Descargar la presentación
La descarga está en progreso. Por favor, espere

2
ALGUNOS HECHOS ALGUNAS PREGUNTAS
SIDA Y BIOÉTICA ALGUNOS HECHOS ALGUNAS PREGUNTAS IV ENCUENTRO GeSIDA. ALICANTE 2007 Pedro Montilla de Mora. Infectólogo

6
Una “intuición” que nunca es pura y estrictamente racional
Poseedor de un alma racional Ente de razón Creado a imagen de Dios Libre albedrio y potestad Autodeterminable Fin en si mismo Capaz de … Autodominable Autorreflexivo “DIGNIDAD” Capaz de vida emocional Capaz de sufrimiento Una “intuición” que nunca es pura y estrictamente racional

7
¿QUÉ ES LA DIGNIDAD HUMANA?
“En todo individuo hay algo incondicional que impone respeto” (R. Andorno) ¿QUÉ ES LA DIGNIDAD HUMANA? Polisémica y ambigua. Diferente para el médico que para el enfermo: “Morir dignamente”: - Morir conscientemente, con lucidez - Morir sin consciencia - Morir rodeado de las personas que uno ama - Evitar el encarnizamiento - Morir sin síntomas molestos, dolor… - Morir de acuerdo a las propias creencias NO ES FÁCIL DE DEFINIR
 ¿QUÉ ES LA DIGNIDAD HUMANA Polisémica y ambigua. Diferente para el médico que para el enfermo: Morir dignamente : - Morir conscientemente, con lucidez. - Morir sin consciencia. - Morir rodeado de las personas que uno ama. - Evitar el encarnizamiento. - Morir sin síntomas molestos, dolor… - Morir de acuerdo a las propias creencias. NO ES FÁCIL DE DEFINIR.")
8
¿QUÉ ES LA DIGNIDAD HUMANA?
NO ES FÁCIL DE DEFINIR PERO SI LO ES DISCERNIR QUE ALGUNAS COSAS SON INDIGNAS “Morir indignamente”: - Morir solo - Morir en un espacio anónimo e inhóspito - Morir sufriendo innecesariamente - Morir atado a un artefacto que se convierte en soberano de los últimos días - Morir rodeado de personas insensibles - Morir sin poder decidir cómo La eslavitud, la instrumentalización, la tortura, la vulneración de la intimidad, la cosificación, la crueldad, la guerra, el hambre, la humillación…

9
“La medicina perdió la inocencia en Auschwitz…”
“La investigacion desarrollada en los campos de concentración Nazi no aportó nada relevante al conocimiento …. los métodos utilizados eran muy defectuosos…” Mellanby, “Human Guinea Pigs” 1973 ¿SE TRATA DE UN PROBLEMA DE MÉTODOS O DE PRINCIPIOS?

10
EL ESTUDIO TUKESGEE: Tuskegee syphilis study which took place from 1932 until 1972 in Alabama (in the South of the USA). In this study, 400 rural black men were left untreated when diagnosed with syphilis – despite the fact that a penicillin cure became available ‘by the early 1950s’ – so that the natural course of the disease could be observed ¿ESTAMOS “A SALVO” LAS SOCIEDADES OCCIDENTALES “MODERNAS”?
. In this study, 400 rural black. men were left untreated when diagnosed with syphilis – despite. the fact that a penicillin cure became available ‘by the early. 1950s’ – so that the natural course of the disease could be. observed. ¿ESTAMOS A SALVO LAS SOCIEDADES OCCIDENTALES MODERNAS")
11
MÍNIMOS COMUNMENTE ACEPTADOS
LOS SERES HUMANOS SOMOS PERSONAS, NO COSAS LOS SERES HUMANOS NO PUEDEN SER CONSIDERADOS COMO MEDIOS. SON FINES EN SI MISMOS COMO PERSONAS TIENEN DIGNIDAD, NO PRECIO TODOS LOS SERES HUMANOS MERECEN IGUAL CONSIDERACIÓN Y RESPETO… - EN LA VIDA BIOLÓGICA: NO MALEFICENCIA - EN LA VIDA SOCIAL: JUSTICIA PERO HAY MÁS: ¿QUIÉN PUEDE DEFINIR EL IDEAL DE VIDA DE UN PACIENTE? ¿CÚALES SON LOS VALORES QUE DEBEN PRIMAR?

