Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Curso Superior AMA Modulo Renal 2016
SINDROME NEFROTICO Curso Superior AMA Modulo Renal 2016

2
EL NEFRON

3
EL GLOMERULO Looking more carefully at the glomerulus here then in cross-section, we can see on the left a diagram showing again the arteriole or small artery entering the glomerulus, then this tangle of capillaries, which are cut in cross-section here so we are just seeing them as circular units, and then the blood exiting. To the right is a diagram of just one glomerular capillary. Within the lumen of that capillary are red blood cells, white blood cells, and protein molecules, as well as other important components of the blood. Those elements need to be retained within the capillary. The pressure gradient across that capillary will cause fluid and very tiny molecules to cross into the filtrate that enters the urinary space.

4
EL GLOMERULO How a glomerulus looks under the microscope Here is an actual histologic section of a glomerulus from a patient who underwent a renal biopsy. This glomerulus has relatively normal appearance here, and you can see what it looks like in an actual tissue section that would be examined by the pathologist who was determining what the cause for renal disease might be in that patient. You can see a small artery, an arteriole, coming in over in the right- hand bottom corner. You can even see some red blood cells in the lumen, and then the little capillaries with their delicate walls, and the arteriole exiting over at about 7 o'clock in that photomicrograph.

5
CAPILAR GLOMERULAR NORMAL
The normal glomerular capillary In this diagram then, the green is the epithelial cell; the dark grey is the basement membrane, which is the major barrier that prevents proteins from being lost; the endothelial cell is in yellow, lining the lumen; and the red cell is called a mesangial cell, which sort of supports the capillaries and the glomeruli and has some other functions and can respond to injury by increasing in numbers. You can have mesangial proliferation, as we will discuss

6
BARRERA GLOMERULAR PARA LAS PROTEINAS
Barriers to passage of protein from the glomerular capillary In this diagram, we can see these barriers to proteinuria that need to be disturbed to cause glomerular proteinuria. There is this glomerular basement membrane, the GBM, which is the main barrier. There is the endothelial cell, which at real high magnification actually has holes in it, fenestrations in it, so it is not much of a barrier. The epithelial cell actually has what are called foot processes. They are little extensions that come down to the surface of the capillary. If you cut them in cross section, they look like little feet. Actually we will see that they are fused when there is proteinuria, so there is a change in those cells. But the major barrier to proteinuria is that basement membrane

7
Factores que previenen la proteinuria glomerular
El relativo gran tamaño de la mayoría de las proteinas plasmáticas previene el pasaje a través de los “poros funcionales” de la membrana basal glomerular La carga eléctrica negativa de la mayoría de las proteinas plasmáticas hace que sean repelidas por la pared capilar cargada negativamente. What factors normally prevent us from losing too much protein? As Dr. Toto pointed out, one thing is the size of the protein molecules relative to the functional pore size of this glomerular basement membrane. If you look at that glomerular basement membrane, you really can't see the pores in it. But by testing whether certain sized molecules can go through it, you can determine there is a functional pore size. The proteins in the circulation are mostly too large to go through those functional pore sizes. Also, there is an electrical charge on protein molecules and cells and tissues. It is mainly a negative charge. Like charges repel each other. So the plasma proteins are negatively charged, and the capillary wall is negatively charged. That tends to repel the proteins from getting into these pores and getting through. This pore size and negative charge normally keep proteins from crossing

8
Manejo glomerular de las proteinas
El glomerulo es el sitio de ultrafiltración plasmática. La presión hidrostática de la sangre dentro de los capilares fuerza el líquido hacia afuera, a través de la porosas paredes capilares. La membrana basal glomerular es semipermeable, esto es, pequeñas moléculas pueden pasar pero las grandes moléculas no. La albúmina sérica (PM ) y otras proteínas plasmáticas son demasiado grandes para pasar en condiciones normales
 y otras proteínas plasmáticas son demasiado grandes para pasar en condiciones normales.")
9
Patogénesis

12
Manejo tubular de las proteinas
El túbulo renal es el sitio de reabsorción del líquido, proteínas y otras sustancias. El proceso de reabsorción reduce el volumen del filtrado y cambia su composición. Las moléculas más esenciales (como las proteínas) son recuperadas del filtrado. Casi todas las proteínas filtradas son reabsorbidas.
 son recuperadas del filtrado. Casi todas las proteínas filtradas son reabsorbidas.")
13
Proteínas urinarias: valores normales
En adultos, la proteinuria anormal puede definirse como la excreción de más de 150 mg de proteínas en 24 hs. En niños, la proteinuria anormal es menor que en adultos: aprox 100 mg/m2 de sup corporal por día.

14
Proteinas urinarias en la enfermedad renal
En la enfermedad renal la proteina urinaria puede variar desde valores normales a más de 30 gr por día !

15
Medición de proteínas en orina
La medición de las proteínas en orina es uno de los tests más útiles para detectar y seguir las enfermedades renales. El test de screening más común para la proteinuria es el testeo de una sola muestra al azar con una tira reactiva

