Descargar la presentación
La descarga está en progreso. Por favor, espere

1
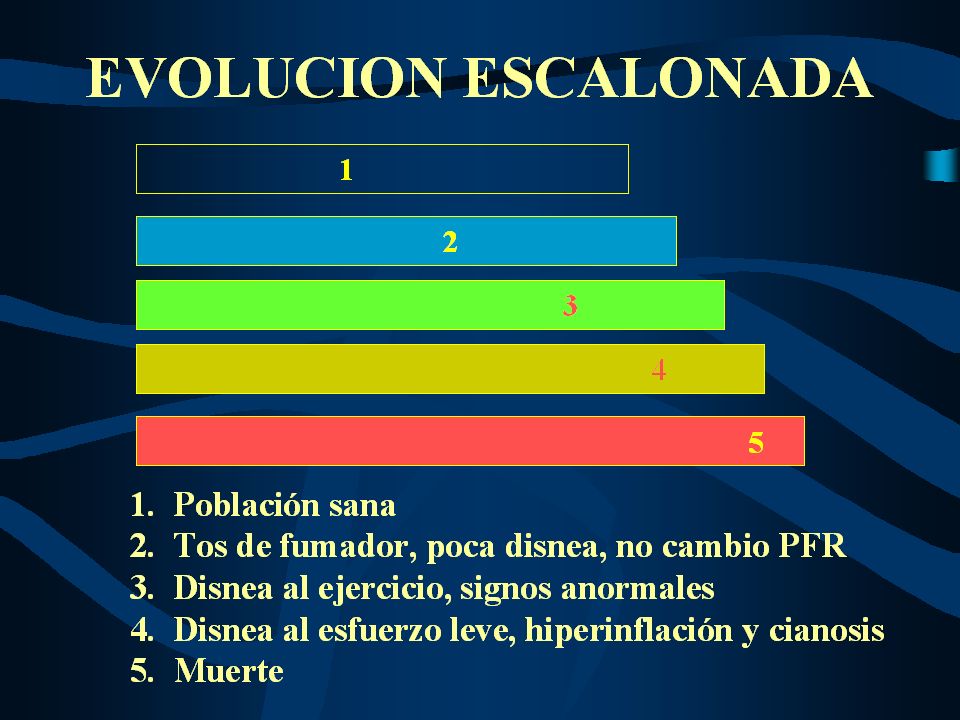
Enfermedades Respiratorias Obstructivas en el Adulto Mayor
Dr. Alfredo Guerreros Benavides HNDAC Clínica Internacional

2
Aumento de la Expectativa de Vida e Impacto Global
Global Burden Disease. Murray y López Países desarrollados : disminución 25% menores de 15 ,incremento 71% mayores de 65. Países en desarrollo incremento 25% menores de 15 e incremento 140% 45 a 59. Poblaciones España e Italia 80 a 105 años. Japón 2002: 17,934 personas de 100 años.

3
Cambios Fisiológicos Disminución de la compliance de la pared torácica y el sistema respiratorio,así como del retroceso elástico resultan en atrapamiento aéreo ( incremento de VR ). Incremento de la CRF y del trabajo respiratorio. Afección de la musculatura respiratoria,cambios en la geometría de la caja torácica,estado nutricional, función cardíaca : sarcopenia. >80 años :PIM valores críticos bajos, hipoventilación alveolar.
. Incremento de la CRF y del trabajo respiratorio. Afección de la musculatura respiratoria,cambios en la geometría de la caja torácica,estado nutricional, función cardíaca : sarcopenia. >80 años :PIM valores críticos bajos, hipoventilación alveolar.")
4
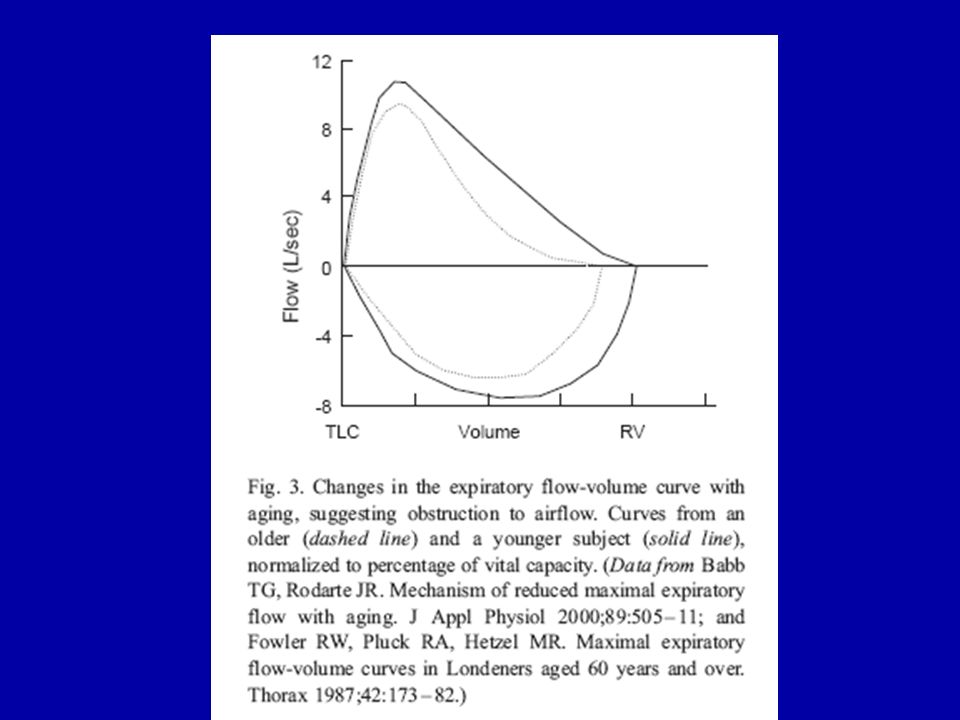
Cambios Fisiológicos Disminuyen las tasas de PEF , y las curvas flujo-volumen sugieren colapso de la vía aérea periférica. El intercambio gaseoso es remarcablemente mejor conservado en reposo y durante el ejercicio a expensas de reducir la superficie alveolar e incrementar el desequilibrio ventilo-perfutorio. Disminución de la sensibilidad de los centros respiratorios a la hipoxemia e hipercapnia, puede resultar en rpta. ventilatoria disminuída en enfermedad aguda o agravar la obstrucción de la vía aérea.