12
¿ETICA / BIOÉTICA / ÉTICA MÉDICA?
COMITÉS DE ÉTICA DE ENSAYOS CLÍNICOS… COMITÉS DE ÉTICA DE LA INVESTIGACIÓN… COMITÉS DE ÉTICA CLÍNICA… ÉTICA EN LA PRÁCTICA ASISTENCIAL… LA GENTE DEPOSITA CONFIANZA EN LOS MÉDICOS…

13
¿QUÉ SE ESPERA DEL MÉDICO?
“La practica medica combina ciencia y arte. El papel de la ciencia es claro….el médico… en el cuidar del que sufre necesita pericia, conocimiento científico, y comprensión humana… …el tacto, la simpatía y la comprensión son (actitudes) esperadas en el médico, el paciente no debe verse como una colección de síntomas, signos, malfunciones, órganos dañados, y emociones alteradas. .. … para el médico, como para el antropólogo, nada humano es extraño o repulsivo. El misántropo puede ser un elegante diagnosticador, pero no puede esperar llegar a tener éxito como médico. El médico de verdad tiene una Shakesperiana amplitud de intereses tanto por el prudente como por el loco, por el orgulloso y el humilde, por el héroe estoico y por el pícaro llorón. Toma a su cuidado personas” Capítulo Primero.”Harrison´s Principles of Internal Medicine”. 1ª Ed. (1958) y siguientes
 esperadas en. el médico, el paciente no debe verse como una colección de síntomas, signos, malfunciones, órganos dañados, y emociones alteradas. .. … para el médico, como para el antropólogo, nada humano es extraño. o repulsivo. El misántropo puede ser un elegante diagnosticador, pero. no puede esperar llegar a tener éxito como médico. El médico de verdad. tiene una Shakesperiana amplitud de intereses tanto por el prudente. como por el loco, por el orgulloso y el humilde, por el héroe estoico y. por el pícaro llorón. Toma a su cuidado personas Capítulo Primero. Harrison´s Principles of Internal Medicine . 1ª Ed. (1958) y siguientes.")
14
“Los médicos con frecuencia se enfrentan en la práctica clínica
con problemas éticos que les dejan perplejos, consumen su tiempo y les dejan emocionalmente exhaustos. La experiencia, el sentido común o ser simplemente “una buena persona” no garantizan que sean capaces de resolverlos….” Capítulo Segundo.”Harrison´s Principles of Internal Medicine”.

15
“POR LO GENERAL LOS PROBLEMAS NO HAY QUE BUSCARLOS,
YA QUE CADA PROFESIÓN SE LOS ENCUENTRA POR EL CAMINO…” Prof. D. Gracia. 1991 Aparecer…, aparecen. ¿Les prestamos atención? “Son problemas de otros…¿de quiénes…? ¿Renunciamos a planteárnoslos por miedo a no encontrar solución?

16
TOMA DE DECISIONES EN SITUACIONES
DE INCERTIDUMBRE ¿OJO CLÍNICO? ¿OLFATO ÉTICO? DECISIONES TÉCNICAS: ¿INDICADA LA P. LUMBAR? DECISIONES ÉTICAS: ¿HAGO CASO AL PACIENTE QUE NO QUIERE RECIBIR TODO O PARTE DEL TRATAMIENTO?

17
TOMAR DECISIONES EN CONDICIONES DE INCERTIDUMBRE
ES LO QUE HACEMOS TODOS LOS DÍAS EN CLÍNICA… …NO DEBEN SER DECISIONES SIN UNA BASE DE CONOCIMIENTO …NO PUEDEN SER DECISIONES IRRACIONALES ¿DECISIONES ÉTICAS (MORALES)? NO ES SOLO UN PROBLEMA DE PROCEDIMIENTOS NO PUEDEN ABORDARSE SIN PROCEDIMIENTOS
 NO ES SOLO UN PROBLEMA DE PROCEDIMIENTOS. NO PUEDEN ABORDARSE SIN PROCEDIMIENTOS.")
18
DECISIONES Y PROBLEMAS ÉTICOS
“La ética como una cuestión burocrática que retrasa el inicio de ensayos clínicos muy interesantes…” “Todo eso del consentimiento informado…¡menos mal que ya no hace falta!” Revised Recommendations for HIV Testing of Adults, Adolescents, and Pregnant Women in Health-Care Settings. MMWR, 2006 “No es un problema de ética, la ley debería obligar a las embarazadas con VIH a tomar antirretrovirales aún contra su voluntad…¡Es la vida de su hijo la que está en juego…!” ¿Hasta donde puedo / debo llegar… … informo … convenzo … persuado … coacciono

19
DECISIONES Y PROBLEMAS ÉTICOS
“Mi paciente, recientemente diagnosticado de infección VIH … … no quiere / no sabe como planteárselo a su pareja” “Si mi paciente toma el tratamiento … - No enferma - No transmite la infección - No selecciona variantes resistentes - No transmite variantes resistentes… …pero me consta que no toma bien el tratamiento” “Además tiene una tuberculosis… - la ley de medidas especiales en materia de salud pública me permitiría ingresarlo contra su voluntad hasta que deje de ser un riesgo para los demás…” ¿es decir…?