16
La proteinuria resulta de uno o más de estos cuatro mecanismos
1) Daño de la membrana basal glomerular 2) Impedimento en la reabsorción de las células tubulares 3) Secreción de proteínas por parte de las células tubulares 4) Filtración de proteínas anormales pequeñas
 Daño de la membrana basal glomerular. 2) Impedimento en la reabsorción de las células tubulares. 3) Secreción de proteínas por parte de las células tubulares. 4) Filtración de proteínas anormales pequeñas.")
17
Caso Clínico 37 años, sexo femeino
Consulta por edema de pies y tobillos. Nota espuma en la orina. Anteced, de HTA leve Sin antec familiares de enf. Renal Ex Fisico: Peso 72 Kg, Talla 1.6 m, TA 170/90 Auscultación cardíaca y torácica s/p Ex físico: 4(+) edema en tobillo y pre tibial would like to begin with a brief case presentation. This is a 37-year old African-American woman who is a lab technician who presented with swelling of her feet and ankles for the past one to two weeks. She noted that her urine had become bubbly recently. Her past medical history was significant only for mild high blood pressure, controlled with a thiazide diuretic. Her review of systems was otherwise negative and there was no history of kidney disease in her family. On physical exam her weight as 198 lbs, height of 5' 6" and her blood pressure was 170/90 with a heart rate of 82. Her head and neck exam was negative, her heart was regular with a normal S1 and S2 and there were no murmurs, rubs nor gallops appreciated. Her lungs were clear. Her abdomen was obese, non-tender and otherwise unremarkable. And she had 4+ pitting edema in her ankles and the pre-tibial area. Case Presentation: Urinalysis and laboratory data Her urinalysis demonstrated a specific gravity of with a pH of 6. There was 1+ blood on the dipstick and 3+ albumin. Under microscopy 5-10 red blood cells were noted as well as white blood cells. There were moderate epithelial cells but no dysmorphic red cells or red cells casts were noted. Laboratory data included a white count of 7.6; a hemoglobin of 11.4; platelets of 284. Her BUN creatinine was 32/4.1; there was no previous creatinine that we knew about. Albumin was 2.7, cholesterol was 431, and the spot urinary protein to creatinine ratio was 682/57, which translates to about 11 g/day of protein excretion. On ultrasound her kidneys were 12 cm bilaterally and noted to be somewhat echogenic. Serologies that were sent included HIV, hepatitis B and C, ANA, rheumatoid factor, cryoglobulins, UPEP and SPEP were all negative.
 edema en tobillo y pre tibial. would like to begin with a brief case presentation. This is a 37-year old African-American woman who is a lab technician who presented with swelling of her feet and ankles for the past one to two weeks. She noted that her urine had become bubbly recently. Her past medical history was significant only for mild high blood pressure, controlled with a thiazide diuretic. Her review of systems was otherwise negative and there was no history of kidney disease in her family. On physical exam her weight as 198 lbs, height of 5 6 and her blood pressure was 170/90 with a heart rate of 82. Her head and neck exam was negative, her heart was regular with a normal S1 and S2 and there were no murmurs, rubs nor gallops appreciated. Her lungs were clear. Her abdomen was obese, non-tender and otherwise unremarkable. And she had 4+ pitting edema in her ankles and the pre-tibial area. Case Presentation: Urinalysis and laboratory data Her urinalysis demonstrated a specific gravity of with a pH of 6. There was 1+ blood on the dipstick and 3+ albumin. Under microscopy 5-10 red blood cells were noted as well as white blood cells. There were moderate epithelial cells but no dysmorphic red cells or red cells casts were noted. Laboratory data included a white count of 7.6; a hemoglobin of 11.4; platelets of 284. Her BUN creatinine was 32/4.1; there was no previous creatinine that we knew about. Albumin was 2.7, cholesterol was 431, and the spot urinary protein to creatinine ratio was 682/57, which translates to about 11 g/day of protein excretion. On ultrasound her kidneys were 12 cm bilaterally and noted to be somewhat echogenic. Serologies that were sent included HIV, hepatitis B and C, ANA, rheumatoid factor, cryoglobulins, UPEP and SPEP were all negative.")
18
Caso Clínico Analisis de orina y sangre
Urea 70 mg/dl, Creatinina 1.5 mg/dl Albumina 2.7, Colesterol 300 Tira reactiva 1+GR y 3+ albúmina Sed orina: 5-10 GR/cpo, no dismorficos No cilindros hematicos. Ecografía: aumento ecogenicidad HIV, HCV, HB, FAN, Anti DNA neg. Case Presentation: Urinalysis and laboratory data Her urinalysis demonstrated a specific gravity of with a pH of 6. There was 1+ blood on the dipstick and 3+ albumin. Under microscopy 5-10 red blood cells were noted as well as white blood cells. There were moderate epithelial cells but no dysmorphic red cells or red cells casts were noted. Laboratory data included a white count of 7.6; a hemoglobin of 11.4; platelets of 284. Her BUN creatinine was 32/4.1; there was no previous creatinine that we knew about. Albumin was 2.7, cholesterol was 431, and the spot urinary protein to creatinine ratio was 682/57, which translates to about 11 g/day of protein excretion. On ultrasound her kidneys were 12 cm bilaterally and noted to be somewhat echogenic. Serologies that were sent included HIV, hepatitis B and C, ANA, rheumatoid factor, cryoglobulins, UPEP and SPEP were all negative

19
Condiciones en las que hay proteinuria

20
Proteinuria funcional
La proteinuria funcional puede ocurrir en personas normales luego de ejercicio extenuante, exposición a calor o frio extremos, stress emocional, y en estados febriles Se cree que el mecanismo es un aumento de la permeabilidad de los glomerulos con disminución de la absorción tubular Functional proteinuria: nothing to worry about Functional proteinuria refers to a condition that is really essentially normal. It is due to certain circumstances that cause the capillary of the glomerulus to leak protein. They are normal effects of living in our environment. So, for instance, excessive exercise, stress of excessive heat or excessive cold, can lead to increases in the amount of protein that is filtered and excreted into the urine. This is generally not considered a disease phenomenon because it is short lived, goes away, and really has no significant clinical consequences. The mechanism by which this takes place is believed to be due to a transient increase in the permeability, that is the membrane allowing protein to pass through it.

21
Proteinuria postural (ortostática)
La proteinuria postural (ortostática) ocurre en un pequeño porcentaje de personas aparentemente normales. La proteinuria está presente cuando el paciente está de pie pero desaparece cuando está acostado. El mecanismo presuntamente se debe a obstrucción parcial temporal de las venas renales. A pesar de que la proteinuria puede persistir, el pronóstico a largo plazo usualmente es benigno. Changes in urine protein excretion on standing (postural proteinuria) Postural proteinuria is a relatively common phenomenon. As far as its pathological significance is concerned, it is kind of controversial. It is a problem because some individuals have this condition. It becomes scary because it goes on for a long period of time. It is not a transient phenomenon, and we really don't know exactly what the mechanisms are. What it means is, that during the daytime when an individual is in the upright position and the urine is collected, we find abnormal amounts of albumin in the urine. It is excessive. The glomerulus is leaking albumin. But when the subject with this condition lies down and goes to sleep at night, the excess protein filtration and excretion by the kidney seems to go away. At least it is dampened substantially. Although the mechanism has not been clear, it is presumably due to some partial temporary obstruction of the veins to the kidney, which is where the blood goes out of the kidney. Dr. Jennette will show you that in a minute. The condition is generally not a serious one. Children or adults who have this condition don't seem to have any long-term consequences from it in terms of kidney disease. I said it is scary because it doesn't seem to go away in a lot of people. You worry--does this harbinger a kidney disease? But individuals can have this condition for a long, long time, and it doesn't seem to lead to kidney damage or their going on a dialysis machine or needing a kidney transplant.
 ocurre en un pequeño porcentaje de personas aparentemente normales. La proteinuria está presente cuando el paciente está de pie pero desaparece cuando está acostado. El mecanismo presuntamente se debe a obstrucción parcial temporal de las venas renales. A pesar de que la proteinuria puede persistir, el pronóstico a largo plazo usualmente es benigno. Changes in urine protein excretion on standing (postural proteinuria) Postural proteinuria is a relatively common phenomenon. As far as its pathological significance is concerned, it is kind of controversial. It is a problem because some individuals have this condition. It becomes scary because it goes on for a long period of time. It is not a transient phenomenon, and we really don t know exactly what the mechanisms are. What it means is, that during the daytime when an individual is in the upright position and the urine is collected, we find abnormal amounts of albumin in the urine. It is excessive. The glomerulus is leaking albumin. But when the subject with this condition lies down and goes to sleep at night, the excess protein filtration and excretion by the kidney seems to go away. At least it is dampened substantially. Although the mechanism has not been clear, it is presumably due to some partial temporary obstruction of the veins to the kidney, which is where the blood goes out of the kidney. Dr. Jennette will show you that in a minute. The condition is generally not a serious one. Children or adults who have this condition don t seem to have any long-term consequences from it in terms of kidney disease. I said it is scary because it doesn t seem to go away in a lot of people. You worry--does this harbinger a kidney disease But individuals can have this condition for a long, long time, and it doesn t seem to lead to kidney damage or their going on a dialysis machine or needing a kidney transplant.")
22
Glomerulopatías Enfermedades caracterizadas por daño estructural de los glomerulos. Cambios en la membraa basal causan proteinuria. La enfermedad puede ser aguda o crónica.