6
Asma en Ancianos Por muchos años considerada enfermedad de niños y jóvenes e infrecuente en la ancianidad. Los Asmáticos ancianos generalmente son aquéllos que adquirieron la enfermedad en la niñez o la adolescencia ,en quienes la enfermedad progresó en el tiempo o se reactivó después de períodos de remisión; sin embargo las primeras manifestaciones de asma pueden ocurrir también después de los 65 años de edad.

7
Asma en Ancianos La presunción de baja prevalencia puede atribuirse a las grandes dificultades para encontrar un diagnóstico correcto en el geronte. Las razones por la que el Asma no es diagnosticado en al adulto mayor , no están claras. Confusión de síntomas Subestimados por el médico Falta de evaluación funcional apropiada. PUEDE DEBERSE A LA CONFUSION CON EPOC

8
Epidemiología Puede ser diagnosticada a cualquier edad y es común en el anciano. Una serie de estudios poblacionales han expuesto que la prevalencia de asma en ancianos es similar a la de otros grupos etáreos 4.5-8%. Diagnosticados como nuevos 0.1% por encima de los 65 años de edad.

9
Asma en el Geronte Puede clasificarse en :
Asma de “inicio tardío” aparición de novo después de los 65 años. Asma de comienzo temprano, continúa una enfermedad que comenzó antes de los 65 años. La relevancia de ésta clasificación es que la enfermedad puede ser severa en persistentes crónicos.

10
Asma en Anciano Diagnóstico
Considerar en todo caso de : Disnea inexplicada Sibilancias Tos nocturna. ( Nivel de Evidencia III ). Revisión cuidadosa en debut reciente : Medicación ASA , AINES ( Nivel de Evidencia II ).
. Revisión cuidadosa en debut reciente : Medicación. ASA , AINES. ( Nivel de Evidencia II ).")
11
Asma en Anciano Diagnóstico
Puede complicarse por diversos factores ,tales como: Síntomas no específicos, comunes a otras patologías. La presencia de enfermedades coexistentes. Diferenciación con EPOC Alteraciones en la percepción de los síntomas en ancianos Menor incidencia de asma y atopía en la tercera edad.

12
Asma en Anciano Diagnóstico
Los tests de función pulmonar tienen un rol muy importante y son fundamentales. Espirometría. Problemas de comprensión y de pobre coordinación afectan sus resultados.

13
Asma en Anciano Diagnóstico
Historia Clínica minuciosa. Laboratorio. Radiografía de tórax frente y perfil. Electrocardiograma. Espirometría. Establecer diagnósticos diferenciales. Puntualizar patologías subyacentes:terapeúticas, dosis, vías, etc.

14
Planes de Tratamiento Consideraciones Especiales
Disminución de la respuesta a estímulos especiales Trastornos de la memoria Pérdida de la coordinación y la fuerza muscular que afecta el uso de algunos dispositivos inhalatorios. Dificultades visuales y auditivas Dificultades del sueño que pueden afectar la esfera cognitiva Trastornos depresivos Elección de la medicación personalizada.

15
Diagnóstico Diferencial
Falla ventricular Izquierda Cáncer pulmonar Reflujo Gastroesofágico Fibrosis Pulmonar Bronquiectasias Tromboembolismo Pulmonar Tuberculosis.

16
Consideraciones Especiales del Manejo Terapeútico
Pacientes polimedicados, mayor cantidad de reacciones adversas e interacciones medicamentosas. Tener en cuenta para las dosis, integridad de la función hepática y renal , para evitar eventos adversos por la metabolización o excreción de las drogas.

17
Objetivos del manejo Prevenir síntomas de asma crónica
Optimizar la función pulmonar Mantener los niveles de actividad normal Minimizar los efectos colaterales de la medicación Reducir o eliminar las exacerbaciones y reconocerlas tempranamente Evitar el agravamiento de las patologías subyacentes.

18
EVENTOS ADVERSOS Beta 2 agonistas: Isquemia miocárdica Arritmias
Hipotensión Tremor Hipokalemia Broncoespasmo paradojal.

19
EVENTOS ADVERSOS Teofilina: Náuseas y vómitos Arritmias Insomnio
Niveles incrementados en enfermedad hepática, interacciones con quinolonas,ketoconazol,macrólidos, antihistamínicos.

20
EVENTOS ADVERSOS Corticoides Sistémicos:
HTA,edemas,falla cardíaca, arritmias. Hiperglicemia Uremia Miopatía Cataratas subcapsular Hipoadrenalismo Alteración de la función cognitiva,depresión. Psicosis, manía. Osteoporosis. Glaucoma Agravamiento de úlcera péptica Atrofia dérmica

21
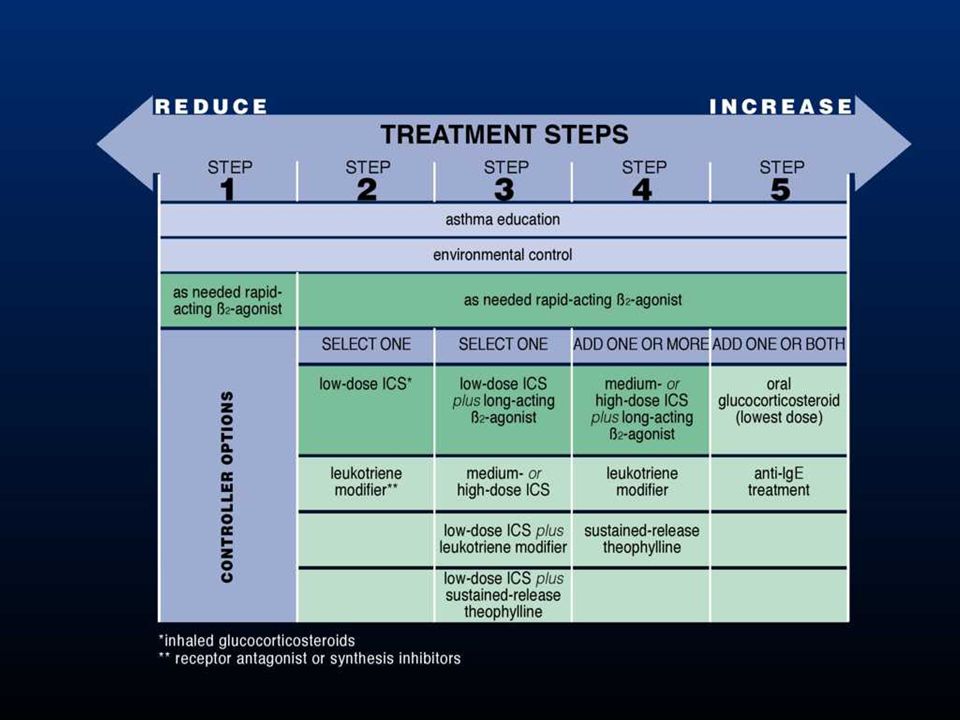
1 2 3 4 5 LEVEL OF CONTROL TREATMENT OF ACTION TREATMENT STEPS REDUCE
controlled partly controlled uncontrolled exacerbation LEVEL OF CONTROL maintain and find lowest controlling step consider stepping up to gain control step up until controlled treat as exacerbation TREATMENT OF ACTION INCREASE TREATMENT STEPS REDUCE INCREASE STEP 1 2 3 4 5

