Descargar la presentación
La descarga está en progreso. Por favor, espere

1
GESTION DE CUIDADOS CONTINUOS A LOS ANCIANOS
CIEDESS GESTION DE CUIDADOS CONTINUOS A LOS ANCIANOS ¿Qué dice la evidencia científica? Dr. Leocadio Rodríguez Mañas Santiago de Chile 21 de Octubre, 2008

2
La supervivencia de cualquier civilización puede medirse por
el respeto y el cuidado que da a sus ciudadanos ancianos. Aquellas sociedades que tratan a los ancianos con desprecio llevan en su seno la semilla de su propia destrucción. Arnold Toynbee Historiador

3
¿De qué vamos a hablar? 1) ¿Qué ha pasado? Cambios demográficos Cambios en el tipo de enfermedad y modo de enfermar Cambios en los modos de relación social 2) Nuevos objetivos 3) Nuevas formas de trabajo
 ¿Qué ha pasado Cambios demográficos Cambios en el tipo de enfermedad y modo de enfermar Cambios en los modos de relación social 2) Nuevos objetivos 3) Nuevas formas de trabajo.")
4
¿De qué vamos a hablar? 1) ¿Qué ha pasado? Cambios demográficos Cambios en el tipo de enfermedad y modo de enfermar Cambios en los modos de relación social 2) Nuevos objetivos 3) Nuevas formas de trabajo
 ¿Qué ha pasado Cambios demográficos Cambios en el tipo de enfermedad y modo de enfermar Cambios en los modos de relación social 2) Nuevos objetivos 3) Nuevas formas de trabajo.")
5
TRANSICION DEMOGRAFICA

6
Corpus Inscriptionum Latinarum. Siglo I DC
ESPAÑA - Siglo I DC ESPAÑA HOMBRES MUJERES Vivos 1111 % Expect. de vida 885 60 a. 269 24,2 13,7 120 13,5 12,3 70 a. 163 14,6 10 66 7,4 9,2 80 a. 70 6,3 8 23 2,6 8,4 90 a. 2 6 7 0,8 7.6 100 a. 0,9 2,5 0,2 HOMBRES MUJERES % Expect. de vida 88 21 95 25 75 13,6 89 17 49,5 7,8 72 9 15 4 32 4,5 1,2 2 3,5 2,1 Corpus Inscriptionum Latinarum. Siglo I DC OMS, 2007.

7
Las Pirámides de población en la España del siglo XX
La evolución de las pirámides de población muestra unas variaciones muy acusadas en la natalidad y en la mortalidad a lo largo del siglo pasado. En , la forma correspondía efectivamente a una pirámide, como consecuencia de la fuerte mortalidad que se venía padeciendo entonces a todas las edades. La esperanza de vida apenas sobrepasaba los 30 años y la mortalidad infantil era muy alta. Las diferencia entre los dos sexos eran pequeñas. En , la disminución de la mortalidad a edades tempranas y medianas, el efecto de la guerra civil y la alta natalidad de esos años habían dado una forma más acampanada a la pirámide. A partir de los 60 años, la mayor supervivencia de la mujer ya se dejaba notar claramente. El crecimiento de la natalidad en los años 60 y 70 —conocido como — fue seguido de una disminución muy acentuada en el número de nacimientos a partir de entonces, lo que provocó el estrechamiento en la base de la . Como consecuencia del ligero avance de la natalidad en los últimos años, en la se aprecia que el colectivo de “0 a 5 años” es algo mayor que el siguiente (”5 a 9 años”). 1900 1960 pirámide de 1991 pirámide de 2001 baby boom
 pirámide de pirámide de baby boom.")
8
EVOLUCION DE LA POBLACION ANCIANA EN ESPAÑA
DISTRIBUCION DE LA POBLACION ANCIANA EN ESPAÑA POR CC.AA.

