Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Quimioterapia en Cáncer de Colon y Recto
Dra. Mayté Lima Pérez Servicio de Oncología Hospital C.Q. “Hnos. Ameijeiras”

2
INTRODUCCION ► A nivel mundial, el CCR es la tercera causa de cáncer
( nuevos casos/año). ► En Europa y USA, el CCR es la segunda causa de cáncer en mortalidad ( y /año, respectivamente). ► En Cuba, es la cuarta en incidencia y mortalidad y la SV a 5 años (poblacional) está por debajo del 40%. ► En Cuba, más del 70% de los casos se presentan en etapas III y IV.
. ► En Europa y USA, el CCR es la segunda causa de cáncer en mortalidad ( y /año, respectivamente). ► En Cuba, es la cuarta en incidencia y mortalidad y la. SV a 5 años (poblacional) está por debajo del 40%. ► En Cuba, más del 70% de los casos se presentan en. etapas III y IV.")
3
CCR: Estadios al Diagnóstico
Only 38% of CRC cases are diagnosed early, in stages I and II. This reflects the often asymptomatic nature of early disease. The majority of CRC cases (57%) are diagnosed in later disease stages. Thirty-eight percent are diagnosed with regional, stage III disease, and 19% with distant metastases (stage IV). Five percent of CRC cases are unstaged. Localizado (Estadio I-II) Regional (Estadio III) A Distancia (Estadio IV) No estadiable National Cancer Institute. Available at: Accessed June 2005. National Cancer Institute. SEER Cancer Statistics Review, Available at: csr/1975_2002/. Accessed June 2005.
 are diagnosed in later disease stages. Thirty-eight percent are diagnosed with regional, stage III disease, and 19% with distant metastases (stage IV). Five percent of CRC cases are unstaged. Localizado. (Estadio I-II) Regional. (Estadio III) A Distancia. (Estadio IV) No estadiable. National Cancer Institute. Available at: Accessed June National Cancer Institute. SEER Cancer Statistics Review, Available at: csr/1975_2002/. Accessed June")
4
Supervivencia 5 años por Estadio Clínico
The 5-year survival rate for patients with CRC is 63%. This is dependent on the stage of disease at presentation. While only 38% of all patients with CRC are identified with localized stage I or II disease, 5-year survival for these patients is 90%. Five-year survival rates drop to 67% with involvement of adjacent organs or lymph nodes in stage III disease. Five-year survival is as low as 10% in patients with stage IV disease with both nodal and metastatic involvement. The changing landscape of first- and second-line therapies for metastatic disease offers increased potential for prolonged survival in such patients. With newer and more sophisticated diagnostic/imaging techniques in CRC, the number of patients diagnosed with early CRC may improve the overall 5-year survival rate for these patients. National Cancer Institute. Available at: Accessed June 2005. National Cancer Institute. SEER Cancer Statistics Review, Available at: Accessed June 2005.

5
Tratamiento Adyuvante del CCR
5-FU/LV superior a 5-FU/Lev 6- y 12-meses tratamiento equivalente Lev innecesario Altas- y Bajas-dosis LV equivalente Mensual o semanalmente son equivalentes Capecitabina es tan efectiva al 5-FU/LV en bolo 5-FU/Lev superior a Cirugía sola LV5FU2 mensualmente IC y bolo equivalentes 5-FU/LV superior a Cirugía sola FOLFOX4 superior a 5-FU/LV Until 2004, 5-FU modulated by LV was the mainstay chemotherapeutic agent available for the adjuvant treatment of colon cancer. The Intergroup 0035 trial demonstrated that the addition of levamisole to a 5-FU regimen in the adjuvant setting reduced 5-year survival by 13% over surgery alone.1 5-FU/LV was evaluated relative to observation in the adjuvant setting for patients with stage II or III colon cancer and found to achieve a 44% relative reduction in recurrence and a 39% reduction in death rate.2 Two adjuvant trials, National Surgical Adjuvant Breast and Bowel Project (NSABP) C04 and Intergroup 0089, investigated the relative efficacy of 5-FU with LV alone, 5-FU with levamisole alone, and 5-FU with LV and levamisole. Overall, the results of these trials suggest that LV may be a more effective modulator of 5-FU than levamisole; however, the trial results were not statistically significant. LV was shown to be effective over shorter (6- to 8- vs 12-month) regimens, and the addition of levamisole to a 5-FU/LV regimen did not have an additive effect. With 5-FU/LV, high and low doses as well as monthly vs weekly treatments were shown to be comparable.3,4 In late 2004, the MOSAIC Phase III trial demonstrated that FOLFOX4 therapy significantly improved disease-free survival (DFS) in patients with completely resected stage II or III colon cancer relative to 5-FU/LV (75.9% vs 69.1%, P=.0008). A statistically significant improvement in DFS was noted in stage III patients (69.7% vs 61.0%, P=.002), but not in stage II patients. 1990 1994 1998 2000 2002 2004 Andre et at. N Engl J Med. 2004;350:2343. Andre et al. Proc Am Soc Clin Oncol. 2002;21:133a. Abstract 529. Francini et al. Gastroenterology. 1994;106:899. Haller et al. Proc Am Soc Clin Oncol. 1998;17:256a. Abstract 982. Moertel et al. Ann Intern Med. 1995;122:321. O’Connell et al. J Clin Oncol. 1998;16:295. Wolmark et al. Proc Am Soc Clin Oncol. 1996;15:205. Abstract 460. Laurie et al. J Clin Oncol. 1989;7:1447. Francini et al. Gastroenterology. 1994;106:899. Wolmark et al. J Clin Oncol. 1999;17:3553. Haller et al. Proc Am Soc Clin Oncol. 1998;17:256a. Abstract 982.
 C04 and Intergroup 0089, investigated the relative efficacy of 5-FU with LV alone, 5-FU with levamisole alone, and 5-FU with LV and levamisole. Overall, the results of these trials suggest that LV may be a more effective modulator of 5-FU than levamisole; however, the trial results were not statistically significant. LV was shown to be effective over shorter (6- to 8- vs 12-month) regimens, and the addition of levamisole to a 5-FU/LV regimen did not have an additive effect. With 5-FU/LV, high and low doses as well as monthly vs weekly treatments were shown to be comparable.3,4. In late 2004, the MOSAIC Phase III trial demonstrated that FOLFOX4 therapy significantly improved disease-free survival (DFS) in patients with completely resected stage II or III colon cancer relative to 5-FU/LV (75.9% vs 69.1%, P=.0008). A statistically significant improvement in DFS was noted in stage III patients (69.7% vs 61.0%, P=.002), but not in stage II patients Andre et at. N Engl J Med. 2004;350:2343. Andre et al. Proc Am Soc Clin Oncol. 2002;21:133a. Abstract 529. Francini et al. Gastroenterology. 1994;106:899. Haller et al. Proc Am Soc Clin Oncol. 1998;17:256a. Abstract 982. Moertel et al. Ann Intern Med. 1995;122:321. O’Connell et al. J Clin Oncol. 1998;16:295. Wolmark et al. Proc Am Soc Clin Oncol. 1996;15:205. Abstract 460. Laurie et al. J Clin Oncol. 1989;7:1447. Francini et al. Gastroenterology. 1994;106:899. Wolmark et al. J Clin Oncol. 1999;17:3553. Haller et al. Proc Am Soc Clin Oncol. 1998;17:256a. Abstract 982.")
6
Qué debe tratarse????? Escenario en Adyuvancia
Escenario en Enfermedad Metastásica