24
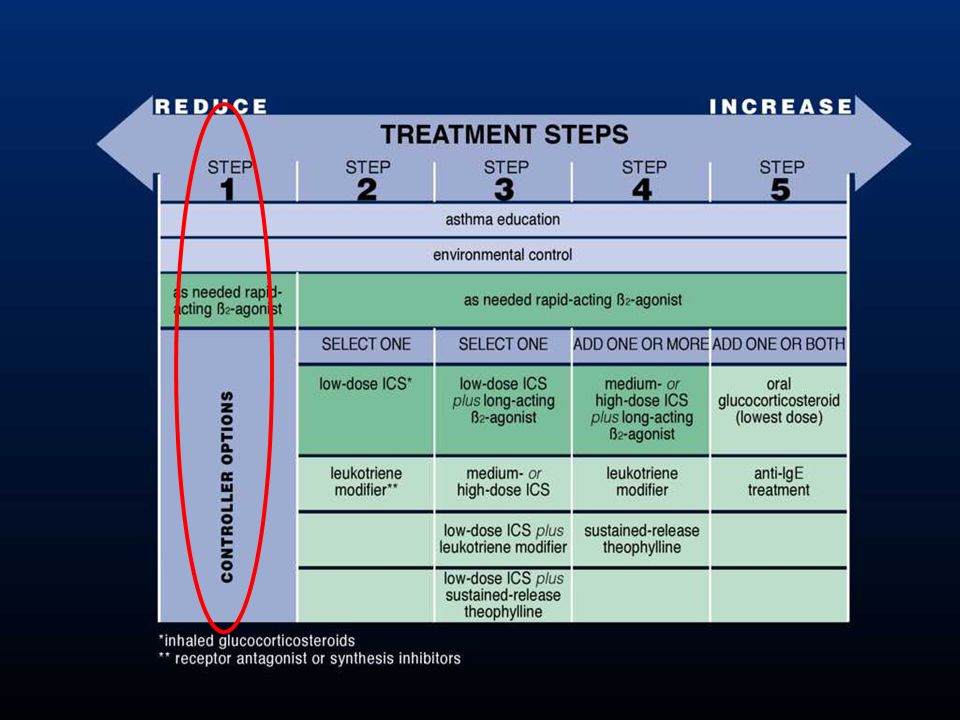
Step 1 – As-needed reliever medication
Treating to Achieve Asthma Control Step 1 – As-needed reliever medication Patients with occasional daytime symptoms of short duration A rapid-acting inhaled β2-agonist is the recommended reliever treatment (Evidence A) When symptoms are more frequent, and/or worsen periodically, patients require regular controller treatment (step 2 or higher)
 When symptoms are more frequent, and/or worsen periodically, patients require regular controller treatment (step 2 or higher)")
26
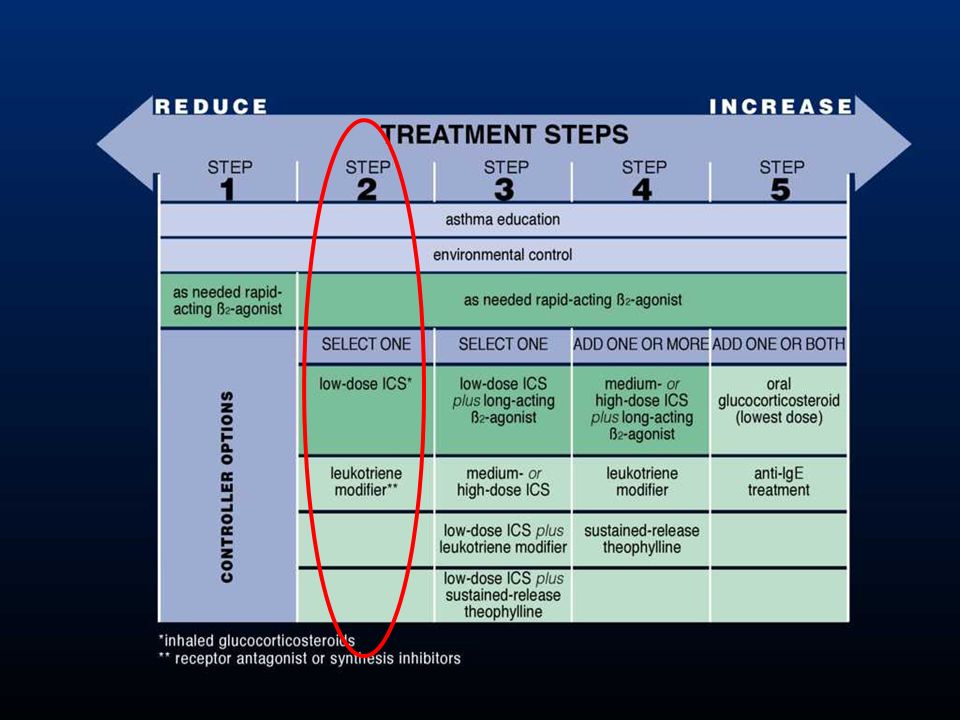
Treating to Achieve Asthma Control
Step 2 – Reliever medication plus a single controller A low-dose inhaled glucocorticosteroid is recommended as the initial controller treatment for patients of all ages (Evidence A) Alternative controller medications include leukotriene modifiers (Evidence A) appropriate for patients unable/unwilling to use inhaled glucocorticosteroids
 Alternative controller medications include leukotriene modifiers (Evidence A) appropriate for patients unable/unwilling to use inhaled glucocorticosteroids.")
28
Treating to Achieve Asthma Control
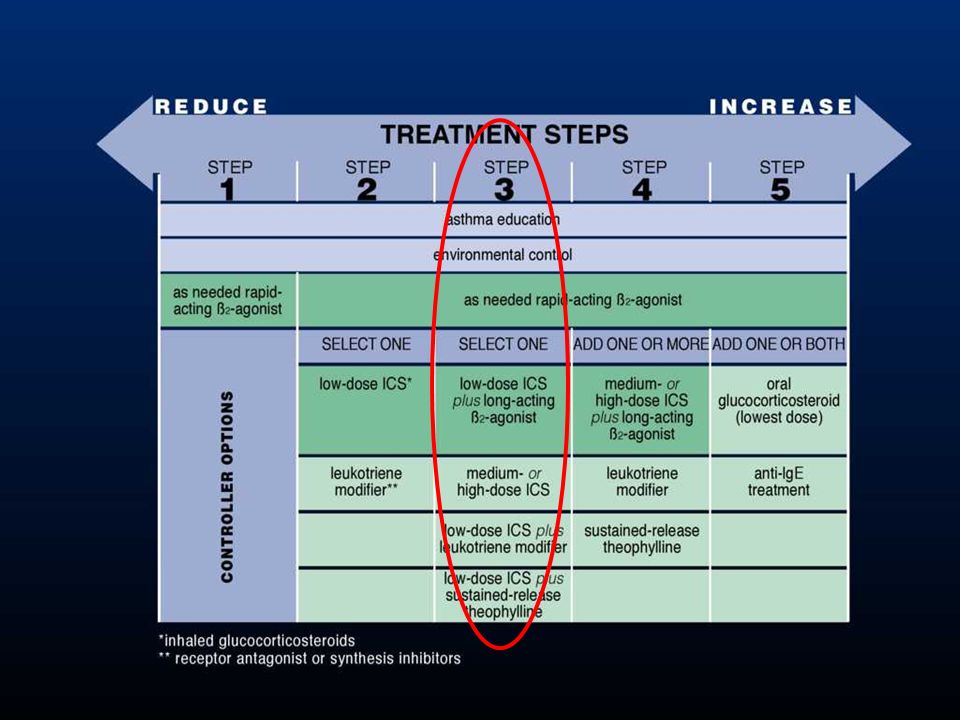
Step 3 – Reliever medication plus one or two controllers For adults and adolescents, combine a low-dose inhaled glucocorticosteroid with an inhaled long-acting β2-agonist either in a combination inhaler device or as separate components (Evidence A) Inhaled long-acting β2-agonist must not be used as monotherapy For children, increase to a medium-dose inhaled glucocorticosteroid (Evidence A)
 Inhaled long-acting β2-agonist must not be used as monotherapy. For children, increase to a medium-dose inhaled glucocorticosteroid (Evidence A)")
29
Treating to Achieve Asthma Control
Additional Step 3 Options for Adolescents and Adults Increase to medium-dose inhaled glucocorticosteroid (Evidence A) Low-dose inhaled glucocorticosteroid combined with leukotriene modifiers (Evidence A) Low-dose sustained-release theophylline (Evidence B)
 Low-dose inhaled glucocorticosteroid combined with leukotriene modifiers (Evidence A) Low-dose sustained-release theophylline (Evidence B)")
31
Treating to Achieve Asthma Control
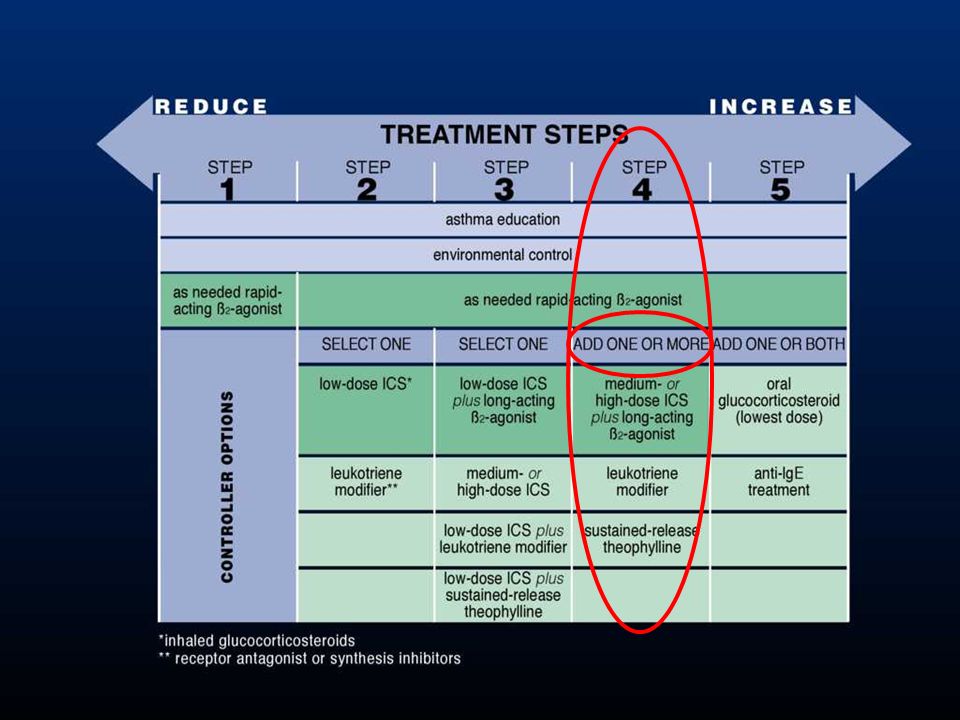
Step 4 – Reliever medication plus two or more controllers Selection of treatment at Step 4 depends on prior selections at Steps 2 and 3 Where possible, patients not controlled on Step 3 treatments should be referred to a health professional with expertise in the management of asthma

