Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Analgesia en pacientes con ERC
Francisco José de la Prada Alvarez Servicio de Nefrología Hospital Son Dureta

4
M01-ANTIINFLAMATORIOS Y ANTIRREUMÁTICOS NO ESTEROIDEOS
Ver en el grupo N02B otros analgésicos y antiinflamatorios no esteroideos disponibles en el hospital NOMBRE GENÉRICO PRESENTACIÓN VIA NOMBRE COMERCIAL Diclofenac Amp 75 mg/3 ml Comp 50 mg Sup 100 mg IM, IV OR REC Voltaren Ibuprofeno Jbe 100 mg/5ml Comp 400 mg Comp 600 mg Sobres 200 mg Dalsy jarabe Neobrufen Indometacina Caps 25 mg Inacid, Artrinovo Isonixina Sup inf 200 mg Nyxin Piroxicam Caps 20 mg Comp 20 mg Sasulen, Feldene 20, Vitaxicam, Feldene flas Nota 1: Otros medicamentos del grupo de los AINEs como por ejemplo: Ketoprofeno (Arcental, Fastum, Orudis), Naproxeno (Naprosyn), Aceclofenaco (Airtal, Falcol, Gerbin), Fenbufeno (Cincopal), Flurbiprofeno (Froben), Namebutona (Dolsinal,, Relif), Tenoxicam (Reutenox, Tilcotil), Meloxicam (Movalis) y Tolmetin (Artrocaptin) son medicamentos no incluidos en la Guía y se consideran equivalentes terapéuticos de los AINEs incluidos. Consultar programa de intercambio.
, Naproxeno (Naprosyn), Aceclofenaco (Airtal, Falcol, Gerbin), Fenbufeno (Cincopal), Flurbiprofeno (Froben), Namebutona (Dolsinal,, Relif), Tenoxicam (Reutenox, Tilcotil), Meloxicam (Movalis) y Tolmetin (Artrocaptin) son medicamentos no incluidos en la Guía y se consideran equivalentes terapéuticos de los AINEs incluidos. Consultar programa de intercambio.")
5
N02B-Analgésicos no narcóticos y antipiréticos
Ver en grupo M01 otros analgésicos no narcóticos y antipiréticos NOMBRE GENÉRICO PRESENTACIÓN Com NOMBRE COMERCIAL Acetilsalicilato de lisina (1)(4) Sobres 1,8 g Vial 900 mg/5 ml OR IM,IV Inyesprin oral forte Inyesprin iny(4) Acido Acetilsalicílico Comp 500 mg Comp 300 mg Comp 125 mg Ácido Acetilsalicilíco, Adiro, Aspirina Aspirina infantil Ketorolaco Comp 10 mg Amp 30 mg/1 ml IV. IM Droal, Toradol Metamizol (Dipirona) (Noramidopirina) Amp 2000 mg/5 ml Caps 575 mg Sup 1 g Sup 500 mg IV, IM, OR REC Nolotil, Lasain Paracetamol Comp 500 mg Gts 100 mg/ml (2) Sup 150 mg Sup 250 mg Vial 1g/100ml IV Termalgin, Dolgesic, Gelocatil (650 mg) Apiretal Febrectal Lactante Melabon Infantil Perfalgan Paracetamol +Codeína Comp 300mg +15mg Comp 650 mg + 30 mg Termalgin Codeína; Gelocatil Codeina Nota 1: 1,8 g de Acetilsalicilato de lisina=1g de Acido Acetil Salicílico. Nota 2: gota=4 mg Nota 3: Propacetamol es un precursor del Paracetamol. Propacetamol 1 g libera Paracetamol 500 mg.
(4) Sobres 1,8 g. Vial 900 mg/5 ml. OR. IM,IV. Inyesprin oral forte. Inyesprin iny(4) Acido Acetilsalicílico. Comp 500 mg. Comp 300 mg. Comp 125 mg. Ácido Acetilsalicilíco, Adiro, Aspirina. Aspirina infantil. Ketorolaco. Comp 10 mg. Amp 30 mg/1 ml. IV. IM. Droal, Toradol. Metamizol (Dipirona) (Noramidopirina) Amp 2000 mg/5 ml. Caps 575 mg. Sup 1 g. Sup 500 mg. IV, IM, OR. REC. Nolotil, Lasain. Paracetamol. Comp 500 mg. Gts 100 mg/ml (2) Sup 150 mg. Sup 250 mg. Vial 1g/100ml. IV. Termalgin, Dolgesic, Gelocatil (650 mg) Apiretal. Febrectal Lactante. Melabon Infantil. Perfalgan. Paracetamol +Codeína. Comp 300mg +15mg. Comp 650 mg + 30 mg. Termalgin Codeína; Gelocatil Codeina. Nota 1: 1,8 g de Acetilsalicilato de lisina=1g de Acido Acetil Salicílico. Nota 2: gota=4 mg. Nota 3: Propacetamol es un precursor del Paracetamol. Propacetamol 1 g libera Paracetamol 500 mg.")
6
Opioides Los opiodes agonistas son aquellos que al fijarse al receptor mu dan lugar a una respuesta farmacológica, que en este caso es la eliminación del dolor.

7
Opioides Los opiodes antagonistas son aquellos que también se unen al receptor mu, pero ello no va seguido de una respuesta farmacológica, es decir, en este caso no se produciría analgesia.

8
Opioides Existe otro tipo de opioides denominados agonistas-antagonistas, que son capaces de actuar como agonistas sobre un tipo de receptores y como antagonistas sobre otro tipo, por lo que producen respuestas imprevisibles. En pacientes que reciben agonistas puros, los agonistas-antagonistas pueden precipitar reacciones de abstinencia.

9
Para dolor moderado-severo Agonistas puros Morfina Metanol Petidina
Semivida corta Semivida larga Para dolor moderado-severo Agonistas puros Morfina Metanol Petidina Levorfanol Heroina Fentanilo Sulfentanilo Tramadol Oxicodona Oximorfona Para dolor ligero-moderado Codeina Dihidrocodeina Dextropropoxifeno

10
Semivida corta Semivida larga Agonistas-Antagonistas Pentazosina Butorfanol Nalbufina Dezocina Meperidina Agonistas parciales Buprenorfina

11
Tratamientos de rescate potenciales para el dolor intercurrente o irruptivo en pacientes con cancer
Opioides utilizados para el dolor crónico de base: Agonistas puros preferentemente en formas de liberación retardada Morfina de liberación lenta Fentanilo via transdermica Tratamiento de rescate: Agonistas puros en forma de liberación rápida o vias de absorción rápida: Morfina por via parenteral. Fentanilo por via transmucosa oral.

12
Tratamientos de rescate potenciales para el dolor intercurrente o irruptivo en pacientes con cancer
Opioides utilizados para el dolor crónico de base: Agonistas parciales: Buprenorfina de liberación transdermica. Tratamiento de rescate: Agonistas parciales: buprenorfina sublingual. Agonistas puros: Morfina por via parenteral. Fentanilo por via transmucosa oral.

13
DOSIS EQUIANALGESICAS ENTRE LOS DISTINTOS OPIOIDES ADMINSTRADOS POR VIA ORAL
Morfina 30-60 mg Meperidina 300 mg Metadona 15-20 mg Tramadol mg Codeina 400 mg Dihidrocodeina 240 mg Hidromorfona 7,5 mg Levorfanol 4 mg Oxicodona 30 mg

14
Equivalent opioid doses
Drug Time to onset (minutes) Oral dose (mg) Parenteral dose (mg) Morphine sulfate parenteral 10 q4 hr Morphine sulfate oral (MSIR, Roxanol) 15 to 60 30 q4 hr Morphine sulfate controlled release (MS contin, Oramorph) 90 q12 hr not available Codeine 10 to 30 200 q4 hr 100 to 120 q4 hr Oxycodone (Percocet, Percodan, Tylox) 15 to 30 15 to 20 q4 hr Oxycodone controlled release (Oxycontin) 45 to 60 q12 hr Hydromorphone (Dilaudid) 8 q4 hr q4 hr Levorphanol (Levodromoran) 30 to 90 4 q6 to q8 hr 2 q6 to q8 hr Meperidine (Demerol) 10 to 45 300 q2 to q3 hr 100 q2 to q3 hr Methadone (Dolophine) 30 to 60 20* q6 to q12 hr 10 q6 hr Equivalent opioid doses * A dose ratio of 1:4 (1 mg of oral methadone = 4 mg of oral morphine) is used for patients receiving less than 90 mg of morphine. Patients receiving 90 to 300 mg/day receive methadone at a ratio of 1:8. Finally, a ratio of 1:12 is used for patients receiving morphine doses greater than 300 mg/day.
 Oral dose (mg) Parenteral dose (mg) Morphine sulfate parenteral. 10 q4 hr. Morphine sulfate oral (MSIR, Roxanol) 15 to q4 hr. Morphine sulfate controlled release (MS contin, Oramorph) 90 q12 hr. not available. Codeine. 10 to q4 hr. 100 to 120 q4 hr. Oxycodone (Percocet, Percodan, Tylox) 15 to to 20 q4 hr. Oxycodone controlled release (Oxycontin) 45 to 60 q12 hr. Hydromorphone (Dilaudid) 8 q4 hr q4 hr. Levorphanol (Levodromoran) 30 to q6 to q8 hr. 2 q6 to q8 hr. Meperidine (Demerol) 10 to q2 to q3 hr. 100 q2 to q3 hr. Methadone (Dolophine) 30 to * q6 to q12 hr. 10 q6 hr. Equivalent opioid doses. * A dose ratio of 1:4 (1 mg of oral methadone = 4 mg of oral morphine) is used for patients receiving less than 90 mg of morphine. Patients receiving 90 to 300 mg/day receive methadone at a ratio of 1:8. Finally, a ratio of 1:12 is used for patients receiving morphine doses greater than 300 mg/day.")
15
Opioid Analgesics - Initial Oral Dosing Commonly Used for Severe Pain
Buprenorphine: Equianalgesic Dose Oral: n/a Parenteral: 0.4 mg Initial Oral Dose Children: n/a Adults: n/a Butorphanol: Equianalgesic Dose Parenteral: 2 mg Levorphanol: Equianalgesic Dose Oral: Acute: 4 mg; Chronic: 1 mg Parenteral: Acute: 2 mg; Chronic: 1 mg Initial Oral Dose Children: 0.04 mg/kg Adults: 2-4 mg/kg Meperidine: Equianalgesic Dose Oral: 300 mg Parenteral: 75 mg Children: Not recommended Adults: Not recommended

16
Opioid Analgesics - Initial Oral Dosing Commonly Used for Severe Pain
Hydromorphone: Equianalgesic Dose Oral: 7.5 mg Parenteral: 1.5 mg Initial Oral Dose Children: 0.06 mg/kg Adults: 4-8 mg Methadone: Equianalgesic Dose Oral: 10 mg Parenteral: 5 mg Children: 0.2 mg/kg Adults: 5-10 mg Morphine: Equianalgesic Dose Oral: 30 mg Parenteral: 10 mg Initial Oral Dose Children: 0.3 mg/kg Adults: mg Nalbuphine: Equianalgesic Dose Oral: n/a Children: n/a Adults: n/a

17
Opioid Analgesics - Initial Oral Dosing Commonly Used for Severe Pain
Pentazocine: Equianalgesic Dose Oral: 50 mg Parenteral: 30 mg Initial Oral Dose Children: n/a Adults: n/a Oxycodone: Equianalgesic Dose Oral: 20 mg Parenteral: n/a Children: 0.3 mg/kg Adults: mg Oxymorphone: Equianalgesic Dose Oral: 1 mg Parenteral: n/a Initial Oral Dose Children: n/a Adults: n/a From "Principles of Analgesic Use in the Treatment of Acute Pain and Cancer Pain,"Am Pain Soc, Fifth Ed.