7
Avances en el Tratamiento Cáncer de Colon
A pesar del tratamiento quirúrgico correcto: el 30% de los pacientes en Estadio II el 60% de los pacientes en Estadio III, van a fallecer por diseminación tumoral.

8
Qué ha sucedido en el escenario de la Adyuvancia????

9
Tratamiento Adyuvante: SLE Variable Principal
18 Ensayos de 20,898 pacientes en estadios II y III de cáncer de colon 80% de las recurrencias ocurre a los tres años de la resección. SLE a los tres años se correlaciona con SG a los 5 años. La SLE es la variable principal para evaluar las nuevas terapias en el escenario adyuvante A combined analysis of 39 adjuvant treatment arms from 17 trials of 5-FU–based regimens used as adjuvant therapy, resulting in a total population of 17,367 patients with stage II or III colon cancer, determined that 3-year DFS is an appropriate surrogate end point for survival in the adjuvant setting. In this analysis, 74% of the recurrences that occurred over an 8-year interval occurred within the first 3 years following resection. Three-year DFS correlated with 5-year OS (r=0.90). Sargent et al. J Clin Oncol. 2005;23:8664. Sargent et al. ASCO Abstract At: _ _ ,00.asp. Accessed November 2004.
. Sargent et al. J Clin Oncol. 2005;23:8664. Sargent et al. ASCO Abstract At: _ _ ,00.asp. Accessed November")
10
CCR: Tratamiento adyuvante
Supervivencia Global a 5 años Estadío I Estadío II Estadío III Estadío IV 85–95% 60–80% 30–60% <5% SG: 8% (5–19%) SLR: 9% (7–16%) Beneficio absoluto (3–5 años) Recurrencia: 16–35% Mortalidad: 12–22% Beneficio relativo: índice de riesgo (3–5 años) Adapted from O’Connell In: ASCO Educational Book 1994
 SLR: 9% (7–16%) Beneficio absoluto (3–5 años) Recurrencia: 16–35% Mortalidad: 12–22% Beneficio relativo: índice de riesgo (3–5 años) Adapted from O’Connell In: ASCO Educational Book")
11
Cambios en el Tratamiento adyuvante del cáncer colorectal
Qué avances en el tratamiento del CCR m se pueden aplicar a las etapas tempranas? Así curaremos más pacientes en estadios II/III del cáncer de colon?

12
EFC3313 (MOSAIC) Adjuvante
FOLFOX: Tratamiento Efectivo en todas las situaciones del Cáncer Colorectal EstadíoII/III EFC3313 (MOSAIC) Adjuvante EstadíoIV N9741 1ra Línea EFC4584 segunda-línea EFC4760 3ra Línea 23% reducción del riesgo de recaída SG:19.5 m SLE: 8.7 m RR: 45% SG: 9.8 m SLE: 5.6 m RR: 9.6% Mejoría Síntomas 28% SLE: 4.6 m RR: 12% Mejoría Síntomas 30% Goldberg R, et al. J Clin Oncol 2004;22:23-30; Rothenberg M, et al. J Clin Oncol 2003;11: ; de Gramont A, Proc Am Soc Clin Oncol 2003;22:253 (abst 1015)
 Adjuvante. EstadíoIV. N9741 1ra Línea. EFC4584 segunda-línea. EFC4760 3ra Línea. 23% reducción. del riesgo. de recaída. SG:19.5 m. SLE: 8.7 m. RR: 45% SG: 9.8 m. SLE: 5.6 m. RR: 9.6% Mejoría Síntomas. 28% SLE: 4.6 m. RR: 12% Mejoría. Síntomas 30% Goldberg R, et al. J Clin Oncol 2004;22:23-30; Rothenberg M, et al. J Clin Oncol 2003;11: ; de Gramont A, Proc Am Soc Clin Oncol 2003;22:253 (abst 1015)")
13
Avances en el Tratamiento del Cáncer de Colon
Redución de 10% en el riesgo de muerte a los 5 años. Aumento supervivencia a los 5 años de 2,3 %. Supervivencia mayor en aquellos pacientes con tratamiento durante más de un año. 5-FU monoquimioterapia: Meta-análisis JAMA 1988 (n= 4700 pacientes)
")
14
NSABP C-07 – SLE superior estadío III Oxaliplatino adyuvante
Probabilidad Estimada 4- años DFS (%) 73.2 67.0 2 3 1 4 0.0 0.2 0.4 0.6 0.8 1.0 Años FLOX (n=1 200) 5-FU/LV (n=1 207) Diferencia Absoluta a 4 años: 6.2% HR=0.80 (95% CI: 0.66–0.93) p= Kuebler et al. J Clin Oncol 2007 Kuebler et al. Oxaliplatin Combined With Weekly Bolus Fluorouracil and Leucovorin As Surgical Adjuvant Chemotherapy for Stage II and III Colon Cancer: Results From NSABP C-07. J Clin Oncol. 2007;25(16):2198–2204. Reprinted with permission from the American Society of Clinical Oncology. 14
 Años. FLOX (n=1 200) 5-FU/LV (n=1 207) Diferencia Absoluta. a 4 años: 6.2% HR=0.80 (95% CI: 0.66–0.93) p= Kuebler et al. J Clin Oncol 2007 Kuebler et al. Oxaliplatin Combined With Weekly Bolus Fluorouracil and Leucovorin As Surgical Adjuvant Chemotherapy for Stage II and III Colon Cancer: Results From NSABP C-07. J Clin Oncol. 2007;25(16):2198–2204. Reprinted with permission from the American Society of Clinical Oncology. 14.")
15
MOSAIC – S Global superior Oxaliplatino adyuvante Estadío III
Probabilidad Estimada 6-años OS (%) 73.0 68.6 1.0 FOLFOX4 (n=672) LV5FU2 (n=675) 0.8 0.6 Diferencia Absoluta a 6 años : 4.4% 0.4 0.2 HR=0.80 (95% CI: 0.66–0.98) p=0.0029 0.0 2 4 6 8 Años de Gramont et al. ASCO 2007 15
 FOLFOX4 (n=672) LV5FU2 (n=675) Diferencia Absoluta. a 6 años : 4.4% HR=0.80 (95% CI: 0.66–0.98) p= Años. de Gramont et al. ASCO")
16
Beneficio del oxaliplatino
C-07 y Mosaic Beneficio del oxaliplatino 5y S Δ HR C-07 80.3 % 2.0 % 0.85 Mosaic 81.3 % 2.2 %

