Descargar la presentación
La descarga está en progreso. Por favor, espere

1
EVALUACIÓN Y REGISTRO DE MEDICAMENTOS EN LA UNIÓN EUROPEA
Cristina Avendaño Solà Hospital Universitario Puerta de Hierro

2
Ideas fundamentales Las Agencias de Medicamentos NO tienen en cuenta el valor terapéutico añadido de los nuevos medicamentos antes de su aprobación Los criterios de aprobación son lo mismos en toda la UE y distintos en EEUU Las aprobaciones (FT) reflejan la evidencia generada por las Compañías encaminada a obtener el “aprobado” Tras la aprobación, se realiza la selección
 reflejan la evidencia generada por las Compañías encaminada a obtener el aprobado Tras la aprobación, se realiza la selección.")
3
¿QUIEN AUTORIZA LOS MEDICAMENTOS EN ESPAÑA?
Si no quieren que lo prescriba... ¿Por qué lo autorizan? AEM/EMEA Entidad financiadora: Listas negativas Indicadores prescripción Selección medicamentos Visado inspección MÉDICO PRESCRIPTOR Industria Farmacéutica Congresos Publicaciones Guías terapéuticas Pacientes

4
¿QUIEN AUTORIZA LOS MEDICAMENTOS EN ESPAÑA?
FINANCIACION POR SNS APROBACION calidad, eficacia y seguridad Dirección General Farmacia y PS COMUNIDADES AUTONOMAS

5
Ensayos clínicos APROBACION NUEVOS MEDICAMENTOS
COMPAÑIAS FARMACEUTICAS Ensayos clínicos Demostración de calidad, eficacia y seguridad APROBACION NUEVOS MEDICAMENTOS Médicos clínicos Investigadores Sociedades científicas Sistemas Nacionales de Salud ... Puesto en terapéutica Guías de práctica clínica Decisiones de reembolso Farmacoeconomía

6
THE EUROPEAN MEDICINES AGENCY
Created in July 1993 Seat : London, October 1993 European Agency operational in 1995 2004: Changes to correct procedures and to adapt to EU enlargement

7
Creation in 1995 as unification of the National Agencies of the EU
Headquarters in London 300 employees 3.000 experts national agencies Creation in 1938 40 buildings (FDA Headquarters) 9.000 employees (60% budget) Internal assessors
 employees (60% budget) Internal assessors.")
8
EVALUACION DE MEDICAMENTOS
AGENCIA EUROPEA DE EVALUACION DE MEDICAMENTOS • Consejo de Administraci ó n • Director Ejecutivo • Comit é s Cient í ficos AGENCIAS NACIONALES CHMP, CVMP, COMP • Secretariado cient í fico • Red de expertos

9
UN ÚNICO SISTEMA DE REGISTRO, VARIOS PROCEDIMIENTOS
Procedimiento Centralizado Reconocimiento Mutuo Procedimiento Nacional Mismos criterios en todos los procedimientos !

13
Autoridades Sanitarias Nacionales/locales
Regulación de medicamentos en la UE EMEA Agencias Nacionales de Medicamentos Autoridades Sanitarias Nacionales/locales Utilización por los SNS Departamentos de Salud en cada Estado Miembro Autorización de medicamentos DG Enterprise en EU (en lugar de DG Health and Consumer Protection): importancia de la competitividad de la Industria Europea Tasas de las Compañías farmacéuticas
: importancia de la competitividad de la Industria Europea. Tasas de las Compañías farmacéuticas.")
15
Regulación de medicamentos en la UE
EMEA Agencias Nacionales de Medicamentos Autoridades Sanitarias Nacionales/locales Precio Reembolso Guías de utilización Valor terapéutico añadido Coste-efectividad Autorización y vigilancia nuevos medicamentos en la UE Demostración de calidad, eficacia y seguridad. Beneficio-riesgo considerando las alternativas existentes (UE USA).
.")
16
Regulación de medicamentos en la UE
EMEA Agencias Nacionales de Medicamentos Autoridades Sanitarias Nacionales/locales Precio Reembolso Guías de utilización Autorización y vigilancia nuevos medicamentos en la UE IDENTICA EN TODOS LOS ESTADOS MIEMBROS DIFERENCIAS ENTRE ESTADOS MIEMBROS

17
DOCUMENTO MARCO DEL GRUPO DE TRABAJO
PARA LA RACIONALIZACIÓN Y LA FINANCIACIÓN DEL GASTO SANITARIO. Barcelona 3 de febrero de 2005 En materia de consumo de medicamentos se proponen las siguientes medidas: PRIMERA : Hacer efectiva la separación entre el registro y la financiación pública de los medicamentos, prevista en la Ley del medicamento. Seleccionar los medicamentos financiados por el SNS sobre la base de los problemas atendidos y de las pruebas disponibles sobre coste-efectividad comparada. (Lista de medicamentos de elección del SNS).
.")
18
El caso de los antipsicóticos
AEMPS 09/03/05 En ancianos tratados por trastornos psicóticos asociados a demencia se observa incremento del riesgo de muerte y ACV con olanzapina En la misma población, incremento del riesgo de ACV con risperidona. Datos limitados para otros antipsicóticos. AEMPS 10/05/05 Recomendaciones para el tratamiento con risperidona en ancianos con demencia

19
El caso de los antipsicóticos
DGFPS 12/01/05: Establecimiento de visado para los mayores de 75 años en todas las indicaciones y para todos los antipsicóticos atípicos. ¿separación clara entre problema de seguridad y problema de financiación/ uso de los medicamentos?

