Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Aterosclerosis Dra. Verónica Irribarra Depto
Aterosclerosis Dra. Verónica Irribarra Depto. Nutrición Diabetes y Metabolismo 2013

2
Aterosclerosis (ATE) “athero” = pasta o engrudo
“sclerosis” = endurecimiento relación entre colesterol y ATE: 1913 Anitschkow y Chalatow: conejos alimentados con huevos ≈ lesiones similares a ateromas humanos (colesterol) ’30 metabolismo del colesterol ’50 Ultracentrífuga› fracciones de lipoproteínas ’70 Ancel Keys: Estudio de siete países
 ’30 metabolismo del colesterol. ’50 Ultracentrífuga› fracciones de lipoproteínas. ’70 Ancel Keys: Estudio de siete países.")
3
Seven Countries Study: Relación entre colesterol y mortalidad
35 Norte de Europa 30 25 Estados Unidos 20 Tasa de mortalidad cqardiovascular/1000 15 Sur de Europa, Irlanda 10 Twenty-five year follow-up data from the Seven Countries study1 show that serum total cholesterol levels are linearly related to CHD mortality across cultures. The relative increase in CHD mortality rates with a given increase in cholesterol are similar. However, the large between-country difference in CHD mortality rates at a given cholesterol level indicates that other factors, such as diet, also play a role in the development of CHD. The link between high cholesterol levels and increased incidence of CHD has also been shown in the prospective part of the Multiple Risk Intervention study.2 In epidemiological studies, measurements of serum cholesterol have been routinely used. The relationship between cholesterol levels and the incidence of CHD is almost entirely dependent on low-density lipoprotein (LDL) cholesterol, the main carrier of cholesterol and a major atherogenic lipoprotein.3 Results from the Framingham study4 during 26 years of observation show that men have twice the incidence of CHD mortality and morbidity of women. This difference tends to diminish during the later years, after the menopause. Other factors that influence susceptibility to CHD include ethnic background and social class. 5-7 References 1. Verschuren WM et al. J Am Med Assoc 1995;274(2):131–136. 2. Martin MJ et al. Lancet 1986;ii:933–936. 3. Kannel WB et al. In Proceeding of Golden Jubilee International Congress, Minnesota, Eds Loan MS, Holman RT.Oxford, Pergamon Press 1982;339–348. 4. Lerner DJ, Kannel WB. Am Heart J 1986;11(2):383–390. 5. Rosamond WD et al. N Engl J Med 1998;339:861–867. 6. Goff DC et al. Circulation 1997;95:1433–1440. 7. Poulter N. In Cardiovascular Disease: Risk Factors and Intervention. Eds: Poulter N, Sever P, Thom S. Radcliffe Medical Press, Oxford, 1993. Serbia Sur de Europa, Mediterraneo 5 Japon 2.60 3.25 3.90 4.50 5.15 5.80 6.45 7.10 7.75 8.40 9.05 Colesterol total (mmol/L) Adapted from Verschuren WM et al. J Am Med Assoc 1995;274(2):131–136
 cholesterol, the main carrier of cholesterol and a major atherogenic lipoprotein.3. Results from the Framingham study4 during 26 years of observation show that men have twice the incidence of CHD mortality and morbidity of women. This difference tends to diminish during the later years, after the menopause. Other factors that influence susceptibility to CHD include ethnic background and social class References. 1. Verschuren WM et al. J Am Med Assoc 1995;274(2):131– Martin MJ et al. Lancet 1986;ii:933– Kannel WB et al. In Proceeding of Golden Jubilee International Congress, Minnesota, Eds Loan MS, Holman RT.Oxford, Pergamon Press 1982;339– Lerner DJ, Kannel WB. Am Heart J 1986;11(2):383– Rosamond WD et al. N Engl J Med 1998;339:861– Goff DC et al. Circulation 1997;95:1433– Poulter N. In Cardiovascular Disease: Risk Factors and Intervention. Eds: Poulter N, Sever P, Thom S. Radcliffe Medical Press, Oxford, Serbia. Sur de Europa, Mediterraneo. 5. Japon Colesterol total (mmol/L) Adapted from Verschuren WM et al. J Am Med Assoc 1995;274(2):131–136.")
4
Enfermedad cardiovascular incidencia por 1000
Estudio de Framingham: Relación entre Colesterol y riesgo cardiovascular 150 125 100 Enfermedad cardiovascular incidencia por 1000 75 50 25 Cardiovascular disease is associated with increased levels of total cholesterol.1 Other risk factors include an increase in total to HDL-cholesterol ratio, hypertension, cigarette smoking, excess weight, elevated blood sugar levels, lack of exercise, stress, and electrocardiographic abnormalities. Intervention trials have shown that identifying and lowering these risk factors may help to reduce the subsequent rate of coronary heart disease, stroke, and other cardiovascular disease. Reference 1. Castelli WP. Am J Med. 1984;76:4-12. <204 205–234 235–264 265–294 >295 Colesterol (mg/100 mL) Adapted from Castelli WP. Am J Med 1984;76:4–12
 Adapted from Castelli WP. Am J Med 1984;76:4–12.")
5
Colesterol: un factor de riesgo modificable
En USA, 37% (102 millones) tienen colesterol total elevado (>200 mg/dL)1 Meta-análisis, 10% reducción en colesterol total permite: 15% reducción en mortalidad por enfermedad coronaria (p<0.001) 11% reducción en mortalidad total (p<0.001)3 LDL-colesterol objetivo primario en prevención de enfermedad coronaria. It has been estimated that in the USA approximately 102 million people have elevated total cholesterol levels of >200 mg/dL (5.2 mmol/L) and 41 million levels of >240 mg/dL (6.2 mmol/L).1 In EUROASPIRE II, 58% (n=5556) of patients with established CHD were found to have elevated cholesterol levels (5 mmol/L, 190 mg/dL).2 Early trials have shown that a reduction in total cholesterol results in a reduction in the incidence of CHD events. In addition, a meta-analysis of 38 trials3 has shown that for every 10% reduction in total cholesterol, CHD mortality is reduced by 15%, and total mortality by 11% (both p<0.001). Similar reductions were seen with all lipid-modifying treatments studied. Thus, total cholesterol is a modifiable risk factor for CHD and total mortality.4 Low-density lipoprotein (LDL) cholesterol has been recognised as a prime target for lipid intervention to prevent CHD. Under NCEP ATP III LDL-C guidelines it has been estimated that approximately 36 million patients would be suitable for drug therapy.5 The intensity of intervention depends not only on raised cholesterol or LDL-cholesterol but also on the presence of a number of other risk factors for CHD. References 1. American Heart Association. Heart and Stroke Statistical Update; 2002. 2. EUROASPIRE II Study Group. Eur Heart J 2001;22:554–572. 3. Gould AL et al. Circulation 1998;97:946–952. 4. National Cholesterol Education Program. Circulation 1994;98(3):1333–1445. 5. Fedder DO, Koro CE, L’Italien GJ. Circulation 2002;105:152–156. Adapted from: 1. American Heart Association. Heart and Stroke Statistical Update; 2002; 2. EUROASPIRE II Study Group. Eur Heart J 2001;22:554–572; 3. Gould AL et al. Circulation 1998;97:946–952
 tienen colesterol total elevado (>200 mg/dL)1. Meta-análisis, 10% reducción en colesterol total permite: 15% reducción en mortalidad por enfermedad coronaria (p<0.001) 11% reducción en mortalidad total (p<0.001)3. LDL-colesterol objetivo primario en prevención de enfermedad coronaria. It has been estimated that in the USA approximately 102 million people have elevated total cholesterol levels of >200 mg/dL (5.2 mmol/L) and 41 million levels of >240 mg/dL (6.2 mmol/L).1 In EUROASPIRE II, 58% (n=5556) of patients with established CHD were found to have elevated cholesterol levels (5 mmol/L, 190 mg/dL).2. Early trials have shown that a reduction in total cholesterol results in a reduction in the incidence of CHD events. In addition, a meta-analysis of 38 trials3 has shown that for every 10% reduction in total cholesterol, CHD mortality is reduced by 15%, and total mortality by 11% (both p<0.001). Similar reductions were seen with all lipid-modifying treatments studied. Thus, total cholesterol is a modifiable risk factor for CHD and total mortality.4. Low-density lipoprotein (LDL) cholesterol has been recognised as a prime target for lipid intervention to prevent CHD. Under NCEP ATP III LDL-C guidelines it has been estimated that approximately 36 million patients would be suitable for drug therapy.5 The intensity of intervention depends not only on raised cholesterol or LDL-cholesterol but also on the presence of a number of other risk factors for CHD. References. 1. American Heart Association. Heart and Stroke Statistical Update; EUROASPIRE II Study Group. Eur Heart J 2001;22:554– Gould AL et al. Circulation 1998;97:946– National Cholesterol Education Program. Circulation 1994;98(3):1333– Fedder DO, Koro CE, L’Italien GJ. Circulation 2002;105:152–156. Adapted from: 1. American Heart Association. Heart and Stroke Statistical Update; 2002; 2. EUROASPIRE II Study Group. Eur Heart J 2001;22:554–572; 3. Gould AL et al. Circulation 1998;97:946–952.")