20
DECISIONES Y PROBLEMAS ÉTICOS
“He conseguido que tome un régimen de antirretrovirales que evitará que el VIH lo mate, pero… …la coinfección por HCV le pone en riesgo de cirrosis, hepatocarcinoma - ¿un momento excelente para hacer ciencia…? - ¿un enorme desafío para él y para mi forma de cuidarlo?” “Mi paciente me hace entender que ya no cree que vaya a morir, pero… ¿quién le va a querer así…?” “Todo esto es tan difícil…¡hagamos ensayos clínicos, estudios de cohortes… lo que sea, necesitamos saber más para poder ayudar…!”

21
DECISIONES Y PROBLEMAS ÉTICOS
A pesar de todo muchos enfermos van mal… - “ART COHORT” (13 cohortes EEUU y UE) pacientes ( pt-año) Lancet, 2002 1.094 pt/año desarrollan Sida - De ellos 344 pt/año mueren Factores asociados a mortal: Inicio targa con < 50 cd4: - 5,5 veces más que si > 350 Edad avanzada Advp como via de adquisición 50 % EN LOS GRUPOS CON MÁS FACT. DE RIESGO …cuidados paliativos… ¿qué es morir dignamente?
 pacientes ( pt-año) Lancet, pt/año desarrollan Sida. - De ellos 344 pt/año mueren. Factores asociados a mortal: Inicio targa con < 50 cd4: - 5,5 veces más que si > 350. Edad avanzada. Advp como via de adquisición. 50 % EN LOS GRUPOS CON MÁS FACT. DE RIESGO. …cuidados paliativos… ¿qué es morir dignamente")
22
DECISIONES Y PROBLEMAS ÉTICOS. RESPUESTAS
ÉTICA MÉDICA CLÁSICA ÉTICAS BASADAS EN EL “CÓDIGO ÚNICO”. LA VERDAD REVELADA Y LAS METAFÍSICAS DE LA “LEY NATURAL”. - CUANDO SE PLANTEAN EXCEPCIONES A LA NORMA SE APLICAN CRITERIOS DE RACIONALIDAD O FILOSÓFICOS: MATAR EN LEGÍTIMA DEFENSA…

23
ÉTICA MÉDICA CLÁSICA EN MEDICINA ENCAJA EN EL ENFOQUE PATERNALISTA – DESPÓTICO: - LA OPINIÓN DEL PACIENTE NO IMPORTA - SI LA OPINIÓN DEL PACIENTE SE AJUSTA AL CÓDIGO, SE CONSIDERA CORRECTA. ES INNECESARIO TENERLA EN CUENTA - SI LA OPINIÓN DEL PACIENTE NO SE AJUSTA AL CÓDIGO DEBE CONSIDERARSE ERRONEA. SERÍA PERJUDICIAL TENERLA EN CUENTA

24
BIOÉTICA “MODERNA” AÑOS 70
ABUSOS EN LA INVESTIGACIÓN. DESDE EL TRIBUNAL DE NÜREMBERG LOS PACIENTES QUIEREN PARTICIPAR EN LAS DECISIONES QUE LES AFECTAN Informe Belmont Declaración de Helsinki Bioética consecuencialista Bioética principialista (Childress y Beauchamp) Casuística Etica de la virtud “Ethical work-up”…
 Casuística. Etica de la virtud. Ethical work-up …")
25
PRINCIPIOS: “NO – MALEFICENCIA”
“PRIMUM NON NOCERE”: Su formulación original decía “curar, o al menos no hacer daño” Me impide hacer daño a otro incluso cuando él me lo pide FORMULACIÓN “POSITIVA”: TRATAR LA VIDA BIOLÓGICA DE TODOS LOS HOMBRES CON IGUAL CONSIDERACIÓN Y RESPETO No es el reverso de la beneficencia Obliga aún en contra de la voluntad Permite la limitación de la libertad cuando su ejercicio causa daño a otros SE CONSIDERA “BÁSICO” Y “UNIVERSAL” (la beneficencia sería “particular”)
")
26
PRINCIPIOS: JUSTICIA (O NO – INJUSTICIA)
PROHIBE LAS DISCRIMINACIONES INJUSTIFICADAS U OFENSIVAS MANDA QUE LAS CARGAS Y LOS BENEFICIOS SE DISTRIBUYAN DE FORMA EQUITATIVA: - ¿Más al que más aporta…? - ¿Más al que más necesita…? RAWLS (“Teoría de la Justicia”) Las diferencias en la distribución de honores y riquezas sólo son justificables si redundan en beneficio de todos, o de los menos favorecidos SE REFIERE A LA VIDA SOCIAL Obliga aún en contra de la voluntad “BÁSICO” Y “UNIVERSAL”
 Las diferencias en la distribución de honores y riquezas sólo son justificables si redundan en beneficio de todos, o de los menos favorecidos. SE REFIERE A LA VIDA SOCIAL. Obliga aún en contra de la voluntad. BÁSICO Y UNIVERSAL")
27
PRINCIPIOS: AUTONOMÍA
LAS PERSONAS TIENEN DERECHO A DECIDIR SOBRE SU PROPIO DESTINO EXIGE A LA SOCIEDAD PROTECCIÓN ESPECIAL PARA CON LAS PERSONAS CUYA AUTONOMÍA ESTÁ COOMPROMETIDA (NIÑOS, ENCARCELADOS, DISCAPACITADOS…) Se refiere a: - La capacidad de autolegislación de la razón humana - La capacidad de tomar decisiones con conocimiento y sin coacción: - La persona autónoma - La elección autónoma
 Se refiere a: - La capacidad de autolegislación de la razón humana. - La capacidad de tomar decisiones con conocimiento y sin coacción: - La persona autónoma. - La elección autónoma.")
28
PRINCIPIOS: BENEFICENCIA
EXIGE QUE FAVOREZCAMOS LOS INTERESES Y EL BIENESTAR DE LAS PERSONAS “MAXIMIZAR BENEFICIOS”: ESTOS “BENEFICIOS” DEPENDEN DEL SISTEMA DE VALORES DE CADA INDIVÍDUO: No se puede “hacer el bién” a otra persona contra su voluntad, aunque si estamos obligados a no “hacerle mal” No es lo mismo “matar” que “dejar morir”