20
Safety Biotechnology Working Party Working Party CHMP Working Parties
Pharmacovigilance Working Party Quality Working Party Blood and Plasma Working Party Efficacy Working Party Specific ad-hoc working groups To elaborate guidelines about Clinical development of medicinal products Guidance to Industry Harmonisation between MS !

22
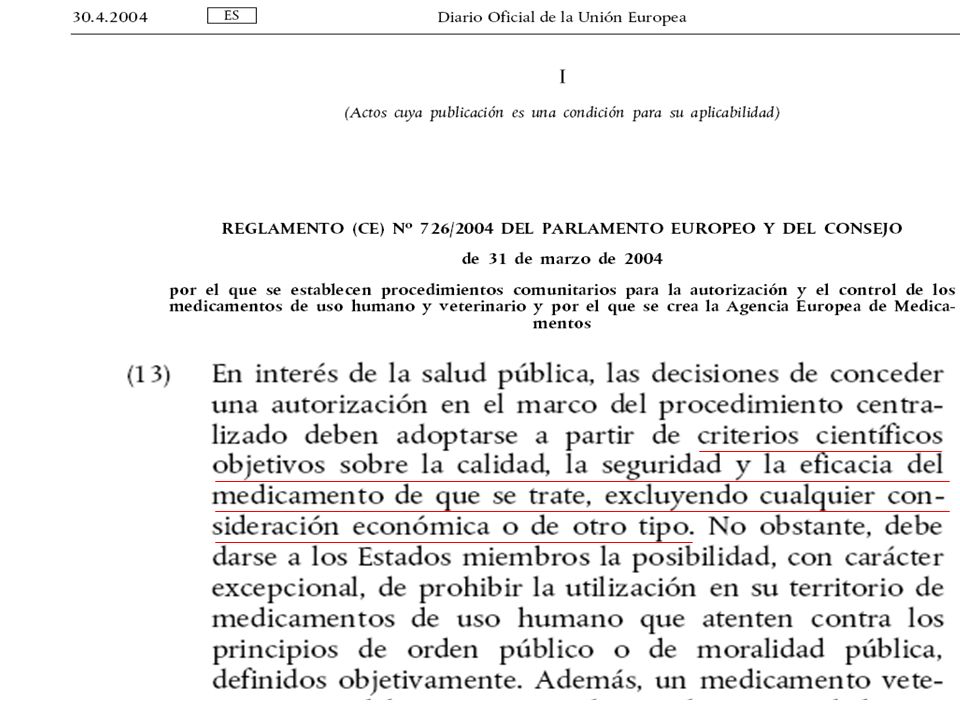
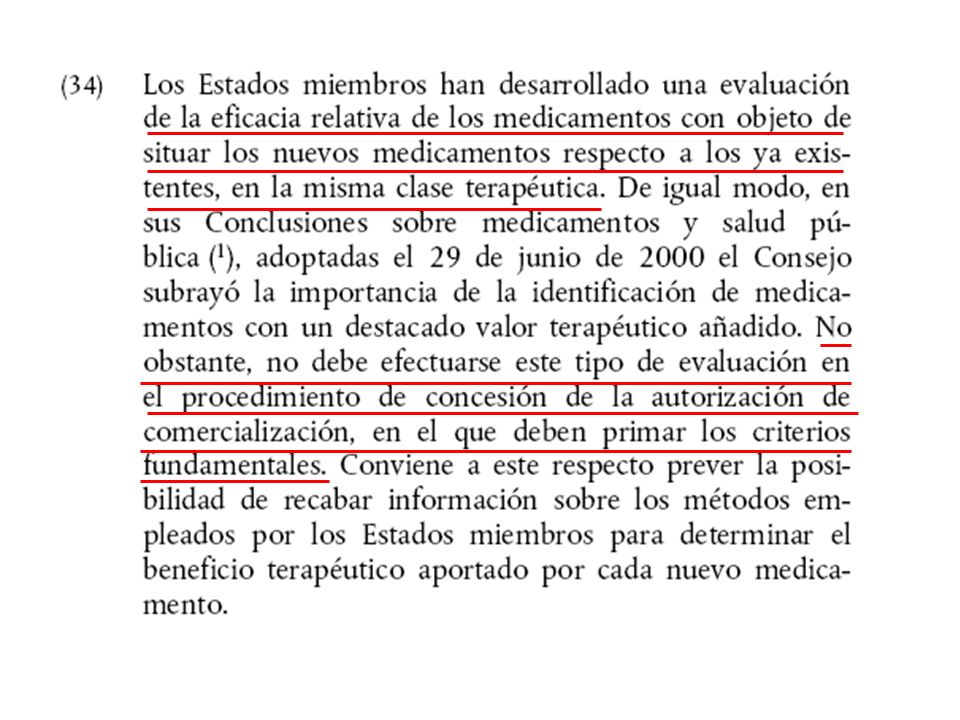
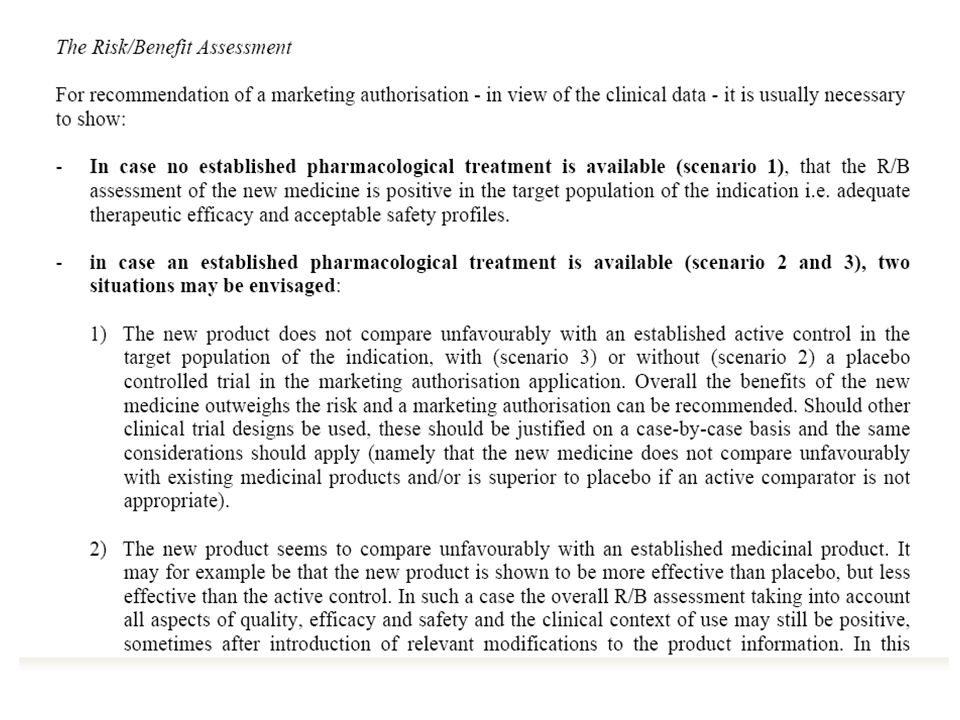
Criterios de la UE para la autorización de medicamentos : Evaluación clínica del beneficio-riesgo - Papel de los estudios frente a comparador activo. EMEA/119319/04.Octubre 2004 The assessment of risk/benefit of a new product being informed by an active comparator is considered part of the assessment of efficacy and safety and fundamentally different from the concepts of “placing the product in the therapeutic strategy” or“relative effectiveness” which implies two components: the added therapeutic value and cost effectiveness . These two components go beyond the standards of marketing authorisation (quality,safety, efficacy).
.")
24
CRITERIOS PARA LA APROBACIÓN DE MEDICAMENTOS EN LA UNIÓN EUROPEA
Centralised Procedure EMEA - FDA Benchmarking 28/65 (43%) No Approval of the EMEA Approval of the FDA
 No Approval of the EMEA. Approval of the FDA.")
25
DIFERENCIAS CRITERIO FDA Y CHMP
Evaluación del beneficio-riesgo comparado ensayos frente a comparador activo (alternativas ya existentes) definición precisa de indicaciones Relevancia clínica del efecto Criterios para la aceptación beneficio-riesgo Variables subrogadas Autonomía vs paternalismo
 definición precisa de indicaciones. Relevancia clínica del efecto. Criterios para la aceptación beneficio-riesgo. Variables subrogadas. Autonomía vs paternalismo.")
26
EFALIZUMAB (RAPTIVA) FDA (2003)
RAPTlVA (efalizumab) is indicated for the treatment of adult patients (18 years or older) with chronic moderate to severe plaque psoriasis who are candidates for systemic therapy or phototherapy. EU (2004) Tratamiento de pacientes adultos con psoriasis en placas, crónica, moderada o grave, en los que ha fracasado la respuesta, o tienen una contraindicación o intolerancia, a otros tratamientos sistémicos, que incluyen ciclosporina, metotrexato y PUVA (ver