6
Enfermedad Cardiovascular: Factores de riesgo
Modificables: Tabaquismo Dislipidemia LDL-colesterol elevado HDL-colesterol bajo Trigliceridos elevados Hipertensión Arterial Diabetes mellitus Obesidad Dieta Factores trombogénicos Sedentarismo Consumo excesivo de alcohol No-modificables: Historia personal de EC Historia familiar de EC Edad Género Some of the risk factors that predispose an individual to the development or progression of CHD are outlined above. Evidence has shown that lifestyles associated with a ‘western’ culture such as a diet rich in saturated fats and high in calories, smoking and physical inactivity, are some of the modifiable risk factors leading to an increase in the prevalence of CHD. Of these, three are considered to be of prime importance:1 Smoking is responsible for 50% of all avoidable deaths, of which half are due to CVD. Raised blood pressure has been found to be an important risk factor for the development of CHD, cardiac failure and cerebrovascular disease. The greater the increase in blood pressure, the higher the risk. Greatest benefit of blood pressure lowering is seen in those at higher risk. Even modest reductions produce substantial benefits in those with multiple risk factors. Dyslipidaemia, in particular, raised low-density lipoprotein (LDL) cholesterol and triglyceride levels, and low high-density lipoprotein (HDL) cholesterol are associated with increased risk of CHD. Since 60–70% of plasma cholesterol is transported in the LDL fraction, total cholesterol measurement has been widely used in epidemiological studies rather than plasma LDL-cholesterol. Reference 1. Pyörälä K et al. Eur Heart J 1994;15:1300–1331. Adapted from: Pyörälä K et al. Eur Heart J 1994;15:1300–1331
 cholesterol and triglyceride levels, and low high-density lipoprotein (HDL) cholesterol are associated with increased risk of CHD. Since 60–70% of plasma cholesterol is transported in the LDL fraction, total cholesterol measurement has been widely used in epidemiological studies rather than plasma LDL-cholesterol. Reference. 1. Pyörälä K et al. Eur Heart J 1994;15:1300–1331. Adapted from: Pyörälä K et al. Eur Heart J 1994;15:1300–1331.")
7
Niveles de riesgo asociados a HTA, hipercolesterolemia y tabaquismo
Hipertensión (Presión sistólica 195 mmHg) x3 x4.5 x9 x16 x1.6 x4 x6 Multiple risk factors for CHD are usually present in an individual; rarely do they occur in isolation. When risk factors co-exist the sum of their combined effect is often much greater than the sum of their individual effects.1 Thus, the patient with severe hypercholesterolaemia may be at lower risk than the patient with moderate hypertension, moderately elevated lipid levels and who smokes. Reference 1. Poulter N. In Cardiovascular Disease: Risk Factors and Intervention. Eds: Poulter N, Sever P, Thom S. Radcliffe Medical Press, Oxford, 1993. Tabaquismo Colesterol (330 mg/dL) Adapted from Poulter N et al., 1993
 x3. x4.5. x9. x16. x1.6. x4. x6. Multiple risk factors for CHD are usually present in an individual; rarely do they occur in isolation. When risk factors co-exist the sum of their combined effect is often much greater than the sum of their individual effects.1 Thus, the patient with severe hypercholesterolaemia may be at lower risk than the patient with moderate hypertension, moderately elevated lipid levels and who smokes. Reference. 1. Poulter N. In Cardiovascular Disease: Risk Factors and Intervention. Eds: Poulter N, Sever P, Thom S. Radcliffe Medical Press, Oxford, Tabaquismo. Colesterol (330 mg/dL) Adapted from Poulter N et al.,")
8
Pared arterial normal Túnica adventicia Túnica media Túnica íntima
Endotelio Tejido conectivo subendotelial Membrana elástica interna Célula muscular lisa The normal artery consists of three distinctive layers: the intima, the innermost layer comprising a single layer of endothelial cells on the luminal surface; the media, a tube of vascular smooth muscle cells (VSMCs) and their extracellular matrix; and the adventitia, the outer protective layer comprising loose connective tissue containing blood vessels and nerves which supply the artery itself.1,2 The endothelial cells of the intima have a number of important functions; forming a non-thrombotic, non-adherent surface, acting as a semi-permeable membrane, synthesising and releasing chemical mediators, maintaining the basement membrane, and modifying lipoproteins as they cross into the artery wall. The VSMCs of the media contract and relax to alter the lumen diameter of the vessel in response to a variety of circulating and local stimuli, regulating vascular tone, blood flow and blood pressure. This is effected through the production of a number of vasoactive substances including prostaglandins, endothelin and nitric oxide (NO).1,2 References 1. Weissberg PL. Eur Heart J Supplements 1999:1:T13–8. 2. In: Statins - The HMG-CoA Reductase Inhibitors in Perspective. Eds Gaw A, Packard CJ, Shepherd J. Martin Dunitz 2000, 1–19. Fibras elásticas/colágenas Membrana elástica interna Adapted from Weissberg PL. Eur Heart J Supplements 1999:1:T13–18
 and their extracellular matrix; and the adventitia, the outer protective layer comprising loose connective tissue containing blood vessels and nerves which supply the artery itself.1,2. The endothelial cells of the intima have a number of important functions; forming a non-thrombotic, non-adherent surface, acting as a semi-permeable membrane, synthesising and releasing chemical mediators, maintaining the basement membrane, and modifying lipoproteins as they cross into the artery wall. The VSMCs of the media contract and relax to alter the lumen diameter of the vessel in response to a variety of circulating and local stimuli, regulating vascular tone, blood flow and blood pressure. This is effected through the production of a number of vasoactive substances including prostaglandins, endothelin and nitric oxide (NO).1,2. References. 1. Weissberg PL. Eur Heart J Supplements 1999:1:T13–8. 2. In: Statins - The HMG-CoA Reductase Inhibitors in Perspective. Eds Gaw A, Packard CJ, Shepherd J. Martin Dunitz 2000, 1–19. Fibras elásticas/colágenas. Membrana elástica interna. Adapted from Weissberg PL. Eur Heart J Supplements 1999:1:T13–18.")
9
Patogénesis de la placa aterosclerótica
Daño endotelial Respuesta protectora lleva a la producción de moléculas de adhesión celular Monocitos y linfocitos T adhieren a La superficie ‘pegajosa’ de las células endoteliales Migración hacia espacio subendotelial The primary event in atherosclerosis is thought to be damage caused to the endothelium of arterial walls, resulting in endothelial dysfunction. This damage may be caused by a variety of factors; haemodynamic forces (shear stress caused by e.g. hypertension), a number of vasoactive substances, mediators (cytokines) from blood cells, cigarette smoke, atherogenic diet, elevated glucose levels and oxidised LDL-cholesterol.1 Initially, damage causes the endothelial cells to express cellular adhesion molecules such as cytokines (interleukin-1, IL-1; tumour necrosis factor , TNF-), chemokines (monocyte chemoattractant factor 1, MCP-1; IL-8) and growth factors (platelet-derived growth factor, PDGF; basic fibroblast growth factor, bFGF).1 This ‘sticky’ surface encourages inflammatory cells such as monocytes and T lymphocytes to attach to the endothelial surface. Once attached they migrate through the intact endothelium into the subendothelial space. Many of the monocytes differentiate into macrophages and take up oxidised LDL, which is more atherogenic than native LDL; these macrophages then become foam cells.1 Oxidised LDL promotes death of endothelial cells and an inflammatory response resulting in impairment of normal function of the endothelium. In addition, it modifies the response to angiotensin II, resulting in vasodilatory impairment, and induces a prothrombic state by affecting platelets and coagulation factors. Thus, the endothelium responds to damage by inducing a protective response which will eventually lead to the formation of fibrofatty and fibrous lesions, the atherosclerotic plaque, preceded and accompanied by inflammation.2 References 1. Koenig W. Eur Heart J Supplements 1999:1:T19–26. 2. Ross R. Nature 1993;362:801–809. Macrófagos atrapan LDL-colesterol oxidado Células espumosas ricas en lípidos Estría lipídica y placa aterosclerótica
