Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Casos clínicos Profilaxis en pacientes médicos

2
CHEST 2012; 141(2)(Suppl):e195S–e226S
(Suppl):e195S–e226S")
4
2013 International Society on Thrombosis and Haemostasis

5
“The American College of Chest Physicians (ACCP) had distinguished itself in previous decades as a producer of excellent “antithrombotic” guidelines used worldwide; guidelines that dealt simply and primarily with evidence and not opinion. Sadly in the last decade methodologists have hijacked the role of the ACCP panellists, their analyses and writing. This is revealed in a letter sent to the journal recently which discusses the reliability of clinical trial data . This subject is at the heart of the changes to the ACCP 2012 recommendations which shares a number of authors with this letter .” 2013 International Society on Thrombosis and Haemostasis

6
The antithrombotic therapy data has been downgraded by an unproven methodology allowing for three main changes: firstly dangerous extrapolations, (AAS en profilaxis ortopédica) secondly the consideration of so called “patient preferences” and the “feeling thermometer” “ETV manifiestamente clínica ( o clínicamente sintomática) como ETV importante para el paciente” and thirdly the potential for bias ( se autocitan, basándose en sus trabajos que no han demostrado su validez) 2013 International Society on Thrombosis and Haemostasis
 secondly the consideration of so called patient preferences and the feeling thermometer ETV manifiestamente clínica ( o clínicamente sintomática) como ETV importante para el paciente and thirdly the potential for bias ( se autocitan, basándose en sus trabajos que no han demostrado su validez) 2013 International Society on Thrombosis and Haemostasis.")
7
The use of neologisms, unscientific terminology and opaque language has made the guidelines impenetrable. There is an apparent intellectual bias in the writing which manifests itself in many ways. One example is giving clinically-presenting VTE the sobriquet ‘patient important VTE’(2). “ETV manifiestamente clínica ( o clínicamente sintomática) como ETV importante para el paciente” The use of neologisms, unscientific terminology and opaque language has made the guidelines impenetrable. There is an apparent intellectual bias in the writing which manifests itself in many ways. One example is giving clinically-presenting VTE the sobriquet ( apodo) ‘patient important VTE’(2). 2013 International Society on Thrombosis and Haemostasis
. ETV manifiestamente clínica ( o clínicamente sintomática) como ETV importante para el paciente The use of neologisms, unscientific terminology and opaque language has made the guidelines. impenetrable. There is an apparent intellectual bias in the writing which manifests itself in many. ways. One example is giving clinically-presenting VTE the sobriquet ( apodo) ‘patient important VTE’(2) International Society on Thrombosis and Haemostasis.")
8
“The main significant finding of ACCP 9 (2012) is that when compared to ACCP 8 (2008) there is a highly significant relative risk reduction (180 versus 29) in 1A recommendations (a reduction greater than 80%) despite almost no change in data. Now that, based on their methodology, is the really shocking finding! The tragedy is that as a result of those changes many patients may receive less effective therapies and more likely to be exposed to life-threatening VTE” 2013 International Society on Thrombosis and Haemostasis