19
Codeína Comp 28 mg OR Codeisan N02A-Analgésicos narcóticos (Opioides)
NOMBRE GENÉRICO PRESENTACIÓN VIA NOMBRE COMERCIAL Buprenorfina Comp 0,2 mg Amp 0,3 mg/1 ml SL IM, IV Buprex CE Codeína Comp 28 mg OR Codeisan Dihidrocodeína (Hidrocodona) Comp 60 mg Contugesic Fentanilo (2) Parche 2,5 mg (3) Parche 5 mg (3) Parche 10 mg (3) TOP Durogesic 25 Durogesic 50 Durogesic 100 Metadona Amp 10 mg/1 ml Comp 5 mg Comp 40 mg SC, IM Metasedin CE Morfina cloruro (sin conservantes) Vial 400 mg/20 ml (vial multidosis, sin conservantes) Amp 10 ml. SC, IV, IM SC IV, IM Cloruro Mórfico Braun 1 % CE Morfina Braun 2 % s/c CE Morfina Braun 4 % s/c CE Morfina clorhidrato Jbe 10 mg/ml Brompton FM CE Morfina sulfato Comp 10 mg Comp 20 mg Sevredol CE (1) Morfina sulfato retard Comp 30 mg Comp 100 mg MST Continus CE Petidina (Meperidina) Amp 100 mg/2 ml SC, IM, IV Dolantina CE Tramadol Caps 50 mg Comp retard 200 mg Comp retard 300 mg Amp 100 mg/2 m Adolonta, Tralgiol Zytram CE: Control de estupefacientes. Nota 1: Comprimidos ranurados. Nota 2: Uso restringido para tratamiento del dolor crónico. Nota 3: Los parches de 2,5, 5 y 10 mg liberan respectivamente 25, 50 y 100 mcg/h durante 72 h.
 Comp 60 mg. Contugesic. Fentanilo (2) Parche 2,5 mg (3) Parche 5 mg (3) Parche 10 mg (3) TOP. Durogesic 25. Durogesic 50. Durogesic 100. Metadona. Amp 10 mg/1 ml. Comp 5 mg. Comp 40 mg. SC, IM. Metasedin CE. Morfina cloruro. (sin conservantes) Vial 400 mg/20 ml. (vial multidosis, sin conservantes) Amp 10 ml. SC, IV, IM. SC. IV, IM. Cloruro Mórfico Braun 1 % CE. Morfina Braun 2 % s/c CE. Morfina Braun 4 % s/c CE. Morfina clorhidrato. Jbe 10 mg/ml. Brompton FM CE. Morfina sulfato. Comp 10 mg. Comp 20 mg. Sevredol CE (1) Morfina sulfato retard. Comp 30 mg. Comp 100 mg. MST Continus CE. Petidina (Meperidina) Amp 100 mg/2 ml. SC, IM, IV. Dolantina CE. Tramadol. Caps 50 mg. Comp retard 200 mg. Comp retard 300 mg. Amp 100 mg/2 m. Adolonta, Tralgiol. Zytram. CE: Control de estupefacientes. Nota 1: Comprimidos ranurados. Nota 2: Uso restringido para tratamiento del dolor crónico. Nota 3: Los parches de 2,5, 5 y 10 mg liberan respectivamente 25, 50 y 100 mcg/h durante 72 h.")
20
N02B-Analgésicos no narcóticos y antipiréticos
Ver en grupo M01 otros analgésicos no narcóticos y antipiréticos NOMBRE GENÉRICO PRESENTACIÓN Com NOMBRE COMERCIAL Acetilsalicilato de lisina (1)(4) Sobres 1,8 g Vial 900 mg/5 ml OR IM,IV Inyesprin oral forte Inyesprin iny(4) Acido Acetilsalicílico Comp 500 mg Comp 300 mg Comp 125 mg Ácido Acetilsalicilíco, Adiro, Aspirina Aspirina infantil Ketorolaco Comp 10 mg Amp 30 mg/1 ml IV. IM Droal, Toradol Metamizol (Dipirona) (Noramidopirina) Amp 2000 mg/5 ml Caps 575 mg Sup 1 g Sup 500 mg IV, IM, OR REC Nolotil, Lasain Paracetamol Comp 500 mg Gts 100 mg/ml (2) Sup 150 mg Sup 250 mg Vial 1g/100ml IV Termalgin, Dolgesic, Gelocatil (650 mg) Apiretal Febrectal Lactante Melabon Infantil Perfalgan Paracetamol +Codeína Comp 300mg +15mg Comp 650 mg + 30 mg Termalgin Codeína; Gelocatil Codeina Nota 1: 1,8 g de Acetilsalicilato de lisina=1g de Acido Acetil Salicílico. Nota 2: gota=4 mg Nota 3: Propacetamol es un precursor del Paracetamol. Propacetamol 1 g libera Paracetamol 500 mg.
(4) Sobres 1,8 g. Vial 900 mg/5 ml. OR. IM,IV. Inyesprin oral forte. Inyesprin iny(4) Acido Acetilsalicílico. Comp 500 mg. Comp 300 mg. Comp 125 mg. Ácido Acetilsalicilíco, Adiro, Aspirina. Aspirina infantil. Ketorolaco. Comp 10 mg. Amp 30 mg/1 ml. IV. IM. Droal, Toradol. Metamizol (Dipirona) (Noramidopirina) Amp 2000 mg/5 ml. Caps 575 mg. Sup 1 g. Sup 500 mg. IV, IM, OR. REC. Nolotil, Lasain. Paracetamol. Comp 500 mg. Gts 100 mg/ml (2) Sup 150 mg. Sup 250 mg. Vial 1g/100ml. IV. Termalgin, Dolgesic, Gelocatil (650 mg) Apiretal. Febrectal Lactante. Melabon Infantil. Perfalgan. Paracetamol +Codeína. Comp 300mg +15mg. Comp 650 mg + 30 mg. Termalgin Codeína; Gelocatil Codeina. Nota 1: 1,8 g de Acetilsalicilato de lisina=1g de Acido Acetil Salicílico. Nota 2: gota=4 mg. Nota 3: Propacetamol es un precursor del Paracetamol. Propacetamol 1 g libera Paracetamol 500 mg.")
21
Codeina Opioide estructuralmente relacionada con la morfina.
Es un alcaloide presente en la Papaver somniferum. Estructuralmente es la metilmorfina y existen estudios que sugieren que sus efectos son, al menos en parte, consecuencia de la desmetilación en el organismo a morfina que sería el principio activo. Sus propiedades analgésicas son similares a las de la morfina pero su potencia es sólo un 12%. La codeína se comporta como un agonista opioide puro de los receptores Mu y, por esta razón, su mecanismo de acción y los efectos derivados de este son, en principio, similares a los de la morfina

22
Codeina Los opioides que actúan sobre el receptor mu aminoran la transmisión en la médula espinal, mediante una inhibición relacionada con la dosis, de la actividad del tracto neural. En los ganglios basales del cerebro, los opioides activan el sistema inhibidor descendente, que limita la transmisión del dolor a la altura de la médula espinal. Los opioides también producen cambios en el cerebro, lo que provoca una alteración de las respuestas emocionales y aminoran en gran medida la percepción del dolor.

23
Properties of opioid receptors
Mu Mu1 Supraspinal analgesia Bradycardia Sedation Mu2 Respiratory depression Euphoria Physical dependence Delta Spinal analgesia Kappa Spinal Analgesia Sigma Dysphoria, delirium Hallucinations Tachycardia, hypertension

24
Codeina DOSING: ADULTS or ELDERLY
Doses >1.5 mg/kg body weight are not recommended. Pain management (analgesic): Oral, regular release: 30 mg every 4-6 hours as needed; patients with prior opiate exposure may require higher initial doses. Usual range: mg every 4-6 hours as needed Oral, controlled release formulation (Codeine Contin®, not available in U.S.): mg every 12 hours. I.M., SubQ: 30 mg every 4-6 hours as needed; patients with prior opiate exposure may require higher initial doses. Usual range: mg every 4-6 hours as needed; more frequent dosing may be needed Cough (antitussive): Oral (for nonproductive cough): mg/dose every 4-6 hours as needed; maximum: 120 mg/day
: Oral, regular release: 30 mg every 4-6 hours as needed; patients with prior opiate exposure may require higher initial doses. Usual range: mg every 4-6 hours as needed Oral, controlled release formulation (Codeine Contin®, not available in U.S.): mg every 12 hours. I.M., SubQ: 30 mg every 4-6 hours as needed; patients with prior opiate exposure may require higher initial doses. Usual range: mg every 4-6 hours as needed; more frequent dosing may be needed. Cough (antitussive): Oral (for nonproductive cough): mg/dose every 4-6 hours as needed; maximum: 120 mg/day.")
26
Codeina DOSING: PEDIATRIC — Analgesic: Oral, I.M., SubQ:
Children: mg/kg/dose every 4-6 hours as needed; maximum: 60 mg/dose Antitussive: Oral (for nonproductive cough): Children: mg/kg/day in divided doses every 4-6 hours as needed: Alternative dose according to age: 2-6 years: mg every 4-6 hours as needed; maximum: 30 mg/day 6-12 years: 5-10 mg every 4-6 hours as needed; maximum: 60 mg/day
: Children: mg/kg/day in divided doses every 4-6 hours as needed: Alternative dose according to age: 2-6 years: mg every 4-6 hours as needed; maximum: 30 mg/day 6-12 years: 5-10 mg every 4-6 hours as needed; maximum: 60 mg/day.")
27
Codeina DOSING: HEPATIC IMPAIRMENT — Dosing adjustment is probably necessary in hepatic insufficiency.

28
Vida media de eliminación prolongada en pacientes en diálisis.
Dosis de carga Dosis de mantenimiento FG > 50 ml/min FG ml/min FG < 10 ml/min Dosis suplemtaria tras HD DPCA TSCR Codeina 100 % 75% 50% Descono-cida Desono-cida Vida media de eliminación prolongada en pacientes en diálisis.

29
Codeina ADVERSE REACTIONS SIGNIFICANT Frequency not defined: AST/ALT increased >10%: Central nervous system: Somnolencia Gastrointestinal: Estreñimiento 1% to 10%: Cardiovascular: Tachycardia or bradycardia, hypotension Central nervous system: Dizziness, lightheadedness, false feeling of well being, malaise, headache, restlessness, paradoxical CNS stimulation, confusion Dermatologic: Rash, urticaria Gastrointestinal: Dry mouth, anorexia, nausea, vomiting Genitourinary: Urination decreased, ureteral spasm Hepatic: LFTs increased Local: Burning at injection site Neuromuscular & skeletal: Weakness Ocular: Blurred vision Respiratory: Dyspnea Miscellaneous: Histamine release <1% (Limited to important or life-threatening): Convulsions, hallucinations, insomnia, mental depression, nightmares
: Convulsions, hallucinations, insomnia, mental depression, nightmares.")
30
Codeina DRUG INTERACTIONS — Substrate of CYP2D6 (major), 3A4 (minor); Inhibits CYP2D6 (weak) CYP2D6 inhibitors: May decrease the effects of codeine. Example inhibitors include chlorpromazine, delavirdine, fluoxetine, miconazole, paroxetine, pergolide, quinidine, quinine, ritonavir, and ropinirole. Decreased effect with cigarette smoking Increased toxicity: CNS depressants, phenothiazines, TCAs, other narcotic analgesics, guanabenz, MAO inhibitors, neuromuscular blockers

31
Codeina Embarazo y Lactancia. Contraindicado.

32
Codeina REFERENCE RANGE — Sobredosis: Therapeutic: Not established;
Toxic: >1.1 mcg/mL Sobredosis: Symptoms include CNS and respiratory depression, gastrointestinal cramping, and constipation. Treatment includes naloxone 2 mg I.V. (0.01 mg/kg for children), with repeat administration as necessary, up to a total of 10 mg.
, with repeat administration as necessary, up to a total of 10 mg.")
33
Codeina PHARMACODYNAMICS / KINETICS
Onset of action: Oral: hour; I.M.: minutes Peak effect: Oral: hours; I.M.: hour Duration: 4-6 hours Absorption: Oral: Adequate Las propiedades farmacocinéticas de la codeína le confieren una aceptable biodisponibilidad oral (50%), lo que permite su administración (casi exclusiva) por esta vía. Distribution: Crosses placenta; enters breast milk Protein binding: 7% Metabolism: Hepatic to morphine (active) 10% de codeina se metaboliza a morfina. Half-life elimination: hours. Su baja semivida de eliminación obliga a la administración cada 4-6 h, lo que ha llevado a la comercialización de algunos derivados, como la dihidrocodeína, en forma de preparados de liberación sostenida, especialmente indicadas en situaciones de dolor crónico Excretion: Urine (3% to 16% as unchanged drug, norcodeine, and free and conjugated morphine)
, lo que permite su administración (casi exclusiva) por esta vía. Distribution: Crosses placenta; enters breast milk. Protein binding: 7% Metabolism: Hepatic to morphine (active) 10% de codeina se metaboliza a morfina. Half-life elimination: hours. Su baja semivida de eliminación obliga a la administración cada 4-6 h, lo que ha llevado a la comercialización de algunos derivados, como la dihidrocodeína, en forma de preparados de liberación sostenida, especialmente indicadas en situaciones de dolor crónico. Excretion: Urine (3% to 16% as unchanged drug, norcodeine, and free and conjugated morphine)")
34
Dihidrocodeína (Hidrocodona) Comp 60 mg Contugesic
N02A-Analgésicos narcóticos (Opioides) NOMBRE GENÉRICO PRESENTACIÓN VIA NOMBRE COMERCIAL Buprenorfina Comp 0,2 mg Amp 0,3 mg/1 ml SL IM, IV Buprex CE Codeína Comp 28 mg OR Codeisan Dihidrocodeína (Hidrocodona) Comp 60 mg Contugesic Fentanilo (2) Parche 2,5 mg (3) Parche 5 mg (3) Parche 10 mg (3) TOP Durogesic 25 Durogesic 50 Durogesic 100 Metadona Amp 10 mg/1 ml Comp 5 mg Comp 40 mg SC, IM Metasedin CE Morfina cloruro (sin conservantes) Vial 400 mg/20 ml (vial multidosis, sin conservantes) Amp 10 ml. SC, IV, IM SC IV, IM Cloruro Mórfico Braun 1 % CE Morfina Braun 2 % s/c CE Morfina Braun 4 % s/c CE Morfina clorhidrato Jbe 10 mg/ml Brompton FM CE Morfina sulfato Comp 10 mg Comp 20 mg Sevredol CE (1) Morfina sulfato retard Comp 30 mg Comp 100 mg MST Continus CE Petidina (Meperidina) Amp 100 mg/2 ml SC, IM, IV Dolantina CE Tramadol Caps 50 mg Comp retard 200 mg Comp retard 300 mg Amp 100 mg/2 m Adolonta, Tralgiol Zytram CE: Control de estupefacientes. Nota 1: Comprimidos ranurados. Nota 2: Uso restringido para tratamiento del dolor crónico. Nota 3: Los parches de 2,5, 5 y 10 mg liberan respectivamente 25, 50 y 100 mcg/h durante 72 h.
 NOMBRE GENÉRICO. PRESENTACIÓN. VIA. NOMBRE COMERCIAL. Buprenorfina. Comp 0,2 mg. Amp 0,3 mg/1 ml. SL. IM, IV. Buprex CE. Codeína. Comp 28 mg. OR. Codeisan. Dihidrocodeína (Hidrocodona) Comp 60 mg. Contugesic. Fentanilo (2) Parche 2,5 mg (3) Parche 5 mg (3) Parche 10 mg (3) TOP. Durogesic 25. Durogesic 50. Durogesic 100. Metadona. Amp 10 mg/1 ml. Comp 5 mg. Comp 40 mg. SC, IM. Metasedin CE. Morfina cloruro. (sin conservantes) Vial 400 mg/20 ml. (vial multidosis, sin conservantes) Amp 10 ml. SC, IV, IM. SC. IV, IM. Cloruro Mórfico Braun 1 % CE. Morfina Braun 2 % s/c CE. Morfina Braun 4 % s/c CE. Morfina clorhidrato. Jbe 10 mg/ml. Brompton FM CE. Morfina sulfato. Comp 10 mg. Comp 20 mg. Sevredol CE (1) Morfina sulfato retard. Comp 30 mg. Comp 100 mg. MST Continus CE. Petidina (Meperidina) Amp 100 mg/2 ml. SC, IM, IV. Dolantina CE. Tramadol. Caps 50 mg. Comp retard 200 mg. Comp retard 300 mg. Amp 100 mg/2 m. Adolonta, Tralgiol. Zytram. CE: Control de estupefacientes. Nota 1: Comprimidos ranurados. Nota 2: Uso restringido para tratamiento del dolor crónico. Nota 3: Los parches de 2,5, 5 y 10 mg liberan respectivamente 25, 50 y 100 mcg/h durante 72 h.")
36
Tramadol Análogo sintético de codeina.
Analgésico no narcótico de acción periférico y central.