epígrafe 5.1 – Eficacia Clínica). La eficacia de Raptiva frente a otros tratamientos sistémicos en pacientes con Psoriasis moderada o grave no se ha evaluado en estudios que comparen directamente Raptiva con otros tratamientos sistémicos. Los resultados actuales de Raptiva frente a placebo en estos pacientes indican una eficacia modesta de Raptiva (en cuanto a la respuesta PASI 75) (ver Tabla 2). En base a los datos de desarrollo clínico generados (ver Tabla 1) y a la limitada experiencia a largo plazo, se recomienda el uso de Raptiva en los pacientes definidos en el epígrafe 4.1.
 is indicated for the treatment of adult patients (18 years or older) with chronic moderate to severe plaque psoriasis who are candidates for systemic therapy or phototherapy. EU (2004) Tratamiento de pacientes adultos con psoriasis en placas, crónica, moderada o grave, en los que ha fracasado la respuesta, o tienen una contraindicación o intolerancia, a otros tratamientos sistémicos, que incluyen ciclosporina, metotrexato y PUVA (ver epígrafe 5.1 – Eficacia Clínica). La eficacia de Raptiva frente a otros tratamientos sistémicos en pacientes con Psoriasis moderada o grave no se ha evaluado en estudios que comparen directamente Raptiva con otros tratamientos sistémicos. Los resultados actuales de Raptiva frente a placebo en estos pacientes indican una eficacia modesta de Raptiva (en cuanto a la respuesta PASI 75) (ver Tabla 2). En base a los datos de desarrollo. clínico generados (ver Tabla 1) y a la limitada experiencia a largo plazo, se recomienda el uso de Raptiva en los pacientes definidos en el epígrafe 4.1.")
29
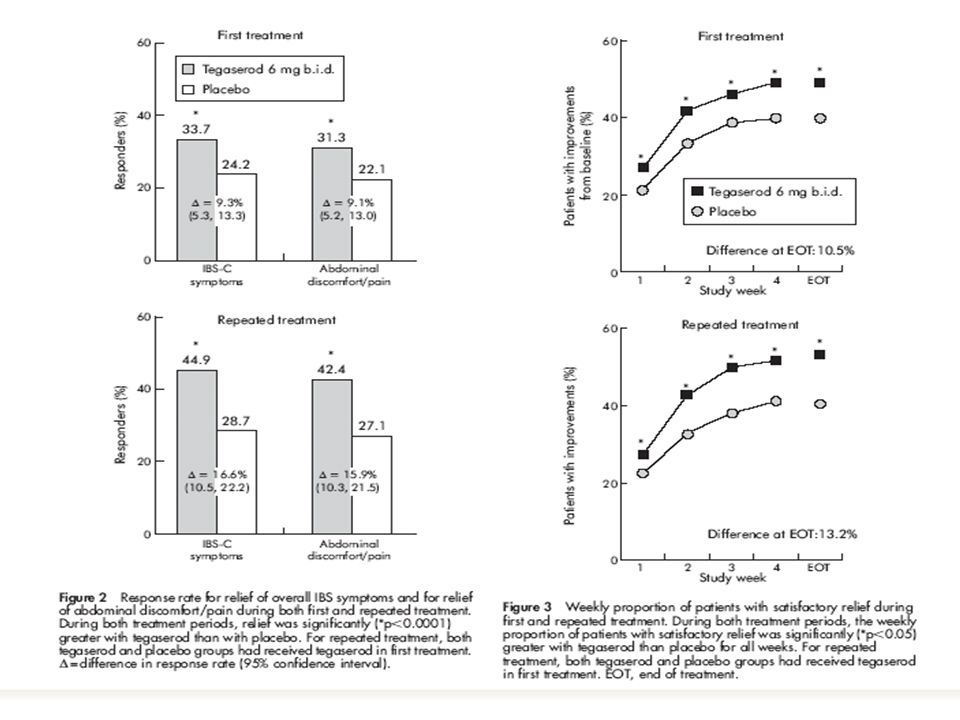
DENEGACION DE LA AUTORIZACION DE ZELNORM (Tegaserod) PARA EL TTO DEL COLON IRRITABLE
“The CHMP was concerned that the results of the study would not translate into real benefit to the patient treated to relieve the symptoms of this disorder in standard health care setting. The CHMP was of the opinion that Zelnorm’s benefits are not greater than its risks. Hence, the CHMP recommended that Zelnorm be refused marketing authorisation.” Tegaserod está aprobado en muchos países, en EEUU desde 2002 Indicado para el tratamiento a corto plazo del Sd intestino irritable en mujeres con síntomas predominantes de estreñimiento