9
Tamaño y distribución de la población mundial de 60 años o más
( ). 20% 7% 1% Fuente: Naciones Unidas/Departamento de Asuntos Económicos y Sociales (DAES).
. 20% 7% 1% Fuente: Naciones Unidas/Departamento de Asuntos Económicos y Sociales (DAES).")
10
¿De qué vamos a hablar? 1) ¿Qué ha pasado? Cambios demográficos Cambios en el tipo de enfermedad y modo de enfermar Cambios en los modos de relación social 2) Nuevos objetivos 3) Nuevas formas de trabajo
 ¿Qué ha pasado Cambios demográficos Cambios en el tipo de enfermedad y modo de enfermar Cambios en los modos de relación social 2) Nuevos objetivos 3) Nuevas formas de trabajo.")
11
TRANSICION EPIDEMIOLOGICA
50 100 150 200 250 300 350 400 1900 1920 1950 Cardiop. Isquémica Cancer Tuberculosis Disentería Neumonía -80 -60 -40 -20 20 40 1950 1960 1975 1995 Cardiop. Isquémica ACVA Mortalidad no CV Muertes/ Cambio (%) Braunwald E, N Engl J Med 1997; 337:
 Braunwald E, N Engl J Med 1997; 337:")
12
Envejecimiento poblacional. Morbilidad asociada a la edad
80 ECV Framingham-1989 70 ICC Demencia 60 50 Incidencia (por 1000) 40 Europa-2000 EE UU-2006 30 20 10 45-54 55-64 65-74 75-84 > 85 Edad (años)
 40. Europa EE UU > 85. Edad (años)")
13
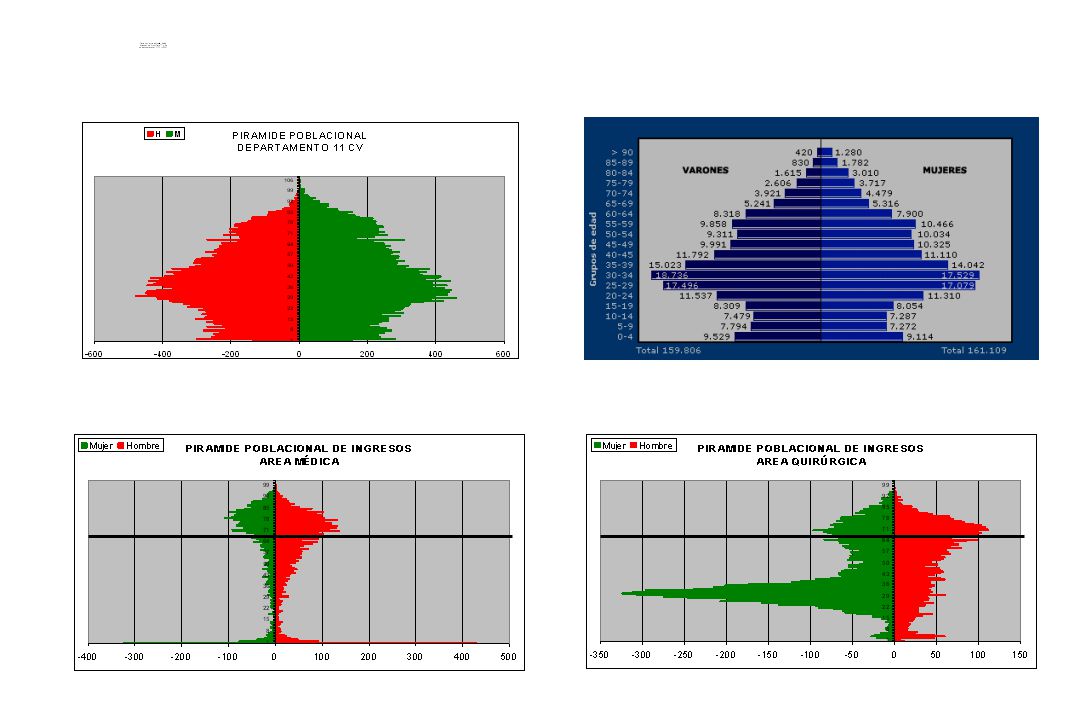
Distribución de la mortalidad (todas las causas) por sexo y edad por 1
Distribución de la mortalidad (todas las causas) por sexo y edad por fallecidos, 1999 47% 82% Hombres Mujeres El principal factor de esta ganancia es el descenso de la mortalidad infantil. La mayoría de los españoles recién nacidos ahora celebrará su 65 cumpleaños. A principio de siglo XX sólo un 26% llegaba a viejo; en las condiciones de mortalidad actuales, de 100 nacidos más de 86 alcanzarán la vejez (las mujeres alcanzan el 91,1% y los varones el 79,3%). El porcentaje de personas que habiendo superado el umbral de los 65 años espera cumplir los 90 ha pasado de dos a veintidós entre 1930 y Un auténtico éxito de la supervivencia (Tabla 2.2; Gráfico 2.2). Nuestra sociedad, como todas las que envejecen, ha sido víctima de este éxito. Fuentes: INE: INEBASE: Defunciones según la Causa de Muerte Distribución de la mortalidad por causas (lista reducida), sexo y edad. INE, 2002.
 por sexo y edad por fallecidos, % 82% Hombres. Mujeres. El principal factor de esta ganancia es el descenso de la mortalidad infantil. La mayoría de los españoles recién nacidos ahora celebrará su 65 cumpleaños. A principio de siglo XX sólo un 26% llegaba a viejo; en las condiciones de mortalidad actuales, de 100 nacidos más de 86 alcanzarán la vejez (las mujeres alcanzan el 91,1% y los varones el 79,3%). El porcentaje de personas que habiendo superado el umbral de los 65 años espera cumplir los 90 ha pasado de dos a veintidós entre 1930 y Un auténtico éxito de la supervivencia (Tabla 2.2; Gráfico 2.2). Nuestra sociedad, como todas las que envejecen, ha sido víctima de este éxito. Fuentes: INE: INEBASE: Defunciones según la Causa de Muerte Distribución de la mortalidad por causas (lista reducida), sexo y edad. INE,")
17
¿De qué vamos a hablar? 1) ¿Qué ha pasado? Cambios demográficos Cambios en el tipo de enfermedad y modo de enfermar Cambios en los modos de relación social 2) Nuevos objetivos 3) Nuevas formas de trabajo
 ¿Qué ha pasado Cambios demográficos Cambios en el tipo de enfermedad y modo de enfermar Cambios en los modos de relación social 2) Nuevos objetivos 3) Nuevas formas de trabajo.")
18
La edad avanzada rara vez llega sola, sino que habitualmente se acompaña de fragilidad, comorbilidad, riesgo de aislamiento social y dificultades económicas. Por tanto, el cuidado de los ancianos requiere una combinación de medicina basada en problemas y de medicina basada en el diagnóstico La edad ejerce influencias heterogéneas sobre la enfermedad y la incapacidad y, como en la pediatría, hay tanto enfermedades edad-específicas como enfermedades de presentación atípica en la vejez Who cares for the elderly? Editorial, Lancet, 22 de Marzo de 2008; 371: 959