, a number of vasoactive substances, mediators (cytokines) from blood cells, cigarette smoke, atherogenic diet, elevated glucose levels and oxidised LDL-cholesterol.1. Initially, damage causes the endothelial cells to express cellular adhesion molecules such as cytokines (interleukin-1, IL-1; tumour necrosis factor , TNF-), chemokines (monocyte chemoattractant factor 1, MCP-1; IL-8) and growth factors (platelet-derived growth factor, PDGF; basic fibroblast growth factor, bFGF).1 This ‘sticky’ surface encourages inflammatory cells such as monocytes and T lymphocytes to attach to the endothelial surface. Once attached they migrate through the intact endothelium into the subendothelial space. Many of the monocytes differentiate into macrophages and take up oxidised LDL, which is more atherogenic than native LDL; these macrophages then become foam cells.1. Oxidised LDL promotes death of endothelial cells and an inflammatory response resulting in impairment of normal function of the endothelium. In addition, it modifies the response to angiotensin II, resulting in vasodilatory impairment, and induces a prothrombic state by affecting platelets and coagulation factors. Thus, the endothelium responds to damage by inducing a protective response which will eventually lead to the formation of fibrofatty and fibrous lesions, the atherosclerotic plaque, preceded and accompanied by inflammation.2. References. 1. Koenig W. Eur Heart J Supplements 1999:1:T19– Ross R. Nature 1993;362:801–809. Macrófagos atrapan LDL-colesterol oxidado. Células espumosas ricas en lípidos. Estría lipídica y placa aterosclerótica.")
10
El endotelio ‘activado’
Moléculas de adhesión celular Inducción de proliferación celular y estado protrombótico endotelio activado Atracción de monocitos y linfocitos T que adhieren a células endoteliales citokinas ( IL-1, TNF-) quimokinas (MCP-1, IL-8) Fact. de crecimiento (PDGF, FGF) Endothelial injury, or exposure to atherogenic stimuli, triggers endothelial cell inflammatory responses leading to recruitment of leukocytes and release of cellular adhesion molecules; cytokines, including tumour necrosis factor- (TNF-), interleukin-1 (IL-1) and interferon gamma (IFN- ), chemokines, including monocyte chemoattractant factor 1 (MCP-1) and interleukin-8 (IL-8), and growth factors, including platelet derived growth factor (PDGF) and fibroblast growth factor (FGF).1 The cytokines, in addition to amplifying the immune response, alter endothelial cell function towards a prothrombotic state, characterised by increased production of platelet activator inhibitor-1 (PAI-1), tissue factor expression (TFE) and activation of the extrinsic coagulation pathway), and release of PDGF. Reference 1. Koenig W. Eur Heart J 1999;1(Suppl T);T19–26. Adapted from Koenig W. Eur Heart J 1999;1(Suppl T);T19–26
 quimokinas (MCP-1, IL-8) Fact. de crecimiento (PDGF, FGF) Endothelial injury, or exposure to atherogenic stimuli, triggers endothelial cell inflammatory responses leading to recruitment of leukocytes and release of cellular adhesion molecules; cytokines, including tumour necrosis factor- (TNF-), interleukin-1 (IL-1) and interferon gamma (IFN- ), chemokines, including monocyte chemoattractant factor 1 (MCP-1) and interleukin-8 (IL-8), and growth factors, including platelet derived growth factor (PDGF) and fibroblast growth factor (FGF).1. The cytokines, in addition to amplifying the immune response, alter endothelial cell function towards a prothrombotic state, characterised by increased production of platelet activator inhibitor-1 (PAI-1), tissue factor expression (TFE) and activation of the extrinsic coagulation pathway), and release of PDGF. Reference. 1. Koenig W. Eur Heart J 1999;1(Suppl T);T19–26. Adapted from Koenig W. Eur Heart J 1999;1(Suppl T);T19–26.")
11
Disfunción endotelial en aterosclerosis
Regulación (+) de moléculas de adhesión endotelial Adhesión de leucocitos Aumento de permeabilidad endotelial Migración de leucocitos dentro de pared arterial Endothelial dysfunction in atherosclerosis is characterised by a series of early changes that precede lesion formation. The changes include greater permeability of the endothelium, up-regulation of leucocyte and endothelial adhesion molecules and migration of leucocytes into the artery wall.1 Reference 1. Ross R. N Engl J Med 1999;362:115–126. Adapted from Ross R. N Engl J Med 1999;362:115–126
 de. moléculas de adhesión. endotelial. Adhesión. de leucocitos. Aumento de. permeabilidad. endotelial. Migración de. leucocitos. dentro de. pared arterial. Endothelial dysfunction in atherosclerosis is characterised by a series of early changes that precede lesion formation. The changes include greater permeability of the endothelium, up-regulation of leucocyte and endothelial adhesion molecules and migration of leucocytes into the artery wall.1. Reference. 1. Ross R. N Engl J Med 1999;362:115–126. Adapted from Ross R. N Engl J Med 1999;362:115–126.")
12
Etapas en el desarrollo de la placa ATE
Figure 8 There are six stages of development of AS: Grades I – IV: accumulation of lipids, first intracellularly, then extracellularly; Grade V: fibrosis around the lipid core forming an atherosclerotic plaque; Grade VI: complicated plaque (rupture, clot or bleed) leading to a clinical event.
 leading to a clinical event.")
13
Formación de la placa aterosclerótica complicada
cápsula fibrosa The development of an atherosclerotic plaque indicates an advanced stage in the atherosclerotic process and results from death and rupture of the lipid-laden foam cells in the fatty streak. Migration of vascular smooth muscle cells (VSMCs) to the intima and laying down of collagen fibres results in the formation of a protective fibrous cap over the lipid core. The fibrous cap is a crucial component of the mature atherosclerotic plaque as it separates the highly thrombogenic lipid-rich core from circulating platelets and other coagulation factors. Stable atherosclerotic plaques are characterised by a necrotic lipid core covered by a thick VSM-rich fibrous cap. Lesions expand at the shoulders by continued leukocyte adhesion. 1 Reference 1. Ross R. N Engl J Med 1999;362:115–126. Formación del centro necrótico Acumulación de macrófagos Adapted from Ross R. N Engl J Med 1999;362:115–126
 to the intima and laying down of collagen fibres results in the formation of a protective fibrous cap over the lipid core. The fibrous cap is a crucial component of the mature atherosclerotic plaque as it separates the highly thrombogenic lipid-rich core from circulating platelets and other coagulation factors. Stable atherosclerotic plaques are characterised by a necrotic lipid core covered by a thick VSM-rich fibrous cap. Lesions expand at the shoulders by continued leukocyte adhesion. 1. Reference. 1. Ross R. N Engl J Med 1999;362:115–126. Formación del. centro necrótico. Acumulación. de macrófagos. Adapted from Ross R. N Engl J Med 1999;362:115–126.")
14
Vulnerabilidad de la placa: rol de los macrófagos
Figure 14 Factors which play a key role in increasing plaque vulnerability. These include: lipid core formation; parietal vascular inflammation; thinning of the fibrous cap; thrombus formation.