33
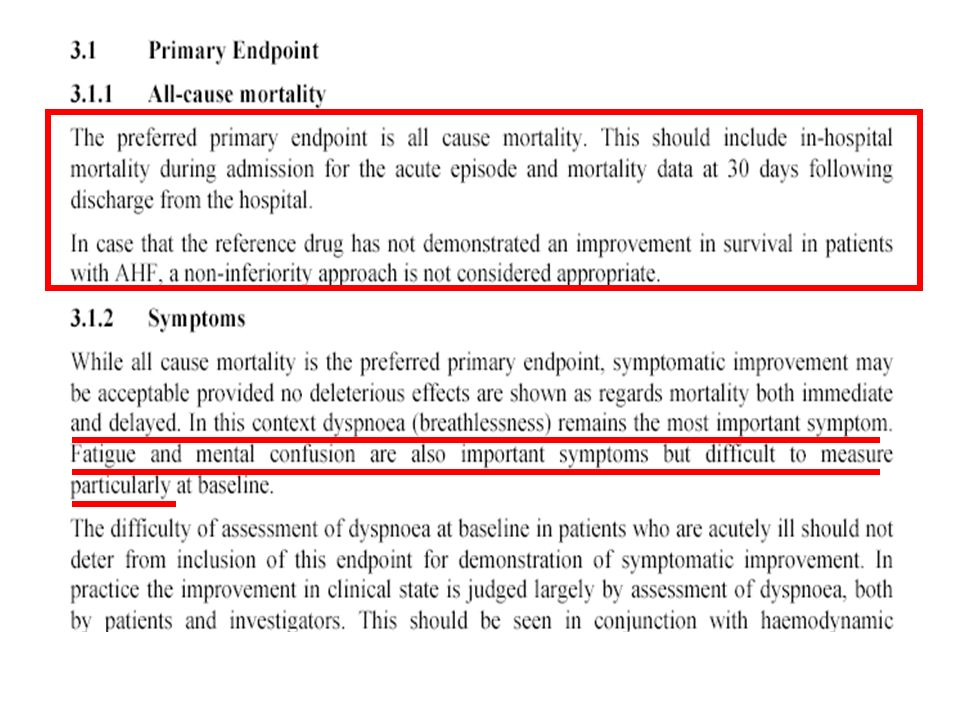
Statistically significant decrease of PCWP:
Intravenous nesiritide vs nitroglycerin for treatment of decompensated congestive heart failure: a randomized controlled trial. DESIGN: 480 patients with acute decompensation of CHF randomised to receive NTG, placebo or nesiritide. Primary end point : change after 3 hours treatment of pulmonary capillary wedge pressure (PCWP) and dyspnea RESULTS: Statistically significant decrease of PCWP: No difference in dyspnes at 6 hours ot 24 hours No difference in global status of the patient * Statistically better than Pbo but no difference vs NTG Trend to less survival at 6 months: mortality 20.8% NTG vs 25.1% NES. JAMA.2002; 287:
 and dyspnea. RESULTS: Statistically significant decrease of PCWP: No difference in dyspnes at 6 hours ot 24 hours. No difference in global status of the patient. * Statistically better than Pbo but no difference vs NTG. Trend to less survival at 6 months: mortality 20.8% NTG vs 25.1% NES. JAMA.2002; 287:")
34
Intravenous nesiritide vs nitroglycerin for treatment of decompensated congestive heart failure: a randomized controlled trial