19
…y son distintos!!! Hay más… …en ellos se concentra
la carga de enfermedad… …y son distintos!!!

20
CONSECUENCIAS Aumento de la expectativa de vida
Aumento de la prevalencia de enfermedades crónicas Mayor tiempo manteniendo el status de enfermo Acumulación de enfermedades en el mismo sujeto Concentración de las enfermedades en la etapa final de la vida ………...

21
… y con repercusión en la situación funcional,
en la capacidad de autonomía del paciente.

22
Envejecimiento Poblacional: Edad Cronológica Discapacidad

24
Esperanza de vida a los 70 años según situación funcional a esa edad
No limitación o Nagi solo iAVD-bAVD limitación Institucionalizados 16 14 12 10 Esperanza de vida (total) 8 6 4 2 No Nagi iAVD bAVD Institución Estado funcional a los 70 años Lubitz J, Health, life expectancy, and health care spending among the elderly. NEJM :
 No. Nagi. iAVD. bAVD. Institución. Estado funcional a los 70 años. Lubitz J, Health, life expectancy, and health care spending among the elderly. NEJM :")
25
Gasto sanitario esperado desde los 70 años hasta la muerte, según situación funcional a los 70 años
No limitación o Nagi solo iAVD-bAVD limitación Institucionalizados Gasto sanitario ($) 50.000 No Nagi iAVD bAVD Institución Limitación en situación funcional a los 70 años Lubitz J, Health, life expectancy, and health care spending among the elderly. NEJM :
 No. Nagi. iAVD. bAVD. Institución. Limitación en situación funcional a los 70 años. Lubitz J, Health, life expectancy, and health care spending among the elderly. NEJM :")
26
¿De qué vamos a hablar? 1) ¿Qué ha pasado? Cambios demográficos Cambios en el tipo de enfermedad y modo de enfermar Cambios en los modos de relación social 2) Nuevos objetivos 3) Nuevas formas de trabajo
 ¿Qué ha pasado Cambios demográficos Cambios en el tipo de enfermedad y modo de enfermar Cambios en los modos de relación social 2) Nuevos objetivos 3) Nuevas formas de trabajo.")
28
¿De qué vamos a hablar? 1) ¿Qué ha pasado? Cambios demográficos Cambios en el tipo de enfermedad y modo de enfermar Cambios en los modos de relación social 2) Nuevos objetivos 3) Nuevas formas de trabajo
 ¿Qué ha pasado Cambios demográficos Cambios en el tipo de enfermedad y modo de enfermar Cambios en los modos de relación social 2) Nuevos objetivos 3) Nuevas formas de trabajo.")
29
MUJERES HOMBRES EXPECTATIVA DE VIDA Edad al diagnóstico 2 4 6 8 10 12
2 4 6 8 10 12 14 16 18 20 65 70 75 80 85 5% 10% 25% 50% NORMAL 2 4 6 8 10 12 14 16 18 20 65 70 75 80 85 EXPECTATIVA DE VIDA Edad al diagnóstico Welch HG et al., Ann Intern Med 1996; 124:

30
muerte Posibles futuros escenarios de morbilidad y longevidad
Incapacidad Morbilidad actual 76 años 55 años 55 años 80 años Extensión de vida 60 años 81 años Desplazamiento a la derecha 65 años 78 años Compresión de la morbilidad Fries JF. Measuring and monitoring success in compressing morbidity. Ann Intern Med 2003:139:

31
Porcentaje de >65 años con discapacidad en España (1986-1999).
Encuesta Nacional de Discapacidad. Participantes 1986 (%) 1999 (%) Diferencia (%) Hombres Total 65-69 70-74 75-79 80-84 ≥85 (39,88) 25,75 35,63 45,33 62,66 76,85 (19,28) 11,07 15,30 23,33 30,81 46,92 -51,64 -57,02 -57,07 -48,54 -50,83 -38,94 Mujeres (48,98) 31,01 40,84 51,07 67,54 86,41 (28,06) 14,66 24,17 31,77 40,14 55,40 -42,70 -52,71 -47,42 -37,80 -40,56 -35,88 Sagarduy-Villamor et al, J Gerontol Med Sci 2005; 60A:
 1999 (%) Diferencia (%) Hombres. Total ≥ (39,88) 25,75. 35,63. 45,33. 62,66. 76, (19,28) 11,07. 15,30. 23,33. 30,81. 46, , , , , , ,94. Mujeres (48,98) 31,01. 40,84. 51,07. 67,54. 86, (28,06) 14,66. 24,17. 31,77. 40,14. 55, , , , , , ,88. Sagarduy-Villamor et al, J Gerontol Med Sci 2005; 60A:")
32
>>> 100%

33
Edad no equivale a discapacidad
Es la enfermedad, y no la edad, quien lleva a la discapacidad Los ancianos son muy heterogéneos Lo caro es la discapacidad, no el envejecimiento …y además El envejecimiento se acompaña de pérdida de reserva funcional Una vez establecida la discapacidad, es difícil de revertir

34
Nuevas características
Nuevas necesidades Nuevos objetivos Nuevos métodos

36
¿Nuevas respuestas? A nuevas características, a nuevas necesidades,
a nuevos objetivos, a nuevos métodos…... ¿Nuevas respuestas?

37
¿De qué vamos a hablar? 1) ¿Qué ha pasado? Cambios demográficos Cambios en el tipo de enfermedad y modo de enfermar Cambios en los modos de relación social 2) Nuevos objetivos 3) Nuevas formas de trabajo
 ¿Qué ha pasado Cambios demográficos Cambios en el tipo de enfermedad y modo de enfermar Cambios en los modos de relación social 2) Nuevos objetivos 3) Nuevas formas de trabajo.")
39
Medicina Geriátrica: Fundamentos
Servicio Geriatría Investigación: Producir conocimiento Unidades Investigación Docencia: Transmitir conocimiento Universidad Pregrado Postgrado Hospital Asistencia: Ejecutar conocimiento Específica Precoz Integral Contínua Eficiente The question students should be taught to ask when faced with an elderly person with disability is: “ what can I do to improve the situation”? Evans JG, Williams TF. Oxford Textbook of Geriatric Medicine, 1992.