29
PRINCIPIOS: JERARQUIZACIÓN
PRIMER ORDEN (DE MÍNIMOS): Obligan a todos: - No hacer daño - Justicia SEGUNDO ORDEN: Sólo obligan a algunos / algunas profesiones - Autonomía - Beneficencia ¡¡ PUEDEN ENTRAR EN CONFLICTO !!
: Obligan a todos: - No hacer daño. - Justicia. SEGUNDO ORDEN: Sólo obligan a algunos / algunas profesiones. - Autonomía. - Beneficencia. ¡¡ PUEDEN ENTRAR EN CONFLICTO !!")
30
PRINCIPIOS: CONFLICTOS Y TRANSGRESIONES
SÓLO EN SITUACIONES CONCRETAS Y EN CONTEXTOS DETERMINADOS IDENTIFICAR LOS POSIBLES CURSOS DE ACCIÓN ANALIZAR LOS EVENTUALES CHOQUES ENTRE PRINCIPIOS EN CADA CURSO ANALIZAR LAS CONSECUENCIAS DE CADA CURSO Y, DE NUEVO SU REPERCUSIÓN SOBRE LOS PRINCIPIOS LA “CARGA DE LA PRUEBA” RECAE SOBRE EL QUE PROPONE LA TRANSGRESIÓN. DEBE SER EXPLÍCITA

31
PRINCIPIOS: CONFLICTOS Y TRANSGRESIONES
MEDIDAS QUE VIOLAN ALGÚN PRINCIPIO: “REGLAS”, LA MEDIDA PROPUESTA DEBE PRETENDER UN FIN LEGÍTIMO Y… …SER EFICAZ …SER PROPORCIONADA …SER LA ÚNICA ALTERNATIVA VIABLE …MINIMA POSIBLE …OTRAS CONDICIONES: - Garantizar soporte y acceso a los servicios - Disponer servicios de calidad - Minimizar daños secundarios…

32
LA RELACIÓN SANITARIO – PACIENTE. PROBLEMAS
RIESGO INDIVIDUAL CUIDAR CURAR PREVENIR ¿ COMO ? LA ENFERMEDAD DEL PACIENTE (biologica) EN LA VIDA DEL PACIENTE (biográfica) ¿ QUE ? SI RIESGO COMUNIDAD
 EN LA VIDA DEL PACIENTE (biográfica) ¿ QUE SI. RIESGO COMUNIDAD.")
33
LA “RAZÓN DE SALUD PÚBLICA”
SÓLO RIESGO INDIVIDUAL * EDUCACIÓN SANIT. "MÍNIMA" * "DEJAR HACER" RIESGO PARA LA SALUD PÚBLICA * INGRESOS FORZOSOS ( ).- TUBERCULOSIS "Homeless" "Sin amigos" Dependientes "Disipados" Viciosos Ignorantes H. Biggs. Riverside Hospital * MARY MALLON (“TYPHOYD MARY”) * NO TRATAR.- ¿ VIH?
.- TUBERCULOSIS. Homeless Sin amigos Dependientes Disipados Viciosos Ignorantes. H. Biggs. Riverside Hospital. * MARY MALLON ( TYPHOYD MARY ) * NO TRATAR.- ¿ VIH")
34
LA “RAZÓN DE SALUD PÚBLICA”
¿ HAART SOLO PARA PACIENTES SELECCIONADOS? LA ADHERENCIA NO ES UN FENÓMENO DE "TODO O NADA" DESCONOCEMOS "CUÁNTA" ADH. ES NECESARIA EN HAART LOS FACTORES PREDICTORES DE NO-ADHERENCIA ENCONTRADOS EN GRUPOS POBLACIONALES HABLAN DE "RIESGO DE NO-ADHERENCIA” ¡¡ NO SON APLICABLES A TODAS LAS PERSONAS EN QUE SE DAN !! - El 40% de los inyectores de drogas en trat. por TB completaron el Tto sin siquiera TDS (Pablos Mendez et al. Am. J. Med 1997) LA NO-ADHERENCIA OCURRE EN TODAS CLASES SOCIALES, RAZAS O NIVELES EDUCATIVOS
 LA NO-ADHERENCIA OCURRE EN TODAS CLASES SOCIALES, RAZAS O NIVELES EDUCATIVOS.")
35
ETICA Y ADHERENCIA CUMPLIMIENTO:
Completa el tratamiento. Se "pliega" a las instrucciones Sanitario sabe / paciente dócil Beneficente - paternalista ADHERENCIA: El paciente coopera en su trat. Opina y finalmente decide Se aceptan las dificultades Autonomista