23
Causas de proteinuria glomerular
Dismiución de la carga negativa de la pared del capilar glomerular Aumento de tamaño del poro funcional en la membrana basal glomerular por cambios estructurales Aumento de la presión en el capilar glomerular forzando un mayor pasaje de proteinas a través de la pared capilar Causes of glomerular proteinuria What causes glomerular proteinuria then? You could surmise from what I have must said a decrease in that negative charge, which is observed in many causes of nephrotic syndrome. There is a loss of that negative charge in the capillary wall which allows protein to get to the wall. There is also an increase in that functional pore size. There is damage to that wall by different factors in different types of disease, which make bigger pores in the wall and allows the protein to spill through. Also, sometimes at the glomerular level, and maybe even in the whole body, there is an increase in blood pressure that can force more protein across the wall, which may be why certain antagonists of increased pressure, such as ACE inhibitors, can reduce the proteinuria in certain patients.

24
When the glomerular capillary fails to hold back protein What happens with proteinuria is, that instead of the molecules here, shown as the little golden spheres, remaining within the capillary lumens, they spill across the capillary wall into the urinary space and are lost from the body, resulting in a lower protein level, especially albumin level, within the plasma ...and all the consequences of the nephrotic syndrome that we will be considering today. There are structural changes that take place within the glomerulus when this happens in different diseases, and this is what we are going to focus on to identify the different types of disease that cause the nephrotic syndrome. One change you can see in this particular diagram, on the right, the normal capillary has the little foot processes intact.... excuse me, the left-hand side is the normal capillary. On the right-hand side some of those little foot processes have fused together. It is just a structural marker that proteinuria has taken place. You see foot process fusion in all patients who have proteinuria, so it is not specific for a particular cause.