40
OPCIONES ¿Seguimos gestionando el fracaso...
…o intentamos buscar el éxito?

41
PREVENCION DEL DETERIORO
PUNTO CRITICO DE INTERVENCION MOMENTO USUAL DEL DIAGNÓSTICO LESION INCAPACIDAD INVALIDEZ

42
Madrid, 2007

43
Población muy heterogénea
Vigoroso Frágil Dependiente

44
Cribado Intervención

45
CONSECUENCIAS DE LA FRACTURA DE CADERA EN OCTOGENARIOS
Coste total por paciente (dólares) Hospitalización Rehospitalizaciones 3.900 Rehabilitación Cuidados continuados Institucion Domicilio TOTAL 2/3 del gasto, despues de 6 meses Braithwaite y cols, JAGS, 2003
 Hospitalización Rehospitalizaciones Rehabilitación Cuidados continuados. Institucion Domicilio TOTAL /3 del gasto, despues de 6 meses. Braithwaite y cols, JAGS,")
46
CONSECUENCIAS DE LA FRACTURA DE CADERA EN OCTOGENARIOS (II)
Sin déficit Algún déficit Expectativa de vida (años) 6,9 (-9%) ,6 (-33%) Tiempo instituc. (días) (+75%) Costes de atención continuada ($) (+2.500%) Braithwaite y cols, JAGS, 2003
 6,9 (-9%) 4,6 (-33%) Tiempo instituc. (días) (+75%) Costes de atención continuada ($) (+2.500%) Braithwaite y cols, JAGS,")
47
Alhacen (965 – 1039) Observación Enunciar el problema Formulación de la hipótesis Experimentar Analizar los resultados Interpretar los datos y formular las conclusiones Publicar los resultados LA VERDAD se debe buscar por si misma. Su búsqueda es difícil y el camino está lleno de dificultades was an Arab[1] Muslim polymath[2][3] who made significant contributions to the principles of optics, as well as to anatomy, astronomy, engineering, mathematics, medicine, ophthalmology, philosophy, physics, psychology, visual perception, and to science in general with his introduction of the scientific method.According to the majority of the historians al-Haytham was the pioneer of the modern scientific method. With his book he changed the meaning of the term optics and established experiments as the norm of proof in the field. His investigations are based not on abstract theories, but on experimental evidences and his experiments were systematic and repeatable. "His work on optics, which includes a theory of vision and a theory of light, is considered by many to be his most important contribution, setting the scene for developments well into the 17th century. His contributions to geometry and number theory go well beyond the archimedean tradition. And by promoting the use of experiments in scientific research, al-Haytham played an important part in setting the scene for modern science."[27] Ibn al-Haytham developed rigorous experimental methods of controlled scientific testing in order to verify theoretical hypotheses and substantiate inductive conjectures.[19] Ibn al-Haytham's scientific method was very similar to the modern scientific method and consisted of the following procedures: Observation Statement of problem Formulation of hypothesis Testing of hypothesis using experimentation Analysis of experimental results Interpretation of data and formulation of conclusion Publication of findings From Alhacen (Ibn Al-Haytham 965 – 1039, a pioneer of scientific method) to the present day, the emphasis has been on seeking truth: "Truth is sought for its own sake. And those who are engaged upon the quest for anything for its own sake are not interested in other things. Finding the truth is difficult, and the road to it is rough.
 to the present day, the emphasis has been on seeking truth: Truth is sought for its own sake. And those who are engaged upon the quest for anything for its own sake are not interested in other things. Finding the truth is difficult, and the road to it is rough.")
48
James Lind (1716-1794) Escorbuto (N=12) I sidra II 25 gotas vitriolo
III vinagre IV agua marina V 2 naranjas y 1 limón VI pasta picante y agua de cebada Pionero higiene naval y prevención Primer ensayo clínico controlado James Lind (1716 in Edinburgh – 1794 in Gosport) was the pioneer of naval hygiene in the Royal Navy. By conducting what was perhaps the first ever clinical trial, he proved that citrus fruits cure scurvy. He also proposed that by distilling sea water you could obtain fresh water. Moreover he fought for the drying of ships by better ventilation, improved clothing and cleanliness of the sailors and introduced fumigaton with sulphur and arsenic. By his work he also influenced practices of preventive medicine and nutrition among British soldiers. The disease scurvy is now known to be due to a deficiency of vitamin C, but in Lind's day, the concept of vitamins was unknown. Lind thought that scurvy was due to putrefaction of the body which could be prevented by acids; that is why he chose to experiment with dietary supplements of acidic quality. In his experiment he divided twelve scorbutic sailors into six groups. They all received the same diet, and in addition group one was given a quart of cider daily, group two twenty-five drops of elixir of vitriol, group three six spoonful of vinegar, group four half a pint of seawater, group five received two oranges and one lemon and the last group a spicy paste plus a drink of barley water. The treatment of group five stopped after six days when they ran out of fruit, but by that time one sailor was fit for duty and the other had almost recovered. Apart from that, only group one also showed some effect of its treatment. In 1753 he published A treatise of the scurvy, which was virtually ignored. In 1758 he was appointed chief physician of the Royal Naval Hospital Haslar at Portsmouth. When James Cook went on his first voyage he carried wort (0.1 mg vitamin C per 100 g), sauerkraut (10-15 mg per 100 g) and a syrup of oranges and lemons (the juice contains mg of vitamin C per 100 g) as antiscorbutics, but only the results of the trials on wort were published. In 1762 Lind’s Essay on the most effectual means of preserving the health of seamen appeared. In it he recommended growing salad, i.e. watercress (662 mg vitamin C per 100 g) on wet blankets. This was actually put in practice, and in the winter of 1775 the British Army in North America was supplied with mustard and cress seeds.