15
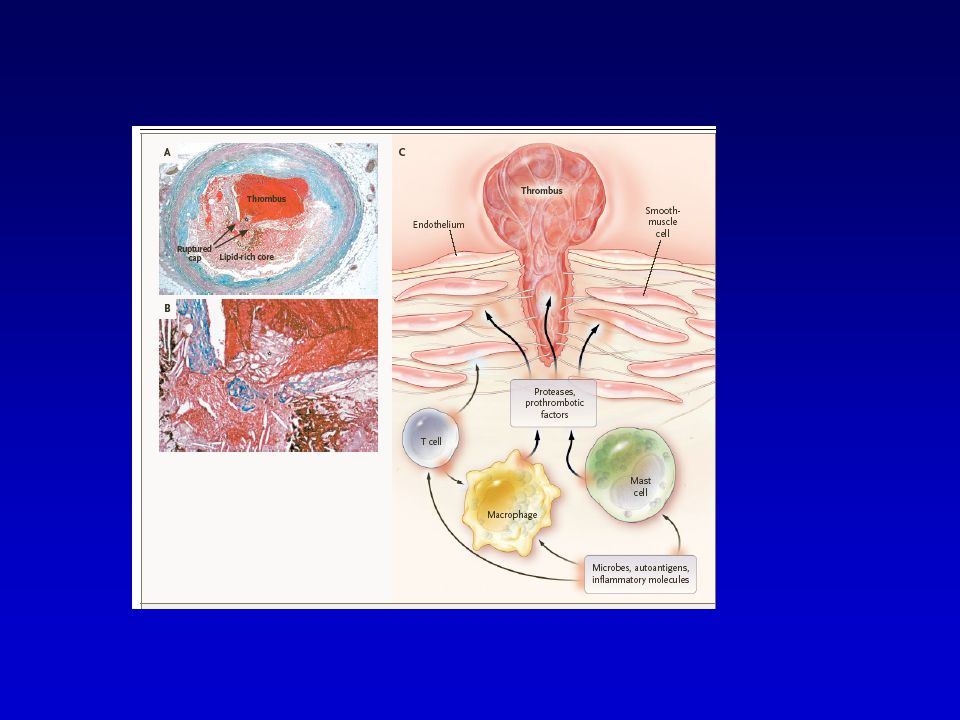
La placa “inestable” Adelgazamiento de la cápsula fibrosa
An atherosclerotic plaque may cause complications as a result of its size, reducing lumen diameter and blood flow, its tendency to rupture, or following its erosion. Plaque erosion or rupture occur in plaques that are intrinsically vulnerable. Factors that may influence their vulnerability include hypertension, high turbulent blood flow, an increased number of inflammatory cells, a lipid-rich core and a thin fibrous cap with few smooth muscle cells or collagen fibres. Both erosion and rupture can lead to thrombus formation on the site of the plaque and vessel occlusion. Plaque formation can also cause hardening of the arteries, resulting in weakening and thinning of the vessel wall, leading to aneurysm and possibly haemorrhage.1 Regression of atherosclerotic plaques can occur with lipid-modifying therapy and with dietary and lifestyle changes. Unstable fibrous plaques in atherosclerosis are prone to rupture and ulceration, followed by rapid development of thrombi. Rupture usually occurs at sites of thinning and is associated with regions where there is greater influx and activation of macrophages, accompanied by release of metalloproteinases.1 Reference 1. Ross R. N Engl J Med 1999;362:115–126. Adelgazamiento de la cápsula fibrosa Hemorragia desde microvasos de la placa Ruptura de la cápsula fibrosa Adapted from Ross R. N Engl J Med 1999;362:115–126