32
Treating to Achieve Asthma Control
Step 4 – Reliever medication plus two or more controllers Medium- or high-dose inhaled glucocorticosteroid combined with a long-acting inhaled β2-agonist (Evidence A) Medium- or high-dose inhaled glucocorticosteroid combined with leukotriene modifiers (Evidence A) Low-dose sustained-release theophylline added to medium- or high-dose inhaled glucocorticosteroid combined with a long-acting inhaled β2-agonist (Evidence B)
 Medium- or high-dose inhaled glucocorticosteroid combined with leukotriene modifiers (Evidence A) Low-dose sustained-release theophylline added to medium- or high-dose inhaled glucocorticosteroid combined with a long-acting inhaled β2-agonist (Evidence B)")
34
Treating to Achieve Asthma Control
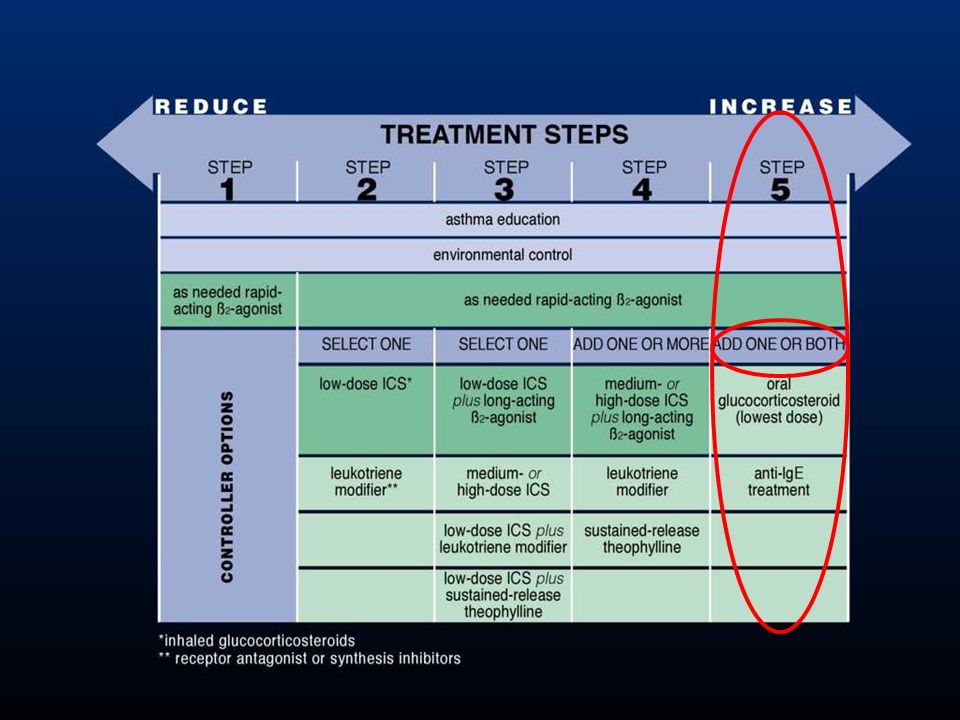
Step 5 – Reliever medication plus additional controller options Addition of oral glucocorticosteroids to other controller medications may be effective (Evidence D) but is associated with severe side effects (Evidence A) Addition of anti-IgE treatment to other controller medications improves control of allergic asthma when control has not been achieved on other medications (Evidence A)
 but is associated with severe side effects (Evidence A) Addition of anti-IgE treatment to other controller medications improves control of allergic asthma when control has not been achieved on other medications (Evidence A)")
35
Treating to Maintain Asthma Control
When control as been achieved, ongoing monitoring is essential to: - maintain control - establish lowest step/dose treatment Asthma control should be monitored by the health care professional and by the patient

