Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Hospital Clínic de Barcelona IV Curso para Médicos Residentes, AEEH
HEPATITIS FULMINANTE (INSUFICIENCIA HEPÁTICA AGUDA GRAVE, FALLO HEPÁTICO FULMINANTE) Antoni Mas UCI del IMDM Consultor Senior Servicio Hepatología Hospital Clínic de Barcelona IV Curso para Médicos Residentes, AEEH Barcelona, Octubre 2013
 Antoni Mas. UCI del IMDM. Consultor Senior. Servicio Hepatología. Hospital Clínic de Barcelona. IV Curso para Médicos Residentes, AEEH. Barcelona, Octubre")
2
Insuficiencia Hepática Aguda Grave
DEFINICIÓN Deterioro agudo (< 26 semanas) y grave de la función hepática en un hígado previamente sano. Se caracteriza por: Ictericia Alteración de la fx hepática (TP<40%, INR1.5) Encefalopatía hepática (cualquier grado) (no exigible en niños) Elevada mortalidad espontánea (40-90%) Potencialmente reversible Mr Chairman, ladies and gentlemen, Acute liver failure is defined as an acute, life-threatening deterioration of liver function in the absence of pre-existing liver disease. The syndrome is characterized by the presence of jaundice, impairment in liver function determined by the prothrombin time, and encephalopathy, which can be a late symptom. ALF before the era of liver transplantation carried a high mortality, of up to 90%, this value has now been reduced thanks to OLT. Despite the severity of ALF, liver damage is potentially reversible by liver regeneration if the patient survives. INTERVALO ICTERICIA ENCEFALOPATIA – DIFERENTES CURSOS CLÍNICOS (fulminante/subfulminante, hiperagudo, agudo, subagudo)
 y grave de la función hepática en un hígado previamente sano. Se caracteriza por: Ictericia. Alteración de la fx hepática (TP<40%, INR1.5) Encefalopatía hepática (cualquier grado) (no exigible en niños) Elevada mortalidad espontánea (40-90%) Potencialmente reversible. Mr Chairman, ladies and gentlemen, Acute liver failure is defined as an acute, life-threatening deterioration of liver function in the absence of pre-existing liver disease. The syndrome is characterized by the presence of jaundice, impairment in liver function determined by the prothrombin time, and encephalopathy, which can be a late symptom. ALF before the era of liver transplantation carried a high mortality, of up to 90%, this value has now been reduced thanks to OLT. Despite the severity of ALF, liver damage is potentially reversible by liver regeneration if the patient survives. INTERVALO ICTERICIA ENCEFALOPATIA – DIFERENTES. CURSOS CLÍNICOS (fulminante/subfulminante, hiperagudo, agudo, subagudo)")
3
IHAG EN ESPAÑA (n=267). ETIOLOGÍA
Desconocida Otras 13.5% 32.6% 28.1% VHB Autoinmune (4.9%) Isquémica (2.2%) The etiology of ALF in Spain is unknown in a little more than one third of the patients. HBV infection is the etiology in almost another third followed by other causes such as drug toxicity. The use of anti-TB drugs, the coexistence of HBV plus HDV, Amanita phalloides poisoning and autoimmune origin make up around 18 % of the cases and the remaining etiologies are practically anecdotical. VHA (1.9%) VHC (1.9%) Paracetamol (2.2%) Amanita (3.7%) Anti-TBC (4.9%) VHB+VHD (4.1%) Liver Transplantation, 2007
 Isquémica (2.2%) The etiology of ALF in Spain is unknown in a little more than one third of the patients. HBV infection is the etiology in almost another third followed by other causes such as drug toxicity. The use of anti-TB drugs, the coexistence of HBV plus HDV, Amanita phalloides poisoning and autoimmune origin make up around 18 % of the cases and the remaining etiologies are practically anecdotical. VHA (1.9%) VHC (1.9%) Paracetamol (2.2%) Amanita (3.7%) Anti-TBC (4.9%) VHB+VHD (4.1%) Liver Transplantation,")
4
IHAG EN ESPAÑA 1992-2000 (n=267). ETIOLOGÍA
Otros fármacos Infiltración neoplásica Esteatosis embarazo Enfermedad de Wilson Desconocida 13.5% 32.6% 28.1% VHB Autoinmune (4.9%) Isquémica (2.2%) The etiology of ALF in Spain is unknown in a little more than one third of the patients. HBV infection is the etiology in almost another third followed by other causes such as drug toxicity. The use of anti-TB drugs, the coexistence of HBV plus HDV, Amanita phalloides poisoning and autoimmune origin make up around 18 % of the cases and the remaining etiologies are practically anecdotical. VHA (1.9%) VHC (1.9%) Paracetamol (2.2%) Amanita (3.7%) Anti-TBC (4.9%) VHB+VHD (4.1%) Liver Transplantation, 2007
 Isquémica (2.2%) The etiology of ALF in Spain is unknown in a little more than one third of the patients. HBV infection is the etiology in almost another third followed by other causes such as drug toxicity. The use of anti-TB drugs, the coexistence of HBV plus HDV, Amanita phalloides poisoning and autoimmune origin make up around 18 % of the cases and the remaining etiologies are practically anecdotical. VHA (1.9%) VHC (1.9%) Paracetamol (2.2%) Amanita (3.7%) Anti-TBC (4.9%) VHB+VHD (4.1%) Liver Transplantation,")
5
ETIOLOGY OF ALF IN EUROPEAN COUNTRIES
Ichai & Samuel, Liver Transpl 2008