36
EFICACIA BIOETICA ADHERENCIA EFECTIVIDAD ETICA Y ADHERENCIA
Análisis de “principios” Análisis de consecuencias Procedimientos: - Evaluación dificultades - Facilitacion - Negociación y pacto ADHERENCIA EFECTIVIDAD

37
0,95 % DE 174.246 ARTÍCULOS PUBLICADOS HASTA EL 10 NOV / 2007
CON HIV O AIDS EN EL TÍTULO O EL ABSTRACT 0,95 % DE ELLOS > 1000 EN LOS PRIMEROS 12 AÑOS

38
EN GENERAL LA BIOÉTICA SE HA OCUPADO POCO DE LAS
ENFERMEDADES INFECCIOSAS: SUS PRINCIPALES TEMAS DE INTERÉS HAN SIDO: - EL PRINCIPIO Y EL FINAL DE LA VIDA - LOS DERIVADOS DE LOS AVANCES BIOTECNOLÓGICOS Selgelid, Bioethics 2005 EL SIDA, INICIALMENTE, FUE UNA EXCEPCIÓN: - TEST OBLIGATORIOS - SCREENING EN DONACIONES, POBLACIONES… - CONFIDENCIALIDAD - AUTONOMÍA - SUICIDIO Y SUICIDIO ASISTIDO - TRANSMISIÓN EVITABLE Y NO EVITADA… ¡¡ GRUPOS AFECTADOS CON “VOZ” Y PODER !!

39
“WHO reported about 57 million
deaths in 2002, of which almost 11 million had an infectious cause. HIV/AIDS accounted for 2·78 million deaths (4·9% of all deaths), second only to respiratory infections as an infectious cause of mortality. As a fraction of all deaths, 4·9% might not look particularly striking, but HIV/AIDS was the leading worldwide cause of mortality among people aged 15–59 years —ie, the most productive years of life.” Lancet 2004 GASTOS EN INVESTIGACIÓN MEDICA EN EL MUNDO: MILLONES DE DOLARES - 90 % PARA EL 10% RICO - 10 % PARA EL 90% POBRE ENFERMEDADES INFECCIOSAS. MORTALIDAD: - 58 % EN EL 20% MAS POBRE DE LA POBLACIÓN - 7 % EN EL 20% MAS RICO
, second only to respiratory. infections as an infectious cause of mortality. As a. fraction of all deaths, 4·9% might not look particularly. striking, but HIV/AIDS was the leading worldwide. cause of mortality among people aged 15–59 years —ie, the most productive years of life. Lancet GASTOS EN INVESTIGACIÓN MEDICA EN EL MUNDO: MILLONES DE DOLARES % PARA EL 10% RICO % PARA EL 90% POBRE. ENFERMEDADES INFECCIOSAS. MORTALIDAD: - 58 % EN EL 20% MAS POBRE DE LA POBLACIÓN. - 7 % EN EL 20% MAS RICO.")
40
EN LOS PAISES RICOS “EL SIDA VA BIÉN”…(?)
¿Y ENTRE LOS POBRES DE LOS PAISES RICOS? ¿Y EN LOS PAISES POBRES? “Relation betwen socioeconomic deprivation and Death from first myocardial infarction in Scotchland: Population based analysis” K. Macintyre et al BMJ. 2001 “The NHS Plan: promises that fail the most vulnerable” Editorial The Lancet. 2000

41
MUNDO, 126 PAISES Predictores de mortalidad

42
UNION EUROPEA Predictores de mortalidad “Conclusions: Income inequality seems to have an influence worldwide, especially for younger adults. Social inequality seems to have a universal negative impact on health. Humans are social animals and are not well constructed physiologically to survive in uncooperative surroundings—particularly during the prime of life.”