 was the pioneer of naval hygiene in the Royal Navy. By conducting what was perhaps the first ever clinical trial, he proved that citrus fruits cure scurvy. He also proposed that by distilling sea water you could obtain fresh water. Moreover he fought for the drying of ships by better ventilation, improved clothing and cleanliness of the sailors and introduced fumigaton with sulphur and arsenic. By his work he also influenced practices of preventive medicine and nutrition among British soldiers. The disease scurvy is now known to be due to a deficiency of vitamin C, but in Lind s day, the concept of vitamins was unknown. Lind thought that scurvy was due to putrefaction of the body which could be prevented by acids; that is why he chose to experiment with dietary supplements of acidic quality. In his experiment he divided twelve scorbutic sailors into six groups. They all received the same diet, and in addition group one was given a quart of cider daily, group two twenty-five drops of elixir of vitriol, group three six spoonful of vinegar, group four half a pint of seawater, group five received two oranges and one lemon and the last group a spicy paste plus a drink of barley water. The treatment of group five stopped after six days when they ran out of fruit, but by that time one sailor was fit for duty and the other had almost recovered. Apart from that, only group one also showed some effect of its treatment. In 1753 he published A treatise of the scurvy, which was virtually ignored. In 1758 he was appointed chief physician of the Royal Naval Hospital Haslar at Portsmouth. When James Cook went on his first voyage he carried wort (0.1 mg vitamin C per 100 g), sauerkraut (10-15 mg per 100 g) and a syrup of oranges and lemons (the juice contains mg of vitamin C per 100 g) as antiscorbutics, but only the results of the trials on wort were published. In 1762 Lind’s Essay on the most effectual means of preserving the health of seamen appeared. In it he recommended growing salad, i.e. watercress (662 mg vitamin C per 100 g) on wet blankets. This was actually put in practice, and in the winter of 1775 the British Army in North America was supplied with mustard and cress seeds.")
49
Creencia Caballo volador. Needham's Science and Civilisation in China
A belief need not be true (although a belief can be true, even if its origins were myth). Needham's Science and Civilisation in China uses the 'flying horse' image as an example of observation: in it, a horse's legs are depicted as splayed, when the stop-action picture by Eadweard Muybridge shows otherwise. Note that the moment that no hoof is touching the ground, the horse's legs are gathered together and are not splayed. Eadweard Muybridge's studies of a horse galloping Earlier paintings depict the incorrect flying horse observation. This demonstrates Ludwik Fleck's caution that we see what we expect to observe, until shown otherwise; our beliefs will affect our observations (and therefore our subsequent actions). But repeated application of scientific method can help us solve our problems by exposing those parts of our beliefs which are false. A scientific community will have the same interests, which allows it to help solve problems together. Caballo volador. Needham's Science and Civilisation in China
. Needham s Science and Civilisation in China uses the flying horse image as an example of observation: in it, a horse s legs are depicted as splayed, when the stop-action picture by Eadweard Muybridge shows otherwise. Note that the moment that no hoof is touching the ground, the horse s legs are gathered together and are not splayed. Eadweard Muybridge s studies of a horse galloping. Earlier paintings depict the incorrect flying horse observation. This demonstrates Ludwik Fleck s caution that we see what we expect to observe, until shown otherwise; our beliefs will affect our observations (and therefore our subsequent actions). But repeated application of scientific method can help us solve our problems by exposing those parts of our beliefs which are false. A scientific community will have the same interests, which allows it to help solve problems together. Caballo volador. Needham s Science and Civilisation in China.")
50
Verdad Estudio del galope equino de Eadweard Muybridge
A belief need not be true (although a belief can be true, even if its origins were myth). Needham's Science and Civilisation in China uses the 'flying horse' image as an example of observation: in it, a horse's legs are depicted as splayed, when the stop-action picture by Eadweard Muybridge shows otherwise. Note that the moment that no hoof is touching the ground, the horse's legs are gathered together and are not splayed. Eadweard Muybridge's studies of a horse galloping Earlier paintings depict the incorrect flying horse observation. This demonstrates Ludwik Fleck's caution that we see what we expect to observe, until shown otherwise; our beliefs will affect our observations (and therefore our subsequent actions). But repeated application of scientific method can help us solve our problems by exposing those parts of our beliefs which are false. A scientific community will have the same interests, which allows it to help solve problems together. Estudio del galope equino de Eadweard Muybridge
. Needham s Science and Civilisation in China uses the flying horse image as an example of observation: in it, a horse s legs are depicted as splayed, when the stop-action picture by Eadweard Muybridge shows otherwise. Note that the moment that no hoof is touching the ground, the horse s legs are gathered together and are not splayed. Eadweard Muybridge s studies of a horse galloping. Earlier paintings depict the incorrect flying horse observation. This demonstrates Ludwik Fleck s caution that we see what we expect to observe, until shown otherwise; our beliefs will affect our observations (and therefore our subsequent actions). But repeated application of scientific method can help us solve our problems by exposing those parts of our beliefs which are false. A scientific community will have the same interests, which allows it to help solve problems together. Estudio del galope equino de Eadweard Muybridge.")
51
VALORACION GERIATRICA