35
Intravenous nesiritide vs nitroglycerin for treatment of decompensated congestive heart failure: a randomized controlled trial

36
INDICATIONS AND USAGE Serostim® [somatropin (rDNA origin) for injection] is indicated for the treatment of HIV patients with wasting or cachexia to increase lean body mass and body weight, and improve physical endurance. Concomitant antiretroviral therapy is necessary
 for injection] is indicated for the treatment of HIV patients with wasting or cachexia to increase lean body mass and body weight, and improve physical endurance. Concomitant antiretroviral therapy is necessary.")
37
The Marketing authorisation is refused on the following grounds

40
Application: first proposal of SPC made by the company
PRE-AUTHORIZATION Application: first proposal of SPC made by the company Assessment by Health Authorities: changes and commentaries to the SPC Succesive versions of SPC ... Proposed by the Company Marketing authorisation includes SPC

41
Marketing authorisation + approved SPC Variations: changes in SPC
POST-AUTHORIZATION New data in Renal Failure Manufacturing changes Pharmacovigilance Pediatric studies Changes in the Marketing autorisation holder Marketing authorisation + approved SPC New efficacy data in new therapeutic indications Much more... Variations: changes in SPC

42
Limitaciones de la FT Reflejan los usos para los que las Agencias de Medicamentos avalan públicamente su eficacia y seguridad Dependen de la evidencia generada por las Compañías No regulan la selección de medicamentos por el SNS No regulan la práctica médica

43
¿Se puede prescribir “fuera” de la FT?
Condiciones autorizadas Condiciones de uso