6
ETIOLOGIA DE LA IHAG EN USA (Acute Liver Failure Study Group)
Lee et al, Hepatology 2008

7
Cambios en la etiología de la IHAG en Francia (1987-2005) (Ichai, 2008)
 (Ichai, 2008)")
8
CAMBIOS EPIDEMIOLOGICOS 1988-2010
Period 1 Period 2 Period 3 Origin, n (%): European Community (EC) Non-EC 60 (97%) 2 (3%) 260 (97%) 7 (3%) 66 (76%) 21 (24%) Etiology, n (%): Viral Toxic Unknown Other 26 (42%) 5 (8%) 27 (44%) 4 (6%) 98 (37%) 52 (19%) 86 (32%) 31 (12%) 25 (29%) 27 (31%) 14 (16%) Viral FH, n (%): HBV (±HDV) HAV Other viruses 25 (96%) 1 (4%) 86 (88%) 5 (5%) 7 (7%) 21 (84%) 3 (12%) Toxic FH, n (%): Paracetamol Non paracetamol 5 (100%) 6 (12%) 46 (88%) 8 (30%) 19 (70%)
: European Community (EC) Non-EC. 60 (97%) 2 (3%) 260 (97%) 7 (3%) 66 (76%) 21 (24%) Etiology, n (%): Viral. Toxic. Unknown. Other. 26 (42%) 5 (8%) 27 (44%) 4 (6%) 98 (37%) 52 (19%) 86 (32%) 31 (12%) 25 (29%) 27 (31%) 14 (16%) Viral FH, n (%): HBV (±HDV) HAV. Other viruses. 25 (96%) 1 (4%) 86 (88%) 5 (5%) 7 (7%) 21 (84%) 3 (12%) Toxic FH, n (%): Paracetamol. Non paracetamol. 5 (100%) 6 (12%) 46 (88%) 8 (30%) 19 (70%)")
9
IHAG EN ESPAÑA 1992-2000. CARACTERISTICAS AL INGRESO
Centros participantes: 15 (población atendida 21.6 millones) Número de casos: 267 (varones 44%) Edad media: años (el 57% < 40 años) Curso: 63 % fulminante, 32 % subfulminante 43 % hiperagudo, 40% agudo, 17 % subagudo Grado de encefalopatia: 0 (7.5 %), I (39.3 %), II (25.5 %), III (16.5 %), IV (10.9 %) Liver Transplantation, 2007
 Número de casos: 267 (varones 44%) Edad media: años (el 57% < 40 años) Curso: 63 % fulminante, 32 % subfulminante. 43 % hiperagudo, 40% agudo, 17 % subagudo. Grado de encefalopatia: 0 (7.5 %), I (39.3 %), II (25.5 %), III (16.5 %), IV (10.9 %) Liver Transplantation,")
10
Diagnóstico etiológico en la IHAG
Valor pronóstico -VHA o paracetamol supervivencia >50% - Wilson, fármacos mortalidad % Tratamientos especificos Indicaciones específicas de Trasplante hepático (y contraindicaciones) Interés académico, epidemiológico, detección de nuevas causas,...
 Interés académico, epidemiológico, detección de nuevas causas,...")
11
IHAG. PRONÓSTICO SEGÚN ETIOLOGIA
Lee W, 2012