52
La valoración geriátrica integral, completada con una anamnesis y manejo diagnóstico apropiados y expertos, junto a una valoración holística, componen el estándar de la atención a los ancianos. La investigación confirma que los equipos multidisciplinares dirigidos por geriatras consiguen mejores resultados en personas con pluripatología y problemas funcionales Los geriatras están inmejorablemente ubicados para dirigir los cuidados integrados dirigidos a los ancianos. Who cares for the elderly? Editorial, Lancet, 22 de Marzo de 2008; 371: 959

53
ASISTENCIA GERIATRICA SECTORIZADA Y COORDINADA
ATENCION PRIMARIA Gestión de casos SERVICIOS SOCIALES - AGD ATENCION ESPECIALIZADA OTROS SERVICIOS HOSPITALARIOS SEVICIO DE GERIATRIA - UGA - UGRF - HDG - Interconsultas - C. Externa AGD: asistencia geriátrica domiciliaria; UGA: Unidad Geriátrica de Agudos; UGRF: Unidad Geriátrica de Recuperación Funcional; HDG: Hospital de Día Geriátrico;

55
Baztán JJ, Suárez F, López-Arrieta J, Rodríguez-Mañas L, Rodríguez-Artalejo F
Br Med J 2009 (in press)
")
56
Baztán JJ, Suárez F, López-Arrieta J, Rodríguez-Mañas L, Rodríguez-Artalejo F
Br Med J 2009 (in press)
")
57
Baztán JJ, Suárez F, López-Arrieta J, Rodríguez-Mañas L, Rodríguez-Artalejo F
Br Med J 2009 (in press)
")
58
Baztán JJ, Suárez F, López-Arrieta J, Rodríguez-Mañas L, Rodríguez-Artalejo F
Br Med J 2009 (in press)
")
59
Beswick AD et al, Lancet 2008; 371: 725-735
0,83-0,90) No vivir en domicilio Muerte Ingreso Residencia Ingreso hospitalario Caídas Función física Valoración geriátrica en pobl. gral. 0,95 (0,93-0,98) 1 (0,98-1,03) 0,86 (0,83-0,90) 0,98 (0,92-1,03) 0,76 (0,67-0,86) -0,12 (-0,16;-0,08) Valoración geriátrica en anc. frágil (0,87-1,15) 1,03 (0,89-1,19) 1,01 (0,83-1,23) 0,9 (0,84-0,98) 0,99 (0.89-1,10) -0,01 (-0,06;-0,04) Cuidados postalta hospitalaria (0,82-0,99) 0,97 (0,89-1,05) 0,77 (0,64-0,91) (0,90-0,99) 0,82 (0,61-1,08) -0,05 (-0,15; 0,04) Prevención de caídas (0,63-1,19) 0,79 (0,66-0,96) 1,26 (0,70-2,27) 0,84 (0,61-1,16) 0,92 (0,87-0,97) -0,25 (-0,36;-0,13) Educación y consejos 0,62 (0,43-0,88) 0,80 (0,42-1,55) 0,50 (0,05-5,49) 0,75 (0,51-1,09) NA 0,05 (-0,20; 0,30) Todas las intervenciones complejas (0,93-0,97) (0,97-1,02) 0,87 0,94 (0,91-0,97) 0,90 (0,86-0,95) -0,08 -0,11;-0,06 Beswick AD et al, Lancet 2008; 371:
 No vivir en domicilio. Muerte. Ingreso Residencia. Ingreso hospitalario. Caídas. Función física. Valoración geriátrica en pobl. gral. 0,95. (0,93-0,98) 1. (0,98-1,03) 0,86. (0,83-0,90) 0,98. (0,92-1,03) 0,76. (0,67-0,86) -0,12. (-0,16;-0,08) Valoración geriátrica en anc. frágil. (0,87-1,15) 1,03. (0,89-1,19) 1,01. (0,83-1,23) 0,9. (0,84-0,98) 0,99. (0.89-1,10) -0,01. (-0,06;-0,04) Cuidados postalta hospitalaria. (0,82-0,99) 0,97. (0,89-1,05) 0,77. (0,64-0,91) (0,90-0,99) 0,82. (0,61-1,08) -0,05. (-0,15; 0,04) Prevención de caídas. (0,63-1,19) 0,79. (0,66-0,96) 1,26. (0,70-2,27) 0,84. (0,61-1,16) 0,92. (0,87-0,97) -0,25. (-0,36;-0,13) Educación y consejos. 0,62. (0,43-0,88) 0,80. (0,42-1,55) 0,50. (0,05-5,49) 0,75. (0,51-1,09) NA. 0,05. (-0,20; 0,30) Todas las intervenciones. complejas. (0,93-0,97) (0,97-1,02) 0,87. 0,94. (0,91-0,97) 0,90. (0,86-0,95) -0,08. -0,11;-0,06. Beswick AD et al, Lancet 2008; 371:")
60
GRADO de RECOMENDACIÓN para la IMPLANTACIÓN DE INTERVENCIONES GERIATRICAS (SEMEG, 2001)
NIVEL DE INTERVENCION RECOMENDACION Intrahospitalaria -Unidad Geriátrica de Agudos Muy recomendable (A) -Unidad Geriátrica de Recuperación Funcional Muy recomendable (A) -Unidades de Ortogeriatría Muy recomendable (A) -Equipo Geriátrico Consultor (COT) Recomendable (B) -Equipo Geriátrico Consultor Desaconsejado (D) Extrahospitalaria -Hospital de Dia Geriátrico Recomendable (B) -Seguimiento Domiciliario Postalta Recomendable (B) -Hospitalización Domiciliaria Desaconsejado (D) -Cuidados de Soporte y Larga Estancia -Domiciliaria Especializada Recomendable (B)