37
Tramadol Mecanismo de acción:
Inhibición de la recaptación de NA y serotonina por las celulas nerviosas. Actúa sobre los receptores opioides Mu.

38
N02A-Analgésicos narcóticos (Opioides)
NOMBRE GENÉRICO PRESENTACIÓN VIA NOMBRE COMERCIAL Tramadol Caps 50 mg Comp retard 200 mg Comp retard 300 mg Amp 100 mg/2 ml OR SC, IM, IV Adolonta, Tralgiol Zytram

39
Tramadol PRESENTACIONES: ADMINISTRACION: SUEROS COMPATIBLES: SF, SG5%.
Adolonta amp de 100 mg en 2 ml Tralgiol amp de 100 mg en 2 ml ADMINISTRACION: INYECCION IV DIRECTA: SI Administrar lentamente. INFUSION INTERMITENTE: SI Diluir la dosis prescrita en ml de SF o SG5%. Administrar en minutos. INFUSION CONTINUA: SI Diluir la dosis prescrita, ejemplo 2 amp en 500 ml de SF o SG5%. El ritmo de infusión adecuado es de gotas/min ó ml/h que equivalen a mg/h de Tramadol. INYECCION IM: SI INYECCION SUBCUTANEA: SI SUEROS COMPATIBLES: SF, SG5%. OBSERVACIONES: La dosificacion máxima diaria en adultos por cualquier vía es de 400 mg/día. También se dispone de estudios de administración vía epidural.

40
Tramadol DOSING: ADULTS — Moderate-to-severe chronic pain: Oral:
Caps 50 mg mg every 4-6 hours (not to exceed 400 mg/day) For patients not requiring rapid onset of effect, tolerability may be improved by starting dose at 25 mg/day and titrating dose by 25 mg every 3 days, until reaching 25 mg 4 times/day. Dose may then be increased by 50 mg every 3 days as tolerated, to reach dose of 50 mg 4 times/day. Comp retard 200 mg. Comp retard 300 mg 100 mg once daily; titrate every 5 days (maximum: 300 mg/day)
 For patients not requiring rapid onset of effect, tolerability may be improved by starting dose at 25 mg/day and titrating dose by 25 mg every 3 days, until reaching 25 mg 4 times/day. Dose may then be increased by 50 mg every 3 days as tolerated, to reach dose of 50 mg 4 times/day. Comp retard 200 mg. Comp retard 300 mg. 100 mg once daily; titrate every 5 days (maximum: 300 mg/day)")
41
Tramadol DOSING: ELDERLY — Oral: >75 years: Caps 50 mg
50 mg every 6 hours (not to exceed 300 mg/day Comp retard 200 mg. Comp retard 300 mg 100 mg once daily; titrate every 5 days (maximum: 300 mg/day). Use with great caution.
. Use with great caution.")
42
Tramadol DOSING: RENAL IMPAIRMENT DOSING: HEPATIC IMPAIRMENT
Clcr <30 mL/minute: mg dose every 12 hours (maximum: 200 mg/day). Should not be used in patients with Clcr < 30 mL/minute. DOSING: HEPATIC IMPAIRMENT Cirrhosis: Recommended dose: 50 mg every 12 hours. Should not be used in patients with severe (Child-Pugh Class C) hepatic dysfunction.
. Should not be used in patients with Clcr < 30 mL/minute. DOSING: HEPATIC IMPAIRMENT. Cirrhosis: Recommended dose: 50 mg every 12 hours. Should not be used in patients with severe (Child-Pugh Class C) hepatic dysfunction.")
44
Tramadol Efectos secundarios: >10%: Cardiovascular: Flushing (8% to 16%) Central nervous system: mareos (16% to 33%), headache (8% to 32%), insomnia (7% to 11%), somnolence (7% to 25%) Dermatologic: Pruritus (6% to 12%) Gastrointestinal: Constipation (12% to 46%), nausea (15% to 40%) Neuromuscular & skeletal: Weakness (4% to 12%)
 Central nervous system: mareos (16% to 33%), headache (8% to 32%), insomnia (7% to 11%), somnolence (7% to 25%) Dermatologic: Pruritus (6% to 12%) Gastrointestinal: Constipation (12% to 46%), nausea (15% to 40%) Neuromuscular & skeletal: Weakness (4% to 12%)")
45
Tramadol Efectos secundarios: 1% to 10%: Cardiovascular: Chest pain (1% to <5%), postural hypotension (2% to 5%), vasodilation (1% to <5%) Central nervous system: Agitation, anxiety (1% to <5%), confusion (1% to <5%), coordination impaired (1% to <5%), depression (1% to <5%), emotional lability, euphoria, hallucinations, hypoesthesia, lethargy, malaise, nervousness (1% to <5%), pain, pyrexia, restlessness Dermatologic: Dermatitis, rash Endocrine & metabolic: Hot flashes (2% to 9%), menopausal symptoms (1% to <5%) Gastrointestinal: Abdominal pain, anorexia (<6%), diarrhea (5% to 10%), dry mouth (5% to 10%), dyspepsia, flatulence, vomiting (5% to 9%), weight loss Genitourinary: Urinary frequency (1% to <5%), urinary retention (1% to <5%), urinary tract infection (1% to <5%) Neuromuscular & skeletal: Arthralgia (1% to <5%), hypertonia (1% to <5%), rigors (<4%), paresthesia (1% to <5%), spasticity (1% to <5%), tremor (1% to <5%), creatinine phosphokinase increased Ocular: Blurred vision (1% to <5%), miosis (1% to <5%) Respiratory: Bronchitis (1% to <5%), cough (1% to <5%), dyspnea (1% to <5%), pharyngitis (1% to <5%), rhinorrhea (1% to <5%), sinusitis (1% to <5%) Miscellaneous: Diaphoresis (2% to 6%), flu-like syndrome (<2%)
, postural hypotension (2% to 5%), vasodilation (1% to <5%) Central nervous system: Agitation, anxiety (1% to <5%), confusion (1% to <5%), coordination impaired (1% to <5%), depression (1% to <5%), emotional lability, euphoria, hallucinations, hypoesthesia, lethargy, malaise, nervousness (1% to <5%), pain, pyrexia, restlessness Dermatologic: Dermatitis, rash Endocrine & metabolic: Hot flashes (2% to 9%), menopausal symptoms (1% to <5%) Gastrointestinal: Abdominal pain, anorexia (<6%), diarrhea (5% to 10%), dry mouth (5% to 10%), dyspepsia, flatulence, vomiting (5% to 9%), weight loss Genitourinary: Urinary frequency (1% to <5%), urinary retention (1% to <5%), urinary tract infection (1% to <5%) Neuromuscular & skeletal: Arthralgia (1% to <5%), hypertonia (1% to <5%), rigors (<4%), paresthesia (1% to <5%), spasticity (1% to <5%), tremor (1% to <5%), creatinine phosphokinase increased Ocular: Blurred vision (1% to <5%), miosis (1% to <5%) Respiratory: Bronchitis (1% to <5%), cough (1% to <5%), dyspnea (1% to <5%), pharyngitis (1% to <5%), rhinorrhea (1% to <5%), sinusitis (1% to <5%) Miscellaneous: Diaphoresis (2% to 6%), flu-like syndrome (<2%)")
46
Tramadol El tramadol presenta una baja o nula capacidad para causar cuadros de farmacodependencia. Epileptógeno en situaciones con disminución del umbral de epilepsia (uremia, tumores cerebrales)
")
47
Tramadol DRUG INTERACTIONS — Substrate of CYP2B6 (minor), 2D6 (major), 3A4 (minor) Carbamazepine: Tramadol metabolism is increased by carbamazepine. Avoid concurrent use; increases risk of seizures. Cyclobenzaprine: May enhance the neuroexcitatory and/or seizure-potentiating effect of tramadol. CYP2D6 inhibitors: May decrease the effects of tramadol. Example inhibitors include chlorpromazine, delavirdine, fluoxetine, miconazole, paroxetine, pergolide, quinidine, quinine, ritonavir, and ropinirole. Ethanol: Tramadol may enhance the CNS depressant effect of ethanol. MAO inhibitors: May increase the neuroexcitatory effects or risk of seizures. Examples of inhibitors include isocarboxazid, linezolid, phenelzine, selegiline, and tranylcypromine. Naloxone: May increase the risk of seizures (if administered in tramadol overdose). Quinidine: May increase the tramadol serum concentrations and decrease serum concentrations of M1 SSRIs: May increase the neuroexcitatory effects or risk of seizures with tramadol. Examples of SSRIs include citalopram, escitalopram, fluoxetine, fluvoxamine, paroxetine, sertraline. Serotonin modulators: May enhance the adverse/toxic effects of tramadol. The development of serotonin syndrome may occur. Sibutramine: May enhance the serotonergic effects of tramadol. Avoid concurrent use. Tricyclic antidepressants: May increase the risk of seizures.
. Quinidine: May increase the tramadol serum concentrations and decrease serum concentrations of M1. SSRIs: May increase the neuroexcitatory effects or risk of seizures with tramadol. Examples of SSRIs include citalopram, escitalopram, fluoxetine, fluvoxamine, paroxetine, sertraline. Serotonin modulators: May enhance the adverse/toxic effects of tramadol. The development of serotonin syndrome may occur. Sibutramine: May enhance the serotonergic effects of tramadol. Avoid concurrent use. Tricyclic antidepressants: May increase the risk of seizures.")
48
Tramadol Embarazo y lactancia. Contraindicado. Atraviesa la placenta.
Aparece en la leche materna.

49
Tramadol Rango terapéutico: ng/mL

50
Tramadol Sobredosis: Clínica: Depresión del SNC, depresion respiratoria, letargia, coma, miosis, convulsiones, fallo cardíaco y muerte. Tratamiento sintomático. La administración de naloxona no revierte completamente los efectos del tramadol, y puede aumentar el riesgo de convulsiones. No se elimina mediante Hemodiálisis.

51
Tramadol Farmacocinética:
Inicio de acción en 1 horas. Duración de acción 9 horas. Absorción oral rápida y completa. VD 2,5-3 l/kg. Unión aproteinas plasmáticas: 20%. Metabolismo: Hepatico (demethylation, glucuronidation, and sulfation) Metabolito activo (O-desmethyl tramadol) Vida media de eliminación: Prolongada en ancianos, daño hepático y renal (en esta última X2). Tramadol: 6-8 horas.(obliga a su administración varias veces al día). O-desmethyl tramadol: 7-9 horas. Excreccion: Urinaria (30% como fármaco; 60% como metabolito)
 Metabolito activo (O-desmethyl tramadol) Vida media de eliminación: Prolongada en ancianos, daño hepático y renal (en esta última X2). Tramadol: 6-8 horas.(obliga a su administración varias veces al día). O-desmethyl tramadol: 7-9 horas. Excreccion: Urinaria (30% como fármaco; 60% como metabolito)")
52
Should not be used in patients with Clcr < 30 mL/minute.
Dosis de carga Dosis de mantenimiento FG > 50 ml/min FG ml/min FG < 10 ml/min Dosis suplemtaria tras HD DPCA TSCR Tramadol Clcr <30 mL/minute: mg dose every 12 hours (maximum: 200 mg/day). Should not be used in patients with Clcr < 30 mL/minute.
. Should not be used in patients with Clcr < 30 mL/minute.")
54
Oxicodona Agonista puro.
Se comercializa como medicamento de liberación controlada (OxyContin) o de liberación rápida (OxyIR, OxyNorm). El OxyContin se presenta en comprimidos de 10, 20, 40 y 80 mg, y debido a su mecanismo de liberación lenta, es efectivo durante unas doce horas. Oxynorm caps. 5, 10 y 20 mg OXYNORM Concentrado 10 mg/ml solución oral OXYNORM Líquido 1 mg/ 1 ml sol.oral
 o de liberación rápida (OxyIR, OxyNorm). El OxyContin se presenta en comprimidos de 10, 20, 40 y 80 mg, y debido a su mecanismo de liberación lenta, es efectivo durante unas doce horas. Oxynorm caps. 5, 10 y 20 mg. OXYNORM Concentrado 10 mg/ml solución oral. OXYNORM Líquido 1 mg/ 1 ml sol.oral.")
55
Oxicodona DOSING: ADULTS — Management of pain: Oral:
Regular or immediate release formulations: mg every 6 hours Controlled release: Opioid naive (not currently on opioid): 10 mg every 12 hours Currently on opioid/ASA or acetaminophen or NSAID combination: 1-5 tablets: mg every 12 hours 6-9 tablets: mg every 12 hours 10-12 tablets: mg every 12 hours May continue the nonopioid as a separate drug. Currently on opioids: Use standard conversion chart to convert daily dose to oxycodone equivalent. Divide daily dose in 2 (for every 12-hour dosing) and round down to nearest dosage form. Note: 80 mg or 160 mg tablets are for use only in opioid-tolerant patients. Special safety considerations must be addressed when converting to OxyContin® doses 160 mg every 12 hours. Dietary caution must be taken when patients are initially titrated to 160 mg tablets.
: 10 mg every 12 hours Currently on opioid/ASA or acetaminophen or NSAID combination: 1-5 tablets: mg every 12 hours 6-9 tablets: mg every 12 hours tablets: mg every 12 hours May continue the nonopioid as a separate drug. Currently on opioids: Use standard conversion chart to convert daily dose to oxycodone equivalent. Divide daily dose in 2 (for every 12-hour dosing) and round down to nearest dosage form. Note: 80 mg or 160 mg tablets are for use only in opioid-tolerant patients. Special safety considerations must be addressed when converting to OxyContin® doses 160 mg every 12 hours. Dietary caution must be taken when patients are initially titrated to 160 mg tablets.")
56
Oxicodona DOSING: PEDIATRIC — Oral: Regular or immediate release formulations: 6-12 years: 1.25 mg every 6 hours as needed >12 years: 2.5 mg every 6 hours as needed