36
Treating to Maintain Asthma Control
Stepping down treatment when asthma is controlled When controlled on medium- to high-dose inhaled glucocorticosteroids: 50% dose reduction at 3 month intervals (Evidence B) When controlled on low-dose inhaled glucocorticosteroids: switch to once-daily dosing (Evidence A)
 When controlled on low-dose inhaled glucocorticosteroids: switch to once-daily dosing (Evidence A)")
37
Treating to Maintain Asthma Control
Stepping down treatment when asthma is controlled When controlled on combination inhaled glucocorticosteroids and long-acting inhaled β2-agonist, reduce dose of inhaled glucocorticosteroid by 50% while continuing the long-acting β2-agonist (Evidence B) If control is maintained, reduce to low-dose inhaled glucocorticosteroids and stop long-acting β2-agonist (Evidence D)
 If control is maintained, reduce to low-dose inhaled glucocorticosteroids and stop long-acting β2-agonist (Evidence D)")
38
Treating to Maintain Asthma Control
Stepping up treatment in response to loss of control Rapid-onset, short-acting or long-acting inhaled β2-agonist bronchodilators provide temporary relief. Need for repeated dosing over more than one/two days signals need for possible increase in controller therapy

39
Treating to Maintain Asthma Control
Stepping up treatment in response to loss of control Use of a combination rapid and long-acting inhaled β2-agonist (e.g., formoterol) and an inhaled glucocorticosteroid (e.g., budesonide) in a single inhaler both as a controller and reliever is effecting in maintaining a high level of asthma control and reduces exacerbations (Evidence A) Doubling the dose of inhaled glucocortico-steroids is not effective, and is not recommended (Evidence A)
 and an inhaled glucocorticosteroid (e.g., budesonide) in a single inhaler both as a controller and reliever is effecting in maintaining a high level of asthma control and reduces exacerbations (Evidence A) Doubling the dose of inhaled glucocortico-steroids is not effective, and is not recommended (Evidence A)")
40
Asthma Management and Prevention Program Component 3: Assess, Treat and Monitor Asthma – Children 5 Years and Younger Childhood and adult asthma share the same underlying mechanisms. However, because of processes of growth and development, effects of asthma treatments in children differ from those in adults.