44
Food Drug & Cosmetic Act
SECTION 906. [ 21 U.S.C. 396] PRACTICE OF MEDICINE. “Nothing in this Act shall be construed to limit or interfere with the authority of a health care practitioner to prescribe or administer any legally marketed device to a patient for any condition or disease within a legitimate health care practitioner-patient relationship” DEVELOPMENT AND USE OF RISK MINIMIZATION ACTION PLANS (FDA GUIDANCE, MARCH 2005) “FDA recognizes that once it approves a product for marketing, healthcare practitioners are the most important managers of product risks. FDA believes that by including information in the FDA-approved professional labeling on the conditions in which medical products can be used safely and effectively by their intended population and for their intended use or uses, the Agency and the sponsor encourage healthcare practitioners to prescribe medical products in circumstances that yield a favorable benefit-risk balance. However, as the Agency has long recognized, the FDCA and FDA regulations establish requirements governing the safety and effectiveness of medical products. FDA does not have authority under these provisions to control decisions made by qualified healthcare practitioners to prescribe products for conditions other than those described in FDA-approved professional labeling, or to otherwise regulate medical or surgical practice”.
 FDA recognizes that once it approves a product for marketing, healthcare practitioners are the most important managers of product risks. FDA believes that by including information in the FDA-approved professional labeling on the conditions in which medical products can be used safely and effectively by their intended population and for their intended use or uses, the Agency and the sponsor encourage healthcare practitioners to prescribe medical products in circumstances that yield a favorable benefit-risk balance. However, as the Agency has long recognized, the FDCA and FDA regulations establish requirements governing the safety and effectiveness of medical products. FDA does not have authority under these provisions to control decisions made by qualified healthcare practitioners to prescribe products for conditions other than those described in FDA-approved professional labeling, or to otherwise regulate medical or surgical practice .")
45
¿Se puede seleccionar “fuera” de la FT?
Condiciones autorizadas Condiciones de uso

46
In 1989, Michigan became the first state to require certain
insurers/third-party payers (collectively, insurers) to provide coverage for the off-label use of prescription drugs for the treatment of cancer. Since that time and through June 30, 2002, 24 other states—Alabama, Arizona, Arkansas, Connecticut, Florida, Georgia, Illinois, Indiana, Kansas, Kentucky, Louisiana, Maine, Massachusetts, Minnesota, Mississippi, New Hampshire, New York, North Carolina, Ohio, Oklahoma, Rhode Island, South Carolina, South Dakota, and Virginia— have followed suit with similar laws. To illustrate the coverage requirement by type of insurer, insurers are divided into three categories. Private Insurers refers to any private insurers specified in the law, and may include individual and/or group insurers. Specified Managed Care means any managed care organization specified in the law, and may include health maintenance organizations, preferred provider organizations, and/or other managed care entities. Public Employee Health Plans includes any specified health plan for state or public employees. All 25 states with off-label prescription drug use laws mandate coverage by specified private insurers. Eighteen states require coverage by private managed care entities and four states mandate coverage by public employee health plans. The provisions contained in the off-label laws in 19 states require that, in order for certain drugs to be covered, they must be recognized for treatment of the specific type of cancer or indication by either standard reference compendia or medical/peer-reviewed literature. Three states specify that the drugs must be recognized by standard reference compendia only, and three states don’t specify such requirements. In addition to the specified coverage, 16 states also mandate coverage for medically necessary services required to administer the drug during treatment. Notably, a number of states, including California, Maryland, New Jersey, Oregon, and Tennessee, have enacted off-label drug use laws that do not explicitly address cancer treatment; instead, they refer to life-threatening conditions or generic offlabel indications. Because they are not cancer-specific, they fall outside the scope of the SCLD Program and are not included on the chart above. Ohio is unique in that it has enacted both a cancer- specific and a generic law. bbIn 1989, Michigan became the first state to require certain
 to provide coverage. for the off-label use of prescription drugs for the treatment. of cancer. Since that time and through June 30, 2002, 24 other. states—Alabama, Arizona, Arkansas, Connecticut, Florida, Georgia, Illinois, Indiana, Kansas, Kentucky, Louisiana, Maine, Massachusetts, Minnesota, Mississippi, New. Hampshire, New York, North Carolina, Ohio, Oklahoma, Rhode Island, South Carolina, South Dakota, and Virginia— have followed suit with similar laws. To illustrate the coverage requirement by type of insurer, insurers. are divided into three categories. Private Insurers refers to any. private insurers specified in the law, and may include individual. and/or group insurers. Specified Managed Care means any. managed care organization specified in the law, and may include. health maintenance organizations, preferred provider organizations, and/or other managed care entities. Public Employee. Health Plans includes any specified health plan for state or public. employees. All 25 states with off-label prescription drug use laws mandate coverage. by specified private insurers. Eighteen states require coverage. by private managed care entities and four states mandate coverage. by public employee health plans. The provisions contained in the off-label laws in 19 states require. that, in order for certain drugs to be covered, they must be recognized. for treatment of the specific type of cancer or indication by. either standard reference compendia or medical/peer-reviewed. literature. Three states specify that the drugs must be recognized. by standard reference compendia only, and three states don’t. specify such requirements. In addition to the specified coverage, 16 states also mandate coverage. for medically necessary services required to administer the. drug during treatment. Notably, a number of states, including California, Maryland, New Jersey, Oregon, and Tennessee, have enacted off-label. drug use laws that do not explicitly address cancer treatment; instead, they refer to life-threatening conditions or generic offlabel. indications. Because they are not cancer-specific, they fall. outside the scope of the SCLD Program and are not included on. the chart above. Ohio is unique in that it has enacted both a cancer- specific and a generic law. bbIn 1989, Michigan became the first state to require certain.")
48
Retos para el futuro Mantener en Europa la solicitud (pre-autorización) de ensayos clínicos frente a comparadores activos Asumir que la AEMPS/EMEA seguirá autorizando nuevos medicamentos caros y de eficacia modesta y NO incorporará criterios de valor añadido o eficiencia a sus decisiones Emprender el desarrollo de un buen sistema de selección de medicamentos por el SNS, basado en la efectividad real del medicamento, transparente, con solidez metodológica, coherencia interna y participación de clínicos y pacientes,