9
Peculiaridades de la metodología: mis comentarios
Termómetro de sentimientos: validado? Quién lo puntúa? Preferencias del paciente en cuanto al tratamiento trombótico: obtenido del escenario de FA ¿Es igual que el de la ETEV? Preferencia del paciente en cuanto al tipo de profilaxis farmacológica ? Por qué desestiman determinados resultados positivos de buena calidad? Sangrado con HBPM vs HNF Por qué en cambio, extrapolan del escenario quirúrgico?- CNI Puntuación de los outcomes: ¿es igual una ETEV sintomática que una hemorragia mayor?. Le dan 1:1 y al ETEV sintomática vs hemorragia intracraneal 1: 2,5. No es infravalorar la HIC?. Por otro lado no toda ETEV sintomática es igual ni debería tener el mismo peso ( TVP poplítea vs TEP masivo???) Little is known about the distribution of patients’ values and preferences in the context of VTE prevention in nonsurgical settings. In developing the recommendations for this guideline, panelists made estimates of patients’ values and preferences often using indirect data from other settings (eg, values and preferences that pertain to anticoagulation in atrial fi brillation). In our populations, the weights (relative importance) given to the harmful effects (disutilities) of the most representative types of critical organ bleeding, namely GI or, less commonly, intracranial bleeding, will greatly impact the tradeoff between desirable and undesirable consequences of antithrombotic therapy. There are limited data to guide us with respect to the relative impact of VTE events vs bleeding events on patient-perceived state of health; available evidence suggests values and preferences for treatments and for health states vary appreciably between individuals. 4 In a values rating exercise, Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines panelists used a “feeling thermometer” with anchors at 0 (representing death) and 100 (representing full health) to rate patient scenarios for various clinical outcomes in terms of the value placed on a year in which the events depicted in the scenario occurred. 3 Median ratings were similar for the outcomes of symptomatic DVT, PE, and catheter thrombosis (80, 75, and 80, respectively) and severe GI bleeding (75), whereas the median rating for intracranial bleeding (stroke scenario) was 40. Therefore, we used 1:1 ratio of symptomatic VTE to major extracranial bleeding and 2.5:1 ratio of symptomatic VTE to intracranial bleeding for tradeoffs. We considered that preventative and screening recommendations require higher-quality evidence supporting benefi t than therapy recommendations. This decision is a value-based judgment. In making our recommendations, when there is uncertain benefi t and an appreciable probability of important harm or patient burden associated with treatment, we recommend against such treatments.
 Little is known about the distribution of patients’ values and. preferences in the context of VTE prevention in nonsurgical settings. In developing the recommendations for this guideline, panelists. made estimates of patients’ values and preferences often. using indirect data from other settings (eg, values and preferences. that pertain to anticoagulation in atrial fi brillation). In our populations, the weights (relative importance) given to. the harmful effects (disutilities) of the most representative types of. critical organ bleeding, namely GI or, less commonly, intracranial. bleeding, will greatly impact the tradeoff between desirable and. undesirable consequences of antithrombotic therapy. There are. limited data to guide us with respect to the relative impact of VTE. events vs bleeding events on patient-perceived state of health; available evidence suggests values and preferences for treatments. and for health states vary appreciably between individuals. 4. In a values rating exercise, Antithrombotic Therapy and Prevention. of Thrombosis, 9th ed: American College of Chest Physicians. Evidence-Based Clinical Practice Guidelines panelists used. a feeling thermometer with anchors at 0 (representing death) and 100 (representing full health) to rate patient scenarios for various. clinical outcomes in terms of the value placed on a year in. which the events depicted in the scenario occurred. 3 Median ratings. were similar for the outcomes of symptomatic DVT, PE, and. catheter thrombosis (80, 75, and 80, respectively) and severe GI. bleeding (75), whereas the median rating for intracranial bleeding. (stroke scenario) was 40. Therefore, we used 1:1 ratio of symptomatic. VTE to major extracranial bleeding and 2.5:1 ratio of. symptomatic VTE to intracranial bleeding for tradeoffs. We considered that preventative and screening recommendations. require higher-quality evidence supporting benefi t than. therapy recommendations. This decision is a value-based judgment. In making our recommendations, when there is uncertain. benefi t and an appreciable probability of important harm or. patient burden associated with treatment, we recommend against. such treatments.")
10
Una gordita de viaje.....

11
Una gordita de viaje..... Mujer de 32 años, con IMC 34 kg/m2, fumadora de 10 cig día,en tratamiento con anticonceptivos orales y una estatina por hipercolesterolemia. Consulta sobre la conveniencia de realizar alguna medida preventiva porque tiene previsto realizar un vuelo de 8 horas de duración.

12
¿Cuál es el riesgo de la paciente de desarrollar una ETEV?
Bajo Medio Alto Muy alto

13
Ultimas guías ACCP Symptomatic VTE is rare in passengers returning from long flights. Travelers at increased risk of VTE, defined as: previous VTE, thrombophilic disorders, severe obesity recent major surgery o trauma, active malignancy, pregnancy, estrogen use advanced age, limited mobility, who are traveling on flights > 6 h, CHEST 2012; 141(2)(Suppl):e195S–e226S
(Suppl):e195S–e226S.")
14
Qué la recomendaría? Nada
Que cogiera un asiento de pasillo y caminara, que hiciera ejercicios de flexoextensión del pie, bebiera mucho agua, no bebiera alcohol. Que se pusiera unas medias de compresión ligera hasta la rodilla HBPM a dosis profiláctica La daría a elegir lo que ella prefiriera porque eso es lo que dicen las guías. AAS Combinaría medidas físicas con farmacológicas

15
Ultimas guías ACCP For long-distance travelers at increased risk of VTE (including previous VTE, recent surgery or trauma, active malignancy, pregnancy, estrogen use, advanced age, limited mobility, severe obesity, or known thrombophilic disorder), we suggest: frequent ambulation, calf muscle exercise, or sitting in an aisle seat if feasible (Grade 2C) . use of properly fitted, below-knee GCS providing 15 to 30 mm Hg of pressure at the ankle during travel (Grade 2C) . For all other long-distance travelers, we suggest against the use of GCS (Grade 2C) . CHEST 2012; 141(2)(Suppl):e195S–e226S
, we suggest: frequent ambulation, calf muscle exercise, or sitting in an aisle seat if feasible (Grade 2C) . use of properly fitted, below-knee GCS providing 15 to 30 mm Hg of pressure at the ankle during travel (Grade 2C) . For all other long-distance travelers, we suggest against the use of GCS (Grade 2C) . CHEST 2012; 141(2)(Suppl):e195S–e226S.")
16
Ultimas guías ACCP Until further, methodologically appropriate studies are available, decisions regarding pharmacologic thromboprophylaxis for travelers who are considered to be at particularly high risk for VTE must be made on an individual basis, considering that adverse effects may outweigh any benefit. CHEST 2012; 141(2)(Suppl):e195S–e226S
(Suppl):e195S–e226S.")
17
De cuáles de estas medidas hay evidencia de su asociación a reducción de riesgo?
Asiento de pasillo Caminar Ejercicios de flexoextensión del pie, Beber mucha agua, No beber alcohol. Medias Todas Ninguna Solo medias