 -Unidad Geriátrica de Recuperación Funcional Muy recomendable (A) -Unidades de Ortogeriatría Muy recomendable (A) -Equipo Geriátrico Consultor (COT) Recomendable (B) -Equipo Geriátrico Consultor Desaconsejado (D) Extrahospitalaria. -Hospital de Dia Geriátrico Recomendable (B) -Seguimiento Domiciliario Postalta Recomendable (B) -Hospitalización Domiciliaria Desaconsejado (D) -Cuidados de Soporte y Larga Estancia. -Domiciliaria Especializada Recomendable (B)")
61
RESULTADOS DEL PRIMER AÑO
1. Prevención de ingresos inadecuados. Resultados primer año RESULTADOS DEL PRIMER AÑO 380 valoraciones completas 240 (62.3%) altas Otras 415 consultas puntuales, por otros pacientes, durante la estancia de la geriatra en el Sº de Urgencias 61
 altas. Otras 415 consultas puntuales, por otros pacientes, durante la estancia de la geriatra en el Sº de Urgencias. 61.")
62
2. Prevención de ingresos inadecuados. Resultados primer año
380 valoraciones completas 240 (62.3%) altas Otras 415 consultas puntuales, por otros pacientes, durante la estancia de la geriatra en el Sº de Urgencias
 altas. Otras 415 consultas puntuales, por otros pacientes, durante la estancia de la geriatra en el Sº de Urgencias.")
63
Beneficios para el paciente:
Tratamiento adecuado (NO negativa a tratamiento) Evita ingreso-medio hostil Desventaja: segunda llamada Beneficios para el Sistema Sanitario 240 ingresos evitados 1990 estancias Ahorro euros (96 millones de pesetas) 63
 Evita ingreso-medio hostil. Desventaja: segunda llamada. Beneficios para el Sistema Sanitario. 240 ingresos evitados estancias. Ahorro euros (96 millones de pesetas) 63.")
64
Indicadores de calidad
Utilización Eficiencia Unidad de Agudos > 1700 ingresos/año Estancia Media < 9,5 dias Consulta Externa > primeras consultas Indice sucesivas/primeras < 2,3 Plan de Prevención Ingresos Inadecuados > 600 consultas año Ingresos evitados > 40% Interconsultas (ortogeriatría) > 600 interconsultas/año (> 200 interconsultas/año) Mejora informes (mayor complejidad) Mejora estancia media (5%) Consultas monográficas (caidas y fracturas) > 500 primeras consultas/año (>100 primeras consultas/año) Disminución en la incidencia de fracturas 10% Mejoría en EM e institucionalización al alta Unidad de Cuidados Comunitarios > 1200 actuaciones Reingresos < 30 días < 15% Hospital de Día > 2500 estancias/año Estancias/paciente < 20 Unidad de Cuidados al Final de la Vida > 300 actuaciones/año Satisfacción de la familia
 > 600 interconsultas/año. (> 200 interconsultas/año) Mejora informes (mayor complejidad) Mejora estancia media (5%) Consultas monográficas (caidas y fracturas) > 500 primeras consultas/año. (>100 primeras consultas/año) Disminución en la incidencia de fracturas 10% Mejoría en EM e institucionalización al alta. Unidad de Cuidados Comunitarios. > 1200 actuaciones. Reingresos < 30 días < 15% Hospital de Día. > 2500 estancias/año. Estancias/paciente < 20. Unidad de Cuidados al Final de la Vida. > 300 actuaciones/año. Satisfacción de la familia.")
65
Sº Geriatría Otros Sº hospital COT Atención Rehabilitación IC-Ortoger
Programa de caídas/fracturas Otros Sº hospital COT Rehabilitación Reuma …. Atención Primaria IC-Ortoger HD Sº Geriatría Asistencia Docencia Investigación Consulta UCC UGA Ciudadanos Sº Sociales Residencias

Presentaciones similares





 año 2009.>")

