25
Sindrome nefrótico Condición producida por importante proteinuria (>3-3,5 g/día) Hipoalbuminemia Edema( Retención Na, P oncotica) Hiperlipidemia ( Producción hepatica) Estado de hipercoagulabilidad HTA, Disminución del FG Nephrotic syndrome Now in dealing with general management of the nephrotic syndrome, we are dealing with a condition caused by heavy albuminuria, of course. You may or may not have hypoalbuminemia, edema, hyperlipidemia, and hypercoagulable state. But nephrologists are fond of talking about nephrotic range proteinuria because if you have 10 grams of albuminuria, whether you have these manifestations or not, you will eventually develop them. Moreover, the diseases that give you 10 grams of proteinuria are the same regardless of whether you have the manifestations. But we are going to focus on these manifestations now, the edema, the hyperlipidemia, the hypercoagulable state. What can you do in general for your patient with nephrotic syndrome?
 Estado de hipercoagulabilidad. HTA, Disminución del FG. Nephrotic syndrome Now in dealing with general management of the nephrotic syndrome, we are dealing with a condition caused by heavy albuminuria, of course. You may or may not have hypoalbuminemia, edema, hyperlipidemia, and hypercoagulable state. But nephrologists are fond of talking about nephrotic range proteinuria because if you have 10 grams of albuminuria, whether you have these manifestations or not, you will eventually develop them. Moreover, the diseases that give you 10 grams of proteinuria are the same regardless of whether you have the manifestations. But we are going to focus on these manifestations now, the edema, the hyperlipidemia, the hypercoagulable state. What can you do in general for your patient with nephrotic syndrome")
26
Sindrome nefrótico Diagnostico
CLÍNICA LABORATORIO ( sangre y orina) SEROLOGÍAS y COMPLEMENTO CAUSA DE SINDROME NEFROTICO BIOPSIA RENAL
 SEROLOGÍAS y COMPLEMENTO. CAUSA DE SINDROME NEFROTICO. BIOPSIA RENAL.")
27
Diagnóstico patológico del sindrome nefrótico
Biopsia renal es la única manera de hacer el diagnóstico de certeza de sme nefrótico a pesar de que algunos datos clínicos pueden sugerir un diagnóstico presuntivo (edad, antec, etc.) Bx renal : microscopía óptica, inmunofluorescencia, y microscopía electrónica.
 Bx renal : microscopía óptica, inmunofluorescencia, y microscopía electrónica.")
28
The pathologists tools: three types of microscopy The optimum evaluation of a renal biopsy is by three procedures that we will be looking at to see how you make the diagnosis: light microscopy, immunofluorescence microscopy, and electron microscopy. Light microscopy involves taking a thin section of a kidney biopsy, which is usually obtained by inserting a needle into the back, a hollow needle, and removing a tiny core of kidney tissue. It is fixed with a fixative and sliced very thinly and stained with textile dye basically. You get a pattern similar to what we see on the far left. Immunofluorescence microscopy allows the specific identification of, in particular, abnormal antibodies that can cause certain kinds of glomerular disease but don't cause others. So this immunofluorescence stains these abnormal antibodies. Electron microscopy allows you to look at a very high magnification that you can't see by standard microscopy. For example, on the far right--that is just one capillary loop. You can see on the far right just one capillary loop; on the left, you can see there are many loops there. So (the rightmost picture was taken at) much higher magnification.
 much higher magnification..")
29
Complicaciones del Sme Nefrótico
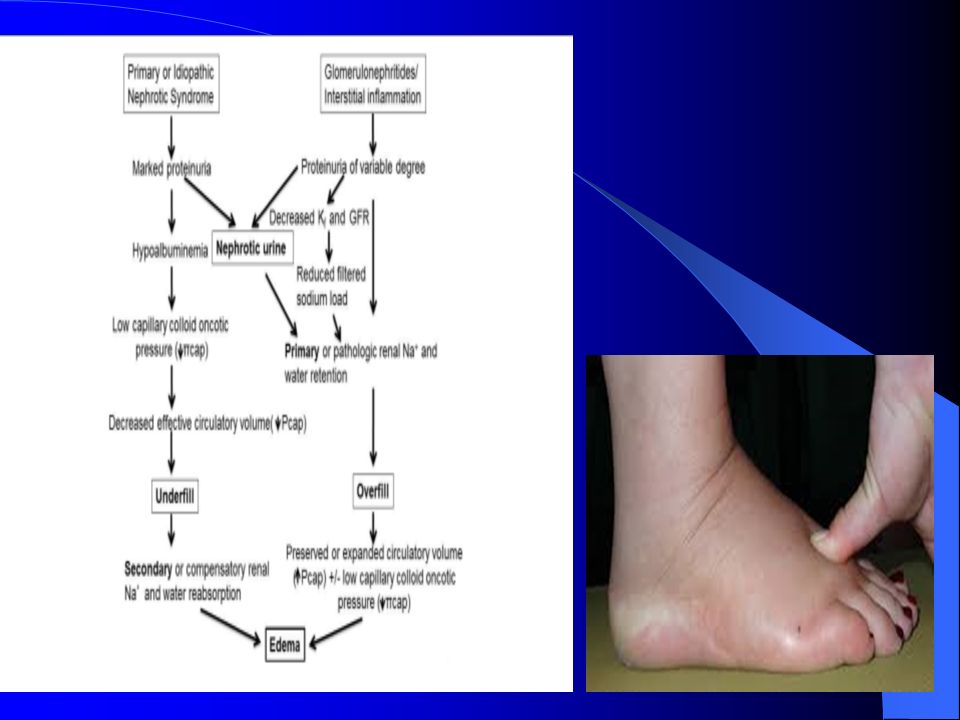
Proteinuria persistente: Promotor de progresión Dislipidemia: Aumento del colesterol, Lp(a), Tg Enf cardiovascular, promotor de progresión Complicaciones tromboembólicas- Hipercoagulabilidad Trombosis venosa TEP Trombosis arterial (raro) Edema (estado de avidez por el Na+) Persistent proteinuria If one had the opportunity to look at some of the literature or the textbooks written on the nephrotic syndrome, one probably wouldn't see the first complication. I have put it up there because I believe it is becoming increasingly important, and that is persistent proteinuria. Persistent proteinuria in many of our recent large clinical trials that have been ongoing within the United States has really been shown to be what we call an independent risk factor for progression of renal disease. That means independent of all the other things that we can look at and measure and check and watch. So we are becoming more and more concerned that proteinuria itself may have some significant implications to the kidney in terms of its ability to actually cause damage and injury and thus be what we call a progression promoter or promoter of progressive renal disease. Dyslipidemia The second group of complications that I would like to talk about is the area of dyslipidemia: Altered cholesterol levels, high cholesterol levels, changes in the amounts of fats and lipids in the body. A large part of this, as I will show you in a moment, is driven by changes in the glomerular filter and the leaking of protein into the urine. But they (changes in blood lipid levels) in themselves have significant implications. They have implications for cardiovascular disease, and there is now a growing body of scientific evidence to suggest that this may be an important and yet overlooked complication that we have in our adult population. There is also a fair amount of clinical data from prospective trials to look at lipids as a progression promoter for renal disease. So not only do the lipids appear to be potentially injurious to the coronary arteries, giving us heart disease, but they may also be injurious to the kidney. Thromboembolic complications The third big area that is important but less frequently seen, and which has been alluded to already, is the area of thromboembolic complications. The nephrotic syndrome has been variably described as a hypercoagulable state, and we will be discussing that in a little bit in a moment. There is a definite prevalence of peripheral thrombosis: Clots in the legs of people, in adults and certainly in children with nephrotic syndrome; and a complication which is quite serious, although it fortunately occurs rarely, called renal vein thrombosis. That means a clot in the renal vein that leads from the kidney. Although we have looked for it extensively, my own personal experience in a large number of patients is, that it is a relatively uncommon complication, although it has been reported in the literature in substantial numbers of patients. Why renal vein thrombosis is important is because of the second complication here, and that is, a clot to the lungs. In patients with peripheral venous thrombosis, and particularly with renal vein thrombosis, clots to the lung are a significant complication and certainly a life-threatening complication that we have to be cognizant of and look for under certain circumstances. Finally very, very rare and more frequent in the children than in the adults, is thrombosis of arteries within the body, usually in the smaller arteries. This is a complication that occurs more commonly in patients who are younger, and usually is found in people who have abnormalities of fluid and electrolyte balance, in patients who are dehydrated, in particular. Edema The fourth major complication that I have listed here and that we have talked about somewhat earlier today is the whole business of edema. Indeed, the nephrotic syndrome can be termed a sodium-avid state. That is why we restrict salt or give diuretics to such patients. They have a propensity to hold on to salt and therefore expand their total body water. That contributes to the development of edema in the legs, in the abdomen, around the eyes and elsewhere in patients with the nephrotic syndrome.
, Tg. Enf cardiovascular, promotor de progresión. Complicaciones tromboembólicas- Hipercoagulabilidad. Trombosis venosa. TEP. Trombosis arterial (raro) Edema (estado de avidez por el Na+) Persistent proteinuria If one had the opportunity to look at some of the literature or the textbooks written on the nephrotic syndrome, one probably wouldn t see the first complication. I have put it up there because I believe it is becoming increasingly important, and that is persistent proteinuria. Persistent proteinuria in many of our recent large clinical trials that have been ongoing within the United States has really been shown to be what we call an independent risk factor for progression of renal disease. That means independent of all the other things that we can look at and measure and check and watch. So we are becoming more and more concerned that proteinuria itself may have some significant implications to the kidney in terms of its ability to actually cause damage and injury and thus be what we call a progression promoter or promoter of progressive renal disease. Dyslipidemia The second group of complications that I would like to talk about is the area of dyslipidemia: Altered cholesterol levels, high cholesterol levels, changes in the amounts of fats and lipids in the body. A large part of this, as I will show you in a moment, is driven by changes in the glomerular filter and the leaking of protein into the urine. But they (changes in blood lipid levels) in themselves have significant implications. They have implications for cardiovascular disease, and there is now a growing body of scientific evidence to suggest that this may be an important and yet overlooked complication that we have in our adult population. There is also a fair amount of clinical data from prospective trials to look at lipids as a progression promoter for renal disease. So not only do the lipids appear to be potentially injurious to the coronary arteries, giving us heart disease, but they may also be injurious to the kidney. Thromboembolic complications The third big area that is important but less frequently seen, and which has been alluded to already, is the area of thromboembolic complications. The nephrotic syndrome has been variably described as a hypercoagulable state, and we will be discussing that in a little bit in a moment. There is a definite prevalence of peripheral thrombosis: Clots in the legs of people, in adults and certainly in children with nephrotic syndrome; and a complication which is quite serious, although it fortunately occurs rarely, called renal vein thrombosis. That means a clot in the renal vein that leads from the kidney. Although we have looked for it extensively, my own personal experience in a large number of patients is, that it is a relatively uncommon complication, although it has been reported in the literature in substantial numbers of patients. Why renal vein thrombosis is important is because of the second complication here, and that is, a clot to the lungs. In patients with peripheral venous thrombosis, and particularly with renal vein thrombosis, clots to the lung are a significant complication and certainly a life-threatening complication that we have to be cognizant of and look for under certain circumstances. Finally very, very rare and more frequent in the children than in the adults, is thrombosis of arteries within the body, usually in the smaller arteries. This is a complication that occurs more commonly in patients who are younger, and usually is found in people who have abnormalities of fluid and electrolyte balance, in patients who are dehydrated, in particular. Edema The fourth major complication that I have listed here and that we have talked about somewhat earlier today is the whole business of edema. Indeed, the nephrotic syndrome can be termed a sodium-avid state. That is why we restrict salt or give diuretics to such patients. They have a propensity to hold on to salt and therefore expand their total body water. That contributes to the development of edema in the legs, in the abdomen, around the eyes and elsewhere in patients with the nephrotic syndrome.")
30
Complicaciones del Sme Nefrótico
Disminución de las proteínas ligadoras Dism vit D y Ca, aum PTH osteodistrofia Dism capacidad de la Alb de ligar drogas Dism metales trazadores( Fe, Cu, Zn) Dism EPO Dism Transferrina Complicaciones infecciosas (desnutrición proteica) Peritonitis (organismos capsulados en niños) Neumonia Infecciones del tracto urinario (?) Insuficiencia renal aguda Anemia
 Dism EPO. Dism Transferrina. Complicaciones infecciosas (desnutrición proteica) Peritonitis (organismos capsulados en niños) Neumonia. Infecciones del tracto urinario ( ) Insuficiencia renal aguda. Anemia.")
31
Complicaciones del Sme Nefrótico: Resumen
Hipertesión, proteinuria persistente e hiperlipidemia asociada son promotores de la progresión de la enfermedad renal. El tratamiento que está dirigido a controlar la hipertensión, proteinuria e hiperlipidemia puede preservar la función renal