18
Epidemiologia Prolonged air travel results in a very small absolute incidence of VTE. RR of 2.8 (95% CI, ). Incidence of a symptomatic VTE in the month following a flight > 4 h is 1 in 4,600 flights, with a reported incidence of asymptomatic VTE on arrival from a trip ranging from 0% to 1.5%. For those on flights > 4 h, immobility during the flight and window seating (especially for obese persons) also increase the risk of VTE. Especially tall or short passengers may have an increased risk. There is no definitive evidence that dehydration, travel in economy class, and drinking alcoholi drinking alcoholic beverages on the flight are related to VTE risk. CHEST 2012; 141(2)(Suppl):e195S–e226S
 also increase the risk of VTE. Especially tall or short passengers may have an increased risk. There is no definitive evidence that dehydration, travel in economy class, and drinking alcoholi drinking alcoholic beverages on the flight are related to VTE risk. CHEST 2012; 141(2)(Suppl):e195S–e226S.")
20
Considera que el estar tomando una estatina modifica su riesgo trombótico?
No Ni idea Depende de qué estatina.

21
Ultimas guías ACCP CHEST 2012; 141(2)(Suppl):e195S–e226S
Statins reduce coagulation potential by decreasing tissue factor expression and decreasing thrombin generation, 161 leading to consideration of statin use to prevent VTE. Statin use has been related to risk of VTE in three prospective cohort studies, six casecontrol studies, and one clinical trial (Tables S31, S32). Considering DVT and PE together, the pooled risk estimate with statin use vs nonuse from several case-control studies was 0.61 (95% CI, ). Two observational studies based on administrative data 166,167 reported no signifi cant difference in the adjusted OR of VTE comparing statin users and nonusers. In contrast, another observational study 168 reported a lower risk of DVT with statin use, with an RR of 0.78 (95% CI, ). The Heart and Estrogen/ Progestin Replacement (HERS) clinical trial 169 of women with coronary artery disease also reported a lower risk of VTE with statin use (not randomized) in women (HR, 0.45; 95% CI, ). A single RCT comparing statin to placebo reported a lower risk of VTE with the statin. 170 The Justifi cation for the Use of Statins in Primary Prevention: an Intervention Trial Using Rosuvastatin (JUPITER) was designed to assess the effi cacy of rosuvastatin in preventing arterial vascular events in those not otherwise eligible for statins based on existing guidelines. Thus, it included a large sample of healthy people with low-density lipoprotein cholesterol , 130 mg/dL and C-reactive protein . 2 mg/L, without diabete The panel considered that it was premature to issue a recommendation concerning the use of statins to prevent VTE in light of the paucity of data and the availability of more established effective treatments. In addition, the patients included in this trial were not at increased risk of thrombosis and are not the patients for whom thromboprophylaxis would be recommended. This area is in need of further research. Trials that enroll patients at high risk of VTE (eg, those with previous VTE) who require thromboprophylaxis are needed. Such trials should have a comparative effectiveness design to better inform guideline developers; to that extent, these trials should have an active treatment of comparison, focus on symptomatic events that matter the most to patients, and report cost effectiveness analyses. The absolute rates of VTE were 2 per 1,000 in statin users compared with 4 per 1,000 in nonusers. The number needed to treat to prevent one DVT was 500 ( Table 22 , Table S33). PLoS Med. 2012;9(9):e doi: /journal.pmed Epub 2012 Sep 18. Effect of statins on venous thromboembolic events: a meta-analysis of published and unpublished evidence from randomised controlled trials. Rahimi K, Bhala N, Kamphuisen P, Emberson J, Biere-Rafi S, Krane V, Robertson M, Wikstrand J, McMurray J. Source George Centre for Healthcare Innovation, University of Oxford, Oxford, United Kingdom. Abstract BACKGROUND: It has been suggested that statins substantially reduce the risk of venous thromboembolic events. We sought to test this hypothesis by performing a meta-analysis of both published and unpublished results from randomised trials of statins. METHODS AND FINDINGS: We searched MEDLINE, EMBASE, and Cochrane CENTRAL up to March 2012 for randomised controlled trials comparing statin with no statin, or comparing high dose versus standard dose statin, with 100 or more randomised participants and at least 6 months' follow-up. Investigators were contacted for unpublished information about venous thromboembolic events during follow-up. Twenty-two trials of statin versus control (105,759 participants) and seven trials of an intensive versus a standard dose statin regimen (40,594 participants) were included. In trials of statin versus control, allocation to statin therapy did not significantly reduce the risk of venous thromboembolic events (465 [0.9%] statin versus 521 [1.0%] control, odds ratio [OR] = 0.89, 95% CI , p = 0.08) with no evidence of heterogeneity between effects on deep vein thrombosis (266 versus 311, OR 0.85, 95% CI ) and effects on pulmonary embolism (205 versus 222, OR 0.92, 95% CI ). Exclusion of the trial result that provided the motivation for our meta-analysis (JUPITER) had little impact on the findings for venous thromboembolic events (431 [0.9%] versus 461 [1.0%], OR = 0.93 [95% CI ], p = 0.32 among the other 21 trials). There was no evidence that higher dose statin therapy reduced the risk of venous thromboembolic events compared with standard dose statin therapy (198 [1.0%] versus 202 [1.0%], OR = 0.98, 95% CI , p = 0.87). Risk of bias overall was small but a certain degree of effect underestimation due to random error cannot be ruled out. Please see later in the article for the Editors' Summary. CONCLUSIONS: The findings from this meta-analysis do not support the previous suggestion of a large protective effect of statins (or higher dose statins) on venous thromboembolic events. However, a more moderate reduction in risk up to about one-fifth cannot be ruled out. CHEST 2012; 141(2)(Suppl):e195S–e226S