17
MOSAIC Update: SG 6 años de seguimiento
1.0 p=0.996 0.9 0.1% 0.8 p=0.029 0.7 4.4% 0.6 Probabilidad 0.5 0.4 HR [95% CI] Estadío II [0.71–1.42] Estadío III [0.66–0.98] FOLFOX4 stage II LV5FU2 stage II FOLFOX4 stage III LV5FU2 stage III 0.3 0.2 0.1 6 12 18 24 30 36 42 48 54 60 66 72 78 84 90 96 Sobrevida Global (meses) ASCO 2007
 ASCO")
18
Conclusiones: MOSAIC FOLFOX4 es la primera combinación que demuestra superioridad sobre 5-FU/LV en adyuvancia del cáncer de colon (SLE 3 años: 78.2% vs 72.9%) Reducción del riesgo de recurrencia de un 23% (p=0.002)
 Reducción del riesgo de recurrencia de un 23% (p=0.002)")
19
Tratamiento Adyuvante del Cáncer de Colon en los Estadios II: ¿Qué Pacientes Tratar?.

20
Cáncer de Colon: Estadio II Grupo Heterogéneo
28% pacientes con CC diagnosticados 25–30% de los pacientes estadios II recurren en 5 años IIA: T3 N0 M0 IIB: T4 N0 M0 Supervivencia Libre de Enfermedad a 5 años IIA: 65–73% IIB: 51–60% AJCC Cancer Staging Manual 2002 Gill et al. J Clin Oncol 2004 20

21
¿Qué enfermos tratar (I)?
El beneficio para el paciente en estadio II existe. Globalmente el beneficio es limitado 3-4 pacientes de cada 100. Necesitamos identificar los subgrupos con peor pronóstico y que puedan beneficiarse realmente del tratamiento complementario.

22
Factores Pronósticos Clásicos
Perforación. Oclusión. Componente mucinoso > 50%. G3. Invasión venosa intramural. CEA preoperatorio elevado.

23
Estudios relevantes PRO Metaanálisis NSABP Gill (ASCO 2003)
NACCP trial CONTRA Meta-análisis IMPACT SEER-Medicare (Scharg). INT 0035 Trial
. INT 0035 Trial.")
24
MOSAIC –Estadío II. No beneficio SG
6-años SG (%) Probabilidad Estimada 1.0 FOLFOX4 (n=451) LV5FU2 (n=448) 86.8 0.8 0.6 HR=1.00 (95% CI: 0.71–1.42) 0.4 0.2 0.0 1 2 3 4 5 6 7 8 Años de Gramont et al. ASCO 2007 24
 Probabilidad Estimada FOLFOX4 (n=451) 86.9 LV5FU2 (n=448) HR=1.00 (95% CI: 0.71–1.42) Años. de Gramont et al. ASCO")
25
MOSAIC –Incremento SLE 7.2% en Estadío II de “alto riesgo”
5-años SLE (%) Probabilidad Estimada 1.0 FOLFOX4 (n=286) LV5FU2 (n=290) 74.9 0.8 Ganancia Absoluta : 7.2% 0.6 HR=0.74 (95% CI: 0.52–1.06) 0.4 0.2 0.0 1 2 3 4 5 6 Años de Gramont et al. ASCO 2007 25
 Probabilidad Estimada FOLFOX4 (n=286) 82.1 LV5FU2 (n=290) Ganancia Absoluta : 7.2% 0.6. HR=0.74 (95% CI: 0.52–1.06) Años. de Gramont et al. ASCO")
26
Factores Pronósticos Emergentes
DNA Aneuploide. Micrometástasis en ganglios por PCR. Niveles TS. Sobreexpresión de p53. Alteración 18q (DCC). Inestabilidad de microsatélite.
. Inestabilidad de microsatélite.")
27
Preguntas en Adyuvancia
Es útil la QT Adyuvante? Sí Cuál es el mejor Esquema? FOLFOX Cuál Estadío recibe adyuvancia? Estadío III y Estadío II de Alto Riesgo Cuál es el futuro? Nuevos fármacos, agentes dianas, farmacogenómica (ECOG 5202,18q, MSI)?
")
28
Escenario Metastásico
Qué Hacer???? Es siempre operable el primario????? Qué hacer con las metástasis hepáticas???