57
Oxicodona DOSING: HEPATIC IMPAIRMENT — Reduce dosage in patients with severe liver disease. DOSING: RENAL IMPAIRMENT – Se prolonga la vida media de eliminación. Relacionado con casos de GNF fibrilar

58
Oxicodona ADVERSE REACTIONS SIGNIFICANT >10%: Central nervous system: Fatigue, drowsiness, dizziness, somnolence Dermatologic: Pruritus Gastrointestinal: Nausea, vomiting, constipation Neuromuscular & skeletal: Weakness 1% to 10%: Cardiovascular: Postural hypotension Central nervous system: Nervousness, headache, restlessness, malaise, confusion, anxiety, abnormal dreams, euphoria, thought abnormalities Dermatologic: Rash Gastrointestinal: Anorexia, stomach cramps, xerostomia, biliary spasm, abdominal pain, dyspepsia, gastritis Genitourinary: Ureteral spasms, decreased urination Local: Pain at injection site Respiratory: Dyspnea, hiccups Miscellaneous: Diaphoresis <1% (Limited to important or life-threatening): Anaphylaxis, anaphylactoid reaction, dysphagia, exfoliative dermatitis, hallucinations, histamine release, hyponatremia, ileus, intracranial pressure increased, mental depression, paradoxical CNS stimulation, paralytic ileus, physical and psychological dependence, SIADH, syncope, urinary retention, urticaria, vasodilation, withdrawal syndrome (may include seizure) Note: Deaths due to overdose have been reported due to misuse/abuse after crushing the sustained release tablets.
: Anaphylaxis, anaphylactoid reaction, dysphagia, exfoliative dermatitis, hallucinations, histamine release, hyponatremia, ileus, intracranial pressure increased, mental depression, paradoxical CNS stimulation, paralytic ileus, physical and psychological dependence, SIADH, syncope, urinary retention, urticaria, vasodilation, withdrawal syndrome (may include seizure) Note: Deaths due to overdose have been reported due to misuse/abuse after crushing the sustained release tablets.")
59
Oxicodona CONTRAINDICATIONS —
Hypersensitivity to oxycodone or any component of the formulation; Significant respiratory depression; hypercarbia; acute or severe bronchial asthma; OxyContin® is also contraindicated in paralytic ileus (known or suspected); pregnancy (prolonged use or high doses at term)
; pregnancy (prolonged use or high doses at term)")
60
Oxicodona Use with caution in the elderly, debilitated, severe hepatic or renal function. Hemodynamic effects (hypotension, orthostasis) may be exaggerated in patients with hypovolemia, concurrent vasodilating drugs, or in patients with head injury. Respiratory depressant effects and capacity to elevate CSF pressure may be exaggerated in presence of head injury, other intracranial lesion, or pre-existing intracranial pressure. Some preparations contain sulfites which may cause allergic reactions.
 may be exaggerated in patients with hypovolemia, concurrent vasodilating drugs, or in patients with head injury. Respiratory depressant effects and capacity to elevate CSF pressure may be exaggerated in presence of head injury, other intracranial lesion, or pre-existing intracranial pressure. Some preparations contain sulfites which may cause allergic reactions.")
61
Oxicodona DRUG INTERACTIONS — Substrate of CYP2D6 (major)
CNS depressants, MAO inhibitors, general anesthetics, and tricyclic antidepressants: May potentiate the effects of opiate agonists; dextroamphetamine may enhance the analgesic effect of opiate agonists CYP2D6 inhibitors: May decrease the effects of oxycodone. Example inhibitors include chlorpromazine, delavirdine, fluoxetine, miconazole, paroxetine, pergolide, quinidine, quinine, ritonavir, and ropinirole.

62
Oxicodona Embarazo: Lactancia: Contraindicado.
Pasa a la leche materna. Usar con precaución.

63
Oxicodona PHARMACODYNAMICS / KINETICS Onset of action: 10-15 minutes.
Peak effect: hour Duration: 3-6 hours; Controlled release: 12 hours Metabolism: Hepatic (noroxycodona y oxymorfona) Half-life elimination: 2-3 hours Excretion: Urine (10% como fármaco)
 Half-life elimination: 2-3 hours. Excretion: Urine (10% como fármaco)")
64
Oxicodona Dosis de carga Dosis de mantenimiento FG > 50 ml/min
Dosis suplemtaria tras HD DPCA TSCR Oxicodona

66
Actiq®: 200 mcg, 400 mcg, 600 mcg, 800 mcg, 1200 mcg, 1600 mcg
N02A-Analgésicos narcóticos (Opioides) NOMBRE GENÉRICO PRESENTACIÓN VIA NOMBRE COMERCIAL Fentanilo (2) Parche 2,5 mg (3) Parche 5 mg (3) Parche 10 mg (3) TOP Durogesic 25 Durogesic 50 Durogesic 100 Actiq®: 200 mcg, 400 mcg, 600 mcg, 800 mcg, 1200 mcg, 1600 mcg CE: Control de estupefacientes. Nota 2: Uso restringido para tratamiento del dolor crónico. Nota 3: Los parches de 2,5, 5 y 10 mg liberan respectivamente 25, 50 y 100 mcg/h durante 72 h.
 NOMBRE GENÉRICO. PRESENTACIÓN. VIA. NOMBRE COMERCIAL. Fentanilo (2) Parche 2,5 mg (3) Parche 5 mg (3) Parche 10 mg (3) TOP. Durogesic 25. Durogesic 50. Durogesic 100. Actiq®: 200 mcg, 400 mcg, 600 mcg, 800 mcg, 1200 mcg, 1600 mcg. CE: Control de estupefacientes. Nota 2: Uso restringido para tratamiento del dolor crónico. Nota 3: Los parches de 2,5, 5 y 10 mg liberan respectivamente 25, 50 y 100 mcg/h durante 72 h.")
67
Fentanilo Mecanismo de acción: Agonistas de los tres receptores opioides. Se caracteriza por su elevada potencia farmacológica, muy por encima de la morfina, su elevada liposolubilidad, y su escasa biodisponibilidad tras la administración oral. Inidicaciones: Parche transdérmico (Duragesic®): Tratamiento del dolor crónico moderado o severo. Transmucosal (Actiq®): Tratamiento del dolor irruptivo. (evita el primer paso hepático)
: Tratamiento del dolor crónico moderado o severo. Transmucosal (Actiq®): Tratamiento del dolor irruptivo. (evita el primer paso hepático)")
68
Fentanilo Chronic pain management:
Dosis inicial 25 mcg/h si el paciente no toma morfina o toma menos de 90 mg/dia.

69
Fentanilo Dose conversion guidelines for transdermal fentanyl 1.
Recommended Initial Duragesic® Dose Based Upon Daily Oral Morphine Dose1 mg morphine oral/day = 25 mcg/hour Duragesic® mg morphine oral/day = 50 mcg/hour Duragesic® mg morphine oral/day = 75 mcg/hour Duragesic® mg morphine oral/day = 100 mcg/hour Duragesic® mg morphine oral/day = 125 mcg/hour Duragesic® mg morphine oral/day = 150 mcg/hour Duragesic® mg morphine oral/day = 175 mcg/hour Duragesic® mg morphine oral/day = 200 mcg/hour Duragesic® mg morphine oral/day = 225 mcg/hour Duragesic® mg morphine oral/day = 250 mcg/hour Duragesic® mg morphine oral/day = 275 mcg/hour Duragesic® mg morphine oral/day = 300 mcg/hour Duragesic®

70
Dosing Conversion Guidelines1,2
Morphine (I.M./I.V.): 10-22 mg/day: recommended fentanyl transdermal dose: 25 mcg/hour 23-37 mg/day: recommended fentanyl transdermal dose: 50 mcg/hour 38-52 mg/day: recommended fentanyl transdermal dose: 75 mcg/hour 53-67 mg/day: recommended fentanyl transdermal dose: 100 mcg/hour Oxycodone (oral): 30-67 mg/day: recommended fentanyl transdermal dose: 25 mcg/hour mg/day: recommended fentanyl transdermal dose: 50 mcg/hour mg/day: recommended fentanyl transdermal dose: 75 mcg/hour mg/day: recommended fentanyl transdermal dose: 100 mcg/hour Oxycodone (I.M./I.V.): 15-33 mg/day: recommended fentanyl transdermal dose: 25 mcg/hour mg/day: recommended fentanyl transdermal dose: 50 mcg/hour mg/day: recommended fentanyl transdermal dose: 75 mcg/hour mg/day: recommended fentanyl transdermal dose: 100 mcg/hour Codeine (oral): mg/day: recommended fentanyl transdermal dose: 25 mcg/hour mg/day: recommended fentanyl transdermal dose: 50 mcg/hour mg/day: recommended fentanyl transdermal dose: 75 mcg/hour mg/day: recommended fentanyl transdermal dose: 100 mcg/hour
: mg/day: recommended fentanyl transdermal dose: 25 mcg/hour mg/day: recommended fentanyl transdermal dose: 50 mcg/hour mg/day: recommended fentanyl transdermal dose: 75 mcg/hour mg/day: recommended fentanyl transdermal dose: 100 mcg/hour. Oxycodone (oral): mg/day: recommended fentanyl transdermal dose: 25 mcg/hour mg/day: recommended fentanyl transdermal dose: 50 mcg/hour mg/day: recommended fentanyl transdermal dose: 75 mcg/hour mg/day: recommended fentanyl transdermal dose: 100 mcg/hour. Oxycodone (I.M./I.V.): mg/day: recommended fentanyl transdermal dose: 25 mcg/hour mg/day: recommended fentanyl transdermal dose: 50 mcg/hour mg/day: recommended fentanyl transdermal dose: 75 mcg/hour mg/day: recommended fentanyl transdermal dose: 100 mcg/hour. Codeine (oral): mg/day: recommended fentanyl transdermal dose: 25 mcg/hour mg/day: recommended fentanyl transdermal dose: 50 mcg/hour mg/day: recommended fentanyl transdermal dose: 75 mcg/hour mg/day: recommended fentanyl transdermal dose: 100 mcg/hour.")
71
Dosing Conversion Guidelines1,2
Hydromorphone (oral): 8-17 mg/day: recommended fentanyl transdermal dose: 25 mcg/hour mg/day: recommended fentanyl transdermal dose: 50 mcg/hour mg/day: recommended fentanyl transdermal dose: 75 mcg/hour mg/day: recommended fentanyl transdermal dose: 100 mcg/hour Hydromorphone (I.M./I.V.): mg/day: recommended fentanyl transdermal dose: 25 mcg/hour mg/day: recommended fentanyl transdermal dose: 50 mcg/hour mg/day: recommended fentanyl transdermal dose: 75 mcg/hour 8-10 mg/day: recommended fentanyl transdermal dose: 100 mcg/hour Meperidine (I.M.): mg/day: recommended fentanyl transdermal dose: 25 mcg/hour mg/day: recommended fentanyl transdermal dose: 50 mcg/hour mg/day: recommended fentanyl transdermal dose: 75 mcg/hour mg/day: recommended fentanyl transdermal dose: 100 mcg/hour
: 8-17 mg/day: recommended fentanyl transdermal dose: 25 mcg/hour mg/day: recommended fentanyl transdermal dose: 50 mcg/hour mg/day: recommended fentanyl transdermal dose: 75 mcg/hour mg/day: recommended fentanyl transdermal dose: 100 mcg/hour. Hydromorphone (I.M./I.V.): mg/day: recommended fentanyl transdermal dose: 25 mcg/hour mg/day: recommended fentanyl transdermal dose: 50 mcg/hour mg/day: recommended fentanyl transdermal dose: 75 mcg/hour 8-10 mg/day: recommended fentanyl transdermal dose: 100 mcg/hour. Meperidine (I.M.): mg/day: recommended fentanyl transdermal dose: 25 mcg/hour mg/day: recommended fentanyl transdermal dose: 50 mcg/hour mg/day: recommended fentanyl transdermal dose: 75 mcg/hour mg/day: recommended fentanyl transdermal dose: 100 mcg/hour.")
72
Dosing Conversion Guidelines1,2
Methadone (oral): 20-44 mg/day: recommended fentanyl transdermal dose: 25 mcg/hour 45-74 mg/day: recommended fentanyl transdermal dose: 50 mcg/hour mg/day: recommended fentanyl transdermal dose: 75 mcg/hour mg/day: recommended fentanyl transdermal dose: 100 mcg/hour Methadone (I.M.): 10-22 mg/day: recommended fentanyl transdermal dose: 25 mcg/hour 23-37 mg/day: recommended fentanyl transdermal dose: 50 mcg/hour 38-52 mg/day: recommended fentanyl transdermal dose: 75 mcg/hour 53-67 mg/day: recommended fentanyl transdermal dose: 100 mcg/hour 1The table should NOT be used to convert from transdermal fentanyl (eg, Duragesic®) to other opioid analgesics. Rather, following removal of the patch, titrate the dose of the new opioid until adequate analgesia is achieved.
: mg/day: recommended fentanyl transdermal dose: 25 mcg/hour mg/day: recommended fentanyl transdermal dose: 50 mcg/hour mg/day: recommended fentanyl transdermal dose: 75 mcg/hour mg/day: recommended fentanyl transdermal dose: 100 mcg/hour. Methadone (I.M.): mg/day: recommended fentanyl transdermal dose: 25 mcg/hour mg/day: recommended fentanyl transdermal dose: 50 mcg/hour mg/day: recommended fentanyl transdermal dose: 75 mcg/hour mg/day: recommended fentanyl transdermal dose: 100 mcg/hour. 1The table should NOT be used to convert from transdermal fentanyl (eg, Duragesic®) to other opioid analgesics. Rather, following removal of the patch, titrate the dose of the new opioid until adequate analgesia is achieved.")
73
Fentanilo Breakthrough cancer pain: Transmucosal: Actiq® dosing should be individually titrated to provide adequate analgesia with minimal side effects. For patients who are tolerant to and currently receiving opioid therapy for persistent cancer pain. Initial starting dose: 200 mcg; the second dose may be started 15 minutes after completion of the first dose. Consumption should be limited to 4 units/day or less. Patients needing more than 4 units/day should have the dose of their long-term opioid re-evaluated.