32
Sindrome nefrótico Tratamiento
1- Tratamiento especifico de la patología causante del sme nefrotico( inmunosupresores y esteroides) 2- Tratamiento sintomatico: Edema: diureticos ( furosemida) Hiperlipidemia: ( Estatinas, fibratos) Proteinuria, HTA: ( IECA, ARA) Hipercoagulabilidad: (AAS, Anticoagulantes?) Dieta baja en proteinas ( g/Kg/d)
 2- Tratamiento sintomatico: Edema: diureticos ( furosemida) Hiperlipidemia: ( Estatinas, fibratos) Proteinuria, HTA: ( IECA, ARA) Hipercoagulabilidad: (AAS, Anticoagulantes ) Dieta baja en proteinas ( g/Kg/d)")
33
Principales causas de proteinuria y sindrome nefrótico
Primarias: Glomerulopatia a cambios mínimos Esclerosis focal y segmentaria Glomerulopatía membranosa Glomerulonefritis membrano proliferativa Secundarias: Nefropatía diabética Amiloidosis renal Lupus eritematoso sistemico These are some of the major categories of glomerular disease that cause proteinuria and the nephrotic syndrome. There are many others. These are some of the most important. These are the ones I am going to focus on today, and maybe mention a few others. Other diseases can cause the nephrotic syndrome that have many effects on the body. For example, diabetes often can cause glomerular disease and the nephrotic syndrome, but that is not a category of disease we are going to be concerned with today. Minimal change glomerulopathy (glomerulopathy means glomerular disease) is also called just minimal- change disease; focal segmental glomerulosclerosis, which is often just abbreviated FSGS, and we will learn what that is. It means a certain kind of scarring, sclerosis, that affects glomeruli. Membranous glomerulopathy, also called membranous glomerulonephritis, which is the most common cause for nephrotic syndrome in adults; and something called membranoproliferative glomerulonephritis. These are fancy-sounding names, but I think you will be able to understand what the basis is for these designations as we go along.
 is also called just minimal- change disease; focal segmental glomerulosclerosis, which is often just abbreviated FSGS, and we will learn what that is. It means a certain kind of scarring, sclerosis, that affects glomeruli. Membranous glomerulopathy, also called membranous glomerulonephritis, which is the most common cause for nephrotic syndrome in adults; and something called membranoproliferative glomerulonephritis. These are fancy-sounding names, but I think you will be able to understand what the basis is for these designations as we go along.")
34
Causas de Sme nefrótico según edad
Causes of nephrotic syndrome change with age The frequency of these various categories of disease varies with age. You can see in young children, in red, minimal change glomerulopathy or minimal change disease is by far the most common cause for the nephrotic syndrome. As you move towards adulthood, more and more other categories of disease contribute to the nephrotic syndrome. In adults, especially in the fourth and fifth decades of life, membranous glomerulopathy is the most frequent cause. But you can see many other causes can also contribute. Focal segmental glomerulosclerosis accounts for 15 or 20 percent of patients at all ages. Membranoproliferative glomerulonephritis is very rare.

35
Causas de Sme nefrótico según edad
< 15 años Cambios minimos Eslerosis focal y segmentaria GN membranoproliferativa 15-40 años Esclerosis focal y segmentaria GN membranosa DBT, LES > 40 años GN membranosa DBT Cambios minimos, Amiloidosis

36
Glomerulopatia a Cambios Minimos
Causa mas frecuente de Sme nefrotico en chicos Linfocitos T liberarían citoquinas contra cel epitelial Creatinina: en gral normal M.O.: normal o leve proliferación mesangial M.E.: fusión de los pies de los podocitos Etiología: Idiopatica en general y puede ser secundaria: AINE, Leucemia, Linfoma, Litio. Comienzo brusco despues de un CVAS.

37
CAMBIOS MINIMOS Foot process effacement By electron microscopy, though, with minimal change glomerulopathy, as shown on the right, there is this foot process effacement, this fusing together of the foot processes, which we will see in all causes of nephrotic syndrome. The difference with minimal change glomerulopathy is that this is the only change. So it is a diagnosis by exclusion. We see this change but nothing else.