16
La placa vulnerable Vulnerable plaques are characterised by a thin fibrous caps, a core rich in lipid and macrophages, and less evidence of smooth muscle proliferation. In contrast, the stable plaque has a relatively thick fibrous cap protecting the lipid core from the contact with blood. Vulnerable plaques are prone to rupture and ulceration, followed by rapid development of thrombi. The size of the plaque does not appear to predict whether a plaque is prone to rupture, indeed clinical data suggest that stable plaques more often show luminal narrowing detectable by angiography than do vulnerable plaques. Rupture usually occurs at sites of thinning (particularly at the shoulder area of the plaque) and is associated with regions where there are relatively few smooth muscle cells but abundant macrophages and T cells. Rupture is associated with greater influx and activation of macrophages, accompanied by release of matrix metalloproteinases that are involved with the breakdown of collagen.1 Reference 1. Libby P. Circulation 1995;91:2844–2850. Adapted from Libby P. Circulation 1995;91:2844–2850
 and is associated with regions where there are relatively few smooth muscle cells but abundant macrophages and T cells. Rupture is associated with greater influx and activation of macrophages, accompanied by release of matrix metalloproteinases that are involved with the breakdown of collagen.1. Reference. 1. Libby P. Circulation 1995;91:2844–2850. Adapted from Libby P. Circulation 1995;91:2844–2850.")
17
Ruptura de la placa: (placa resquebrajada, fisurada, rota – inicio de la trombosis)
Figure 21 Plaque rupture produces occlusive thrombosis. The occlusion may be partial (such as a wall thrombus, which is fibrin- and platelet-rich) and gives rise to unstable angina, or complete myocardial infarction (the thrombi of which are thrombin-rich). Partial occlusions are prone to embolization and, as such, can give rise to distal occlusions.
 and gives rise to unstable angina, or complete myocardial infarction (the thrombi of which are thrombin-rich). Partial occlusions are prone to embolization and, as such, can give rise to distal occlusions.")
19
Manifestaciones clínicas de aterosclerosis
Enfermedad coronaria Angina pectoris, infarto al miocardio, muerte súbita de origen cardíaco Enfermedad cerebrovascular Isquemia transitoria, accidente vascular encefálico Enfermedad vascular periférica Claudicación intermitente, gangrena Coronary heart disease Restriction of blood flow to the myocardium may be caused by an atherosclerotic plaque narrowing the lumen of the coronary arteries. If the diameter of the coronary artery is reduced by more than 50%, ischaemia will develop and the patient will experience tightness or crushing pain in the chest (angina pectoris). However, pain does not always accompany myocardial ischaemia: this is called silent ischaemia. Coronary plaque rupture and erosion have been shown to result in thrombus formation within coronary arteries. If blood flow is completely obstructed, either due to a thrombus or by a large atherosclerotic plaque, death to part of the myocardium may ensue, resulting in an MI. Depending on the magnitude or site of the damage to the myocardium the pumping action of the heart may be impaired and/or the heart rate and rhythm may become disturbed. These can result in congestive heart failure or, if very severe, sudden cardiac death.1 Cerebrovascular disease Narrowing of the carotid, vertebral and cerebral arteries supplying blood to the brain can cause a brief interruption in the blood supply to the brain resulting in a transient ischaemic attack. This may cause temporary impairment of vision, speech, sensation or movement and may be followed by a stroke. A stroke may also be caused by formation of a thrombus or embolus, arterial rupture or haemorrhage of the cerebral arteries stopping the oxygen supply to parts of the brain. Sudden loss of consciousness often occurs with subsequent paralysis of parts of the body. It can lead to permanent damage and disability and sudden death.1 Peripheral vascular disease When the lumen of arteries such as the femoral and iliac arteries supplying blood to the legs has been significantly narrowed, by 60% or more, the symptoms of intermittent claudication become evident. These include an aching or cramping pain, most often in the legs when walking, which occurs when insufficient oxygen is reaching the muscles in the legs. In advanced cases of peripheral vascular disease, blood supply to the legs may become completely blocked, possibly by thrombus formation, and painful leg and foot ulcers may develop. If left untreated gangrene may eventually ensue, requiring amputation of the affected limb.1 Reference 1. In: Statins - The HMG-CoA Reductase Inhibitors in Perspective. Eds Gaw A, Packard CJ, Shepherd J. Martin Dunitz 2000,
. However, pain does not always accompany myocardial ischaemia: this is called silent ischaemia. Coronary plaque rupture and erosion have been shown to result in thrombus formation within coronary arteries. If blood flow is completely obstructed, either due to a thrombus or by a large atherosclerotic plaque, death to part of the myocardium may ensue, resulting in an MI. Depending on the magnitude or site of the damage to the myocardium the pumping action of the heart may be impaired and/or the heart rate and rhythm may become disturbed. These can result in congestive heart failure or, if very severe, sudden cardiac death.1. Cerebrovascular disease Narrowing of the carotid, vertebral and cerebral arteries supplying blood to the brain can cause a brief interruption in the blood supply to the brain resulting in a transient ischaemic attack. This may cause temporary impairment of vision, speech, sensation or movement and may be followed by a stroke. A stroke may also be caused by formation of a thrombus or embolus, arterial rupture or haemorrhage of the cerebral arteries stopping the oxygen supply to parts of the brain. Sudden loss of consciousness often occurs with subsequent paralysis of parts of the body. It can lead to permanent damage and disability and sudden death.1. Peripheral vascular disease When the lumen of arteries such as the femoral and iliac arteries supplying blood to the legs has been significantly narrowed, by 60% or more, the symptoms of intermittent claudication become evident. These include an aching or cramping pain, most often in the legs when walking, which occurs when insufficient oxygen is reaching the muscles in the legs. In advanced cases of peripheral vascular disease, blood supply to the legs may become completely blocked, possibly by thrombus formation, and painful leg and foot ulcers may develop. If left untreated gangrene may eventually ensue, requiring amputation of the affected limb.1. Reference. 1. In: Statins - The HMG-CoA Reductase Inhibitors in Perspective. Eds Gaw A, Packard CJ, Shepherd J. Martin Dunitz 2000,")
20
Funciones Biologicas del Colesterol
Componente de membrana, controla su fluidez Precursor de ácidos sales biliares Precursor de hormonas esteroidales Precursor de la vitamina D