43
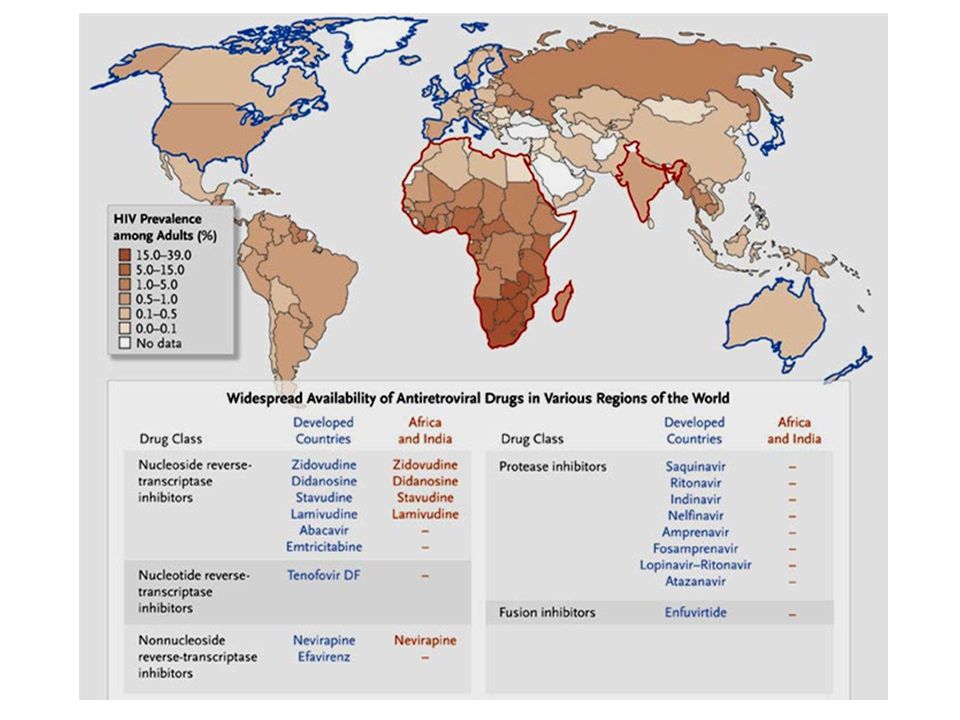
INEQUIDAD Y SIDA. AFRICA

44
A mayor porcentaje de población pobre (<1$/d) mayor prevalencia de VIH
A mayor desigualdad entre ricos y pobres mucha mayor prevalencia

47
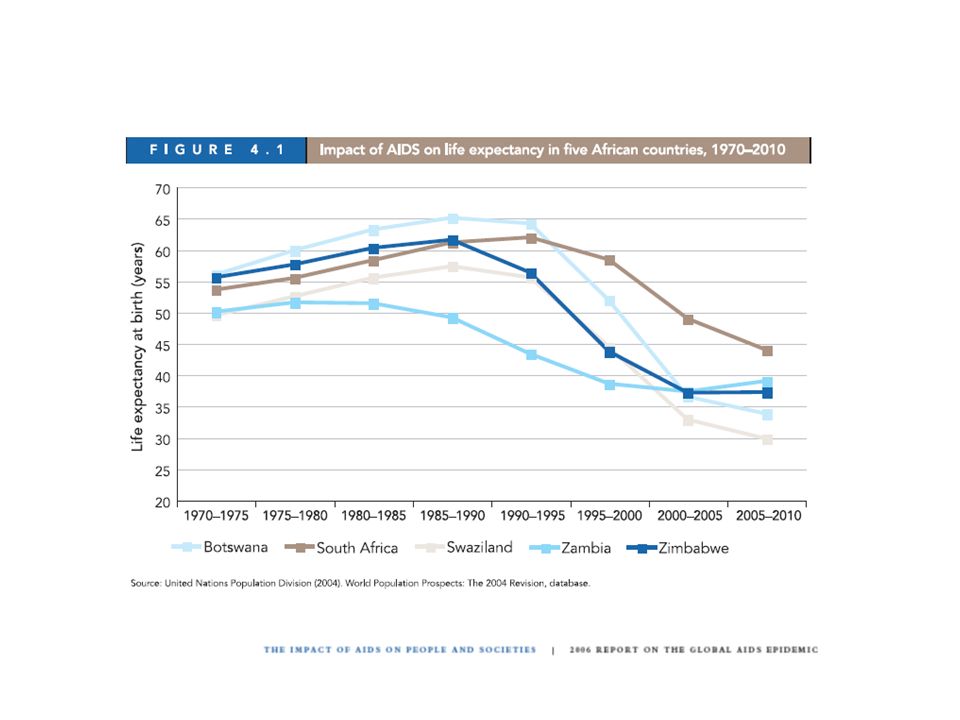
PNAS, 2007 A PESAR DE TODO, AFRICA SOBREVIVIRÁ UNA VEZ MÁS

48
Since 2002 the price of antiretroviral therapy has fallen by 50%. Indeed, in December last year the Clinton Foundation negotiated the price down to US$140 per person per year, This sum is still more than most people in the worst affected countries can afford, but the falling price does mean that donors are now prepared to fund mass treatment campaigns.