74
Fentanilo DOSING: PEDIATRIC
Breakthrough cancer pain: Children 16 years: Transmucosal: Refer to adult dosing. Chronic pain management: Children 2 years (opioid-tolerant patients): Transdermal patch: Refer to adult dosing.
: Transdermal patch: Refer to adult dosing.")
75
Fentanilo DOSING: ELDERLY —
Elderly have been found to be twice as sensitive as younger patients to the effects of fentanyl. A wide range of doses may be used. When choosing a dose, take into consideration the following patient factors: age, weight, physical status, underlying disease states, other drugs used, type of anesthesia used, and the surgical procedure to be performed. Transmucosal: Dose should be reduced to mcg/kg. Suck on lozenge vigorously approximately minutes before the start of procedure.

76
Fentanilo Transdermal patch (eg, Duragesic®):
Apply to nonirritated and nonirradiated skin, such as chest, back, flank, or upper arm. Do not shave skin; hair at application site should be clipped. Prior to application, clean site with clear water and allow to dry completely. Do not use damaged or cut patches; a rapid release of fentanyl and increased systemic absorption may occur. Firmly press in place and hold for 30 seconds. Change patch every 72 hours. Do not use soap, alcohol, or other solvents to remove transdermal gel if it accidentally touches skin; use copious amounts of water. Avoid exposing application site to external heat sources (eg, heating pad, electric blanket, heat lamp, hot tub).
.")
77
Fentanilo Transmucosal:
Foil overwrap should be removed just prior to administration. Place the unit in mouth and allow it to dissolve. Do not chew. Actiq® units may be moved from one side of the mouth to the other. The unit should be consumed over a period of 15 minutes. Unit should be removed after it is consumed or if patient has achieved an adequate response and/or shows signs of respiratory depression. For patients who have received transmucosal product within 6-12 hours, it is recommended that if other narcotics are required, they should be used at starting doses 1/4 to 1/3 those usually recommended.

78
Fentanilo ADVERSE REACTIONS SIGNIFICANT >10%: Cardiovascular: Hypotension, bradycardia Central nervous system: CNS depression, confusion, drowsiness, sedation Gastrointestinal: Nausea, vomiting, constipation, xerostomia Local: Application-site reaction (iontophoretic system 14%) Neuromuscular & skeletal: Chest wall rigidity (high dose I.V.), weakness Ocular: Miosis Respiratory: Respiratory depression Miscellaneous: Diaphoresis
 Neuromuscular & skeletal: Chest wall rigidity (high dose I.V.), weakness Ocular: Miosis Respiratory: Respiratory depression Miscellaneous: Diaphoresis.")
79
Fentanilo ADVERSE REACTIONS SIGNIFICANT 1% to 10%: Cardiovascular: Cardiac arrhythmia, edema, orthostatic hypotension, hypertension, syncope, tachycardia Central nervous system: Abnormal dreams, abnormal thinking, agitation, amnesia, anxiety, dizziness, euphoria, fatigue, fever, hallucinations, headache, insomnia, nervousness, paranoid reaction Dermatologic: Erythema, papules, pruritus (iontophoretic system 6%), rash Gastrointestinal: Abdominal pain, anorexia, biliary tract spasm, diarrhea, dyspepsia, flatulence, ileus Genitourinary: Urinary retention (iontophoretic transdermal system 3%) Hematologic: Anemia Neuromuscular & skeletal: Abnormal coordination, abnormal gait, back pain, paresthesia, rigors, tremor Respiratory: Apnea, bronchitis, dyspnea, hemoptysis, hypoxia, pharyngitis, rhinitis, sinusitis, upper respiratory infection Miscellaneous: Hiccups, flu-like syndrome, speech disorder <1% (Limited to important or life-threatening): Amblyopia, anorgasmia, aphasia, bradycardia, bronchospasm, circulatory depression, CNS excitation or delirium, convulsions, dental caries (Actiq®), depersonalization, dysesthesia, ejaculatory difficulty, exfoliative dermatitis, gum line erosion (Actiq®), hyper-/hypotonia, laryngospasm, paradoxical dizziness, physical and psychological dependence with prolonged use, stertorous breathing, stupor, tachycardia, tooth loss (Actiq®), urinary tract spasm, urticaria, vertigo
, rash Gastrointestinal: Abdominal pain, anorexia, biliary tract spasm, diarrhea, dyspepsia, flatulence, ileus Genitourinary: Urinary retention (iontophoretic transdermal system 3%) Hematologic: Anemia Neuromuscular & skeletal: Abnormal coordination, abnormal gait, back pain, paresthesia, rigors, tremor Respiratory: Apnea, bronchitis, dyspnea, hemoptysis, hypoxia, pharyngitis, rhinitis, sinusitis, upper respiratory infection Miscellaneous: Hiccups, flu-like syndrome, speech disorder. <1% (Limited to important or life-threatening): Amblyopia, anorgasmia, aphasia, bradycardia, bronchospasm, circulatory depression, CNS excitation or delirium, convulsions, dental caries (Actiq®), depersonalization, dysesthesia, ejaculatory difficulty, exfoliative dermatitis, gum line erosion (Actiq®), hyper-/hypotonia, laryngospasm, paradoxical dizziness, physical and psychological dependence with prolonged use, stertorous breathing, stupor, tachycardia, tooth loss (Actiq®), urinary tract spasm, urticaria, vertigo.")
80
Fentanilo CONTRAINDICATIONS — Hypersensitivity to fentanyl or any component of the formulation; increased intracranial pressure; severe respiratory disease or depression including acute asthma (unless patient is mechanically ventilated); paralytic ileus; severe liver or renal insufficiency; pregnancy (prolonged use or high doses near term) Transmucosal lozenges (Actiq®) or transdermal patches (eg, Duragesic®) must not be used in patients who are not opioid tolerant. Patients are considered opioid-tolerant if they are taking at least 60 mg morphine/day, 30 mg oral oxycodone/day, 8 mg oral hydromorphone/day, 25 mcg transdermal fentanyl/hour, or an equivalent dose of another opioid for 1 week. Transdermal patches are not for use in acute pain, mild pain, intermittent pain, or postoperative pain management.
; paralytic ileus; severe liver or renal insufficiency; pregnancy (prolonged use or high doses near term) Transmucosal lozenges (Actiq®) or transdermal patches (eg, Duragesic®) must not be used in patients who are not opioid tolerant. Patients are considered opioid-tolerant if they are taking at least 60 mg morphine/day, 30 mg oral oxycodone/day, 8 mg oral hydromorphone/day, 25 mcg transdermal fentanyl/hour, or an equivalent dose of another opioid for 1 week. Transdermal patches are not for use in acute pain, mild pain, intermittent pain, or postoperative pain management.")
81
Fentanilo Transdermal patches (eg, Duragesic®):
Serious or life-threatening hypoventilation may occur, even in opioid-tolerant patients. Serum fentanyl concentrations may increase approximately one-third for patients with a body temperature of 40ºC secondary to a temperature-dependent increase in fentanyl release from the patch and increased skin permeability. Avoid exposure of application site to direct external heat sources. Patients who experience adverse reactions should be monitored for at least 24 hours after removal of the patch. Transdermal patch does not contain any metal-based compounds; the printed ink used to indicate strength on the outer surface of the patch does contain titanium dioxide but the amount is minimal; adverse events have not been reported while wearing during an MRI. Safety and efficacy of transdermal patch have been limited to children 2 years of age who are opioid tolerant.

82
Fentanilo Actiq®: For patients who have received transmucosal product within 6-12 hours, it is recommended that if other narcotics are required, they should be used at starting doses 1/4 to 1/3 those usually recommended. Actiq® preparations contain an amount of medication that can be fatal to children. Keep all units out of the reach of children and discard any open units properly. Patients and caregivers should be counseled on the dangers to children including the risk of exposure to partially-consumed units. Safety and efficacy have not been established in children <16 years of age.

83
Fentanilo DRUG INTERACTIONS — Substrate of CYP3A4 (major); Inhibits CYP3A4 (weak) Antipsychotic agents (phenothiazines): May enhance the hypotensive effect of analgesics (narcotic). CNS depressants: Increased sedation with CNS depressants.; CYP3A4 inhibitors: May increase the levels/effects of fentanyl. Potentially fatal respiratory depression may occur when a potent inhibitor is used in a patient receiving chronic fentanyl (eg, transdermal patch). Example inhibitors include azole antifungals, clarithromycin, diclofenac, doxycycline, erythromycin, imatinib, isoniazid, nefazodone, nicardipine, propofol, protease inhibitors, quinidine, telithromycin, and verapamil. MAO inhibitors: Not recommended to use Actiq® within 14 days. Severe and unpredictable potentiation by MAO inhibitors has been reported with opioid analgesics. Pegvisomant: Analgesics (narcotic) may diminish the therapeutic effect of pegvisomant. Protease inhibitors: May decrease the metabolism, via CYP isoenzymes, of fentanyl. Selective serotonin reuptake inhibitors (SSRIs): Analgesics (narcotic) may enhance the serotonergic effect of SSRIs. This may cause serotonin syndrome. Sibutramine: Fentanyl may enhance the serotonergic effect of sibutramine.
: May enhance the hypotensive effect of analgesics (narcotic). CNS depressants: Increased sedation with CNS depressants.; CYP3A4 inhibitors: May increase the levels/effects of fentanyl. Potentially fatal respiratory depression may occur when a potent inhibitor is used in a patient receiving chronic fentanyl (eg, transdermal patch). Example inhibitors include azole antifungals, clarithromycin, diclofenac, doxycycline, erythromycin, imatinib, isoniazid, nefazodone, nicardipine, propofol, protease inhibitors, quinidine, telithromycin, and verapamil. MAO inhibitors: Not recommended to use Actiq® within 14 days. Severe and unpredictable potentiation by MAO inhibitors has been reported with opioid analgesics. Pegvisomant: Analgesics (narcotic) may diminish the therapeutic effect of pegvisomant. Protease inhibitors: May decrease the metabolism, via CYP isoenzymes, of fentanyl. Selective serotonin reuptake inhibitors (SSRIs): Analgesics (narcotic) may enhance the serotonergic effect of SSRIs. This may cause serotonin syndrome. Sibutramine: Fentanyl may enhance the serotonergic effect of sibutramine.")
84
Fentanilo Embarazo: Su uso de forma crónica puede producir dependencia en el recien nacido. De forma aguda cruza la placenta pero se ha utilizado de forma segura durante el trabajo del parto. Lactancia: Pasa a la leche materna. No recomendado.

85
Fentanilo MONITORING PARAMETERS — Control de la función respiratoria y cardiovascular, Tensión arterial y frecuencia cardíaca. Transdermal patch: Monitorizar a las 24 horas de la aplicación del parche.

86
Fentanilo Sobredosis:
Síntomas: depresión del SNC, depresión respiratoria, miosis. Tratamiento: De soporte. Naloxone, 2 mg I.V. with repeat administration as necessary up to a total of 10 mg, can also be used to reverse toxic effects of the opiate. Los pacientes que presentan reacciones adversas durante el uso del parche transdérmico deben ser monitorizados durante 24 horas tras la retirada del parche.

87
Fentanilo Farmacocinética: Onset of action:
Transmucosal: 5-15 minutes Peak effect: Transmucosal: Analgesic: minutes Time to peak: Transdermal patch: hours Absorption: Transmucosal: Rapid, ~25% from the buccal mucosa; 75% swallowed with saliva and slowly absorbed from GI tract Actiq® contains 2 g sugar per unit. Distribution: Highly lipophilic, redistributes into muscle and fat Metabolism: Hepatic, primarily via CYP3A4 Bioavailability: Transmucosal: ~50% (range: 36% to 71%) Half-life elimination: 2-4 hours Transdermal patch: 17 hours (half-life is influenced by absorption rate) Transmucosal: 6.6 hours (range: 5-15 hours) Excretion: Urine (primarily as metabolites, 10% as unchanged drug)
 Half-life elimination: 2-4 hours Transdermal patch: 17 hours (half-life is influenced by absorption rate) Transmucosal: 6.6 hours (range: 5-15 hours) Excretion: Urine (primarily as metabolites, 10% as unchanged drug)")
88
Dosis de carga Dosis de mantenimiento FG > 50 ml/min FG ml/min FG < 10 ml/min Dosis suplemtaria tras HD DPCA TSCR Fentanilo 100% 75% 50% No aplicable Su aclaramiento se reduce en pacientes con ERC avanzada, pudiendo aparecer sedación prologada y depresion respiratoria en pacientes con ERC avanzada. (sobre todo en administración parenteral).
.")
90
Morfina Alcaloide de la Papaver somniferum.
Sigue constituyendo el analgésico más potente del que se dispone para tratar todo tipo de dolores agudos y muchos de los crónicos. Modelo de agonista puro de los receptores opioides. Actúa activando los tres receptores opioides.