29
Los pacientes no tratados con lesiones metastásicas hepáticas tienen una mediana de supervivencia meses 15-35% sobrevive 1 año 27% si las lesiones están en un lóbulo o segmento 60% metástasis únicas 29

30
“Historia Natural” después de la Resección Hepática
1.0 Resección R0 (n = 473) SLE Resección R1/2 (n = 72) 0.8 0.6 43.6 m 41% (159) Probabilidad de supervivencia 0.4 29% (60) 26.8 m 35% (137) 14.2 m 0.2 28% (57) vs. p < 0.001 0.0 2 4 6 8 10 Mortalidad operatoria excluida años de resección hepática Scheele J et al Surg Oncol Clin N Amer 2003 30
 SLE. Resección R1/2 (n = 72) m. 41% (159) Probabilidad de supervivencia % (60) 26.8 m. 35% (137) 14.2 m % (57) vs. p < Mortalidad operatoria excluida. años de resección hepática. Scheele J et al Surg Oncol Clin N Amer")
31
Era Moderna: Resecciones Hepáticas
Mortalidad % Supervivencia (años) Mediana Autor # Pac Operatoria (meses) Scheele, ‘ % Nordlinger, ‘ % Jenkins, ‘ % Jamison, ‘ % Fong, ‘ % Choti, ’ % Fernández, ’ % NR Elias, ’ % Pawlik, ’ % Wei, ’ % 31
 Mediana. Autor # Pac Operatoria (meses) Scheele, ‘ % Nordlinger, ‘ % Jenkins, ‘ % Jamison, ‘ % Fong, ‘ % Choti, ’ % Fernández, ’ % NR. Elias, ’ % Pawlik, ’ % Wei, ’ %")
32
Candidatos para Resecciones Quirúrgicas
Ausencia de Enfermedad extrahepática no resecable No invasión vascular bilobular Márgenes de resección negativos Reserva hepática adecuada > 20-25% volumen residual funcional Problema: Solo % de los pacientes con metástasis hepáticas son candidatos para resección hepática Aproximadamente 120,000/año mundo 32