49
En los paises más afectados el presupuesto estatal
en gastos sanitarios es de 10 $ por persona y año “Another ray of hope is the growing realisation among leaders of the high-income nations that HIV/AIDS is a global security issue…”

50
WHO – UNAIDS. 2007: Africa subsahariana
25 millones infectados en Africa Reciben antirretrovirales 1,3 millones Cada año mueren 2 millones Cada año se infectan 3 millones Retención en los programas de tratamiento: - 50 % a los 2 años - 25 % muertos el los 2 años (inicio tardio) - 25 % perdidos PloS Medicine Metaánalisis Acceso a antirretrovirales en embarazadas: - 11% media - 16% algunas regiones de Namibia Acceso a antirretrovirales en niños: - 15% de los que los necesitan
 - 25 % perdidos. PloS Medicine Metaánalisis. Acceso a antirretrovirales en embarazadas: - 11% media. - 16% algunas regiones de Namibia. Acceso a antirretrovirales en niños: - 15% de los que los necesitan.")
51
POBREZA ENFERMEDAD ¿EL HUEVO O LA GALLINA? ATRAPAMIENTO
Michael Mermot. University College of London “A PERRO FLACO...”

52
POBREZA, INEQUIDAD... UN PROBLEMA PROPIO DE NUESTRO
OFICIO… ¿O ALGO QUE NOS TOCA “DE REFILÓN”? DETERMINANTES DE SUSCEPTIBILIDAD INDIVIDUAL DETERMINANTES DE VULNERABILIDAD SOCIAL HUESPED MICROORG. FÁRMACOS DAVIS DETERMINANTES MOLECULARES DE RESISTENCIA - LA BÚSQUEDA DEL “SANTO GRIAL” EN SALUD PÚBLICA - HARVEY V. FINEBERG. HARVARD SCHOOL OF PUBLIC HEALTH NEJM. 1996

53
DESIGUALDADES E INEQUIDADES
DESIGUALDAD EN SALUD ¿DECISION LIBRE INDIVIDUO? NO SI DESIGUALDAD ACEPTABLE INEVITABLE DESIG. INEVITABLE EVITABLES E INJUSTAS INEQUIDADES

54
BIOETICA. INVESTIGACIÓN
AZT “Unethical Trials of Interventions to Reduce Perinatal Transmission of the Human Immunodeficiency Virus in Developing Countries” Lurie, NEJM. Sept, 18, 1997 WMA: Declaración de Helsinki (versión Oct/2000): Clause 19 “Medical research is only justified if there is a reasonable likelihood that the populations in which the research is carried out stand to benefit from the results of the research.” Clause 30 “At the conclusion of the study, every patient entered into the study should be assured of access to the best proven prophylactic, diagnostic and therapeutic methods identified by the study”.
: Clause 19. Medical research is only justified if there is a reasonable likelihood. that the populations in which the research is carried out. stand to benefit from the results of the research. Clause 30. At the conclusion of the study, every patient entered into the. study should be assured of access to the best proven prophylactic, diagnostic and therapeutic methods identified by the. study .")
55
IVERMECTINA: EFICAZ EN LAS INFESTACIONES POR HELMINTOS EN ANIMALES EFICAZ EN HUMANOS LOS GOBIERNOS DE LOS PAISES POBRES NO PUEDEN PAGARLOS LA EMPRESA FABRICANTE LOS PROPORCIONA GRATUITAMENTE ¿AZT…?

57
PRIORIDADES EN SIDA. PAISES POBRES:
EVALUACIONES DE COSTE – EFECTIVIDAD - USO DE CONDONES - TRATAMIENTO DE LAS ETS - EN PROSTITUTAS - EN MUJERES DE ALTO RIESGO - SCREENING DE SANGRE Y HEMODERIVADOS - REGÍMENES ULTRACORTOS PARA MTCT - TRATAMIENTO DE LA TUBERCULOSIS N/A 3-30 - COTRIMOXAZOL EN VIH + TB N/A 6 - ARTs EN ADULTOS $/CASO PREV $/DALY The Lancet 2002

58
“Now comes the potential problem. In some instances, the
JAMA, August 23/30, 2006—Vol 296, No. 8 “Now comes the potential problem. In some instances, the marketing goal of a company dominates the scientific aspect of the company-funded research.” “For-profit companies…can exert inappropriate influence in research via control of study data and statistical analysis, ghostwriting, managing all or most aspects of manuscript preparation, and dictating to investigators the journals to which they should submit their manuscripts.”