91
N02A-Analgésicos narcóticos (Opioides)
NOMBRE GENÉRICO PRESENTACIÓN VIA NOMBRE COMERCIAL Morfina cloruro Amp 10 mg/1 ml (sin conservantes) Vial 400 mg/20 ml (vial multidosis, sin conservantes) Amp 10 ml. SC, IV, IM SC IV, IM Cloruro Mórfico Braun 1 % CE Morfina Braun 2 % s/c CE Morfina Braun 4 % s/c CE Morfina clorhidrato Jbe 10 mg/ml OR Brompton FM CE Morfina sulfato Comp 10 mg Comp 20 mg Sevredol CE (1) Morfina sulfato retard Comp 30 mg Comp 60 mg Comp 100 mg MST Continus CE CE: Control de estupefacientes. Nota 1: Comprimidos ranurados. Nota 2: Uso restringido para tratamiento del dolor crónico. Nota 3: Los parches de 2,5, 5 y 10 mg liberan respectivamente 25, 50 y 100 mcg/h durante 72 h.
 Vial 400 mg/20 ml. (vial multidosis, sin conservantes) Amp 10 ml. SC, IV, IM. SC. IV, IM. Cloruro Mórfico Braun 1 % CE. Morfina Braun 2 % s/c CE. Morfina Braun 4 % s/c CE. Morfina clorhidrato. Jbe 10 mg/ml. OR. Brompton FM CE. Morfina sulfato. Comp 10 mg. Comp 20 mg. Sevredol CE (1) Morfina sulfato retard. Comp 30 mg. Comp 60 mg. Comp 100 mg. MST Continus CE. CE: Control de estupefacientes. Nota 1: Comprimidos ranurados. Nota 2: Uso restringido para tratamiento del dolor crónico. Nota 3: Los parches de 2,5, 5 y 10 mg liberan respectivamente 25, 50 y 100 mcg/h durante 72 h.")
92
Morfina ADMINISTRACION: INYECCION IV DIRECTA: SI
Administrar la dosis precrita muy lentamente. Diluir la dosis en 4-5 ml de agua p.i. antes de administrar. La administración rápida aumenta el riesgo de aparición de efectos secundarios (depresión respiratoria, apnea, hipotensión). INFUSION INTERMITENTE: SI Diluir la dosis prescrita en ml de SF ó SG5%. INFUSION CONTINUA: SI Diluir la dosis prescrita en ml de SF ó SG5%. INYECCION IM: SI Esta vía es preferible sobre la vía subcutánea cuando deben administrarse dosis repetidas. Aunque la absorción es más irregular y la duración de acción menor que si se usa la vía sc. INYECCION SUBCUTANEA: SI La absorción es más lenta que por vía IM, pero la analgesia suele ser más constante y duradera. SUEROS COMPATIBLES: SF, SG5% OBSERVACIONES: El preparado sin conservante también se puede administrar via epidural e intratecal.
. INFUSION INTERMITENTE: SI. Diluir la dosis prescrita en ml de SF ó SG5%. INFUSION CONTINUA: SI. Diluir la dosis prescrita en ml de SF ó SG5%. INYECCION IM: SI. Esta vía es preferible sobre la vía subcutánea cuando deben administrarse dosis repetidas. Aunque la absorción es más irregular y la duración de acción menor que si se usa la vía sc. INYECCION SUBCUTANEA: SI. La absorción es más lenta que por vía IM, pero la analgesia suele ser más constante y duradera. SUEROS COMPATIBLES: SF, SG5% OBSERVACIONES: El preparado sin conservante también se puede administrar via epidural e intratecal.")
93
Morfina DOSING: ADULTS — Acute pain (moderate-to-severe):
Oral: Prompt release formulations: Opiate-naive: Initial: 10 mg every 3 to 4 hours as needed; patients with prior opiate exposure may require higher initial doses: usual dosage range: mg every 3-4 hours as needed I.M., SubQ:. Initial: Opiate-naive: 5-10 mg every 3-4 hours as needed; patients with prior opiate exposure may require higher initial doses; usual dosage range: 5-20 mg every 3-4 hours as needed Rectal: mg every 3-4 hours I.V.: Initial: Opiate-naive: mg every 3 to 4 hours; patients with prior opiate exposure may require higher initial doses. Note: Repeated doses (up to every 5 minutes if needed) in small increments (eg, 1-4 mg) may be preferred to larger and less frequent doses.
 in small increments (eg, 1-4 mg) may be preferred to larger and less frequent doses.")
95
Morfina DOSING: PEDIATRIC —
Acute pain (moderate-to-severe): Children >6 months and <50 kg: Oral (prompt release): mg/kg every 3-4 hours as needed I.M.: 0.1 mg/kg every 3-4 hours as needed I.V.: mg/kg every 3-4 hours as needed I.V. infusion: Range: mcg/kg/hour Sedation/analgesia for procedures: Adolescents >12 years: I.V.: 3-4 mg and repeat in 5 minutes if necessary
: Children >6 months and <50 kg: Oral (prompt release): mg/kg every 3-4 hours as needed I.M.: 0.1 mg/kg every 3-4 hours as needed I.V.: mg/kg every 3-4 hours as needed I.V. infusion: Range: mcg/kg/hour. Sedation/analgesia for procedures: Adolescents >12 years: I.V.: 3-4 mg and repeat in 5 minutes if necessary.")
96
Morfina DOSING: ELDERLY — Refer to adult dosing. Use with caution; may require reduced dosage in the elderly and debilitated patients. DOSING: RENAL IMPAIRMENT Clcr mL/minute: Administer 75% of normal dose. Clcr <10 mL/minute: Administer 50% of normal dose. DOSING: HEPATIC IMPAIRMENT — Unchanged in mild liver disease; substantial extrahepatic metabolism may occur. Excessive sedation may occur in cirrhosis.

97
Morfina ADVERSE REACTIONS SIGNIFICANT —
>10%: Cardiovascular: Palpitations, hypotension, bradycardia Central nervous system: Somnolencia (48%, tolerance usually develops to drowsiness with regular dosing for 1-2 weeks); mareos (20%), confusion, headache (following epidural or intrathecal use) Dermatologic: Pruritus (may be secondary to histamine release) Note: Pruritus may be dose-related, but not confined to the site of administration. Gastrointestinal: Nausea (28%, tolerance usually develops to nausea and vomiting with chronic use); constipation (40%, tolerance develops very slowly if at all); xerostomia (78%) Genitourinary: Urinary retention (16%; may be prolonged, up to 20 hours, following epidural or intrathecal use) Local: Pain at injection site Neuromuscular & skeletal: Weakness Miscellaneous: Histamine release
; mareos (20%), confusion, headache (following epidural or intrathecal use) Dermatologic: Pruritus (may be secondary to histamine release) Note: Pruritus may be dose-related, but not confined to the site of administration. Gastrointestinal: Nausea (28%, tolerance usually develops to nausea and vomiting with chronic use); constipation (40%, tolerance develops very slowly if at all); xerostomia (78%) Genitourinary: Urinary retention (16%; may be prolonged, up to 20 hours, following epidural or intrathecal use) Local: Pain at injection site Neuromuscular & skeletal: Weakness Miscellaneous: Histamine release.")
98
Morfina DRUG INTERACTIONS — Substrate of CYP2D6 (minor)
Antipsychotic agents: May increase hypotensive effects of morphine; monitor. CNS depressants: May increase the effects/toxicity of morphine; monitor. MAO inhibitors: May increase the effects/toxicity of morphine; some manufacturers recommend avoiding use within 14 days of MAO inhibitors Pegvisomant: Therapeutic efficacy may be decreased by concomitant opiates, possibly requiring dosage adjustment of pegvisomant. Rifamycin derivatives: May decrease levels/effects of morphine; monitor. Selective serotonin reuptake inhibitors (SSRIs) and meperidine: Serotonergic effects may be additive, leading to serotonin syndrome.
 and meperidine: Serotonergic effects may be additive, leading to serotonin syndrome.")
99
Morfina PREGNANCY IMPLICATIONS — Morphine crosses the placenta. The frequency of congenital malformations has not been reported to be greater than expected in children from mothers treated with morphine during pregnancy. Reduced growth and behavioral abnormalities in offspring have been observed in animal studies. Neonates born to mothers receiving chronic opioids during pregnancy should be monitored for neonatal withdrawal syndrome. LACTATION — Enters breast milk

100
Morfina REFERENCE RANGE — TOXICOLOGY / OVERDOSE COMPREHENSIVE —
Therapeutic: Surgical anesthesia: ng/mL (SI: nmol/L); Toxic: ng/mL (SI: ,500 nmol/L) TOXICOLOGY / OVERDOSE COMPREHENSIVE — Symptoms include respiratory depression, miosis, hypotension, bradycardia, apnea, and pulmonary edema. Treatment includes airway support, establishment of an I.V. line, and administration of naloxone 2 mg I.V. (0.01 mg/kg for children), with repeat administration as necessary, up to a total of 10 mg. Primary attention should be directed to ensuring adequate respiratory exchange.
; Toxic: ng/mL (SI: ,500 nmol/L) TOXICOLOGY / OVERDOSE COMPREHENSIVE — Symptoms include respiratory depression, miosis, hypotension, bradycardia, apnea, and pulmonary edema. Treatment includes. airway support, establishment of an I.V. line, and. administration of naloxone 2 mg I.V. (0.01 mg/kg for children), with repeat administration as necessary, up to a total of 10 mg. Primary attention should be directed to ensuring adequate respiratory exchange.")
101
Morfina PHARMACODYNAMICS / KINETICS Onset of action:
Oral (immediate release): ~30 minutes; I.V.: 5-10 minutes Duration: Pain relief: Immediate release formulations: 4 hours Extended release epidural injection (DepoDur™): >48 hours Absorption: Variable Distribution: Vd: 3-4 L/kg; binds to opioid receptors in the CNS and periphery (eg, GI tract) Protein binding: 30% to 35%
: ~30 minutes; I.V.: 5-10 minutes. Duration: Pain relief: Immediate release formulations: 4 hours Extended release epidural injection (DepoDur™): >48 hours. Absorption: Variable. Distribution: Vd: 3-4 L/kg; binds to opioid receptors in the CNS and periphery (eg, GI tract) Protein binding: 30% to 35%")
102
Morfina PHARMACODYNAMICS / KINETICS
Metabolism: Hepatic via conjugation with glucuronic acid to morphine-3-glucuronide (inactive), morphine-6-glucuronide (active), and in lesser amounts, morphine-3-6-diglucuronide; other minor metabolites include normorphine (active) and the 3-ethereal sulfate Bioavailability: Oral: 17% to 33% (first-pass effect limits oral bioavailability oral; parenteral effectiveness reportedly varies from 1:6 in opioid naive patients to 1:3 with chronic use) Half-life elimination: Adults: 2-4 hours (immediate release forms) Time to peak, plasma: Kadian®: ~10 hours
, morphine-6-glucuronide (active), and in lesser amounts, morphine-3-6-diglucuronide; other minor metabolites include normorphine (active) and the 3-ethereal sulfate. Bioavailability: Oral: 17% to 33% (first-pass effect limits oral bioavailability oral; parenteral effectiveness reportedly varies from 1:6 in opioid naive patients to 1:3 with chronic use) Half-life elimination: Adults: 2-4 hours (immediate release forms) Time to peak, plasma: Kadian®: ~10 hours.")
103
Morfina PHARMACODYNAMICS / KINETICS
Excretion: Urine (primarily as morphine-3-glucuronide, ~2% to 12% excreted unchanged); feces (~7% to 10%). It has been suggested that accumulation of morphine-6-glucuronide might cause toxicity with renal insufficiency. All of the metabolites (ie, morphine-3-glucuronide, morphine-6-glucuronide, and normorphine) have been suggested as possible causes of neurotoxicity (eg, myoclonus).
; feces (~7% to 10%). It has been suggested that accumulation of morphine-6-glucuronide might cause toxicity with renal insufficiency. All of the metabolites (ie, morphine-3-glucuronide, morphine-6-glucuronide, and normorphine) have been suggested as possible causes of neurotoxicity (eg, myoclonus).")
104
Morfina Dosis de carga Dosis de mantenimiento FG > 50 ml/min
Dosis suplemtaria tras HD DPCA TSCR Morfina 100% 75% 50% Ninguna Descono-cida Dosis FG 10-50%

105
Buprenorfina Agonista parcial. Ello significa que la activación del receptor opioide mu por la buprenorfina a dosis máximas no consigue alcanzar los efectos máximos de la morfina. Presenta una intensa unión al receptor opioide, lo que tiene repercusiones en el tratamiento de la intoxicación aguda Efecto máximo inferior al de morfina o fentanilo, pero difícil de revertir con antagonistas puros.

106
Buprenorfina Cuando se administra buprenorfina a pacientes que están recibiendo agonistas puros, puede producirse un cierto grado de antagonismo funcional que, incluso, puede producir un cierto síndrome de abstinencia.