38
GLOMERULOPATIA A CAMBIOS MINIMOS
Minimal change glomerulopathy Minimal change glomerulopathy or minimal change disease is the first one we are going to consider. It is the most common cause for the nephrotic syndrome in children, one that is oft times very responsive to corticosteroid treatment. The light microscopy looks usually completely normal. There are minimal changes by light microscopy if any. You can't diagnose the disease (by light microscopy). Immunofluorescence microscopy (right panel) also is negative. There is no evidence for abnormal antibodies deposited. There are no changes here by light or immunofluorescence microscopy, which doesn't give you a diagnosis; but as we will see, it rules out the other diagnoses we are going to consider because they do have specific changes with these modes of examination. So even the negative data help you decide that this patient has minimal change glomerulopathy rather than one of the other diseases. Some patients have a mild variation on this where there is some increase in the mesangial cells, those cells in the middle of the glomerulus. That is called mesangial proliferation or mesangioproliferative glomerulonephritis. It can be very closely related and similar to minimal change with respect to the natural history and response to management, but it does have a slightly different prognosis.
. Immunofluorescence microscopy (right panel) also is negative. There is no evidence for abnormal antibodies deposited. There are no changes here by light or immunofluorescence microscopy, which doesn t give you a diagnosis; but as we will see, it rules out the other diagnoses we are going to consider because they do have specific changes with these modes of examination. So even the negative data help you decide that this patient has minimal change glomerulopathy rather than one of the other diseases. Some patients have a mild variation on this where there is some increase in the mesangial cells, those cells in the middle of the glomerulus. That is called mesangial proliferation or mesangioproliferative glomerulonephritis. It can be very closely related and similar to minimal change with respect to the natural history and response to management, but it does have a slightly different prognosis.")
39
CAMBIOS MINIMOS Tratamiento inicial de ataque Tratamiento de:
CARACTERISTICAS DEL TRATAMIENTO: Tratamiento inicial de ataque Tratamiento de: Recaídas frecuentes Esteroideo dependencia Esterioideo resistencia ( proteinuria nefrotica persistente >8-16 semanas)
")
40
CAMBIOS MINIMOS/Tratamiento
RECOMENDACIONES Dosis de ataque: prednisona 1mg/Kg/d por 8-16 sem y luego se baja la dosis en forma lenta Recaída: igual a dosis de ataque hasta la remisión. Recaídas frecuentes: Pensar en inmunosupresores como: ciclofosfamida, ciclosporina, Rituximab. Drug therapy for minimal change disease (MCD) in adults So what do we do? We recommend that for adults with this disorder of minimal change disease, prednisone, which is the corticosteroid, 60 mg/meter squared for six weeks and then 40 mg every second day for another six weeks, so a total of 12 weeks before we can say that in fact they have failed initial treatment.
 in adults So what do we do We recommend that for adults with this disorder of minimal change disease, prednisone, which is the corticosteroid, 60 mg/meter squared for six weeks and then 40 mg every second day for another six weeks, so a total of 12 weeks before we can say that in fact they have failed initial treatment.")
41
CAMBIOS MINIMOS/Tratamiento
RECOMENDACIONES: Esteroideo dependencia: ciclofosfamida, ciclofosforina, Rituximab ? Esteroideo resistencia: ciclofosfamida o ciclosporina

42
Esclerosis focal y segmentaria
Causa relativamente común de Sme Nefrotico M.O.:Areas de esclerosis, colapso mesangial, oclusión de capilares por depositos hialinos en algunos glomer (focal) y en parte del glomer (segmentaria). En IF no depositos inmunes. M.E.: fusión de los pies de los podocitos. Etiología: usualmente idiopatica. Puede ser secundaria a malignidad, HTA, Reflujo, GN, HIV.
 y en parte del glomer (segmentaria). En IF no depositos inmunes. M.E.: fusión de los pies de los podocitos. Etiología: usualmente idiopatica. Puede ser secundaria a malignidad, HTA, Reflujo, GN, HIV.")
43
Esclerosis focal y segmentaria
Historia natural (idiopatica): presentación Nefrótico: 70% niños 50% adultos Proteinuria asintomática 30-50% Hallazgos asociados HTA 25% niños Alt.FG % Microhematuria % Presentation and natural history of FSGS in adults So this condition has a completely different outlook than the minimal change disease, but in a great percentage of the time in children, it presents exactly in the same way, that is, with the nephrotic syndrome. In adults it is a little bit different. You see here the associated findings of hypertension, high blood pressure, found in 50 percent of adults, a lower GFR, that is a raised serum creatinine or a decreased creatinine clearance; some impairment of kidney function is also found in about a third of these patients; and microhematuria, which is pretty rare in minimal change disease, is found in as high as 60 percent of these patients. So you know even from the start, even though the biopsy might look pretty much the same, most of the glomeruli are going to look pretty normal. The clinical findings, the features that you see in the patient, are completely different for minimal change in many cases. And it also gives you an idea that these patients are not going to do as well as, in fact, the minimal change disease type.
: presentación. Nefrótico: 70% niños. 50% adultos. Proteinuria asintomática 30-50% Hallazgos asociados. HTA 25% niños. Alt.FG 20-40% Microhematuria 40-60% Presentation and natural history of FSGS in adults So this condition has a completely different outlook than the minimal change disease, but in a great percentage of the time in children, it presents exactly in the same way, that is, with the nephrotic syndrome. In adults it is a little bit different. You see here the associated findings of hypertension, high blood pressure, found in 50 percent of adults, a lower GFR, that is a raised serum creatinine or a decreased creatinine clearance; some impairment of kidney function is also found in about a third of these patients; and microhematuria, which is pretty rare in minimal change disease, is found in as high as 60 percent of these patients. So you know even from the start, even though the biopsy might look pretty much the same, most of the glomeruli are going to look pretty normal. The clinical findings, the features that you see in the patient, are completely different for minimal change in many cases. And it also gives you an idea that these patients are not going to do as well as, in fact, the minimal change disease type.")
44
Esclerosis Focal y Segmentaria
Prevalencia (idiopatica) 3-15% de todas las biopsias renales 7-12% de todos los pacientes con proteinuria Progresiva es el tipo más común en Niños Negros de cualquier edad Aumento de frecuencia en la última década Género : Niños : M:F 1:1 Adultos:M:F 2:1
 3-15% de todas las biopsias renales. 7-12% de todos los pacientes con proteinuria. Progresiva es el tipo más común en. Niños. Negros de cualquier edad. Aumento de frecuencia en la última década. Género : Niños : M:F 1:1. Adultos:M:F 2:1.")
45
Esclerosis Focal y Segmentaria Historia natural
Remisión espontánea % Fallo renal rápidamente progresivo 10-15% Fallo renal lentamente progresivo 40-60% Proteinuria persistente * * Pacientes subnefróticos = “mejor” pronóstico