. Considering DVT and PE together, the pooled. risk estimate with statin use vs nonuse from several. case-control studies was 0.61 (95% CI, ). Two observational studies based on administrative. data 166,167 reported no signifi cant difference in the. adjusted OR of VTE comparing statin users and. nonusers. In contrast, another observational study 168. reported a lower risk of DVT with statin use, with an. RR of 0.78 (95% CI, ). The Heart and Estrogen/ Progestin Replacement (HERS) clinical trial 169. of women with coronary artery disease also reported. a lower risk of VTE with statin use (not randomized) in women (HR, 0.45; 95% CI, ). A single RCT comparing statin to placebo reported. a lower risk of VTE with the statin. 170 The Justifi cation. for the Use of Statins in Primary Prevention: an. Intervention Trial Using Rosuvastatin (JUPITER) was designed to assess the effi cacy of rosuvastatin in. preventing arterial vascular events in those not otherwise. eligible for statins based on existing guidelines. Thus, it included a large sample of healthy people. with low-density lipoprotein cholesterol , 130 mg/dL. and C-reactive protein . 2 mg/L, without diabete. The panel considered that it was premature to. issue a recommendation concerning the use of statins. to prevent VTE in light of the paucity of data and. the availability of more established effective treatments. In addition, the patients included in this trial. were not at increased risk of thrombosis and are not. the patients for whom thromboprophylaxis would be. recommended. This area is in need of further research. Trials that. enroll patients at high risk of VTE (eg, those with. previous VTE) who require thromboprophylaxis are. needed. Such trials should have a comparative effectiveness. design to better inform guideline developers; to that extent, these trials should have an active treatment. of comparison, focus on symptomatic events. that matter the most to patients, and report cost effectiveness. analyses. The absolute rates of VTE were 2 per 1,000. in statin users compared with 4 per 1,000 in nonusers. The number needed to treat to prevent one DVT. was 500 ( Table 22 , Table S33). PLoS Med. 2012;9(9):e doi: /journal.pmed Epub 2012 Sep 18. Effect of statins on venous thromboembolic events: a meta-analysis of published and unpublished evidence from randomised controlled trials. Rahimi K, Bhala N, Kamphuisen P, Emberson J, Biere-Rafi S, Krane V, Robertson M, Wikstrand J, McMurray J. Source. George Centre for Healthcare Innovation, University of Oxford, Oxford, United Kingdom. Abstract. BACKGROUND: It has been suggested that statins substantially reduce the risk of venous thromboembolic events. We sought to test this hypothesis by performing a meta-analysis of both published and unpublished results from randomised trials of statins. METHODS AND FINDINGS: We searched MEDLINE, EMBASE, and Cochrane CENTRAL up to March 2012 for randomised controlled trials comparing statin with no statin, or comparing high dose versus standard dose statin, with 100 or more randomised participants and at least 6 months follow-up. Investigators were contacted for unpublished information about venous thromboembolic events during follow-up. Twenty-two trials of statin versus control (105,759 participants) and seven trials of an intensive versus a standard dose statin regimen (40,594 participants) were included. In trials of statin versus control, allocation to statin therapy did not significantly reduce the risk of venous thromboembolic events (465 [0.9%] statin versus 521 [1.0%] control, odds ratio [OR] = 0.89, 95% CI , p = 0.08) with no evidence of heterogeneity between effects on deep vein thrombosis (266 versus 311, OR 0.85, 95% CI ) and effects on pulmonary embolism (205 versus 222, OR 0.92, 95% CI ). Exclusion of the trial result that provided the motivation for our meta-analysis (JUPITER) had little impact on the findings for venous thromboembolic events (431 [0.9%] versus 461 [1.0%], OR = 0.93 [95% CI ], p = 0.32 among the other 21 trials). There was no evidence that higher dose statin therapy reduced the risk of venous thromboembolic events compared with standard dose statin therapy (198 [1.0%] versus 202 [1.0%], OR = 0.98, 95% CI , p = 0.87). Risk of bias overall was small but a certain degree of effect underestimation due to random error cannot be ruled out. Please see later in the article for the Editors Summary. CONCLUSIONS: The findings from this meta-analysis do not support the previous suggestion of a large protective effect of statins (or higher dose statins) on venous thromboembolic events. However, a more moderate reduction in risk up to about one-fifth cannot be ruled out. CHEST 2012; 141(2)(Suppl):e195S–e226S.")
22
September 18, 2012