41
Asthma Management and Prevention Program Component 3: Assess, Treat and Monitor Asthma – Children 5 Years and Younger Many asthma medications (e.g. glucocorticosteroids, β2- agonists, theophylline) are metabolized faster in children than in adults, and younger children tend to metabolize medications faster than older children
 are metabolized faster in children than in adults, and younger children tend to metabolize medications faster than older children.")
42
Asthma Management and Prevention Program Component 3: Assess, Treat and Monitor Asthma – Children 5 Years and Younger Long-term treatment with inhaled glucocorticosteroids has not been shown to be associated with any increase in osteoporosis or bone fracture Studies including a total of over 3,500 children treated for periods of 1 – 13 years have found no sustained adverse effect of inhaled glucocorticosteroids on growth

43
Asthma Management and Prevention Program Component 3: Assess, Treat and Monitor Asthma – Children 5 Years and Younger Rapid-acting inhaled β2-agonists are the most effective reliever therapy for children These medications are the most effective bronchodilators available and are the treatment of choice for acute asthma symptoms

44
Asthma Management and Prevention Program Component 4: Manage Asthma Exacerbations
Exacerbations of asthma are episodes of progressive increase in shortness of breath, cough, wheezing, or chest tightness Exacerbations are characterized by decreases in expiratory airflow that can be quantified and monitored by measurement of lung function (FEV1 or PEF) Severe exacerbations are potentially life-threatening and treatment requires close supervision
 Severe exacerbations are potentially life-threatening and treatment requires close supervision.")
45
Treatment of exacerbations depends on: The patient
Asthma Management and Prevention Program Component 4: Manage Asthma Exacerbations Treatment of exacerbations depends on: The patient Experience of the health care professional Therapies that are the most effective for the particular patient Availability of medications Emergency facilities

46
Primary therapies for exacerbations:
Asthma Management and Prevention Program Component 4: Manage Asthma Exacerbations Primary therapies for exacerbations: Repetitive administration of rapid-acting inhaled β2-agonist Early introduction of systemic glucocorticosteroids Oxygen supplementation Closely monitor response to treatment with serial measures of lung function

47
Asthma Management and Prevention Program Special Considerations
Special considerations are required to manage asthma in relation to: Pregnancy Surgery Rhinitis, sinusitis, and nasal polyps Occupational asthma Respiratory infections Gastroesophageal reflux Aspirin-induced asthma Anaphylaxis and Asthma

48
Asthma Management and Prevention Program: Summary
Asthma can be effectively controlled in most patients by intervening to suppress and reverse inflammation as well as treating bronchoconstriction and related symptoms Although there is no cure for asthma, appropriate management that includes a partnership between the physician and the patient/family most often results in the achievement of control

49
Asthma Management and Prevention Program: Summary
A stepwise approach to pharmacologic therapy is recommended. The aim is to accomplish the goals of therapy with the least possible medication The availability of varying forms of treatment, cultural preferences, and differing health care systems need to be considered

50
EPOC y Asma en Ancianos Comparten similitudes clínicas y funcionales
Presentaciones patológicas diferentes : dos enfermedades distintas. No se puede excluir la coexistencia de ambas enfermedades. Importante reconocerlas y distinguirlas tempranamente para el tratamiento apropiado.

51
PREVENCION DE LA MORTALIDAD EN EPOC
Cesación de Fumar Vacunación Influenza Oxigenoterapia a largo plazo Tratamiento Farmacológico de la EPOC Tratamiento Farmacológico de comorbilidades Tratamiento de las exacerbaciones NUEVOS TRATAMIENTOS PARA EPOC Y ENFERMEDADES CRONICOS.

52
EPOC es la unica causa de muerte que se ha incrementado significativamente en los últimos años.
Cambio en edad ajustado a tasa de muerte en USA, de 1965 a 1998 (%) +163 160 120 80 40 These data from the USA, collected from 1965 to 1998, show a 163% increase in age-adjusted death rates from chronic obstructive pulmonary disease (COPD). While the death rate is declining from diseases such as coronary heart disease (CHD) (a 59% decrease) and cerebrovascular disease (CVD) (a 35% decrease), the death rate from COPD is increasing markedly. All other causes of age-adjusted US deaths also saw a decline of 7%. It may that this is partly a feature of increased recognition of COPD including an increase in the mention of the term on death certificates, but this does not detract from the overall trends illustrated in the figure. The Global Burden of Disease (GBD) study attributed more than 2.2 million deaths to COPD in 1990 (4.4% of worldwide deaths), ranking COPD as the sixth most serious cause of worldwide mortality.1 Furthermore, the 2004 World Health Organization (WHO) report indicated that COPD deaths are on the increase, with over 2.7 million deaths (4.8%) in Even more concerning, COPD deaths are projected to rise to third place in the worldwide ranking with 4.5 million deaths in The 2004 American Lung Association Report estimated approximately 120,000 deaths in the USA in The European Lung White Book, the first comprehensive survey on respiratory health in Europe, estimated annual COPD mortality in Europe as 200,000–300,000.4 References Murray CJ, Lopez AD. Alternative projections of mortality and disability by cause 1990–2020: Global Burden of Disease Study. Lancet 1997;349:1498–504. World Health Organization. The World Health Report: Changing History American Lung Association Epidemiology and Statistics Unit Research and Scientific Affairs. Trends in Chronic Bronchitis and Emphysema: Morbidity and Mortality. November 2004. European Lung White Book: The First Comprehensive Survey on Respiratory Health in Europe. Editor in chief R Loddenkemper. ERSJ Ltd. 2003;34–43. –7 –40 –35 –59 –80 –64 ECA Stroke ECV EPOC Todas las otras causas Adapted from:
 These data from the USA, collected from 1965 to 1998, show a 163% increase in age-adjusted death rates from chronic obstructive pulmonary disease (COPD). While the death rate is declining from diseases such as coronary heart disease (CHD) (a 59% decrease) and cerebrovascular disease (CVD) (a 35% decrease), the death rate from COPD is increasing markedly. All other causes of age-adjusted US deaths also saw a decline of 7%. It may that this is partly a feature of increased recognition of COPD including an increase in the mention of the term on death certificates, but this does not detract from the overall trends illustrated in the figure. The Global Burden of Disease (GBD) study attributed more than 2.2 million deaths to COPD in 1990 (4.4% of worldwide deaths), ranking COPD as the sixth most serious cause of worldwide mortality.1 Furthermore, the 2004 World Health Organization (WHO) report indicated that COPD deaths are on the increase, with over 2.7 million deaths (4.8%) in Even more concerning, COPD deaths are projected to rise to third place in the worldwide ranking with 4.5 million deaths in The 2004 American Lung Association Report estimated approximately 120,000 deaths in the USA in The European Lung White Book, the first comprehensive survey on respiratory health in Europe, estimated annual COPD mortality in Europe as 200,000–300, References. Murray CJ, Lopez AD. Alternative projections of mortality and disability by cause 1990–2020: Global Burden of Disease Study. Lancet 1997;349:1498–504. World Health Organization. The World Health Report: Changing History American Lung Association Epidemiology and Statistics Unit Research and Scientific Affairs. Trends in Chronic Bronchitis and Emphysema: Morbidity and Mortality. November European Lung White Book: The First Comprehensive Survey on Respiratory Health in Europe. Editor in chief R Loddenkemper. ERSJ Ltd. 2003;34–43. –7. –40. –35. –59. –80. –64. ECA. Stroke. ECV. EPOC. Todas las. otras. causas. Adapted from:")
53
EPOC está proyectado a ser el tercer más grande asesino para el 2020
1990 2020 Enf. Isquémica cardíaca Enfermedad CVD Infección Respiratoria Enfermedad Diarreica Desórdenes Perinatales EPOC Tuberculosis Measles Accidentes de tránsito Cáncer Pulmonar 3ro 6to As part of the Global Burden of Disease Study, Murray and Lopez1 projected future mortality rates based on the most common causes of death in The top 10 most important causes of death are presented in this slide. The majority of these leading causes of deaths are projected to remain stable or decline. Notably, COPD is expected to rise from the sixth biggest killer in 1990 to the third in Of the top 10 leading causes of death in 1990, only deaths caused by COPD, lung cancer and road traffic accidents are projected to rise. Reference Murray CJ, Lopez AD. Alternative projections of mortality and disability by cause 1990–2020: Global Burden of Disease Study. Lancet 1997;349:1498–504. Cancer de Estómago HIV Suicidio Murray & Lopez 1997

