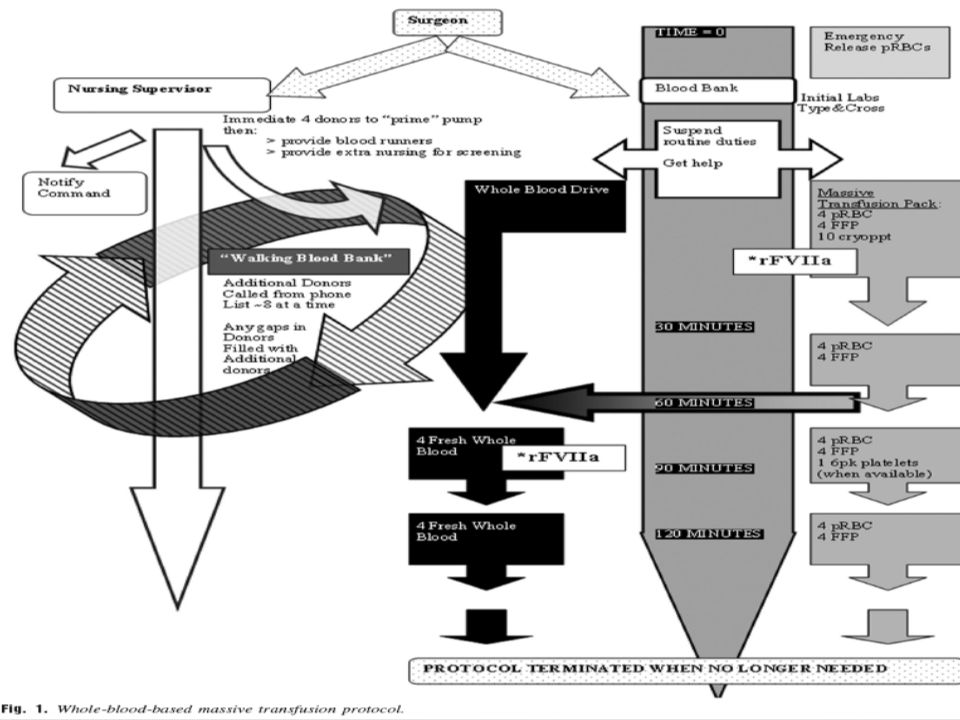
Uso de sangre total La sangre puede ser usada más eficientemente si se separan sus componentes En el ámbito militar se ha continuado con su uso por la imposibilidad para conservar plaquetas y PFC El almacenamiento de sangre total puede incrementar la capacidad de respuesta de un banco de sangre con alto flujo para casos de multitud de lesionados Under these circumstances, whole blood use can increase the blood bank’s ability to deliver lifesaving transfusions in a timely manner Repine, T. The Use of Fresh Whole Blood in Massive Transfusion. J Trauma. 2006;60:S59 –S69

29
Uso de sangre total Repine, T. The Use of Fresh Whole Blood in Massive Transfusion. J Trauma. 2006;60:S59 –S69

30
Uso de sangre total Repine, T. The Use of Fresh Whole Blood in Massive Transfusion. J Trauma. 2006;60:S59 –S69

32
Sangrado masivo en la paciente obstétrica
Aumento de la volemia 50% entre las semanas 32-34 No aumento de la masa eritrocitaria (anemia fisiológica) Flujo sanguíne del útero: cc /min Pérdida sanguínea normal parto: 500 cc Cesárea: 1000 cc B Lynch, C. A Textbook of POSTPARTUM HEMORRHAGE. Sapiens Publishing Pag 10-15
 Flujo sanguíne del útero: cc /min. Pérdida sanguínea normal parto: 500 cc. Cesárea: 1000 cc. B Lynch, C. A Textbook of POSTPARTUM HEMORRHAGE. Sapiens Publishing Pag")
33
Sangrado masivo en la paciente obstétrica
Tono Hemorragia obstétrica Trombina Trauma Tejido B Lynch, C. A Textbook of POSTPARTUM HEMORRHAGE. Sapiens Publishing Pag 10-15

34
Protocolo de transfusión masiva
Burtelow, M. How we treat: management of life-threatening primary postpartum hemorrhage with a standardized massive transfusion protocol. TRANSFUSION Volume 47, September 2007

35
Complicaciones de la transfusión masiva
Las esperadas en cualquier transfusión TRALI FOM Hipercalemia: 12 mEq a los 7 días de recolectados 32 mEq a los 14 días Arritmias ventriculares Perkins, J. Massive transfusion and nonsurgical hemostatic agents. Crit Care Med 2008; 36:[Suppl.]:S325-S339

36
Complicaciones de la transfusión masiva
Hipocalcemia: El citrato se liga al calcio ionizado Mayor con plaquetas y PFC Metabolismo hepático Disminución de la deformabilidad eritrocitaria Hipotermia Acidosis Alcalosis metabólica: Generación de bicarbonato a partir del citrato Perkins, J. Massive transfusion and nonsurgical hemostatic agents. Crit Care Med 2008; 36:[Suppl.]:S325-S339

37
Conclusiones La transfusión masiva debe realizarse dentro de protocolos previamente establecidos La activación del protocolo de transfusión masiva no debe estar sujeta a resultados de paraclínicos El pronóstico del paciente con coagulopatía mejora si ésta antes de prevenirse se trata Se ha encontrado un beneficio significativo en la administración agresiva de PFC en relación 1:1 con los GRE en cuanto a supervivencia y estancia hospitalaria

38
Conclusiones La transfusión de sangre total es una buena estrategia para centros de trauma con alto flujo de pacientes La sangre total si se administra dentro de la primeras 12 horas de recolectada es una alternativa más fisiológica y con menos riesgos de transmisión de infección La paciente obstétrica tiene ciertas particularidades que la hacen diferente del paciente de trauma El riesgo permanente de una hemorragia de origen obstétrico obliga a éstos servicios a desarrollar protocolos de transfusión masiva

39
Gracias www.nacer.udea.edu.co

Presentaciones similares



 es una alteración fisiopatólogica sistémica, trombohemorrágica, que se presenta en algunas situaciones.>")















>")