107
N02A-Analgésicos narcóticos (Opioides)
NOMBRE GENÉRICO PRESENTACIÓN VIA NOMBRE COMERCIAL Buprenorfina Comp 0,2 mg Amp 0,3 mg/1 ml SL IM, IV Buprex CE Metadona Amp 10 mg/1 ml Comp 5 mg Comp 40 mg SC, IM OR Metasedin CE Petidina (Meperidina) Amp 100 mg/2 ml SC, IM, IV Dolantina CE CE: Control de estupefacientes. Nota 1: Comprimidos ranurados. Nota 2: Uso restringido para tratamiento del dolor crónico. Nota 3: Los parches de 2,5, 5 y 10 mg liberan respectivamente 25, 50 y 100 mcg/h durante 72 h.
 Amp 100 mg/2 ml. SC, IM, IV. Dolantina CE. CE: Control de estupefacientes. Nota 1: Comprimidos ranurados. Nota 2: Uso restringido para tratamiento del dolor crónico. Nota 3: Los parches de 2,5, 5 y 10 mg liberan respectivamente 25, 50 y 100 mcg/h durante 72 h.")
108
Buprenorfina DOSING: ADULTS — Long-term use is not recommended
Acute pain (moderate to severe): I.M.: Initial: Opiate-naive: 0.3 mg every 6-8 hours as needed; initial dose (up to 0.3 mg) may be repeated once in minutes after the initial dose if needed; usual dosage range: mg every 4-8 hours as needed Slow I.V.: Initial: Opiate-naive: 0.3 mg every 6-8 hours as needed; initial dose (up to 0.3 mg) may be repeated once in minutes after the initial dose if needed
: I.M.: Initial: Opiate-naive: 0.3 mg every 6-8 hours as needed; initial dose (up to 0.3 mg) may be repeated once in minutes after the initial dose if needed; usual dosage range: mg every 4-8 hours as needed Slow I.V.: Initial: Opiate-naive: 0.3 mg every 6-8 hours as needed; initial dose (up to 0.3 mg) may be repeated once in minutes after the initial dose if needed.")
109
Buprenorfina Heroin or opiate withdrawal (unlabeled use): I.M., slow I.V.: Variable; mg every 6 hours Opioid dependence: Sublingual: Induction: Range: mg/day (doses during an induction study used 8 mg on day 1, followed by 16 mg on day 2; induction continued over 3-4 days). Treatment should begin at least 4 hours after last use of heroin or short-acting opioid, preferably when first signs of withdrawal appear. Titrating dose to clinical effectiveness should be done as rapidly as possible to prevent undue withdrawal symptoms and patient drop-out during the induction period. Maintenance: Target dose: 16 mg/day; range: 4-24 mg/day; patients should be switched to the buprenorphine/naloxone combination product for maintenance and unsupervised therapy
. Treatment should begin at least 4 hours after last use of heroin or short-acting opioid, preferably when first signs of withdrawal appear. Titrating dose to clinical effectiveness should be done as rapidly as possible to prevent undue withdrawal symptoms and patient drop-out during the induction period. Maintenance: Target dose: 16 mg/day; range: 4-24 mg/day; patients should be switched to the buprenorphine/naloxone combination product for maintenance and unsupervised therapy.")
110
Buprenorfina DOSING: PEDIATRIC
Acute pain (moderate to severe): Children 2-12 years: I.M., slow I.V.: 2-6 mcg/kg every 4-6 hours Children 13 years: Refer to adult dosing. DOSING: ELDERLY — Moderate to severe pain: I.M., slow I.V.: 0.15 mg every 6 hours; elderly patients are more likely to suffer from confusion and drowsiness compared to younger patients. Long-term use is not recommended.
: Children 2-12 years: I.M., slow I.V.: 2-6 mcg/kg every 4-6 hours Children 13 years: Refer to adult dosing. DOSING: ELDERLY — Moderate to severe pain: I.M., slow I.V.: 0.15 mg every 6 hours; elderly patients are more likely to suffer from confusion and drowsiness compared to younger patients. Long-term use is not recommended.")
111
Buprenorfina DRUG INTERACTIONS — Substrate of CYP3A4 (major); Inhibits CYP1A2 (weak), 2A6 (weak), 2C19 (weak), 2D6 (weak) Cimetidine: May increase sedation from narcotic analgesics; however, histamine blockers may attenuate the cardiovascular response from histamine release associated with narcotic analgesics. CNS depressants: May produce additive respiratory and CNS depression; includes benzodiazepines, barbiturates, ethanol, and other sedatives. Respiratory and CV collapse was reported in a patient who received diazepam and buprenorphine. CYP3A4 inducers: CYP3A4 inducers may decrease the levels/effects of buprenorphine. Example inducers include aminoglutethimide, carbamazepine, nafcillin, nevirapine, phenobarbital, phenytoin, and rifamycins. CYP3A4 inhibitors: May increase the levels/effects of buprenorphine. Example inhibitors include azole antifungals, clarithromycin, diclofenac, doxycycline, erythromycin, imatinib, isoniazid, nefazodone, nicardipine, propofol, protease inhibitors, quinidine, and verapamil. Naltrexone: May antagonize the effect of narcotic analgesics; concurrent use or use within 7-10 days of injection for pain relief is contraindicated.

112
Buprenorfina PREGNANCY IMPLICATIONS — Withdrawal has been reported in infants of women receiving buprenorphine during pregnancy. Onset of symptoms ranged from day 1 to day 8 of life, most occurring on day 1. LACTATION — Enters breast milk. Not recommended

113
Buprenorfina TOXICOLOGY / OVERDOSE COMPREHENSIVE —
Symptoms include CNS depression, pinpoint pupils, hypotension, and bradycardia. Treatment is supportive. Naloxone may have limited effects in reversing respiratory depression; Doxapram has also been used to stimulate respirations

114
Buprenorfina PHARMACODYNAMICS / KINETICS
Onset of action: Analgesic: minutes Duration: 6-8 hours Absorption: I.M., SubQ: 30% to 40% Distribution: Vd: L/kg Protein binding: High Metabolism: Primarily hepatic; extensive first-pass effect Half-life elimination: hours Excretion: Feces (70%); urine (20% as unchanged drug)
; urine (20% as unchanged drug)")
115
Meperidina Existe otro tipo de opioides denominados agonistas-antagonistas, que son capaces de actuar como agonistas sobre un tipo de receptores y como antagonistas sobre otro tipo, por lo que producen respuestas imprevisibles. En pacientes que reciben agonistas puros, los agonistas-antagonistas pueden precipitar reacciones de abstinencia.

116
Meperidina Agonistas-antagonista.
Estos fármacos tienen afinidad, variable de unos a otros, por los diferentes subtipos de receptores. En general se comportan como agonistas totales de kappa, pero como agonistas parciales, e incluso antagonistas, de receptores mu. Las consecuencias, dependen de si se ha administrado previamente un agonista total o no. En ausencia de éstos, el resultado es un efecto analgésico, resultado de la activación de receptores mu (parcial) y kappa (total). Ahora bien, si los pacientes están recibiendo un agonista total (morfina, fentanilo), el resultado será un desplazamiento del receptor y una activación parcial de éste por los agonistas-antagonistas. En consecuencia, los pacientes sentirán un grado menor de analgesia, lo que se interpreta como un antagonismo, cuando con frecuencia realmente no lo es desde un punto farmacológico estricto.
 y kappa (total). Ahora bien, si los pacientes están recibiendo un agonista total (morfina, fentanilo), el resultado será un desplazamiento del receptor y una activación parcial de éste por los agonistas-antagonistas. En consecuencia, los pacientes sentirán un grado menor de analgesia, lo que se interpreta como un antagonismo, cuando con frecuencia realmente no lo es desde un punto farmacológico estricto.")
117
N02A-Analgésicos narcóticos (Opioides)
NOMBRE GENÉRICO PRESENTACIÓN VIA NOMBRE COMERCIAL Buprenorfina Comp 0,2 mg Amp 0,3 mg/1 ml SL IM, IV Buprex CE Metadona Amp 10 mg/1 ml Comp 5 mg Comp 40 mg SC, IM OR Metasedin CE Petidina (Meperidina) Amp 100 mg/2 ml SC, IM, IV Dolantina CE CE: Control de estupefacientes. Nota 1: Comprimidos ranurados. Nota 2: Uso restringido para tratamiento del dolor crónico. Nota 3: Los parches de 2,5, 5 y 10 mg liberan respectivamente 25, 50 y 100 mcg/h durante 72 h.
 Amp 100 mg/2 ml. SC, IM, IV. Dolantina CE. CE: Control de estupefacientes. Nota 1: Comprimidos ranurados. Nota 2: Uso restringido para tratamiento del dolor crónico. Nota 3: Los parches de 2,5, 5 y 10 mg liberan respectivamente 25, 50 y 100 mcg/h durante 72 h.")
118
Meperidina INYECCION IV DIRECTA: SI
Administrar la dosis prescrita en forma de inyección IV lenta, para ello disolver con SF de forma que la concentración final sea 5 o 10 mg/ml. Ejemplo tomar 1 o 2 ml de la ampolla con una jeringa y completar el volumen hasta 10 ml. Administrar en 1 a 2 minutos. INFUSION INTERMITENTE: SI Diluir la dosis prescrita en ml de SF ó SG5%. Administrar según pauta médica.( Ejemplo 0,3 mg/Kg/hora). INFUSION CONTINUA: SI En ocasiones, para mantener a un paciente sedado se utiliza el llamado "coctel lítico", éste está compuesto por: Meperidina (Dolantina), Clorpromazina (Largactil) y Prometacina (Frinova). se administra en forma de infusión continua, en SF ó SG5%. INYECCION IM: SI Administrar la dosis prescrita en forma de inyección IM profunda. Es de elección especialmente en dosis múltiples se prefiere a la vía SC INYECCION SUBCUTANEA: SI Cuando deban administrarse dosis repetidas, es preferible la vía IM, ya que la vía SC es irritante de los tejidos. SUEROS COMPATIBLES: SF, SG5%
. INFUSION CONTINUA: SI. En ocasiones, para mantener a un paciente sedado se utiliza el llamado coctel lítico , éste está compuesto por: Meperidina (Dolantina), Clorpromazina (Largactil) y Prometacina (Frinova). se administra en forma de infusión continua, en SF ó SG5%. INYECCION IM: SI. Administrar la dosis prescrita en forma de inyección IM profunda. Es de elección especialmente en dosis múltiples se prefiere a la vía SC. INYECCION SUBCUTANEA: SI. Cuando deban administrarse dosis repetidas, es preferible la vía IM, ya que la vía SC es irritante de los tejidos. SUEROS COMPATIBLES: SF, SG5%")
119
Meperidina DOSING: ADULTS —
Not recommended for chronic pain. In patients with normal renal function, doses of 600 mg/24 hours and use for 48 hours are recommended (American Pain Society, 1999). Pain (analgesic): I.M., SubQ: Initial: Opiate-naive: mg every 3-4 hours as needed; patients with prior opiate exposure may require higher initial doses.
. Pain (analgesic): I.M., SubQ: Initial: Opiate-naive: mg every 3-4 hours as needed; patients with prior opiate exposure may require higher initial doses.")
120
Meperidina DOSING: PEDIATRIC — DOSING: ELDERLY —
Oral, I.M., I.V., SubQ: Children: mg/kg/dose every 3-4 hours as needed; 1-2 mg/kg as a single dose preoperative medication may be used; maximum 100 mg/dose. (Oral route is not recommended for acute pain.) DOSING: ELDERLY — Oral: 50 mg every 4 hours I.M.: 25 mg every 4 hours
 DOSING: ELDERLY — Oral: 50 mg every 4 hours. I.M.: 25 mg every 4 hours.")
121
Meperidina DOSING: RENAL IMPAIRMENT
Clcr mL/minute: Administer 75% of normal dose. Clcr <10 mL/minute: Administer 50% of normal dose. Repeated use in renal impairment should be avoided due to potential accumulation of neuroexcitatory metabolite. DOSING: HEPATIC IMPAIRMENT — Increased narcotic effect in cirrhosis; reduction in dose is more important for oral than I.V. route.

122
Meperidina ADVERSE REACTIONS SIGNIFICANT — Cardiovascular: Hypotension
Central nervous system: Fatigue, drowsiness, dizziness, nervousness, headache, restlessness, malaise, confusion, mental depression, hallucinations, paradoxical CNS stimulation, increased intracranial pressure, seizure (associated with metabolite accumulation), serotonin syndrome Dermatologic: Rash, urticaria Gastrointestinal: Nausea, vomiting, constipation, anorexia, stomach cramps, xerostomia, biliary spasm, paralytic ileus, sphincter of Oddi spasm Genitourinary: Ureteral spasms, decreased urination Local: Pain at injection site Neuromuscular & skeletal: Weakness Respiratory: Dyspnea Miscellaneous: Histamine release, physical and psychological dependence
, serotonin syndrome. Dermatologic: Rash, urticaria. Gastrointestinal: Nausea, vomiting, constipation, anorexia, stomach cramps, xerostomia, biliary spasm, paralytic ileus, sphincter of Oddi spasm. Genitourinary: Ureteral spasms, decreased urination. Local: Pain at injection site. Neuromuscular & skeletal: Weakness. Respiratory: Dyspnea. Miscellaneous: Histamine release, physical and psychological dependence.")
123
Meperidina PRECAUTIONS —
Meperidine is not recommended for the management of chronic pain. When used for acute pain (in patients without renal or CNS disease), treatment should be limited to 48 hours and doses should not exceed 600 mg/24 hours. Normeperidine (an active metabolite and CNS stimulant) may accumulate and precipitate anxiety, tremors, or seizures; risk increases with renal dysfunction and cumulative dose.
, treatment should be limited to 48 hours and doses should not exceed 600 mg/24 hours. Normeperidine (an active metabolite and CNS stimulant) may accumulate and precipitate anxiety, tremors, or seizures; risk increases with renal dysfunction and cumulative dose.")
124
Meperidina DRUG INTERACTIONS Substrate (minor) of CYP2B6, 2C19, 3A4
Acyclovir: May increase meperidine metabolite concentrations. Use caution. Barbiturates: May decrease analgesic efficacy and increase sedative and/or respiratory depressive effects of meperidine. Cimetidine: May increase meperidine metabolite concentrations; use caution. CNS depressants (including benzodiazepines): May potentiate the sedative and/or respiratory depressive effects of meperidine. MAO inhibitors: May enhance the serotonergic effect of meperidine, which may cause serotonin syndrome. Concurrent use with or within 14 days of an MAO inhibitor is contraindicated. Phenothiazines: May potentiate the sedative and/or respiratory depressive effects of meperidine; may increase the incidence of hypotension. Phenytoin: May decrease the analgesic effects of meperidine Ritonavir: May increase meperidine metabolite concentrations; use caution. Serotonin agonists: Serotonin agonists and meperidine may enhance serotonin levels in the brain. Serotonin syndrome may occur. Serotonin reuptake inhibitors: May potentiate the effects of meperidine, increasing serotonin levels in the brain. Serotonin syndrome may occur. Sibutramine: May enhance the serotonergic effect of meperidine. Serotonin syndrome may occur. Tricyclic antidepressants: May potentiate the sedative and/or respiratory depressive effects of meperidine. In addition, potentially may increase the risk of serotonin syndrome.
: May potentiate the sedative and/or respiratory depressive effects of meperidine. MAO inhibitors: May enhance the serotonergic effect of meperidine, which may cause serotonin syndrome. Concurrent use with or within 14 days of an MAO inhibitor is contraindicated. Phenothiazines: May potentiate the sedative and/or respiratory depressive effects of meperidine; may increase the incidence of hypotension. Phenytoin: May decrease the analgesic effects of meperidine. Ritonavir: May increase meperidine metabolite concentrations; use caution. Serotonin agonists: Serotonin agonists and meperidine may enhance serotonin levels in the brain. Serotonin syndrome may occur. Serotonin reuptake inhibitors: May potentiate the effects of meperidine, increasing serotonin levels in the brain. Serotonin syndrome may occur. Sibutramine: May enhance the serotonergic effect of meperidine. Serotonin syndrome may occur. Tricyclic antidepressants: May potentiate the sedative and/or respiratory depressive effects of meperidine. In addition, potentially may increase the risk of serotonin syndrome.")
125
Meperidina PREGNANCY IMPLICATIONS — LACTATION —
Meperidine is known to cross the placenta, which may result in respiratory or CNS depression in the newborn. LACTATION — Enters breast milk. contraindicated