54
Resultados de las Exacerbaciones de la EPOC
Mortalidad Hospitalaria 20%-24% (1 año) En pacientes UCI En pacientes Hospitalizados Mortalidad Hospitalaria 2.5%-10% (5 días) Treatment failure is defined as not responsive to initial treatment(s). Outcomes = health utilizations. This slide shows outcomes of patients with acute exacerbations: 20-24% of patients in the ICU with an exacerbation died; 6-12% of patients in general hospital beds, not ICU beds, died. Of those who visited the ER for an acute exacerbation, 22-32% of those patients had to revisit the emergency room after being discharged. Those who were treated as outpatients 13-33% of those patients did not response to initial treatments and needed further medical intervention. Main point: Acute exacerbations are a serious matter and should be of concern to the health care provider. Recaída 22%-32% (14 días) En pacientes en Emergencia Tasa de falla al tratamiento 13%-33% (14 días) Ambulatorios Seneff MG, Wagner DP, Wagner RP, Zimmerman JE, Knaus WA. Hospital and 1-year survival of patients admitted to intensive care units with acute exacerbation of chronic obstructive pulmonary disease. JAMA. 1995;274: Murata GH, Gorby MS, Chick TW, Halperin AK. Treatment of decompensated chronic obstructive pulmonary disease in the emergency department—correlation between clinical features and prognosis. Ann Emerg Med. 1991;20: Adams SG, Melo J, Luther M, Anzueto A. Antibiotics are associated with lower relapse rates in outpatients with acute exacerbations of COPD. Chest. 2000;117: Patil SP, Krishnan JA, Lechtzin N, Diette GB. In-hospital mortality following acute exacerbations of chronic obstructive pulmonary disease. Arch Int Med. 2003; 160: Seneff et al. JAMA. 1995; 274: ; Murata et al. Ann Emerg Med. 1991;20: ; Adams et al. Chest. 2000; 117: ; Patil et al. Arch Int Med. 2003; 163:
 En pacientes UCI. En pacientes Hospitalizados. Mortalidad Hospitalaria. 2.5%-10% (5 días) Treatment failure is defined as not responsive to initial treatment(s). Outcomes = health utilizations. This slide shows outcomes of patients with acute exacerbations: 20-24% of patients in the ICU with an exacerbation died; 6-12% of patients in general hospital beds, not ICU beds, died. Of those who visited the ER for an acute exacerbation, 22-32% of those patients had to revisit the emergency room after being discharged. Those who were treated as outpatients 13-33% of those patients did not response to initial treatments and needed further medical intervention. Main point: Acute exacerbations are a serious matter and should be of concern to the health care provider. Recaída. 22%-32% (14 días) En pacientes en Emergencia. Tasa de falla al tratamiento. 13%-33% (14 días) Ambulatorios. Seneff MG, Wagner DP, Wagner RP, Zimmerman JE, Knaus WA. Hospital and 1-year survival of patients admitted to intensive care units with acute exacerbation of chronic obstructive pulmonary disease. JAMA. 1995;274: Murata GH, Gorby MS, Chick TW, Halperin AK. Treatment of decompensated chronic obstructive pulmonary disease in the emergency department—correlation between clinical features and prognosis. Ann Emerg Med. 1991;20: Adams SG, Melo J, Luther M, Anzueto A. Antibiotics are associated with lower relapse rates in outpatients with acute exacerbations of COPD. Chest. 2000;117: Patil SP, Krishnan JA, Lechtzin N, Diette GB. In-hospital mortality following acute exacerbations of chronic obstructive pulmonary disease. Arch Int Med. 2003; 160: Seneff et al. JAMA. 1995; 274: ; Murata et al. Ann Emerg Med. 1991;20: ; Adams et al. Chest. 2000; 117: ; Patil et al. Arch Int Med. 2003; 163:")
55
EPOC versus edad 40-49 50-59 >=60 p < 0,001 SP MX MN SANT CARAC
32 30 26 18 23 SP MX MN SANT CARAC

56
TABACO EN EL PERÚ: MAGNITUD DEL PROBLEMA
Se estima que aproximadamente 8´000,000 de peruanos ha probado tabaco 1´000,000 de fumadores 500,000 dependientes de tabaco 50,000 adolescentes se inician como fumadores cada año MINISTERIO DE SALUD – PERÚ / NOTABACO CENTER PERÚ / DEVIDA 2002

57
TABACO EN EL PERU: MAGNITUD DEL PROBLEMA
Proporción varón / mujer 3/1 En menores de 18 años la proporción es 2/1 40% de la población peruana ha tenido exposición involuntaria a humo de tabaco PLAN NACIONAL PARA PREVENCION Y CONTROL DE TABAQUISMO EN EL PERU MINSA / COLAT/ OPS – DEVIDA