23
Si el viaje en lugar de en avión fuera en un autobús, cambiaria de actitud?
No Depende del tipo de autobus No lo tengo muy claro

24
Most individuals with travel-associated VTE have one or more known risk factors for thrombosis, including previous VTE, recent surgery or trauma, active malignancy, pregnancy, estrogen use, advanced age, limited mobility, severe obesity, or a thrombophilic disorder. Among healthy volunteers, coagulation activation observed after an 8-h fl ight was greater in carriers of factor V Leiden and in women taking oral contraceptives. Case-control studies have reported an increased risk of VTE in travelers who have thrombophilia and use oral contraceptives. Brands of below-knee GCS (providing mm Hg compression at the ankle) reduced the rate of asymptomatic DVT detected by screening from 3.6% to 0.2% (RR, 0.10; 95% CI, ); In a small study of high-dose enoxaparin (1 mg/kg), administered once 2 to 4 h before travel lasting 7 to 8 h, vs aspirin, one dose daily for 3 days starting 12 h before the beginning of the fl ight, vs control, there were zero of 82, three of 84, and four of 83 asymptomatic DVT in the three groups, respectively, but no symptomatic DVT or PE events in any group, although follow-up ended after the subjects left the airport. Cesarone. Angiologia de 2002.
 reduced the rate of asymptomatic DVT detected by screening from 3.6% to 0.2% (RR, 0.10; 95% CI, ); In a small study of high-dose enoxaparin (1 mg/kg), administered once 2 to 4 h before travel lasting 7 to 8 h, vs aspirin, one dose daily for 3 days starting 12 h before the beginning of the fl ight, vs control, there were zero of 82, three of 84, and four of 83 asymptomatic DVT in the three groups, respectively, but no symptomatic DVT or PE events in any group, although follow-up ended after the subjects left the airport. Cesarone. Angiologia de")
25
Varón EPOC, hepatópata que ingresa por infección respiratoria

26
Varón EPOC, hepatópata que ingresa por infección respiratoria
79 años O2 domiciliario. Solo se desplaza al servicio (Nivel de inmovilización 2) Obesidad Sangrado por varices esofágicas dos meses antes Hb 12 gd/dl. Plaquetas , INR 1,5 FGE 58 ml/m Ingreso por infección respiratoria con insuficiencia respiratoria global.
 Obesidad. Sangrado por varices esofágicas dos meses antes. Hb 12 gd/dl. Plaquetas , INR 1,5. FGE 58 ml/m. Ingreso por infección respiratoria con insuficiencia respiratoria global.")
27
¿cuál es mayor su riesgo trombótico o hemorrágico?
El hemorrágico El trombótico Similares