12
IHAG. PRONÓSTICO SEGÚN ETIOLOGIA
Lee W, 2012

13
Exploraciones a realizar en la IHAG
Historia clínica y exploración física Pruebas standard de función hepática Serologías virales: virus hepatotropos, CMV, EBV, HSV, Parvovirus... Inmunologia: Autoanticuerpos Tóxicos: paracetamol, amanitinas Metabolismo del Cu Evaluación cardiorespiratoria Pruebas de imagen (ecografía-doppler) Hematología: anemia hemolítica, plaquetopenia,.. Biopsia hepática (vía transyugular) DIAGNÓSTICO, ETIOLOGIA, INDICACIÓN DE TRATAMIENTO ESPECÍFICO, VALORACION DE TRASPLANTE URGENTE
 Hematología: anemia hemolítica, plaquetopenia,.. Biopsia hepática (vía transyugular) DIAGNÓSTICO, ETIOLOGIA, INDICACIÓN DE TRATAMIENTO ESPECÍFICO, VALORACION DE TRASPLANTE URGENTE.")
14
Necrosis masiva Zona central Zona portal

15
IHAG por Linfoma difuso B
CD 20

16
Diagnóstico etiológico en la IHAG
Diagnóstico etiológico en la IHAG. Ejemplos basados en datos clínico-analíticos Dolor abdominal, hepatomegalia, ascitis: S. de Budd-Chiari agudo Anemia hemolítica Coombs -, individuo joven, Ratio FA/Bil, GPT poco altas: Enf. de Wilson Fiebre muy alta, GPT extraordinariamente elevadas: Infección por HSV o VZH Curso subfulminante, ingesta de fármacos nuevos en los 2-3 meses previos, fiebre, eosinofilia: IHAG por hipersensibilidad Cuadro diarreico, fase de quiescencia, deterioro de función hepática y renal: Amanita phalloides

17
Por qué es tan importante enviar al paciente a un centro de trasplante hepático?
Existen medios para establecer el diagnóstico etiológico Permite la aplicación de tratamientos específicos dirigidos al hígado Permite evaluar e iniciar un posible TOH Benhamou: En la IHAG, el hígado falla antes de que aparezca la encefalopatía. Wendon: Debe considerarse la encefalopatía como un síntoma tardio de la IHAG. Once the diagnosis has been established, the patient should be referred to a liver unit to allow a definite etiological diagnosis, to initiate specific treatments and evaluate the criteria for possible OLT. Remember, the liver fails before encephalopathy,… and encephalopathy should be considered as a late symptom of ALF.