50
CRITERIOS PARA LA APROBACIÓN DE MEDICAMENTOS EN LA UNIÓN EUROPEA
¿CAMBIOS EN ESTA REGULACION ? These new provisions provide tools to speed up patients’ and healthcare professionals’ access to medicinal products in the Community. They also introduce measures for better safety monitoring of medicinal products for human and veterinary use, as well as tools for increased transparency, provision of information and improved communication between the Agency and national competent authorities and the different stakeholders of the EU pharmaceuticals regulatory system

51
In 1989, Michigan became the first state to require certain insurers/third-party payers (collectively, insurers) to provide coverage for the off-label use of prescription drugs for the treatment of cancer. Since that time and through June 30, 2002, 24 other states—Alabama, Arizona, Arkansas, Connecticut, Florida,Georgia, Illinois, Indiana, Kansas, Kentucky, Louisiana,Maine, Massachusetts, Minnesota, Mississippi, NewHampshire, New York, North Carolina, Ohio, Oklahoma, Rhode Island, South Carolina, South Dakota, and Virginia—have followed suit with similar laws. To illustrate the coverage requirement by type of insurer, insurers are divided into three categories. Private Insurers refers to any private insurers specified in the law, and may include individual and/or group insurers. Specified Managed Care means any managed care organization specified in the law, and may include health maintenance organizations, preferred provider organizations,and/or other managed care entities. Public EmployeeHealth Plans includes any specified health plan for state or public employees. All 25 states with off-label prescription drug use laws mandate coverage by specified private insurers. Eighteen states require coverageby private managed care entities and four states mandate coverage by public employee health plans. The provisions contained in the off-label laws in 19 states require that, in order for certain drugs to be covered, they must be recognized for treatment of the specific type of cancer or indication by either standard reference compendia or medical/peer-reviewed literature. Three states specify that the drugs must be recognized by standard reference compendia only, and three states don’t specify such requirements. In addition to the specified coverage, 16 states also mandate coverage for medically necessary services required to administer the drug during treatment. Notably, a number of states, including California, Maryland,New Jersey, Oregon, and Tennessee, have enacted off-label drug use laws that do not explicitly address cancer treatment; instead, they refer to life-threatening conditions or generic off label indications. Because they are not cancer-specific, they fall outside the scope of the SCLD Program and are not included on the chart above. Ohio is unique in that it has enacted both a cancer- specific and a generic law. In 1989, Michigan became the first state to require certain insurers/third-party payers (collectively, insurers) to provide coverage for the off-label use of prescription drugs for the treatment of cancer. Since that time and through June 30, 2002, 24 other states—Alabama, Arizona, Arkansas, Connecticut, Florida, Georgia, Illinois, Indiana, Kansas, Kentucky, Louisiana, Maine, Massachusetts, Minnesota, Mississippi, New Hampshire, New York, North Carolina, Ohio, Oklahoma, Rhode Island, South Carolina, South Dakota, and Virginia— have followed suit with similar laws. To illustrate the coverage requirement by type of insurer, insurers are divided into three categories. Private Insurers refers to any private insurers specified in the law, and may include individual and/or group insurers. Specified Managed Care means any managed care organization specified in the law, and may include health maintenance organizations, preferred provider organizations, and/or other managed care entities. Public Employee Health Plans includes any specified health plan for state or public employees. All 25 states with off-label prescription drug use laws mandate coverage by specified private insurers. Eighteen states require coverage
 to provide coverage. for the off-label use of prescription drugs for the treatment. of cancer. Since that time and through June 30, 2002, 24 other. states—Alabama, Arizona, Arkansas, Connecticut, Florida, Georgia, Illinois, Indiana, Kansas, Kentucky, Louisiana, Maine, Massachusetts, Minnesota, Mississippi, New. Hampshire, New York, North Carolina, Ohio, Oklahoma, Rhode Island, South Carolina, South Dakota, and Virginia— have followed suit with similar laws. To illustrate the coverage requirement by type of insurer, insurers. are divided into three categories. Private Insurers refers to any. private insurers specified in the law, and may include individual. and/or group insurers. Specified Managed Care means any. managed care organization specified in the law, and may include. health maintenance organizations, preferred provider organizations, and/or other managed care entities. Public Employee. Health Plans includes any specified health plan for state or public. employees. All 25 states with off-label prescription drug use laws mandate coverage. by specified private insurers. Eighteen states require coverage.")
52
Aprepitant (Emend) Prevention of acute and delayed nausea and vomiting associated with highly emetogenic cisplatin based cancer chemotherapy. Prevention of nausea and vomiting associated with moderately emetogenic cancer chemotherapy.