28
Padua Prediction Score.
A Patients with local or distant metastases and/or in whom chemotherapy or radiotherapy had been performed in the previous 6 mo. B Anticipated bed rest with bathroom privileges (either because of patient’s limitations or on physician’s order) for at least 3 d. C Carriage of defects of antithrombin, protein C or S, factor V Leiden, G20210A prothrombin mutation, antiphospholipid syndrome. To estimate baseline risk for patients with low and high VTE risk, we used data from risk assessment models (RAMs). Several RAMs have been proposed for use in hospitalized medical patients (Table S3). 5-7 Limitations of most RAMs include lack of prospective validation, applicability only to high-risk subgroups, inadequate follow-up time, and excessive complexity. In a prospective observational study of 1,180 inpatients, a predefi ned RAM (Padua Prediction Score, modifi ed after Kucher 8 ) assigned points to 11 common VTE risk factors ( Table 2 ) 9 and categorized hospitalized medical patients as low risk ( , 4 points; 60.3% of patients) or high risk ( 4 points; 39.7% of patients) for VTE. Attending physicians were not notifi ed of their patients’ risk categories. Patients were followed for symptomatic VTE for 90 days. VTE occurred in 11.0% of high-risk patients who did not receive prophylaxis vs 0.3% of low-risk patients, a . 30-fold difference in risk (hazard ratio [HR], 32.0; 95% CI, ). Among 711 low-risk patients, two (0.3%) developed VTE (1 PE, 1 PE with DVT). Among 283 high-risk patients who did not receive prophylaxis, the risk of DVT was 6.7%, nonfatal PE 3.9%, and fatal PE 0.4%. Hence, for baseline risk for low- and high-risk strata, we used risk estimates provided by the Padua Prediction Score. 9 Despite the limitations of this risk model (small number of events, suboptimal We considered a number of options for baseline risk of major bleeding. We considered bleeding events reported in the Padua prediction score study. However, this study stratifi ed bleeding events according to thrombosis risk, not bleeding risk (1 of 283 in the low VTE risk group [0.4%; 95% CI, ] and 1 of 711 in the high VTE risk group [0.1%; 95% CI, ]). 9 We also considered bleeding events in a large observational study by Decousus 10 ; however, this study did not report bleeding according to use of pharmacoprophylaxis. Therefore, we chose to use 0.4% (19 of 4,304) derived from the control arm of trials of thromboprophylaxis in medical patients as the estimate of baseline risk of major bleeding (section 2.1). Where possible, we presented data on intracranial bleeding separately from major bleeding events. low risk ( < 4 points;) or high risk (>= 4 points) for VTE. A Patients with local or distant metastases and/or in whom chemotherapy or radiotherapy had been performed in the previous 6 mo. B Anticipated bed rest with bathroom privileges (either because of patient’s limitations or on physician’s order) for at least 3 d. C Carriage of defects of antithrombin, protein C or S, factor V Leiden, G20210A prothrombin mutation, antiphospholipid syndrome. CHEST 2012; 141(2)(Suppl):e195S–e226S
 for at least 3 d. C Carriage of defects of antithrombin, protein C or S, factor V Leiden, G20210A prothrombin mutation, antiphospholipid syndrome. To estimate baseline risk for patients with low and high VTE. risk, we used data from risk assessment models (RAMs). Several. RAMs have been proposed for use in hospitalized medical patients. (Table S3). 5-7 Limitations of most RAMs include lack of prospective. validation, applicability only to high-risk subgroups, inadequate. follow-up time, and excessive complexity. In a prospective observational study of 1,180 inpatients, a. predefi ned RAM (Padua Prediction Score, modifi ed after. Kucher 8 ) assigned points to 11 common VTE risk factors ( Table 2 ) 9. and categorized hospitalized medical patients as low risk. ( , 4 points; 60.3% of patients) or high risk ( 4 points; 39.7% of. patients) for VTE. Attending physicians were not notifi ed of. their patients’ risk categories. Patients were followed for symptomatic. VTE for 90 days. VTE occurred in 11.0% of high-risk. patients who did not receive prophylaxis vs 0.3% of low-risk. patients, a . 30-fold difference in risk (hazard ratio [HR], 32.0; 95% CI, ). Among 711 low-risk patients, two (0.3%) developed VTE (1 PE, 1 PE with DVT). Among 283 high-risk. patients who did not receive prophylaxis, the risk of DVT was. 6.7%, nonfatal PE 3.9%, and fatal PE 0.4%. Hence, for baseline. risk for low- and high-risk strata, we used risk estimates. provided by the Padua Prediction Score. 9 Despite the limitations. of this risk model (small number of events, suboptimal. We considered a number of options for baseline risk of. major bleeding. We considered bleeding events reported in the. Padua prediction score study. However, this study stratifi ed. bleeding events according to thrombosis risk, not bleeding risk. (1 of 283 in the low VTE risk group [0.4%; 95% CI, ] and 1 of 711 in the high VTE risk group [0.1%; 95% CI, ]). 9. We also considered bleeding events in a large observational. study by Decousus 10 ; however, this study did not report bleeding. according to use of pharmacoprophylaxis. Therefore, we chose. to use 0.4% (19 of 4,304) derived from the control arm of trials. of thromboprophylaxis in medical patients as the estimate of. baseline risk of major bleeding (section 2.1). Where possible, we presented data on intracranial bleeding separately from major. bleeding events. low risk ( < 4 points;) or high risk (>= 4 points) for VTE. A Patients with local or distant metastases and/or in whom chemotherapy or radiotherapy had been performed in the previous 6 mo. B Anticipated bed rest with bathroom privileges (either because of patient’s limitations or on physician’s order) for at least 3 d. C Carriage of defects of antithrombin, protein C or S, factor V Leiden, G20210A prothrombin mutation, antiphospholipid syndrome. CHEST 2012; 141(2)(Suppl):e195S–e226S.")
29
Bajo riesgo de sangrado