58
Estudio Prepocol – EPOC en Colombia Análisis de multivarianza (5
Estudio Prepocol – EPOC en Colombia Análisis de multivarianza (5.539 adultos) Variables Odds ratio IC95% Valor de p EDAD (≥ 60 años vs < 60 años) 3.74 <0.001 Tuberculosis 3.19 1.70 – 5.98 Tabaquismo (alguna vez vs nunca) 2.74 Escolaridad (nunca vs alguna) 2.03 Tabaquismo pasivo 1.70 0.003 Sexo (hombres vs. mujeres) 1.68 Leña (≥10 años vs < 10 años) 1.40 1.13 – 1.73 Caballero A. et al. Arch Bronconeumol 2004; 40(4):20
 Variables. Odds ratio. IC95% Valor de p. EDAD. (≥ 60 años vs < 60 años) < Tuberculosis – Tabaquismo. (alguna vez vs nunca) Escolaridad. (nunca vs alguna) Tabaquismo pasivo Sexo. (hombres vs. mujeres) Leña. (≥10 años vs < 10 años) – Caballero A. et al. Arch Bronconeumol 2004; 40(4):20.")
59
Incidence of COPD by age
Johannesen A, ERJ 2002

60
Estimated cumulative 9 years incidence and adjusted odds
ratios of COPD in Bergen, Norway 6.7 ( ) 245 smokers 2.2 ( ) 163 ex-smokrs 1 507 never Smoking 10.6 (4.3-26) 130 60-74 3.4 ( ) 210 45-59 2.1 ( ) 333 30-44 242 18-29 Age (years in 1987/88) 1.5 ( ) 474 men 441 women Gender Adjusted odds ratio (95% CI)* Popltn at risk * Adjusted for gender, age and smoking habits.
 245. smokers. 2.2 ( ) 163. ex-smokrs never. Smoking (4.3-26) ( ) ( ) Age (years in 1987/88) 1.5 ( ) 474. men women. Gender. Adjusted odds ratio. (95% CI)* Popltn at risk. * Adjusted for gender, age and smoking habits.")
61
Prevalence of COPD by age and smoking
Lindberg A, Respir Med 2005

64
Rasgos Sistémicos del EPOC
Stress Oxidativo Sistémico. Incremento de los niveles plasmáticos de citoquinas pro inflamatorias Células inflamatorias circulantes. Mecanismos de Inflamación Sistémica.

65
Metas del Manejo de EPOC
Prevenir la progresión de la enfermedad Aliviar síntomas Mejorar la tolerancia al ejercicio Mejorar el estado de salud Prevenir y tratar las complicaciones Prevenir y tratar las exacerbaciones Reducir la mortalidad Prevenir o minimizar los efectos colaterales del tratamiento The key goals of COPD treatment are included in the GOLD guidelines. GOLD: Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. NIH publication No. 2701, March 2001. Adapted from the GOLD Workshop Report 2003

68
EXPOSICION A FACTORES DE RIESGO
EPOC: Diagnóstico EXPOSICION A FACTORES DE RIESGO SINTOMAS Tos Tabaco Esputo Ocupación Disnea Polución è ESPIROMETRIA

69
Clasificación de severidad
Estadio Características 0: At risk Normal spirometry Chronic symptoms (cough, sputum) I: Leve FEV1/FVC < 70%; FEV1 ³ 80% predicted With or without symptoms (cough, sputum) II: Moderado FEV1/FVC < 70%; 30% £ FEV1 < 80% predicted (IIA: 50% £ FEV1 < 80% predicted; IIB: 30% £ FEV1 < 50% predicted) With or without chronic symptoms (cough, sputum, dyspnea) III: Severo FEV1/FVC < 70%; FEV1 < 30% predicted or FEV1 < 50%predicted plus respiratory failure or clinical signs of right heart failure
 I: Leve FEV1/FVC < 70%; FEV1 ³ 80% predicted With or without symptoms (cough, sputum) II: Moderado FEV1/FVC < 70%; 30% £ FEV1 < 80% predicted. (IIA: 50% £ FEV1 < 80% predicted; IIB: 30% £ FEV1 < 50% predicted) With or without chronic symptoms (cough, sputum, dyspnea) III: Severo FEV1/FVC < 70%; FEV1 < 30% predicted or FEV1 < 50%predicted plus respiratory failure or clinical signs of right heart failure.")
70
EPOC: Manejo Cese definitivo del consumo de cigarrillo
Evitar la exposición pasiva Evaluación ocupacional Manejo psicológico

71
EPOC: Manejo Uso de broncodilatadores; beta-2 agonistas, anticolinérgicos,teofilina y combinaciones. Terapia inhalatoria es preferible Priorizar uso de beta-2 agonistas de larga acción (vg. Formoterol, salmeterol) Individualizar la terapia Evaluar uso de corticosteroides y de antibióticos
 Individualizar la terapia. Evaluar uso de corticosteroides y de antibióticos.")
72
EPOC: Manejo La administración de oxígeno (> 15 horas/día) mejora la supervivencia. Ejercicios respiratorios Vacuna anti-influenza Manejo de las complicaciones

73
EPOC: Manejo Estadio 0 Caracteristicas Terapia recomendada
Síntomas crónicos - Tos - Esputo Sin anormalidad espirométrica Medidas generales Sintomáticos

74
EPOC: Manejo Estadio I: EPOC leve
Caracteristicas Terapia recomendada FEV1/FVC < 70 % FEV1 > 80 % predicted With or without symptoms Beta-2 agonistas de acción rápida

75
EPOC: Manejo Estadio IIA: EPOC moderado
Caracteristicas Terapia recomendada FEV1/FVC < 70% 50% < FEV1< 80% prefijado Con o sin síntomas Uno o más broncodilatadores Rehabilitación Corticosteroides inhalatorios según respuesta

76
EPOC: Manejo Estadio IIB: EPOC moderado
Caracteristicas Terapia recomendada FEV1/FVC < 70% 30% < FEV1 < 50% prefijado Con o sin síntomas Uno o más broncodilatadores Rehabilitación Corticosteroides inhalatorios

77
EPOC: Manejo Estadio III: EPOC Severo
Caracteristicas Terapia recomendada FEV1/FVC < 70% FEV1 < 30% prefijado o falla cardiaca o falla respiratoria Uso regular de broncodilatadores y de corticosteroides Tratar complicaciones Rehabilitación Oxigenoterapia Considerar cirugía

78
EPOC: EXACERBACIÓN Tos productiva, fiebre, disnea
Se benefician con antibióticos Mayor riesgo de neumonía Deben hospitalizarse (Rayos-X, gasometría)
")
Presentaciones similares



 European Transfer Credit System (ECTS) Methodology in.>")

