18
CRITERIA FOR IMMEDIATE TRANSFER TO A LIVER UNIT WITH OLT FACILITIES IN PATIENTS WIH ACUTE LIVER DISEASE (NON-P) AND COAGULOPATHY WITHOUT HE PT % - Children < 15 years - Adults > 40 years and unfavorable etiology - Fever > 38 ºC or uncommon etiology - Postoperative - Pregnancy - ALD superimposed on chronic liver disease - Comorbidities: diabetes mellitus, HIV infection, previous cured cancer, malaria, severe ARF - Hyperbilurrubinemia > 250 umol/L PT < 30 % - Any patient (especially if age > 40 years or unfavorable etiology) Bernuau et al, J Hepatol, 2009
 Bernuau et al, J Hepatol,")
19
COMPLICACIONES EXTRAHEPÁTICAS DE LA IHAG
Insuficiencia renal aguda Insuficiencia circulatoria Alteraciones metabólicas Coagulopatía SIRS / Sepsis (bacteriana y/o fúngica) Hipertensión intracraneana COMPLICACIONES EXTRAHEPÁTICAS And what about new developments in the treatment of extrahepatic complications of ALF? which may be acute renal…..
 Hipertensión intracraneana. COMPLICACIONES. EXTRAHEPÁTICAS. And what about new developments in the treatment of extrahepatic complications of ALF which may be acute renal…..")
20
TRATAMIENTO ETIOLÓGICO DE LA IHAG
Parar cualquier fármaco !!! N-acetilcisteína (sobredosis de paracetamol) Provocar el parto (esteatosis aguda del embarazo) Corticoides (hepatitis autoinmune) Antídotos en la intoxicación por Amanita Phalloides Aciclovir si se sospecha infección por herpes virus Antivirales orales en la reactivación de una infección crónica por VHB (e incluso en la primoinfección) D-penicilamina y recambio plasmático en la enfermedad de Wilson ¡¡¡PRECOCIDAD (ANTES EH) FUNDAMENTAL !!!
 Provocar el parto (esteatosis aguda del embarazo) Corticoides (hepatitis autoinmune) Antídotos en la intoxicación por Amanita Phalloides. Aciclovir si se sospecha infección por herpes virus. Antivirales orales en la reactivación de una infección crónica por VHB (e incluso en la primoinfección) D-penicilamina y recambio plasmático en la enfermedad de Wilson. ¡¡¡PRECOCIDAD (ANTES EH) FUNDAMENTAL !!!")
21
TRATAMIENTO ETIOLÓGICO DE LA IHAG Restauración del drenaje hepático
Conseguir la estabilidad hemodinámica en el shock (como causa de IHAG). QTA en caso de infiltración neoplásica masiva. TIPS precoz en el síndrome de Budd-Chiari agudo. Restauración del drenaje hepático TIPS
. QTA en caso de infiltración neoplásica masiva. TIPS precoz en el síndrome de Budd-Chiari agudo. Restauración del drenaje hepático. TIPS.")
22
Supervivencia Espontánea
Intravenous NAC Improves Spontaneous Survival in Early Stage Non-Acetaminophen ALF AASLD 2007 % 25 50 75 100 Supervivencia Espontánea (sin trasplante) Supervivencia Global Serie Global n=173 EH I-II n=114 EH III-IV n=59 70% 66% 40% 27% 52% 30% 9% 22% p=0.02 NS NAC Controles Lee, AASLD 2007
 Supervivencia. Global. Serie Global. n=173. EH I-II. n=114. EH III-IV. n=59. 70% 66% 40% 27% 52% 30% 9% 22% p=0.02. NS. NAC. Controles. Lee, AASLD")
23
Larsen et al, Curr Op Crit Care 2011

24
EL DILEMA DEL TOH URGENTE EN LA IHAG
DEMASIADO PRONTO (TOO EARLY) Situación reversible (restitutio ‘ad integrum’ en los supervivientes) Gasto innecesario de un órgano, útil para otro paciente Nueva enfermedad (por los inmunosupresores) DEMASIADO TARDE (TOO LATE) Paciente con sepsis incontrolable, shock, con lesiones cerebrales irreversibles,... Gasto innecesario de un órgano, útil para otro paciente
 Situación reversible (restitutio ‘ad integrum’ en los supervivientes) Gasto innecesario de un órgano, útil para otro paciente. Nueva enfermedad (por los inmunosupresores) DEMASIADO TARDE (TOO LATE) Paciente con sepsis incontrolable, shock, con lesiones cerebrales irreversibles,... Gasto innecesario de un órgano, útil para otro paciente.")
25
The old OLT criteria for ALF (80’s)
proceed with OLT when three expert hepatologists consider that the patient will die without an urgent trasplant The newest comment about OLT criteria for ALF (O’ Grady, Postgrad. Course, EASL, 2010) in most programms, a pragmatic case by case evaluation of the risk/benefit profile is employed
 in most programms, a pragmatic case by case evaluation of the risk/benefit profile is employed.")
26
SUPERVIVENCIA EN LA IHAG SEGUN CRITERIOS DE TOH URGENTE
No criterios de TOH n=55 Criterios de TOH n=212 Muerte en lista n=11 Contraindicado n=51 Trasplantados n=150 Vivos Sobrevida 47 86% 0% 4 8% 104 69%

27
Hospital Clínic Trasplante Hepático Supervivencia comparativa de pacientes s/ indicación principal m e s 1 2 8 9 6 4 7 3 . p = 0.03 p = 0.02 p = 0.03 colestásicas hepatocelulares insuficiencia hepática aguda grave