21
Intercambio del Colesterol
Síntesis Hepática Sintesis Extrahepática Dieta Pool hepático de Colesterol Conversión Hormonas esteroidales Secrecion de HDL y VLDL Colesterol libre biliar Conversión a Ácidos / Sales biliares

22
Fuentes alimentarias de Colesterol
El Colesterol prácticamente sólo está presente en los alimentos de origen animal Sus principales fuentes son: yema del huevo, vísceras, mariscos crustáceos mantequilla, margarinas y mantecas de origen marino o marino-vegetal

23
Metabolismo de lipoproteínas
Moléculas compuestas, constituidas por dos fracciones lipídicas: Hidrofílica: fosfolípidos y colesterol libre Hidrofóbica: Colesterol éster y triglicéridos Función es el transporte de lípidos en el espacio vascular.

24
Estructura de lipoproteínas
Colesterol libre Fosfolípidos Triglicéridos Lipoproteins are macromolecular aggregates of lipids and apolipoproteins. Lipids can be divided into two main groups, simple and complex. The two most important simple lipids are cholesterol and fatty acids. Lipids become complex lipids when fatty acids undergo esterification to produce esters.1-3 Simple lipids Cholesterol is a soft waxy substance present in all cells of the body. Most tissues can produce cholesterol, but it is synthesised primarily in the liver and small intestine. Approximately 50% of the cholesterol requirement is synthesised, whilst the rest is obtained from animal produce in the diet. Cholesterol is important in the repair of cell membranes and in the synthesis of steroid hormones, vitamin D and bile acids. Fatty acids are the simplest form of lipid found in the body and are an important energy source. They exist as saturated, monounsaturated and polyunsaturated forms, distinguished by the number of bonds between the hydrocarbon chain and carbon atoms. The most common fatty acids in the body are stearic and palmitic (saturated), and oleic (monounsaturated). Fatty acids exist freely in the plasma mostly bound to albumin, but are stored in adipose tissue as triglycerides.1-3 Complex lipids Triglycerides are mainly stored in adipose tissue and are the main lipid currency of the body. Phospholipids are glycerol esters containing two fatty acids. They have a water-soluble and a lipid-soluble surface and are an important component of the cell membrane. Cholesterol esters, oleate and linoleate, are the storage molecules of cholesterol in cells.1-3 Apolipoproteins In order for these water-insoluble lipids to be transported around the body in the the aqueous medium, blood, they are aggregated with apolipoproteins to form lipoproteins. These multimolecular packages consist of a hydrophobic core containing cholesteryl esters and triglyceride, surrounded by a hydrophilic surface layer of phospholipids, proteins and some free cholesterol. While structurally similar, lipoproteins vary in their proportions of component molecules and the type of proteins present.1-3 References 1. In: Fast Facts - Hyperlipidaemia. Eds Durrington P, Sniderman A. Health Press Ltd, Oxford, –17. 2. In: Manual of Lipid Disorders, 2nd Edition. Eds Gotto A, Pownall H. Williams & Wilkins, US, 3. In: Statins - The HMG-CoA Reductase Inhibitors in Perspective. Eds Gaw A, Packard CJ, Shepherd J. Martin Dunitz 2000, 1-19. Esteres de colesterol Apolipoproteina
, and oleic (monounsaturated). Fatty acids exist freely in the plasma mostly bound to albumin, but are stored in adipose tissue as triglycerides.1-3. Complex lipids Triglycerides are mainly stored in adipose tissue and are the main lipid currency of the body. Phospholipids are glycerol esters containing two fatty acids. They have a water-soluble and a lipid-soluble surface and are an important component of the cell membrane. Cholesterol esters, oleate and linoleate, are the storage molecules of cholesterol in cells.1-3. Apolipoproteins In order for these water-insoluble lipids to be transported around the body in the the aqueous medium, blood, they are aggregated with apolipoproteins to form lipoproteins. These multimolecular packages consist of a hydrophobic core containing cholesteryl esters and triglyceride, surrounded by a hydrophilic surface layer of phospholipids, proteins and some free cholesterol. While structurally similar, lipoproteins vary in their proportions of component molecules and the type of proteins present.1-3. References. 1. In: Fast Facts - Hyperlipidaemia. Eds Durrington P, Sniderman A. Health Press Ltd, Oxford, – In: Manual of Lipid Disorders, 2nd Edition. Eds Gotto A, Pownall H. Williams & Wilkins, US, In: Statins - The HMG-CoA Reductase Inhibitors in Perspective. Eds Gaw A, Packard CJ, Shepherd J. Martin Dunitz 2000, Esteres de colesterol. Apolipoproteina.")
25
Clasificación de Lipoproteinas
Basada en densidad: Quilomicrones Very low-density lipoprotein (VLDL) Intermediate-density lipoprotein (IDL)= remanentes de Qm y VLDL Low-density lipoprotein (LDL) A: grandes B: pequeñas y densas High-density lipoprotein (HDL) HDLn, HDL2 HDL3 There are five major classes of lipoproteins based on their density. The degree to which lipoproteins cause atherosclerosis depends to some extent on their size, and thus their ability to enter and form deposits within the arterial wall. Thus, smaller VLDL, IDL and LDL are all atherogenic, whereas large VLDL and chylomicrons are not. HDL, largely by its ability to carry cholesterol away from the arterial wall, is anti-atherogenic. Chylomicrons are the largest in size, lowest in density and are not associated with atherosclerosis. They are synthesised in the intestinal mucosal cells after a fatty meal. They transport dietary triglyceride from the intestine to the sites of use and storage, and are cleared rapidly from the bloodstream, generally being undetectable 12 hours after a meal.1,2 VLDL are similar in structure to chylomicrons but are smaller. They are produced in the liver and are the main carriers of endogenous (synthesised in the liver rather then dietary) triglycerides and cholesterol to sites for use or storage. As they are also involved in the synthesis of LDL, VLDL are implicated in atherosclerosis development.1,2 IDL are highly atherogenic. They are formed during the breakdown of VLDL and chylomicrons and are also implicated in atherosclerosis development. They contain less triglyceride and more cholesterol than VLDL, and are involved in the recycling of cholesterol by the liver as well as formation of LDL in the blood.1,2 LDL are generated from IDL in the circulation and are the principal lipoproteins involved in atherosclerosis. Oxidised LDL is the most atherogenic form of LDL. They are the main carriers of cholesterol, accounting for 60–70% of plasma cholesterol. They comprise four main subtypes: LDL I, II, III and IV, of which LDL-III is the most atherogenic subclass.1,2 HDL are the smallest but most abundant of the lipoproteins. They do not cause atherosclerosis, but actually protect against its development. This is because they return about 20–30% of cholesterol in the blood to the liver from peripheral tissue for excretion. They also inhibit the oxidation of LDL and they decrease the attraction of macrophages to the artery wall. There are two main subtypes: HDL2 and HDL3.1,2 References 1. In: Fast Facts - Hyperlipidaemia. Eds Durrington P, Sniderman A. Health Press Ltd, Oxford, –17. 2. In: Manual of Lipid Disorders, 2nd Edition. Eds Gotto A, Pownall H. Williams & Wilkins, US, –10.
 Intermediate-density lipoprotein (IDL)= remanentes de Qm y VLDL. Low-density lipoprotein (LDL) A: grandes. B: pequeñas y densas. High-density lipoprotein (HDL) HDLn, HDL2 HDL3. There are five major classes of lipoproteins based on their density. The degree to which lipoproteins cause atherosclerosis depends to some extent on their size, and thus their ability to enter and form deposits within the arterial wall. Thus, smaller VLDL, IDL and LDL are all atherogenic, whereas large VLDL and chylomicrons are not. HDL, largely by its ability to carry cholesterol away from the arterial wall, is anti-atherogenic. Chylomicrons are the largest in size, lowest in density and are not associated with atherosclerosis. They are synthesised in the intestinal mucosal cells after a fatty meal. They transport dietary triglyceride from the intestine to the sites of use and storage, and are cleared rapidly from the bloodstream, generally being undetectable 12 hours after a meal.1,2. VLDL are similar in structure to chylomicrons but are smaller. They are produced in the liver and are the main carriers of endogenous (synthesised in the liver rather then dietary) triglycerides and cholesterol to sites for use or storage. As they are also involved in the synthesis of LDL, VLDL are implicated in atherosclerosis development.1,2. IDL are highly atherogenic. They are formed during the breakdown of VLDL and chylomicrons and are also implicated in atherosclerosis development. They contain less triglyceride and more cholesterol than VLDL, and are involved in the recycling of cholesterol by the liver as well as formation of LDL in the blood.1,2. LDL are generated from IDL in the circulation and are the principal lipoproteins involved in atherosclerosis. Oxidised LDL is the most atherogenic form of LDL. They are the main carriers of cholesterol, accounting for 60–70% of plasma cholesterol. They comprise four main subtypes: LDL I, II, III and IV, of which LDL-III is the most atherogenic subclass.1,2. HDL are the smallest but most abundant of the lipoproteins. They do not cause atherosclerosis, but actually protect against its development. This is because they return about 20–30% of cholesterol in the blood to the liver from peripheral tissue for excretion. They also inhibit the oxidation of LDL and they decrease the attraction of macrophages to the artery wall. There are two main subtypes: HDL2 and HDL3.1,2. References. 1. In: Fast Facts - Hyperlipidaemia. Eds Durrington P, Sniderman A. Health Press Ltd, Oxford, – In: Manual of Lipid Disorders, 2nd Edition. Eds Gotto A, Pownall H. Williams & Wilkins, US, –10.")
26
Apolipoproteinas Principal contenido protéico de lipoproteinas