53
respondieron por grupo de tratamiento y fase durante elCiclo 1
Tabla 1: Porcentaje de pacientes que estaban recibiendo quimioterapia altamente emetógena que respondieron por grupo de tratamiento y fase durante elCiclo 1 Régimen con aprepitant (n=521) Tto estándar (n=524) Diferencias(IC al 95%) Respuesta completa (sin emesis y sin tratamiento de rescate) Global (0-120h) 67,7% 47,8% 19,9% (14,0-25,8) 0-24h 86,0% 73,2% 12,7% (7,9-17,6) 25-120h 71,5% 51,2% 20,3% (14,5-26,1) Tabla 2: Porcentaje de pacientes que respondieron por grupo de tratamiento y fase durante elCiclo 1. QT moderadamente emetógena Régimen con aprepitant (n=433) Tto estándar (n=424) Diferencias(IC al 95%) Respuesta completa (sin emesis y sin tratamiento de rescate) Global (0-120h) 50,8% 42,5% 8,3% (1,6-15,0) 0-24h 75,7% 69,0% 6,7% (0,7-12,7) 25-120h 55,4% 49,1% 6,3% (14,5-26,1)
 Tto estándar (n=524) Diferencias(IC al 95%) Respuesta completa (sin emesis y sin tratamiento de rescate) Global (0-120h) 67,7% 47,8% 19,9% (14,0-25,8) 0-24h. 86,0% 73,2% 12,7% (7,9-17,6) h. 71,5% 51,2% 20,3% (14,5-26,1) Tabla 2: Porcentaje de pacientes que respondieron por grupo de tratamiento y fase durante elCiclo 1. QT moderadamente emetógena. Régimen con aprepitant (n=433) Tto estándar (n=424) Diferencias(IC al 95%) Respuesta completa (sin emesis y sin tratamiento de rescate) Global (0-120h) 50,8% 42,5% 8,3% (1,6-15,0) 0-24h. 75,7% 69,0% 6,7% (0,7-12,7) h. 55,4% 49,1% 6,3% (14,5-26,1)")
54
CONCLUSIONES La asociación de aprepitant al tratamiento estándar para la prevención de náuseas y vómitos por QT altamente emetógena (platino) supone una mejoría de eficacia que puede ser relevante para los pacientes. En un intento de buscar el máximo beneficio con el menor coste, podría valorarse la utilización inicial (desde el primer ciclo) sólo en pacientes de alto riesgo (mujeres, antecedentes hiperemesis gravídica,..). En la prevención de las nausea y vómitos asociados a QT moderadamente emetógena, el beneficio de aprepitant es menos relevante y no parece justificado asociar este fármaco al tratamiento estándar. Es previsible que clínicos y pacientes consideren adecuado asociar este fármaco en los ciclos siguientes una vez han aparecido vómitos en el primer ciclo o en ciclos anteriores. No existen datos que permitan evaluar el beneficio de la asociación de aprepitant en ciclos siguientes una vez ya ha fracasado la prevención en los primeros ciclos. En caso de que el medicamento se utilice de ese modo, conviene re-evaluar la eficacia en cuanto se disponga de datos.
 supone una mejoría de eficacia que puede ser relevante para los pacientes. En un intento de buscar el máximo beneficio con el menor coste, podría valorarse la utilización inicial (desde el primer ciclo) sólo en pacientes de alto riesgo (mujeres, antecedentes hiperemesis gravídica,..). En la prevención de las nausea y vómitos asociados a QT moderadamente emetógena, el beneficio de aprepitant es menos relevante y no parece justificado asociar este fármaco al tratamiento estándar. Es previsible que clínicos y pacientes consideren adecuado asociar este fármaco en los ciclos siguientes una vez han aparecido vómitos en el primer ciclo o en ciclos anteriores. No existen datos que permitan evaluar el beneficio de la asociación de aprepitant en ciclos siguientes una vez ya ha fracasado la prevención en los primeros ciclos. En caso de que el medicamento se utilice de ese modo, conviene re-evaluar la eficacia en cuanto se disponga de datos.")
Presentaciones similares





 European Transfer Credit System (ECTS) Methodology in.>")



.>")