28
IHAG Y TRASPLANTE HEPATICO URGENTE ALTERNATIVAS AL TRASPLANTE CONVENCIONAL
Trasplante auxiliar: más complejo, problemas técnicos, pero evita inmunosupresión de por vida Trasplante de donante vivo: rapidez en la evaluación del donante, problemas éticos, básicamente pediátrico, útil en países con largo tiempo de espera Sistemas de soporte hepático artificial o bioartificial Trasplante de hepatocitos

29
Results of CoPrimary endpoint Transplant free survival / Etiology (ITT analysis)
Non Paracetamol Paracetamol 85.0% 68.5% Saliba 2008

30
Predictive factors of survival free of transplantation Results of the multivariate analysis
RR IC95 p MELD score < 40 7.6 0.001 Treatment with MARS® ≥ 3 sessions 6.3 0.01 Fibrinogen (normal or high) 3.2 Saliba 2009
 Saliba")
31
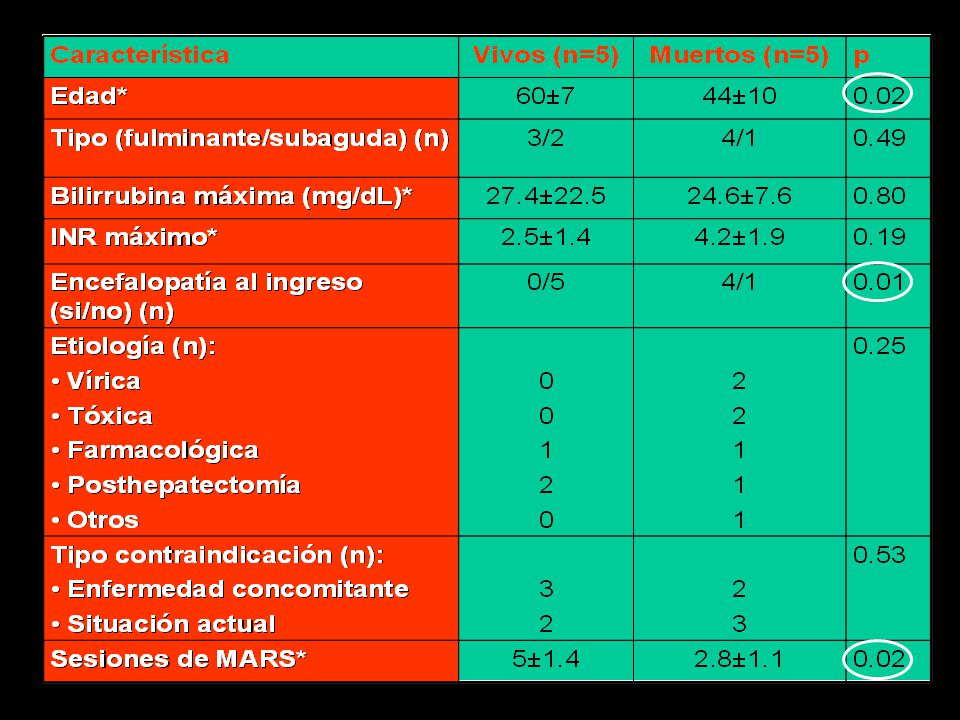
MARS EN INSUFICIENCIA HEPÁTICA AGUDA GRAVE Y
CONTRAINDICACIONES PARA EL TRASPLANTE EXPERIENCIA HOSPITAL CLÍNIC

33
MENSAJES IMPORTANTES PARA RECORDAR
INSUFICIENCIA HEPÁTICA AGUDA GRAVE: El cuadro más grave de la Hepatología Importancia de la etiología (pronóstico, tratamiento) Intervalo ictericia-encefalopatía Aparición muy frecuente de problemas extrahepáticos, causa frecuente de muerte El trasplante hepático urgente ha modificado su pésimo pronóstico Traslado urgente a un centro de trasplante hepático Existen alternativas al trasplante convencional que en el futuro quizás consigan evitarlo
 Intervalo ictericia-encefalopatía. Aparición muy frecuente de problemas extrahepáticos, causa frecuente de muerte. El trasplante hepático urgente ha modificado su pésimo pronóstico. Traslado urgente a un centro de trasplante hepático. Existen alternativas al trasplante convencional que en el futuro quizás consigan evitarlo.")
34
In ALF, Work quickly Stay paranoid Expect the worst
Lee, Postgraduate Course, AASLD 2009

Presentaciones similares











. Protocolo de actuación H.C.Bidasoa>")