33
Historia de los Regímenes Terapéuticos en el Tratamiento de CCR m
25+ 24 ~15-20 ~15-17 18 ~12-14 ~11-12 Mediana SG (meses) 12 ~4-6 6 KEY POINT: With the current chemotherapeutic armamentarium, patients with mCRC may live an average of 15 to 20 months. 1980s 2000s 1990s 1960s ADDITIONAL INFORMATION Combination therapy with multiple agents may increase the efficacy of mCRC treatment. First-line treatment of mCRC: key milestones 1985: Addition of leucovorin (LV) to 5-FU therapy 2000: Addition of irinotecan to IV 5-FU/LV shows survival advantage over IV 5-FU/LV alone. 2004: Intergroup trial N9741 finds FOLFOX (oxaliplatin, folinic acid, 5-fluorouracil) superior to bolus irinotecan/5-FU/LV (IFL). 2004: Exposure to all active agents is associated with increased survival. 2004: Biologics approved for treatment. Avastin in first-line treatment Cetuximab in irinotecan-refractory patients Before the 1960s, patients with untreated mCRC had a median OS of only 4 to 6 months.1 With the introduction of 5-FU treatment, survival of these patients was extended to approximately 1 year. 5-FU has continued to be a mainstay of anticancer therapy.2 The addition of the biomodulator LV in the 1980s improved survival rates 2 to 3 months more than 5-FU therapy alone.3 Irinotecan was initially approved as a second-line treatment for patients with mCRC in 1996 and was later approved as a first-line treatment in Irinotecan therapy in addition to 5-FU–containing chemotherapy further extended survival of patients with mCRC.5,6 Capecitabine was the first oral agent approved for the treatment of mCRC, in Capecitabine had been approved previously for the treatment of metastatic breast cancer (MBC) in Oxaliplatin was initially approved for use in the United States in 2002 and is currently approved in both the first- and second-line settings,8-10 With the current chemotherapeutic armamentarium, patients with mCRC may live an average of 15 to 20 months.8,9 Cetuximab, an antiepidermal growth factor receptor monoclonal antibody (mAb), was approved by the United States Food and Drug Administration for use in patients with mCRC in Upon its approval in 2004, Avastin became the first antiangiogenic agent for first-line treatment of patients with mCRC.12 Currently the armamentarium of approved chemotherapies for mCRC includes 4 different agents.13 5-FU is a fluoropyrimidine, which upon conversion to its active metabolite (fluorodeoxyuridine monophosphate) inhibits thymidylate synthase, preventing pyrimidine and therefore DNA synthesis. 5-FU may be given with or without the biomodulator LV. Capecitabine is an oral fluoropyrimidine prodrug converted into 5-FU by thymidine phosphorylase. Irinotecan (CPT-11) is a topoisomerase I inhibitor. Oxaliplatin is a third-generation platinum analog that induces DNA crosslinks and results in apoptosis. Various combinations of these chemotherapeutic agents are commonly used.13 Panitumumab was approved in September 2006 for the treatment of EGFR-expressing mCRC with disease progression on or following fluoropyrimidine-, oxaliplatin-, and irinotecan-containing chemotherapy regimens.14 5-FU 5-FU biomodulación Irinotecan Oxaliplatino Cetuximab Bevacizumab Panitumumab REFERENCES Scheithaurer et al. Br Med J. 1993;306:752. Poon et al. J Clin Oncol. 1989;7:1407; Camptosar® (irinotecan) PI. July 2005. Petrelli et al. J Clin Oncol. 1989:7:1419. Saltz et al. N Engl J Med. 2000:343:905. Douillard et al. Lancet. 2000:355:1041. Xeloda® (capecitabine) PI. April 2003. Goldberg et al. J Clin Oncol. 2004;22:23. de Gramont et al. J Clin Oncol. 2000;18:2938. Eloxatin™ (oxaliplatin) PI. April 2005; Erbitux™ (cetuximab) PI. June 2004. Avastin® (bevacizumab) PI. June 2006. Vectibix™ (panitumumab) PI. September 2006. NCCN. Clinical Practice Guidelines in Oncology: Colon Cancer. v 33
 12. ~ KEY POINT: With the current chemotherapeutic armamentarium, patients with mCRC may live an average of 15 to 20 months. 1980s. 2000s. 1990s. 1960s. ADDITIONAL INFORMATION. Combination therapy with multiple agents may increase the efficacy of mCRC treatment. First-line treatment of mCRC: key milestones. 1985: Addition of leucovorin (LV) to 5-FU therapy. 2000: Addition of irinotecan to IV 5-FU/LV shows survival advantage over IV 5-FU/LV alone. 2004: Intergroup trial N9741 finds FOLFOX (oxaliplatin, folinic acid, 5-fluorouracil) superior to bolus irinotecan/5-FU/LV (IFL). 2004: Exposure to all active agents is associated with increased survival. 2004: Biologics approved for treatment. Avastin in first-line treatment. Cetuximab in irinotecan-refractory patients. Before the 1960s, patients with untreated mCRC had a median OS of only 4 to 6 months.1. With the introduction of 5-FU treatment, survival of these patients was extended to approximately 1 year. 5-FU has continued to be a mainstay of anticancer therapy.2. The addition of the biomodulator LV in the 1980s improved survival rates 2 to 3 months more than 5-FU therapy alone.3. Irinotecan was initially approved as a second-line treatment for patients with mCRC in 1996 and was later approved as a first-line treatment in Irinotecan therapy in addition to 5-FU–containing chemotherapy further extended survival of patients with mCRC.5,6. Capecitabine was the first oral agent approved for the treatment of mCRC, in Capecitabine had been approved previously for the treatment of metastatic breast cancer (MBC) in Oxaliplatin was initially approved for use in the United States in 2002 and is currently approved in both the first- and second-line settings,8-10. With the current chemotherapeutic armamentarium, patients with mCRC may live an average of 15 to 20 months.8,9. Cetuximab, an antiepidermal growth factor receptor monoclonal antibody (mAb), was approved by the United States Food and Drug Administration for use in patients with mCRC in Upon its approval in 2004, Avastin became the first antiangiogenic agent for first-line treatment of patients with mCRC.12. Currently the armamentarium of approved chemotherapies for mCRC includes 4 different agents FU is a fluoropyrimidine, which upon conversion to its active metabolite (fluorodeoxyuridine monophosphate) inhibits thymidylate synthase, preventing pyrimidine and therefore DNA synthesis. 5-FU may be given with or without the biomodulator LV. Capecitabine is an oral fluoropyrimidine prodrug converted into 5-FU by thymidine phosphorylase. Irinotecan (CPT-11) is a topoisomerase I inhibitor. Oxaliplatin is a third-generation platinum analog that induces DNA crosslinks and results in apoptosis. Various combinations of these chemotherapeutic agents are commonly used.13. Panitumumab was approved in September 2006 for the treatment of EGFR-expressing mCRC with disease progression on or following fluoropyrimidine-, oxaliplatin-, and irinotecan-containing chemotherapy regimens FU. 5-FU biomodulación. Irinotecan. Oxaliplatino. Cetuximab. Bevacizumab. Panitumumab. REFERENCES. Scheithaurer et al. Br Med J. 1993;306:752. Poon et al. J Clin Oncol. 1989;7:1407; Camptosar® (irinotecan) PI. July Petrelli et al. J Clin Oncol. 1989:7:1419. Saltz et al. N Engl J Med. 2000:343:905. Douillard et al. Lancet. 2000:355:1041. Xeloda® (capecitabine) PI. April Goldberg et al. J Clin Oncol. 2004;22:23. de Gramont et al. J Clin Oncol. 2000;18:2938. Eloxatin™ (oxaliplatin) PI. April 2005; Erbitux™ (cetuximab) PI. June Avastin® (bevacizumab) PI. June Vectibix™ (panitumumab) PI. September NCCN. Clinical Practice Guidelines in Oncology: Colon Cancer. v")
34
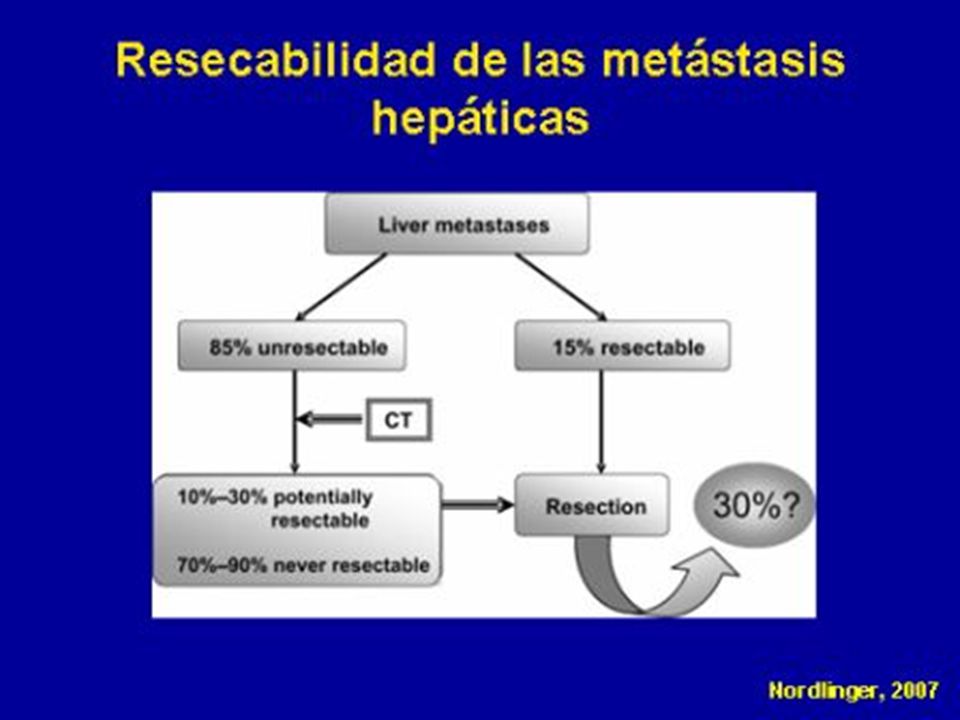
Resecable? Adam et al, Ann Surg 2004 34