30
¿Utilizaría tromboprofilaxis durante el ingreso?
No Sí, con medios físicos Sí, con medios farmacológicos Sí, con ambos

31
Ultimas guías ACCP For acutely ill hospitalized medical patients at increased risk of thrombosis who are bleeding or are at high risk for major bleeding, we suggest mechanical thromboprophylaxis with graduated compression stockings (GCS) (Grade 2C) or intermittent pneumatic compression (IPC) (Grade 2C). Uncertainty in the estimates of benefits, risks, and burden; benefi ts, risk, and burden may be closely balanced. Calidad de la evidencia pobre. CHEST 2012; 141(2)(Suppl):e195S–e226S
 (Grade 2C) or intermittent pneumatic compression (IPC) (Grade 2C). Uncertainty in the estimates of benefits, risks, and burden; benefi ts, risk, and burden may be closely balanced. Calidad de la evidencia pobre. CHEST 2012; 141(2)(Suppl):e195S–e226S.")
32
Stockings to Prevent VTE: Direct evidence
from hospitalized nonsurgical patients is available from three randomized trials that have evaluated the use of thigh-length GCS to prevent VTE in patients with myocardial infarction (one trial) 45 and stroke (two trials) 46,47 ( Table 7 , Table S8). In pooled analyses, results failed to demonstrate or exclude a benefi cial effect on symptomatic DVT or PE. Stocking use increased the risk of skin breaks/ulcers but failed to demonstrate or exclude an effect on lower limb ischemia or amputation. It is not known if hospitalized medical patients have a similar risk of skin complications as hospitalized stroke patients. In a recent multicenter RCT that compared kneelength to thigh-length GCS to prevent VTE in immobilized patients with acute stroke, proximal DVT (symptomatic or asymptomatic) occurred in 98 of 1,552 (6.3%) patients who received thigh-length stockings vs 138 of 1,562 (8.8%) who received belowknee stockings (RR, 0.71; 95% CI, ), with no differences between groups in rates of deaths or PE. 48 Skin breaks occurred in 3.9% and 2.9% of patients allocated to thigh-length and knee-length GCS, respectively. These results are diffi cult to interpret alongside evidence from the CLOTS1 trial that thigh-length GCS were not effective to prevent VTE but suggest that if GCS are used, thigh length is preferred to knee length Intermittent Pneumatic Compression Devices to Prevent VTE: An international registry of 15,156 hospitalized acutely ill medical patients found that 22% of US patients received IPC to prevent VTE compared with only 0.2% of patients in other countries. 31 There are no published studies of IPC or VFP devices in hospitalized medical patients. Data are available from a meta-analysis of 22 trials that assessed IPC and VFP, primarily in surgical patients. 50 IPC devices failed to demonstrate or to exclude a benefi - cial effect on mortality or PE but reduced the risk of DVT ( Table 8 , Table S9). No data are available on IPC DVT. skin complications of IPC use, but one might plausibly expect rates to be similar to those of GCS. The panel considered that the evidence for the different outcomes should be rated down due to indirectness because the RR estimates are derived from surgical populations, in whom effects of IPC may be different than in medical patients, and from a mix of symptomatic and asymptomatic events. In summary, indirect data derived primarily from surgical populations suggest that GCS may be modestly effective at preventing asymptomatic DVT and possibly PE in hospitalized medical patients. Direct evidence of low to moderate quality in nonsurgical patients (primarily stroke patients) does not support benefi t, and their use in stroke patients is associated with a 5% risk of skin breakdown. IPCs failed to reduce PE in surgical patients but reduced DVT. Of the two methods, GCS has lower cost and greater ease of use and application than IPCs. Despite the uncertain benefi t, mechanical thromboprophylaxis with GCS or IPCs may be preferable to no prophylaxis in patients at appreciable risk for VTE who are also at high risk for bleeding, as the Eppsteiner meta-analysis showed similar effectiveness but reduced rates of bleeding with mechanical compared with heparin prophylaxis among surgical patients. 51 However, as subgroup analysis in that meta-analysis suggested that LMWH may be more effective than compression, and taking into account that the baseline rate of bleeding is lower among medical patients (average from RCTs, 0.4%) than surgical patients, if the bleeding risk is temporary and if patients remain at high risk of VTE ( Table 2 ), pharmacologic thromboprophylaxis should be initiated once the bleeding risk has decreased.
 45 and stroke. (two trials) 46,47 ( Table 7 , Table S8). In pooled analyses, results failed to demonstrate or exclude a benefi cial. effect on symptomatic DVT or PE. Stocking use. increased the risk of skin breaks/ulcers but failed. to demonstrate or exclude an effect on lower limb. ischemia or amputation. It is not known if hospitalized. medical patients have a similar risk of skin complications. as hospitalized stroke patients. In a recent multicenter RCT that compared kneelength. to thigh-length GCS to prevent VTE in immobilized. patients with acute stroke, proximal DVT. (symptomatic or asymptomatic) occurred in 98 of. 1,552 (6.3%) patients who received thigh-length. stockings vs 138 of 1,562 (8.8%) who received belowknee. stockings (RR, 0.71; 95% CI, ), with. no differences between groups in rates of deaths or. PE. 48 Skin breaks occurred in 3.9% and 2.9% of. patients allocated to thigh-length and knee-length. GCS, respectively. These results are diffi cult to interpret. alongside evidence from the CLOTS1 trial that. thigh-length GCS were not effective to prevent VTE. but suggest that if GCS are used, thigh length is preferred. to knee length. Intermittent Pneumatic Compression Devices. to Prevent VTE: An international registry of 15,156 hospitalized. acutely ill medical patients found that. 22% of US patients received IPC to prevent VTE. compared with only 0.2% of patients in other countries. 31 There are no published studies of IPC or VFP. devices in hospitalized medical patients. Data are. available from a meta-analysis of 22 trials that assessed. IPC and VFP, primarily in surgical patients. 50 IPC. devices failed to demonstrate or to exclude a benefi - cial effect on mortality or PE but reduced the risk of. DVT ( Table 8 , Table S9). No data are available on. IPC. DVT. skin complications of IPC use, but one might plausibly. expect rates to be similar to those of GCS. The. panel considered that the evidence for the different. outcomes should be rated down due to indirectness. because the RR estimates are derived from surgical. populations, in whom effects of IPC may be different. than in medical patients, and from a mix of symptomatic. and asymptomatic events. In summary, indirect data derived primarily from. surgical populations suggest that GCS may be modestly. effective at preventing asymptomatic DVT and. possibly PE in hospitalized medical patients. Direct. evidence of low to moderate quality in nonsurgical. patients (primarily stroke patients) does not support. benefi t, and their use in stroke patients is associated. with a 5% risk of skin breakdown. IPCs failed to. reduce PE in surgical patients but reduced DVT. Of. the two methods, GCS has lower cost and greater. ease of use and application than IPCs. Despite the uncertain benefi t, mechanical thromboprophylaxis. with GCS or IPCs may be preferable. to no prophylaxis in patients at appreciable risk for. VTE who are also at high risk for bleeding, as the. Eppsteiner meta-analysis showed similar effectiveness. but reduced rates of bleeding with mechanical. compared with heparin prophylaxis among surgical. patients. 51 However, as subgroup analysis in that. meta-analysis suggested that LMWH may be more. effective than compression, and taking into account. that the baseline rate of bleeding is lower among. medical patients (average from RCTs, 0.4%) than. surgical patients, if the bleeding risk is temporary. and if patients remain at high risk of VTE ( Table 2 ), pharmacologic thromboprophylaxis should be initiated. once the bleeding risk has decreased.")
34
¿Reduciría el riesgo trombótico la utilización de medias además de la tromboprofilaxis farmacológica? No Sí No hay evidencia