46
Esclerosis Focal y Segmentaria predictores de pronostico
Buen pronóstico Remisión completa Respondedores a esteroides Mal pronóstico Fibrosis intersticial Alteración del FG Persistencia de importante proteinuria

47
Esclerosis Focal y Segmentaria
Focal segmental glomerulosclerosis (FSGS) Let's consider next focal segmental glomerulosclerosis, which is an important cause for the nephrotic syndrome in children because it is not quite as easy to treat as minimal change glomerulopathy and it also can be a cause for nephrotic syndrome in adults. "Focal" means that SOME glomeruli are involved and not others. So of those millions of glomeruli you've got, only some have this lesion. "Segmental" means that parts of the tuft of the glomerulus are involved and not others. So on the right-hand panel, the black area there is the injured area. "Sclerosis" means scarring. So what you have is focal, segmental scarring of these glomeruli. It begins as just a few spots of scar here and there in your glomeruli. But with time, often it can progress. More and more glomeruli are involved; more and more glomeruli are completely scarred; and of course, the ultimate result could be renal failure.
 Let s consider next focal segmental glomerulosclerosis, which is an important cause for the nephrotic syndrome in children because it is not quite as easy to treat as minimal change glomerulopathy and it also can be a cause for nephrotic syndrome in adults. Focal means that SOME glomeruli are involved and not others. So of those millions of glomeruli you ve got, only some have this lesion. Segmental means that parts of the tuft of the glomerulus are involved and not others. So on the right-hand panel, the black area there is the injured area. Sclerosis means scarring. So what you have is focal, segmental scarring of these glomeruli. It begins as just a few spots of scar here and there in your glomeruli. But with time, often it can progress. More and more glomeruli are involved; more and more glomeruli are completely scarred; and of course, the ultimate result could be renal failure.")
48
Esclerosis Focal y Segmentaria
FSGS: Light microscope examination of renal biopsy In this light micrograph, we can see relatively normal capillary loops on the right-hand side of this glomerulus, but this patient has extensive scarring on the left-hand side of that glomerular tuft and has focal segmental glomerulosclerosis.

49
Esclerosis Focal y Segmentaria/ Tratamiento
Es primordial establecer el diagnóstico Tratar las complicaciones ej: hiperlipidemia, HTA, etc Pacientes nefróticos: prednisona 1 a 2 mg/kg/día por 3-6 meses FSGS: Management plan So what is the management plan? First, you make sure that the renal disease primary, that is, that it is only affecting the kidney. Then you treat the comorbid conditions, which will be discussed subsequently. And for nephrotic patients, that is, those with high-grade proteinuria and the features of the nephrotic syndrome, we recommend prednisone treatment, 1 mg/kg for a minimum of three to six months of treatment. The evidence for this is not great. There has never been a randomized, controlled study in using steroids in this disorder, but there have been several large studies that indicate this complete remission rate. It is very hard to design a study when you have demonstrated a complete remission, where one of the alternatives would be no treatment at all.

50
Esclerosis Focal y Segmentaria/ Tratamiento
Si no hay respuesta: Ciclosporina 4-6 mg/kg por 6 meses o Ciclofosfamida mg/kg por 3 a 6 meses Pacientes subnefróticos con FG estable: Tratamiento con esteroides y observación FSGS: Management plan for failure of initial treatment As I mentioned, somewhere between 20 and 40 percent of patients will have a complete remission with steroid therapy. So what do we do with the other 60 percent? As I mentioned earlier, I think cyclosporin, if our study is borne out in other studies, would be the second line of therapy combined usually with low-dose prednisone. Cyclophosphamide has been tried in children, with reasonably good results, but it is hard to say how secure the evidence is in adults because it hasn't really been tried. So I put that grade of evidence for that down significantly. The other important point to remember is that there is that persistent proteinuria group, that is patients who have 1, 2, maybe even 3 grams/day of protein excretion and who are relatively symptom free, who may not even have any hypertension. It does appear that either they are in a partial remission or their disease is relatively mild and they don't need a lot of aggressive treatment. We now have followed those patients for up to 20 or 25 years without any deterioration in renal function. So I have put that as a separate category -- subnephrotic with stable renal function -- probably don't need anything more than observation.

51
GN Membranosa Causa mas común de Sme Nefrotico en el adulto
M.O.: Engrosamiento de la Membrana basal y spikes ( meteramia de plata) IF: Depositos de IgG y complemento M.E.:Depositos electrodensos en el espacio subepitelial Etiología: Usualmente idiopatica (Anti PLA2 + 75%) Secundaria: Malignidad, LES, Sales de Oro, AR, HB, HCV.
 IF: Depositos de IgG y complemento. M.E.:Depositos electrodensos en el espacio subepitelial. Etiología: Usualmente idiopatica (Anti PLA2 + 75%) Secundaria: Malignidad, LES, Sales de Oro, AR, HB, HCV.")
52
GN Membranosa HISTORIA NATURAL 5-10 % de todas las biopsias
10-20% de todos los ptes con proteinuria Raro en niños Se encuentran causas 2rias en 20-30% de los casos Riesgo de GNM asociado a Tumor maligno aumenta con la edad

53
GN Membranosa Presentación: Hallazgos asociados: Nefrótico 60-70%
Proteinuria asintomática % Hallazgos asociados: Insuficiencia renal 10% HTA % Microhematuria % Trombosis de la vena renal 5-30%

54
GN Membranosa Curso clínico: Remisión espontánea 20-30%
Proteinuria persistente % Fallo renal progresivo %

55
GN Membranosa Buenos: Malos: FACTORES PRONOSTICOS Remisión completa
Bajo grado de proteinuria (< 3.5 g/día) Sexo femenino Malos: Persistencia de alto grado de proteinuria Insuficiencia renal Biopsia renal con < 50 % de esclerosis insterticial HTA Sexo masculino
 Sexo femenino. Malos: Persistencia de alto grado de proteinuria. Insuficiencia renal. Biopsia renal con < 50 % de esclerosis insterticial. HTA. Sexo masculino.")
56
Glomerulonefritis Membranosa
Membranous glomerulopathy: schematic The reason it is thicker is that there are abnormal accumulations of antibody molecules in the zone between that epithelial cell and the basement membrane. There shouldn't be any antibody molecules out there. As you know, antibodies are molecules we normally use to fight off foreign invaders. They are molecules that can specifically attach to other molecules and attack them and eliminate them from our bodies, which is a beneficial process.

57
Glomerulonefritis Membranosa
In some diseases, called immune complex diseases, these antibodies, bound to antigen, get stuck in tissues. In tissues, they cause injury. They can attract white blood cells in some circumstances; or in others, they can just disturb function, as in this case. So there is this abnormal accumulation of these antibodies and antigen that we usually can't identify in the patient. We don't really know what these antibodies are directed against in most patients.