38
Qué sucede con la Quimioterapia neo-adyuvante en la Enfermedad resecable?

39
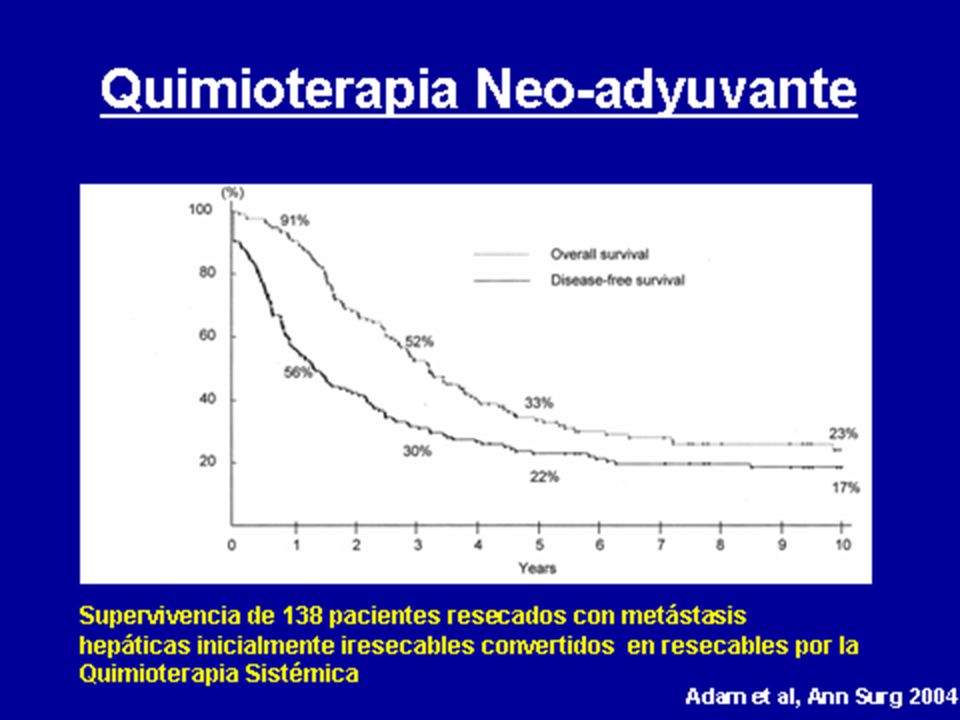
Quimioterapia neo-adyuvante
Disminuye el tamaño tumoral Incrementa las tasas de resección Resecciones más seguras Tratamiento simultáneo de la enfermedad sistémica Identificar respondedores de los no-responderos Minimiza los regímenes inefectivos “Diseña” mejores regímenes adyuvantes 39

40
Quimioterapia neo-adyuvante
Aspectos Controversiales Segura – toxicidad hepática Ventajas de la Supervivencia? Papel de la Quimioterapia adyuvante ? Evidencia Significativa de los beneficios de QT neo-adyuvante Menor tamaño, márgenes seguros

41
Cuando usar la Quimioterapia neo-adyuvante?
Alto riesgo de Enfermedad metastásica Tumores sincrónicos ILE < 12 meses Más de 4 lesiones o bilobulares Ganglios positivos CEA > 200 Lesiones voluminosas Consideraciones Anatómicas Inseguridad de márgenes negativos No hígado residual