59
EL VIH COMO USURPADOR DE LA MAQUINARIA
METABÓLICA Y GENÉTICA CELULAR (J. Mann) ¿PODRÍA DECIRSE QUE LA INDUSTRIA FARMACÉUTICA HA USURPADO LA MAQUINARIA INVESTIGADORA DE LA COMUNIDAD MÉDICA…?
 ¿PODRÍA DECIRSE QUE LA INDUSTRIA FARMACÉUTICA. HA USURPADO LA MAQUINARIA INVESTIGADORA DE LA. COMUNIDAD MÉDICA…")
60
¿“COBAYAS HUMANOS” O SUJETOS DE EXPERIMENTACIÓN
CON TODAS LAS GARANTIAS?. USA TODAY: 16 de Mayo de 2005 “…giant drug outfits are outsourcing increasing numbers of drug trials outside the United States and Europe. Merck is now conducting 50 percent of its trials outside the United States. By 2006, 70 percent of Wyeth Pharmaceuticals trials are expected to occur offshore. Across Latin America, Eastern Europe, Asia and Africa, the sick are abundant, desperate and doc-trusting, and so recruitment into clinical trials is rapid. As one executive from an outfit specializing in running drug trials in Asia put it, patients in developing countries are "more willing to be guinea pigs."

61
¿NOS ENFRENTAMOS A “ELEGANTES” PROBLEMAS DE BASE
FILOSÓFICA Y ESPECULATIVA? ¿NO SE TRATA, CON FRECUENCIA, DE PROBLEMAS DE JUSTICIA? ¿SERÁN CAPACES DE HACERSE OIR LOS QUE ESTÁN ALEJADOS DE LOS MEDIOS DE COMUNICACIÓN Y DEL PODER? ¿TENEMOS CONOCIMIENTOS SUFICIENTES PARA ABORDAR LOS PROBLEMAS ÉTICOS DEL DÍA A DÍA?

62
EN MEMORIA DE VICTOR ROCA
me consta que sus enfermos todavía lloran su pérdida

63
“malnutrition and extreme poverty are
the root causes of the African AIDS…” THABO MBEKI (2000) Although poverty is neither necessary nor sufficient for an individual to contract HIV infection or AIDS, it may be necessary for an epidemic on the scale currently witnessed by parts of sub-Saharan Africa. The factors that underpin poverty in less-developed countries chronic national dept, unfair trade, corruption in the North and South, the cost of arms purchases, and the consequences of chronic conflict. Colin Butler National Centre for Epidemiology and Population Health, Australian National University THE LANCET • Vol 356 • October 21, 2000
 Although poverty is neither. necessary nor sufficient for an. individual to contract HIV infection or. AIDS, it may be necessary for an. epidemic on the scale currently. witnessed by parts of sub-Saharan. Africa. The factors that underpin poverty in. less-developed countries. chronic national. dept, unfair trade, corruption in the. North and South, the cost of arms. purchases, and the consequences of. chronic conflict. Colin Butler. National Centre for Epidemiology and. Population Health, Australian National. University. THE LANCET • Vol 356 • October 21,")
64
ZAMBIA: LOS HOGARES ENCABEZADOS POR MUJERES QUE CUIDAN A ALGUIEN CON SIDA - SOPORTAN ADEMÁS EL PESO DE 3,6 HUERFANOS DE MEDIA - DISPONEN DE MENOS ALIMIENTOS QUE LOS IMPRESCINDIBLES DURANTE 3,4 MESES CADA AÑO ¡¡ Y NO DISPONEN DE TIEMPO NI DE RECURSOS PARA DEDICARLOS A LA AGRICULTURA NI LA “LEVANTAR LA VOZ” !!

65
In Botswana, where free antiretroviral
therapy, infant formula and safe drinking water are widely available, stigma was given as the reason why over half of the pregnant women in a study did not feed their babies with Formula (unaids, 2006)
")
66
Women in sub-Saharan Africa are infected
more often and earlier in their lives than men. Young women aged 15–24 are between two and six times as likely to be HIV-positive than men of a similar age.

67
Botswana lost approximately
17% of its health-care workforce due to AIDS between 1999 and In Zambia, an estimated 40% of midwives in Lusaka are believed to be HIV-positive delivering antiretroviral therapy to everyone needing it would take the full-time services of almost half the existing health workforce

68
In India, the epidemic could have a
severe impact on the poorest citizens’ access to health care. Health insurance, both public and private, currently covers only 15% of the population, and the public health facilities available to the poor are underfunded and understaffed.

69
At the same time, the total number of
public school teachers is declining; between 1998 and 2003, the net reduction was over 5%. HIV prevalence among South African teachers is 21% among those aged 25–34 and 13% among those aged 35–44.

71
Algunos de mis enfermos:
cuando dejaron de preguntarse “¿quién me va a querer a mí?...” tienen que preguntarse… “¿quién me va a querer así?” (Scarlet Johansson, en “El hombre que susurraba a los caballos”) ¿Por qué nos sorprende que se dejen caer?
 ¿Por qué nos sorprende que se dejen caer")
Presentaciones similares