58
Glomerulonefritis Membranosa
Membranous glomerulopathy Let's consider now membranous glomerulopathy, the most common cause for the nephrotic syndrome in adults, but it does occur in children. Sometimes in children it is secondary to an infectious process, for example hepatitis B, or related to some systemic disease, like something called lupus erythematosus. Membranous glomerulopathy can occur at any age. It is most frequent in adults. Membranous glomerulopathy by light microscopy has a thickening of the capillary wall, sort of referred to as the membrane of the capillary, although it is not just the basement membrane that is thickened. As we will see, there are other changes. You can see on the right in a glomerulus from a patient with membranous glomerulopathy, the capillary walls are very thick compared to the normal glomerulus, on the left. This is somewhat paradoxical, you would think--well, the wall is thicker, you should have less protein getting across it. But, in fact, you have a lot more because there is abnormal permeability. Even though it is thicker, it is more permeable.

59
Glomerulonefritis Membranosa
By immunofluorescence microscopy, now we can see very bright staining that is indicating the location of these antibody molecules. The minimal change glomerulopathy was just black by immunofluorescence microscopy. Remember that in focal segmental glomerulosclerosis, in areas that weren't scarred there was no staining. But here we have massive accumulation of abnormal antibodies injuring the capillaries. So the cause, the pathogenesis, what generates the pathology, the lesions, in membranous glomerulopathy is some antibody attaching to an antigen and forming these aggregates in the wall of the glomerulus, leading to proteinuria and can eventually lead to progressive scarring of the glomeruli and renal failure in those patients who don't have remission, either spontaneously or in response to treatment.

60
Glomerulonefritis Membranosa

61
Glomerulonefritis Membranosa/ Tratamiento
Regimen de Ponticelli 6 meses de ciclos de clorambucil y prednisona La tasa de remisión parcial y completa es significativamente mejor en el grupo tratado; dos veces más de remisión parcial o completa a los 10 años. Probabilidad de sobrevida sin IRCT a los 10 años fue del 92% en el grupo tratado y 60% en el grupo control Kidney int 48: , 1995

62
GN Membranoproliferativa
Causa poco común de sindr Nefrotico Edad: 8 a 30 años M.O.: Egrosamiento de MB glomerular, proliferación mesangial e interposición de mesangio entre MBG y la cel endotelial. M.E.: tipo 1) depositos inmunes en mesangio y espacio subendotelial tipo 2) depositos inmunes sobre la MBG, MB tubular y MB capsula bowman.
 depositos inmunes en mesangio y espacio subendotelial. tipo 2) depositos inmunes sobre la MBG, MB tubular y MB capsula bowman.")
63
GN Membranoproliferativa
Cursa con hipocomplementemia en gral. Etiología: Idiopatica o asociada a otras patologias: LES, Hepatitis B, C, malignidad, abcesos vicerales, Crioglobulinemia, Edocarditis bacteriana, etc. Presentación clínica: 1- Sindrome Nefritico 30 % 2- Hematuria macroscopica recurrente 10-20% 3- Sindrome nefrotico 50% 4- Microhematuria o proteinuria leve.10-20%

64
GN Membranoproliferativa
By electron microscopy, here you can see these deposits, too, as the dark areas in the mesangial region, causing the mesangial cells to be stimulated and to proliferate, and also some of these deposits underneath the glomerular basement membrane near the circulation, where they can stimulate white blood cells to attack the kidney because it has a lot of these antibodies in it which normally stimulate white blood cells to attach something. Here it is an inappropriate attack on the kidney.

65
GN Membranoproliferativa
The pathogenesis, the genesis of the disease in membranoproliferative glomerulonephritis, again, is antibodies binding to antigen, but here localizing on the inside of the basement membrane and in the mesangium, causing membranoproliferative glomerulonephritis instead of localizing on the outside of the basement membrane just causing membranous glomerulopathy. Once again, we often don't know what the antigen is that is stimulating this disease, but sometimes we do. Once again, sometimes hepatitis B infection can elicit this (membranoproliferative GN), hepatitis C infection, some neoplasms, and some autoimmune diseases where you attack an antigen of your own body.
, hepatitis C infection, some neoplasms, and some autoimmune diseases where you attack an antigen of your own body.")
66
GN Membranoproliferativa
Membranoproliferative glomerulonephritis The last category of nephrotic syndrome I would like to mention is membranoproliferative glomerulonephritis, which is another immune complex glomerulonephritis. Here (right panel) by light microscopy, there also is a very obvious structural abnormality compared to normal (left panel). There is the thickening of the capillary wall, sort of the membranous component we just looked at with membranous glomerulopathy, but there is also hypercellularity, including mesangial proliferation. So it is sort of a combination, at least structurally, of the mesangial proliferative pattern I mentioned earlier, which is closer related, at least in natural history, to minimal change glomerulopathy, and the membranous, and the term for it then is membranoproliferative glomerulonephritis.
 by light microscopy, there also is a very obvious structural abnormality compared to normal (left panel). There is the thickening of the capillary wall, sort of the membranous component we just looked at with membranous glomerulopathy, but there is also hypercellularity, including mesangial proliferation. So it is sort of a combination, at least structurally, of the mesangial proliferative pattern I mentioned earlier, which is closer related, at least in natural history, to minimal change glomerulopathy, and the membranous, and the term for it then is membranoproliferative glomerulonephritis.")
67
GN Membranoproliferativa
In this disease, there is also localization of immune complexes, that is antibodies bound to antigen, in the capillary walls, also down in the mesangium. The deposits are stimulating this mesangial proliferation. They are also producing this capillary wall thickening, and there can be substantial injury to the glomerulus.

68
GN Membranoproliferativa
Tratamiento: 1- Tratar la enfermedad de base 2- Agentes antiplaquetarios ( posible rol de las plaq en la patogenia) 3- Una terapia optima para la GNMP idiopatica no existe. En algunos reportes hubo respuesta favorable a los esteroides.
 3- Una terapia optima para la GNMP idiopatica no existe. En algunos reportes hubo respuesta favorable a los esteroides.")
69
Causas secundarias de sindrome nefrotico
LES: Proliferativa focal (III), difusa (IV) y la Membranosa(V) son las causantes de sme nefrotico. AMILOIDOSIS: Mieloma Multiple, gamapatía monoclonal. Nefropatía Diabetica
, difusa (IV) y la Membranosa(V) son las causantes de sme nefrotico. AMILOIDOSIS: Mieloma Multiple, gamapatía monoclonal. Nefropatía Diabetica.")
70
MUCHAS GRACIAS!

Presentaciones similares



















>")