42
Qué QT utilizar para la enfermedad resecable?

43
Fase III de Bevacizumab en 1ra-Línea CCRm
IFL + Placebo (n=411) IFL + Bevacizumab (n=402) P Value ORR (%) CR PR 35 2.2 32.5 45 3.7 41.2 0.0036 Bevacizumab reached its primary end points in this trial, resulting in improved survival, PFS, ORR, and duration of response. Median survival: 15.6 months with IFL + placebo vs 20.3 months for IFL + bevacizumab (P= ). PFS: 6.24 months with IFL + placebo vs 10.6 months for IFL + bevacizumab (P< ). ORR: 35% with IFL + placebo vs 45% for IFL + bevacizumab (P=0.0036). Duration of response: 7.1 months with IFL + placebo vs 10.4 months for IFL + bevacizumab (P=0.0014). Interestingly, the increase in ORR was similar to the increase in ORR in the phase III bevacizumab trial in patients with MBC (10%). The success of this trial may be due in part to tumor type, combination therapy used, or the stage of disease. Agents that block angiogenesis may have more clinical benefit when administered earlier in disease progression, before tumor vasculature becomes entrenched. Hurwitz H, et al. N Engl J Med 2004;350:2235–42 Hurwitz et al. Proc Am Soc Clin Oncol. 2003;22. Abstract 3646.
 IFL + Bevacizumab (n=402) P Value. ORR (%) CR. PR Bevacizumab reached its primary end points in this trial, resulting in improved survival, PFS, ORR, and duration of response. Median survival: 15.6 months with IFL + placebo vs 20.3 months for IFL + bevacizumab (P= ). PFS: 6.24 months with IFL + placebo vs 10.6 months for IFL + bevacizumab (P< ). ORR: 35% with IFL + placebo vs 45% for IFL + bevacizumab (P=0.0036). Duration of response: 7.1 months with IFL + placebo vs 10.4 months for IFL + bevacizumab (P=0.0014). Interestingly, the increase in ORR was similar to the increase in ORR in the phase III bevacizumab trial in patients with MBC (10%). The success of this trial may be due in part to tumor type, combination therapy used, or the stage of disease. Agents that block angiogenesis may have more clinical benefit when administered earlier in disease progression, before tumor vasculature becomes entrenched. Hurwitz H, et al. N Engl J Med 2004;350:2235–42. Hurwitz et al. Proc Am Soc Clin Oncol. 2003;22. Abstract")
44
Primera Línea en CCR avanzado
50 40 30 20 10 ORR (%) FOLFIRI Avastin Placebo Avastin FOLFOX Placebo Control Cetuximab Control Avastin Cetuximab Panitumumab + Avastin IFL XELOX/FOLFOX FOLFOX FOLFIRI Irinotecan-based CTx p=0.60 p=0.004 p=0.99 p=0.064 p=0.0038 n.s. Colucci et al JCO 2005 Hurwitz et al NEJM 2004 Saltz et al. JCO 2008 Bokemeyer et al. ECCO 2007 Van Cutsem et al. ASCO 2007 Hecht et al. ASCO GI 2008 ORR = overall response rate; CTx = chemotherapy
 FOLFIRI. Avastin. Placebo. Avastin. FOLFOX. Placebo. Control. Cetuximab. Control. Avastin. Cetuximab. Panitumumab + Avastin. IFL. XELOX/FOLFOX. FOLFOX. FOLFIRI. Irinotecan-based CTx. p=0.60. p= p=0.99. p= p= n.s. Colucci et al. JCO Hurwitz et al. NEJM Saltz et al. JCO Bokemeyer et al. ECCO Van Cutsem et al. ASCO Hecht et al. ASCO GI ORR = overall response rate; CTx = chemotherapy.")
45
Escenario Clínico EGFR Tipo de Tumor Expression EGFR (%) NSCLC 40-80 SCCHN 95 Colorectal* 25-77 Glioblastoma 40-60 Breast 14-91 Prostate 41-100 Ovarian 35-70 Esophageal 35-88 Pancreatic 30-50 Sobre-expresión 75%-89% (Cunningham et al, ‘04; Saltz et al, ‘04) La sobre-expresión se correlaciona con la pobre SV-Pronóstico (Hemming et al, ‘92; Mayer et al ’93) CCR: la expresión de EGFR no es biomarcador clínico predictivo de eficacia para el uso de terapias anti EGFR (NCCN).
 La sobre-expresión se correlaciona con la pobre SV-Pronóstico (Hemming et al, ‘92; Mayer et al ’93) CCR: la expresión de EGFR no es biomarcador clínico predictivo de eficacia para el uso de terapias anti EGFR (NCCN).")
46
Evidencias Clínicas: Cetuximab
BOND I: (Cunningham et al, 2004) Ptes: CCRm Irinotecan-refractarios, 329 ptes Tto: IRI+Cetuximab vs Cetuximab. Rta: RR (%) = 22,9 vs 10,8 p=0.0074 TTP = 4,1 vs 1,5 mo p= <0.0001 OS = 8.6 mo vs 6.9 mo p=0.48 Junio ‘04 – Registro (FDA & EMEA): Erbitux + Q (IRI) en CCRm IRI-Refractarios - 2da y 3ra linea Abril ‘06 – Registro (EMEA) locally advanced squamous cell carcinoma of the head and neck (SCCHN) NCIC-Co 17: (Jonker et al, 2007) Ptes: CCR QT-refractarios, 572 ptes Tto: Cetuximab+ BSC vs BSC. Rta: OS 6.1 mo vs 4.6 mo
 Ptes: CCRm Irinotecan-refractarios, 329 ptes. Tto: IRI+Cetuximab vs Cetuximab. Rta: RR (%) = 22,9 vs 10,8 p= TTP = 4,1 vs 1,5 mo p= < OS = 8.6 mo vs 6.9 mo p=0.48. Junio ‘04 – Registro (FDA & EMEA): Erbitux + Q (IRI) en CCRm IRI-Refractarios - 2da y 3ra linea. Abril ‘06 – Registro (EMEA) locally advanced squamous cell carcinoma of the head and neck (SCCHN) NCIC-Co 17: (Jonker et al, 2007) Ptes: CCR QT-refractarios, 572 ptes. Tto: Cetuximab+ BSC vs BSC. Rta: OS 6.1 mo vs 4.6 mo.")
47
Evidencias Clínicas Previas: Cetuximab
Cx en 1ra linea con Q? EC randomizados y controlados para demostrar eficacia de Cetuximab en combinación con QT estandar en 1ra –linea para tratar CCRm. OPUS (fase II) (‘04): Cx + FOLFOX vs FOLFOX RR = 46 vs 36 %, TTP = 4,1 vs 1,5 mo. CRYSTAL (fase III) (‘07): Cx + FOLFIRI vs FOLFIRI PFS = 8,9 vs 8 mo, RR = 46,9 vs 38,7 %.Resección secundaria de met hepáticas ( 9,8 vs 4,5 %). Mayo ‘08 – Registro (EMEA): Cetuximab en 1ra-Linea en CCR EMEA recomienda uso de Cetuximab en tratamiento de pacientes con: Expresión de EGFR y KRAS wild-type mCRC En combinación con QT Como un agente simple en pacientes que han fallado al tratamiento con Oxaliplatino e Irinotecan y quienes son intolerantes al Irinotecan.
 (‘04): Cx + FOLFOX vs FOLFOX. RR = 46 vs 36 %, TTP = 4,1 vs 1,5 mo. CRYSTAL (fase III) (‘07): Cx + FOLFIRI vs FOLFIRI. PFS = 8,9 vs 8 mo, RR = 46,9 vs 38,7 %.Resección secundaria de met hepáticas ( 9,8 vs 4,5 %). Mayo ‘08 – Registro (EMEA): Cetuximab en 1ra-Linea en CCR. EMEA recomienda uso de Cetuximab en tratamiento de pacientes con: Expresión de EGFR y KRAS wild-type mCRC. En combinación con QT. Como un agente simple en pacientes que han fallado al tratamiento con Oxaliplatino e Irinotecan y quienes son intolerantes al Irinotecan.")
48
Otros Biomarcadores: K-ras
KRAS normal, no mutado o salvaje en 65% CCRm. KRAS mutado en 35-45% de CCRm*. (pancreas*, pulmón* adenocarcinoma, vejiga, tiroides). *alta frecuencia de mutación. Status del gen K-ras: predictivo de eficacia para el uso de terapias anti-EGFR en CCR (Cetuximab (Erbitux, Merck), Panitumumab (Vectibix, Amgen), Erlotinib (Tarceva, Roche/OSI Pharmaceuticals), or Gefitinib (Iressa, AstraZeneca) . monoterapia ó c/QT. K-ras normal K-ras mutado The KRAS protein is tightly regulated and only activated in response to certain stimuli such as EGFR signaling allowing an effective blockade of the downstream signaling by the EGFR targeted antibody Erbitux. In mutant KRAS tumors the KRAS protein is permanently “turned on” and therefore it has been hypothesized that the drug’s inhibition of the downstream effects is less efficient and the tumor may continue to grow, proliferate and spread.
. *alta frecuencia de mutación. Status del gen K-ras: predictivo de eficacia para el uso de terapias anti-EGFR en CCR (Cetuximab (Erbitux, Merck), Panitumumab (Vectibix, Amgen), Erlotinib (Tarceva, Roche/OSI Pharmaceuticals), or Gefitinib (Iressa, AstraZeneca) . monoterapia ó c/QT. K-ras normal. K-ras mutado. The KRAS protein is tightly regulated and only activated in response to certain stimuli such as EGFR signaling allowing an effective blockade of the downstream signaling by the EGFR targeted antibody Erbitux. In mutant KRAS tumors the KRAS protein is permanently turned on and therefore it has been hypothesized that the drug’s inhibition of the downstream effects is less efficient and the tumor may continue to grow, proliferate and spread.")
49
CRYSTAL: Efectos del estado del K-Ras en la eficacia de la Primera Línea del CCRm
Cetuximab 400 mg/m2 initial dose cycle 1, wk 1, 250 mg/m2 weekly (n=50) Irinotecan 180 mg/m2 5-FU mg/m2 bolus mg/m2 40-h CI LV every 2 weeks EGFR-expressing mCRC R Irinotecan 180 mg/m2 5-FU mg/m2 bolus mg/m2 40-h CI LV every 2 weeks Estratificación: Regiones ECOG PS Pacientes Aleatorizados: 1217 Van Cutsem, et al. ASCO 2008
 Irinotecan 180 mg/m2. 5-FU mg/m2 bolus mg/m2 40-h CI. LV every 2 weeks. EGFR-expressing. mCRC. R. Irinotecan 180 mg/m2. 5-FU mg/m2 bolus mg/m2 40-h CI. LV every 2 weeks. Estratificación: Regiones. ECOG PS. Pacientes Aleatorizados: Van Cutsem, et al. ASCO")
50
CRYSTAL: Respuesta de acuerdo al Estado de K-Ras
Cetuximab + FOLFIRI FOLFIRI 70 60 50 40 30 20 10 70 60 50 40 30 20 10 59 43 40 36 Tasa Respuesta (%) Tasa Respuesta (%) Wild-type Mutant p=0.0025 Odds ratio = 1.91 p=0.46 Odds ratio = 0.80 Van Cutsem, et al. ASCO 2008
 Tasa Respuesta (%) Wild-type. Mutant. p= Odds ratio = p=0.46. Odds ratio = Van Cutsem, et al. ASCO")
51
Evidencias Clínicas Previas: Panitumumab