126
Meperidina REFERENCE RANGE — Therapeutic: ng/mL (SI: nmol/L); Toxic: >1000 ng/mL (SI: >4043 nmol/L) TOXICOLOGY / OVERDOSE COMPREHENSIVE — Symptoms include CNS depression, respiratory depression, mydriasis, bradycardia, pulmonary edema, chronic tremors, CNS excitability, and seizures. Treatment of overdose includes airway support, establishment of an I.V. line, and administration of naloxone 2 mg I.V. (0.01 mg/kg for children), with repeat administration as necessary, up to a total of 10 mg. Naloxone should not be used to treat meperidine-induced seizures. Naloxone does not reverse the adverse effects of normeperidine.
, with repeat administration as necessary, up to a total of 10 mg. Naloxone should not be used to treat meperidine-induced seizures. Naloxone does not reverse the adverse effects of normeperidine.")
127
Meperidina PHARMACODYNAMICS / KINETICS Onset of action: Analgesic: Oral, SubQ: minutes; I.V.: ~5 minutes Peak effect: SubQ.: ~1 hour; Oral: 2 hours Duration: Oral, SubQ.: 2-4 hours Absorption: I.M.: Erratic and highly variable Distribution: Crosses placenta; enters breast milk Protein binding: 65% to 75% Metabolism: Hepatic; hydrolyzed to meperidinic acid (inactive) or undergoes N-demethylation to normeperidine (active; has 1/2 the analgesic effect and 2-3 times the CNS effects of meperidine) Bioavailability: ~50% to 60%; increased with liver disease Half-life elimination: Parent drug: Terminal phase: Adults: hours, Liver disease: 7-11 hours Normeperidine (active metabolite): hours; can accumulate with high doses or with decreased renal function Excretion: Urine (as metabolites)
 or undergoes N-demethylation to normeperidine (active; has 1/2 the analgesic effect and 2-3 times the CNS effects of meperidine) Bioavailability: ~50% to 60%; increased with liver disease. Half-life elimination: Parent drug: Terminal phase: Adults: hours, Liver disease: 7-11 hours Normeperidine (active metabolite): hours; can accumulate with high doses or with decreased renal function. Excretion: Urine (as metabolites)")
128
Dosis de carga Dosis de mantenimiento FG > 50 ml/min FG ml/min FG < 10 ml/min Dosis suplemtaria tras HD DPCA TSCR Meperidina 75% 50% Clcr mL/minute: Administer 75% of normal dose. Clcr <10 mL/minute: Administer 50% of normal dose. Repeated use in renal impairment should be avoided due to potential accumulation of neuroexcitatory metabolite.

129
Gracias.

Presentaciones similares
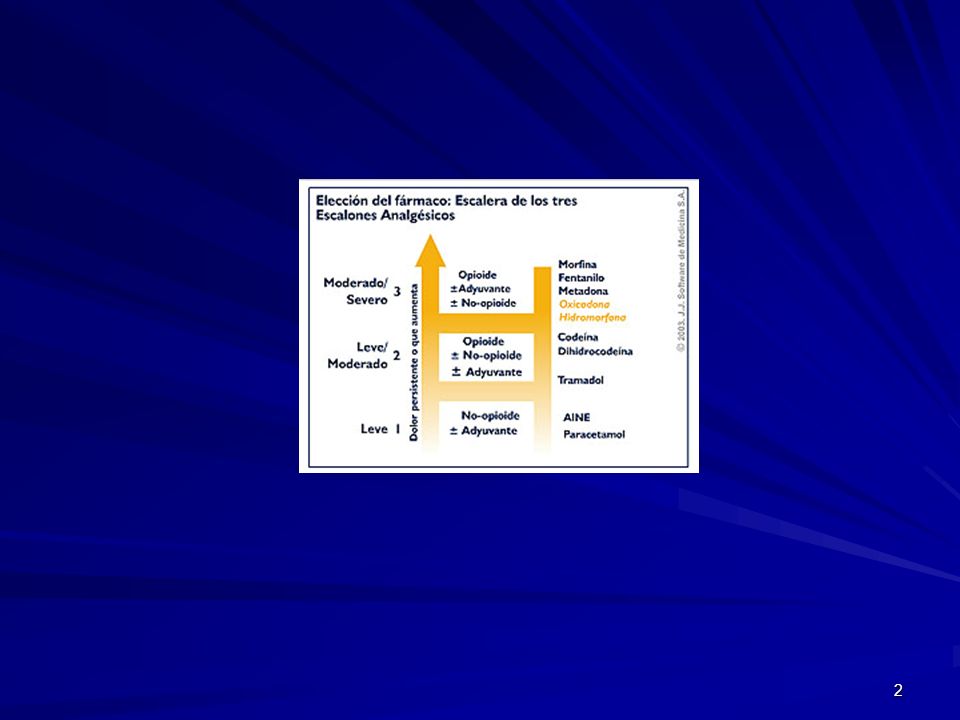


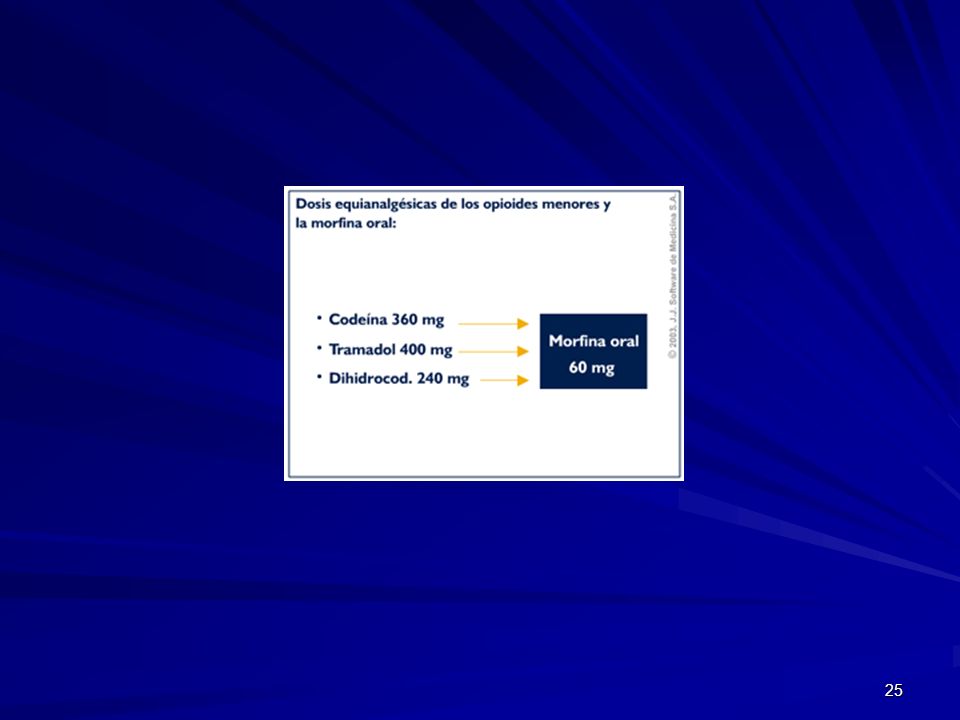
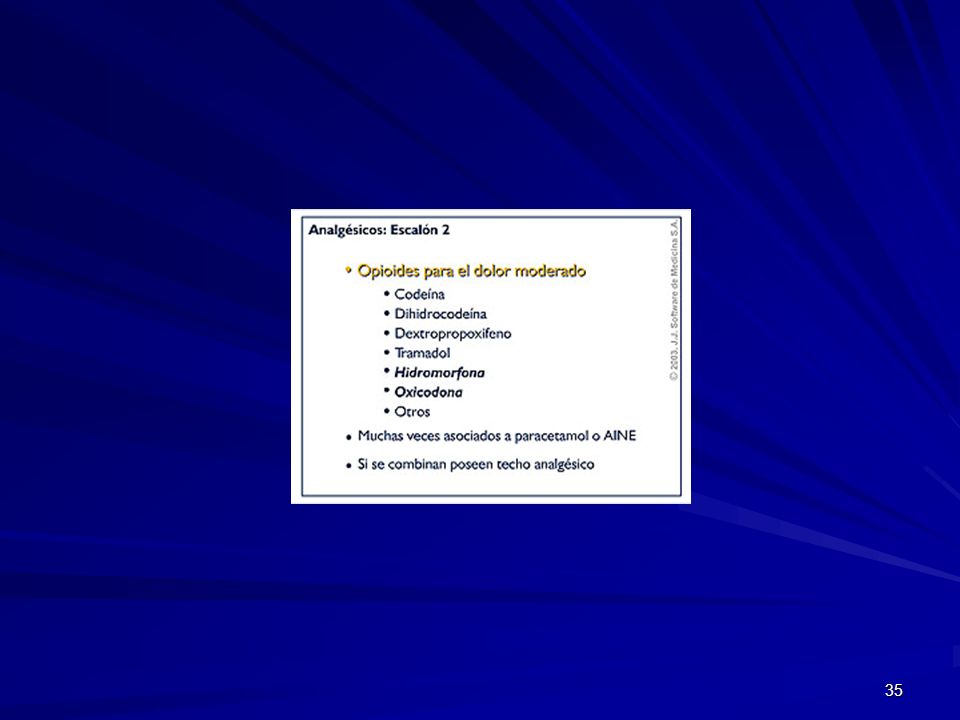

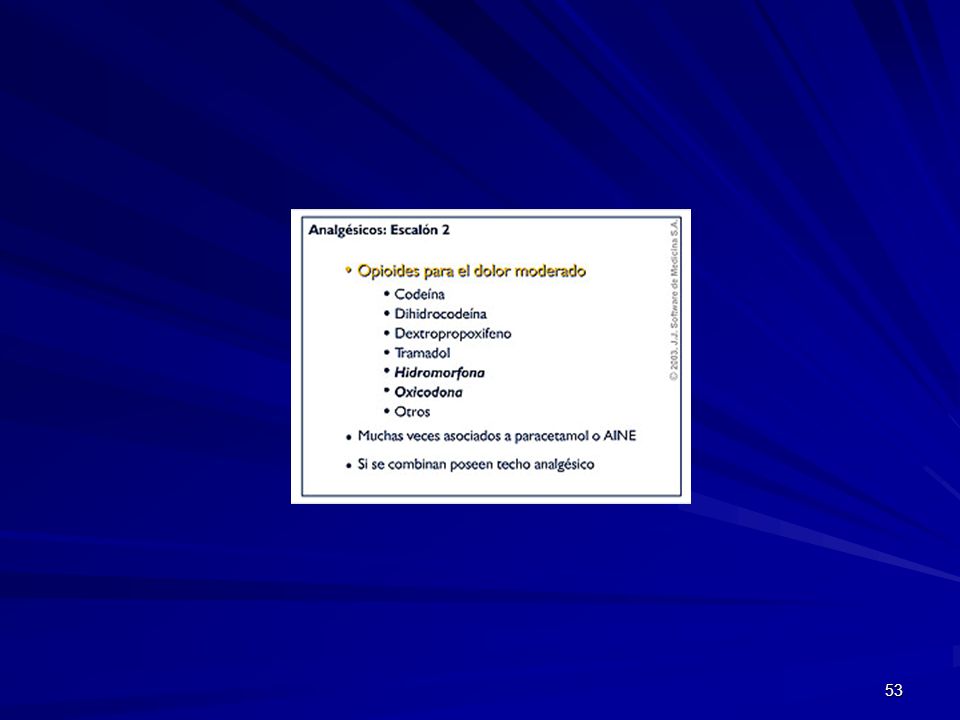
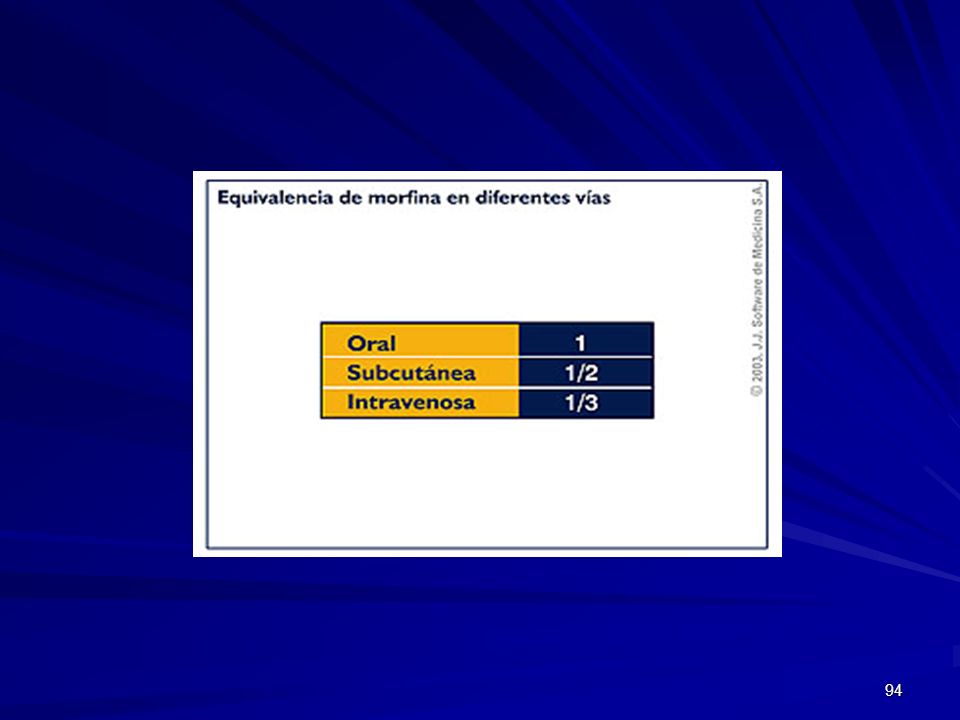












 Noviembre de 2004.>")
 29 de julio de 2004.>")