Funciones incluyen: Facilitación de transporte lipídico Regulación del metabolismo de lipoproteínas lecithin cholesterol acyltransferase (LCAT) lipoprotein lipase (LPL) hepatic triglyceride lipase (HTGL) Vectorización de lipoproteínas y unión a receptores específicos Apolipoproteins are the protein constituents of lipoproteins and they have three main functions:1 1. They facilitate lipid transport by stabilising the water-soluble lipids, cholesterol esters and triglycerides in aqueous plasma. 2. They regulate the interaction of these lipids with the enzymes lecithin cholesterol acyltransferase (LCAT), lipoprotein lipase (LPL) and hepatic triglyceride lipase (HTGL). 3. They bind to cell surface receptors. There are eight broad groups of apolipoproteins that have currently been identified. These are designated apo A to F, apo H and apo J. The form of apolipoprotein B that is made in the liver (apo B100) is associated with high levels of LDL and is an important marker for atherosclerosis.2 References 1. In: Statins - The HMG-CoA Reductase Inhibitors in Perspective. Eds Gaw A, Packard CJ, Shepherd J. Martin Dunitz 2000, 1–19. 2. In: Fast Facts - Hyperlipidaemia. Eds Durrington P, Sniderman A. Health Press Ltd, Oxford, –17.
 lipoprotein lipase (LPL) hepatic triglyceride lipase (HTGL) Vectorización de lipoproteínas y unión a receptores específicos. Apolipoproteins are the protein constituents of lipoproteins and they have three main functions:1. 1. They facilitate lipid transport by stabilising the water-soluble lipids, cholesterol esters and triglycerides in aqueous plasma. 2. They regulate the interaction of these lipids with the enzymes lecithin cholesterol acyltransferase (LCAT), lipoprotein lipase (LPL) and hepatic triglyceride lipase (HTGL). 3. They bind to cell surface receptors. There are eight broad groups of apolipoproteins that have currently been identified. These are designated apo A to F, apo H and apo J. The form of apolipoprotein B that is made in the liver (apo B100) is associated with high levels of LDL and is an important marker for atherosclerosis.2. References. 1. In: Statins - The HMG-CoA Reductase Inhibitors in Perspective. Eds Gaw A, Packard CJ, Shepherd J. Martin Dunitz 2000, 1– In: Fast Facts - Hyperlipidaemia. Eds Durrington P, Sniderman A. Health Press Ltd, Oxford, –17.")
27
HDL-Colesterol HDL-colesterol tiene efecto protector para riesgo de ATE y enfermedad cardiovascular A menor nivel de HDL-colesterol, es mayor el riesgo para aterosclerosis y enfermedad CV Bajo nivel (<40 mg/dL) aumenta riesgo HDL-colesterol tiende a ser bajo cuando los triglicéridos son altos HDL-colesterol disminuye por tabaquismo, obesidad e inactividad física. There is a strong inverse association between plasma HDL cholesterol and the risk of CHD; therefore, HDL-cholesterol has a protective effect. This has been shown in both patients with CHD and asymptomatic subjects, in men and women, and is independent of LDL-cholesterol and other risk factors. The lower the HDL-cholesterol level the higher the risk for CHD; a low level (<40 mg/dL) increases risk and a higher level (60 mg/dL, 1.6 mmol/L) can be considered a negative risk factor.1 Concentrations of HDL-cholesterol tend to be low when triglycerides are high. Low concentrations of HDL-cholesterol are also associated with an atherogenic lifestyle, as HDL-cholesterol is lowered by smoking, obesity and physical inactivity.2 A combination of plasma triglycerides >2 mmol/L (180 mg/dL) and HDL-cholesterol <1 mmol/L (40 mg/dL) predicts a high risk of CHD, in particular if the cholesterol to HDL-cholesterol ratio is greater than 5.2 References 1. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. JAMA 2001:285;2486–2497. 2. Wood D et al, for the Joint European Committee, Second Task Force of European and other Societies. Atherosclerosis 1998;140:199–270.
 aumenta riesgo. HDL-colesterol tiende a ser bajo cuando los triglicéridos son altos. HDL-colesterol disminuye por tabaquismo, obesidad e inactividad física. There is a strong inverse association between plasma HDL cholesterol and the risk of CHD; therefore, HDL-cholesterol has a protective effect. This has been shown in both patients with CHD and asymptomatic subjects, in men and women, and is independent of LDL-cholesterol and other risk factors. The lower the HDL-cholesterol level the higher the risk for CHD; a low level (<40 mg/dL) increases risk and a higher level (60 mg/dL, 1.6 mmol/L) can be considered a negative risk factor.1 Concentrations of HDL-cholesterol tend to be low when triglycerides are high. Low concentrations of HDL-cholesterol are also associated with an atherogenic lifestyle, as HDL-cholesterol is lowered by smoking, obesity and physical inactivity.2. A combination of plasma triglycerides >2 mmol/L (180 mg/dL) and HDL-cholesterol <1 mmol/L (40 mg/dL) predicts a high risk of CHD, in particular if the cholesterol to HDL-cholesterol ratio is greater than 5.2. References. 1. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. JAMA 2001:285;2486– Wood D et al, for the Joint European Committee, Second Task Force of European and other Societies. Atherosclerosis 1998;140:199–270.")
28
70% de hombres con enfermedad coronaria tenían HDL ≤ 44mg/dL Framingham 35-54
Figure 65 The importance of HDL-cholesterol as a risk factor was confirmed in the Framingham Male Offspring study. The study showed that almost 70% of men with premature CAD had low HDL (<44 mg/dL) whereas almost 70% had normal or only moderately elevated LDL.
 whereas almost 70% had normal or only moderately elevated LDL.")
29
LDL-Colesterol Fuertemente asociado con aterosclerosis y eventos coronarios 10% elevación produce un 20% de aumento en riesgo cardiovascular Riesgo asociado con LDL-C aumentado por otros factores de riesgo: HDL-colesterol bajo tabaquismo hipertensión diabetes LDL-cholesterol has been shown to be strongly associated with the development of atherosclerosis and the risk of CHD events in patients with established CHD (history of angina pectoris, MI etc.) and in those without CHD. This applies to women as well as men, but in women the general level of CHD risk is lower.1 A 10% increase in LDL-cholesterol is associated with an approximate 20% increase in risk for CHD.1 The association between LDL-cholesterol and the risk of CHD events is considerably increased by other risk factors, such as low HDL-cholesterol, smoking, hypertension and diabetes. This modification is apparent especially when total cholesterol and LDL-cholesterol are only moderately elevated.1 Reference 1. Wood D et al, for the Joint European Committee, Second Task Force of European and other Societies. Atherosclerosis 1998;140:199–270.
 and in those without CHD. This applies to women as well as men, but in women the general level of CHD risk is lower.1 A 10% increase in LDL-cholesterol is associated with an approximate 20% increase in risk for CHD.1. The association between LDL-cholesterol and the risk of CHD events is considerably increased by other risk factors, such as low HDL-cholesterol, smoking, hypertension and diabetes. This modification is apparent especially when total cholesterol and LDL-cholesterol are only moderately elevated.1. Reference. 1. Wood D et al, for the Joint European Committee, Second Task Force of European and other Societies. Atherosclerosis 1998;140:199–270.")
30
Triglicéridos Asociados con alto riesgo de eventos cardíacos que puede estar relacionado a: Bajos niveles de HDL Formas de LDL-colesterol altamente aterogénicas hiperinsulinemia/ resistencia a insulina Estado procoagulante HTA Obesidad abdominal Dislipidemias asociadas Trigliceridos normales<150 mg/dL Trigliceridos muy elevados (>1000 mg/dL) aumentan riesgo depancreatitis Hypertriglyceridaemia has been shown to be associated with increased risk of CHD events. However, the association is not as strong as that of LDL-cholesterol, and becomes much weaker when other risk factors are taken into account. The link between triglycerides and increased CHD risk is complex. It may reflect the atherogenic effects of the triglyceride-rich lipoproteins themselves, particularly the smaller particles. It may also mark the presence of other atherogenic risks such as low levels of HDL, the presence of small dense LDL particles and the presence of the Metabolic Syndrome.1 In fasting plasma, triglycerides are transported in VLDL synthesised in the liver, and after meals are also found in chylomicrons. Catabolism of these triglyceride-rich lipoproteins produces remnant lipoproteins that have atherogenic potential. Normal triglyceride levels are <150 mg/dL (1.7 mmol/L), borderline-high 150–199 mg/dL ( mmol/L), high mg/dL ( mmol/L) and very high 500 mg/dL (5.6 mmol/L).1 Patients with elevated triglycerides may have accompanying dyslipidaemias that increase the risk for CHD (e.g. familial combined hyperlipidaemia or diabetic dyslipidaemia). Severe hypertriglyceridaemia (>1000 mg/dL, 11.3 mmol/L), possibly due to chylomicrons and large forms of VLDL, increases the risk of pancreatitis but not CHD, as chylomicrons and VLDL are too large to enter the arterial wall. Reference 1. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. JAMA 2001:285;
 aumentan riesgo depancreatitis. Hypertriglyceridaemia has been shown to be associated with increased risk of CHD events. However, the association is not as strong as that of LDL-cholesterol, and becomes much weaker when other risk factors are taken into account. The link between triglycerides and increased CHD risk is complex. It may reflect the atherogenic effects of the triglyceride-rich lipoproteins themselves, particularly the smaller particles. It may also mark the presence of other atherogenic risks such as low levels of HDL, the presence of small dense LDL particles and the presence of the Metabolic Syndrome.1 In fasting plasma, triglycerides are transported in VLDL synthesised in the liver, and after meals are also found in chylomicrons. Catabolism of these triglyceride-rich lipoproteins produces remnant lipoproteins that have atherogenic potential. Normal triglyceride levels are <150 mg/dL (1.7 mmol/L), borderline-high 150–199 mg/dL ( mmol/L), high mg/dL ( mmol/L) and very high 500 mg/dL (5.6 mmol/L).1. Patients with elevated triglycerides may have accompanying dyslipidaemias that increase the risk for CHD (e.g. familial combined hyperlipidaemia or diabetic dyslipidaemia). Severe hypertriglyceridaemia (>1000 mg/dL, 11.3 mmol/L), possibly due to chylomicrons and large forms of VLDL, increases the risk of pancreatitis but not CHD, as chylomicrons and VLDL are too large to enter the arterial wall. Reference. 1. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. JAMA 2001:285;")
31
PROCAM Incidencia de infarto v/s LDL-colesterol y trigliceridos