52
Evidencias Clínicas Previas: Nimotuzumab
Tumores sólidos avanzados y refractarios: 13ptes CCR→/17, fase-I Escalado de dosis: mg/sem x 6 sem y luego c/ 2 sem x 18 meses (ó tox. limit). DCR : 56% (9 ptes), 1 RP (mesotelioma) y 8 SD (CCR). mSV: 10 mo y 7,6-media. PFS prolongado en 3/16. La SD y la Rta al Tto contribuyen a prolongar la supervivencia, mientras que la respuesta tumoral por sí sola no es un indicador surrogado adecuado de respuesta. (Masson y cols, 2008, Canadá)
. DCR : 56% (9 ptes), 1 RP (mesotelioma) y 8 SD (CCR). mSV: 10 mo y 7,6-media. PFS prolongado en 3/16. La SD y la Rta al Tto contribuyen a prolongar la supervivencia, mientras que la respuesta tumoral por sí sola no es un indicador surrogado adecuado de respuesta. (Masson y cols, 2008, Canadá)")
53
Evidencias Clínicas Previas: Nimotuzumab
CCRm QT-refractarios (61ptes, fase-II, abierto, aleatorizado) 2008,Canadá, YMB: → Nimo (400mg/sem x 12 sem y luego quincenal hasta progresion) Diferencias en la población de pacientes (solamente) SG y TPP parecen ser comparables a los controles históricos Diferencias moleculares entre Nimotuzumab y otros anti-EGF-R son consideraciones importantes para el desarrollo del producto BOND MABEL LABEL ELSIE YM RR (%) 22.9 20.1 26.6 13.8 3.4 DCR (%) 55.5 45.2 55.7 49.6 50 mTTP (w) 18 14.1 17.4 12.1 12 mOS (95%CI) 8.6 ( ) 9.2 ( ) ( ) 9.5 ( ) 9.3 (5.5-IND)
 2008,Canadá, YMB: → Nimo (400mg/sem x 12 sem y luego quincenal hasta progresion) Diferencias en la población de pacientes (solamente) SG y TPP parecen ser comparables a los controles históricos. Diferencias moleculares entre Nimotuzumab y otros anti-EGF-R son consideraciones importantes para el desarrollo del producto. BOND. MABEL. LABEL. ELSIE. YM. RR (%) DCR (%) mTTP (w) mOS. (95%CI) 8.6. ( ) 9.2. ( ) ( ) 9.5. ( ) 9.3. (5.5-IND)")
54
Eventos Adversos (hR3) YMB N=60 % MABEL N=1147
Tumores sólidos avanzados y refractarios (dose-escalating up to 800 mg) fatiga, nauseas, escalofríos y vómitos y casi en su totalidad de intensidad ligera y moderada (G-1 y 2). 1 EA G-3: fatiga (100 mg, en la primera infusión) CCRm QT-refractarios → YMB N=60 % MABEL N=1147 Any related AE Alopecia Asthenia Diarrhea Fatigue Nausea Vomiting 7 15 33 13 23 67 22 41 28
 fatiga, nauseas, escalofríos y vómitos y casi en su totalidad de intensidad ligera y moderada (G-1 y 2). 1 EA G-3: fatiga (100 mg, en la primera infusión) CCRm. QT-refractarios → YMB. N=60. % MABEL. N=1147. Any related AE. Alopecia. Asthenia. Diarrhea. Fatigue. Nausea. Vomiting")
55
Mecanismo de acción Cetuximab (Mab de alta afinidad):
acne-like skin rash se correlaciona con una buena respuesta al tratamiento (Saltz y cols, 2003; Cunningham y cols, 2004; Perez-Soler y Saltz, 2005; Jonker y cols, 2007) Cerca del 5% de pacientes desarrollan reacciones de hipersensibilidad durante el tratamiento. La mitad de ellas son reacciones severas. Nimotuzumab (Mab de afinidad intermedia): Hasta 800 mg no produce rash cutáneo severo ¿Dosis mayores de nimotuzumab pueden llegar a inducir rash cutáneo y convertir este indicador en un predictor de respuesta clínica?
 Cerca del 5% de pacientes desarrollan reacciones de hipersensibilidad durante el tratamiento. La mitad de ellas son reacciones severas. Nimotuzumab (Mab de afinidad intermedia): Hasta 800 mg no produce rash cutáneo severo. ¿Dosis mayores de nimotuzumab pueden llegar a inducir rash cutáneo y convertir este indicador en un predictor de respuesta clínica")
Presentaciones similares










 Noviembre de 2004.>")









>")