32
PROCAM: Incidencia de infarto LDL y TG v/s HDL-C
Figure 64 The PROCAM study identified low HDL-cholesterol as an independent risk factor for MI (in addition to raised TGs and LDL).
.")
33
Transporte de lípidos Figure 38 Lipid transportation: cholesterol is mainly carried by LDL (70% of total plasma cholesterol [TPC]) and high-density lipoprotein (HDL) (20% of TPC), whilst triglycerides are mainly carried by chylomicrons and very-low-density lipoproteins (VLDL).
 and high-density lipoprotein (HDL) (20% of TPC), whilst triglycerides are mainly carried by chylomicrons and very-low-density lipoproteins (VLDL).")
34
Características de lipoproteinas
Figure 39 Characteristics of lipoproteins

36
Vía exógena del metabolismo lipídico
Intestine Intestine Dieta triglicéridos y colesterol quilomicron LP lipasa LP lipase Liver Liver Skeletal muscle Remanente Remnant receptor receptor quilomicron FFA remanente a ateroma Adipose Adipose tissue tissue

38
Vía endógena del metabolismo lipídico
LPL Lipoprotein lipase LPL Lipoprotein lipase HL Hepatic lipase HL Hepatic lipase LPL LDL LDL IDL IDL IDL HL LDL LPL LDL receptor receptor Whilst chylomicrons transport triglyceride from the gut to the liver, VLDL is the analogous particle that transports triglycerides from the liver to the rest of the body. Triglycerides together with cholesterol, cholesterol ester and other lipoprotein particles are transported in VLDL in the bloodstream, where VLDL undergoes delipidation with the enzyme lipoprotein lipase in a similar way to chylomicrons; this is the endogenous pathway of lipid metabolism. During this process, triglyceride is removed from the core and exchanged for cholesterol esters, principally from HDL. Whilst most VLDL is transformed into LDL, the larger VLDL particles are lipolysed to IDL, which is then removed from the plasma directly. Lipoprotein lipase is the main enzyme used in the lipolysis of large VLDL particles, whereas hepatic lipase reacts with the small VLDL and IDL particles.1 IDL is highly atherogenic. The product of this metabolic cascade, LDL, exists in the plasma in the form of a number of subfractions; LDL I–IV. It has been shown that small dense LDL particles are the most atherogenic. They are absorbed by macrophages within the arterial wall to form lipid-rich foam cells, the initial stage in the pathogenesis of atherosclerotic plaques.1 The enterohepatic circulation provides a route for the excretion of cholesterol and bile acids.1 Reference 1. In: Fast Facts - Hyperlipidaemia. Eds Durrington P, Sniderman A. Health Press Ltd, Oxford, –17. HL Small Small VLDL VLDL LPL HL Large Large VLDL VLDL Liver Liver

39
Transporte Reverso de Colesterol
Hígado Membrana Celular SRB1 LDL receptor CE CE FC ABCA1 VLDL, IDL, LDL LCAT CETP HDL HDL3 TG Peripheral tissues FC Colesterol libre TG Triglicéridos CE Esteres de Colesterol LCAT Lecitin colesterol acyl transferasa CETP Colesteryl ester transfer protein

40
Clasificación de Dislipidemias: Fredrickson (OMS)
Fenotipo I IIa IIb III IV V Lipoproteina elevada Quilomicrones LDL LDL y VLDL IDL VLDL VLDL y quilomicrones colesterol sérico TGs Aterogenicidad No observada +++ + Prevalencia Rara Común Intermedia Normal a Normal Normal a The Fredrickson classification was the first classification of dyslipidaemias. It was based on the analysis of plasma for various lipoprotein fractions, but took no account of the underlying aetiology of any of the dyslipidaemias. In addition, high-density lipoprotein (HDL) cholesterol levels are not considered in this classification.1 Today it is more common to identify the dyslipidaemias by the particular lipoprotein or apolipoprotein that is abnormal. Once dyslipidaemia has been identified it is important to determine the cause where possible. Dyslipidaemia may be secondary to other disorders or a primary abnormality. Common causes of secondary dyslipidaemia include: diabetes mellitus, the nephrotic syndrome, chronic renal failure, hepatobiliary disease (generally of the obstructive variety) and hypothyroidism. It should be recognised that these cause some but not all dyslipidaemias. For example, diabetes can lead to elevation of triglyceride-rich lipoproteins and reduction of HDL, but does not necessarily increase the levels of LDL. On the other hand, hepatobiliary disease is associated with an increase in the levels of LDL. Of the primary causes of dyslipidaemia, the most severe forms are caused by genetic disorders of lipoprotein metabolism. The most easily identifiable in clinical practice are familial hypercholesterolaemia (FH), polygenic hypercholesterolaemia and familial combined hypercholesterolaemia, all of which increase the risk of premature development of CHD. Patients presenting with severe forms of hypercholesterolaemia should undergo family screening to detect other family members for therapy.2 FH is an autosomal dominant disease with defects in the gene for the LDL receptor. In its heterozygous form, it is present in about 1/500 of the population. It is a highly variable disorder, with the age of onset of CHD ranging from 30–70 years for patients with the same LDL-cholesterol levels at diagnosis, and with a poor prognosis when using older lipid-modifying drugs. Women with FH tend to develop CHD 10–15 years later than male siblings with the identical LDL-receptor mutation.3 Therapy of these disorders is directed towards aggressive management of hypercholesterolaemia with a target LDL-cholesterol that depends on the overall coronary risk of the affected person.3 References 1. Yeshurun D, Gotto AM. Southern Med J 1995;88(4):379–391. 2. National Cholesterol Education Program. Circulation 1994;98(3):1333–1445. 3. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. JAMA 2001:285;2486–2497. Normal a LDL – low-density lipoprotein; IDL – intermediate-density lipoprotein; VLDL – very low-density lipoprotein. (High-density lipoprotein (HDL) colesterol, sus niveles no se consideran en la clasificación de Fredrickson.) Adapted from Yeshurun D, Gotto AM. Southern Med J 1995;88(4):379–391
 cholesterol levels are not considered in this classification.1 Today it is more common to identify the dyslipidaemias by the particular lipoprotein or apolipoprotein that is abnormal. Once dyslipidaemia has been identified it is important to determine the cause where possible. Dyslipidaemia may be secondary to other disorders or a primary abnormality. Common causes of secondary dyslipidaemia include: diabetes mellitus, the nephrotic syndrome, chronic renal failure, hepatobiliary disease (generally of the obstructive variety) and hypothyroidism. It should be recognised that these cause some but not all dyslipidaemias. For example, diabetes can lead to elevation of triglyceride-rich lipoproteins and reduction of HDL, but does not necessarily increase the levels of LDL. On the other hand, hepatobiliary disease is associated with an increase in the levels of LDL. Of the primary causes of dyslipidaemia, the most severe forms are caused by genetic disorders of lipoprotein metabolism. The most easily identifiable in clinical practice are familial hypercholesterolaemia (FH), polygenic hypercholesterolaemia and familial combined hypercholesterolaemia, all of which increase the risk of premature development of CHD. Patients presenting with severe forms of hypercholesterolaemia should undergo family screening to detect other family members for therapy.2. FH is an autosomal dominant disease with defects in the gene for the LDL receptor. In its heterozygous form, it is present in about 1/500 of the population. It is a highly variable disorder, with the age of onset of CHD ranging from 30–70 years for patients with the same LDL-cholesterol levels at diagnosis, and with a poor prognosis when using older lipid-modifying drugs. Women with FH tend to develop CHD 10–15 years later than male siblings with the identical LDL-receptor mutation.3. Therapy of these disorders is directed towards aggressive management of hypercholesterolaemia with a target LDL-cholesterol that depends on the overall coronary risk of the affected person.3. References. 1. Yeshurun D, Gotto AM. Southern Med J 1995;88(4):379– National Cholesterol Education Program. Circulation 1994;98(3):1333– Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. JAMA 2001:285;2486–2497. Normal a. LDL – low-density lipoprotein; IDL – intermediate-density lipoprotein; VLDL – very low-density lipoprotein. (High-density lipoprotein (HDL) colesterol, sus niveles no se consideran en la clasificación de Fredrickson.) Adapted from Yeshurun D, Gotto AM. Southern Med J 1995;88(4):379–391.")
41
Cómo reducir riesgo de ruptura placa
Figure 31 In those with established AS, reducing the risk of plaque rupture can be approached via two broad therapeutic routes: by increasing plaque stability; by decreasing plaque rupture-inducing factors.

42
Características de una placa inestable
Figure 34 Plaques become more unstable as: the lipid core increases as a percentage of the total plaque area; macrophages constitute a larger proportion of the fibrous cap; the fibrous cap loses smooth muscle density.

Presentaciones similares















 To revise animals 2) To brainstorm countries where they talk Spanish 3) to revise numbers 1-31 4) To learn numbers 1 to a million 5) Play.>")