35
Si utilizara tromboprofilaxis farmacológico ¿ qué utilizaria?
HBPM a dosis de bajo riesgo HBPM a dosis de alto riesgo HNF cada 12 horas HNF cada 8 horas Fondaparinux Rivaroxaban 10 mg/días Apixaban 2,5 mg/d

36
Ultimas guías ACCP For acutely ill hospitalized medical patients at increased risk of thrombosis, we recommend anticoagulant thromboprophylaxis with low-molecular-weight heparin (LMWH), low-dose unfractionated heparin (LDUH) bid, LDUH tid, or fondaparinux (Grade 1B) Benefi ts clearly outweigh risk and burdens or viceversa. Calidad de la evidencia media Recomendaciones basadas en tres metaana´lisi s y revisiones sistyemáticas Alikhan R , Cohen AT . Heparin for the prevention of venous thromboembolism in general medical patients (excluding stroke and myocardial infarction) . Cochrane Database Syst Rev ;( 3 ): CD 24 . Dentali F , Douketis JD , Gianni M , Lim W , Crowther MA . Meta-analysis: anticoagulant prophylaxis to prevent symptomatic venous thromboembolism in hospitalized medical patients . Ann Intern Med ; 146 ( 4 ): 25 . Lloyd NS, Douketis JD, Moinuddin I, Lim W, Crowther MA. Anticoagulant prophylaxis to prevent asymptomatic deep vein thrombosis in hospitalized medical patients: a systematic review and meta-analysis . J Thromb Haemost ; 6 ( 3 ): The potential for less bleeding with LMWH represents a benefi t that is small, and it may be very small. From a patient preference perspective, twice daily injections are likely to be preferred and better tolerated than thrice daily injections. In summary, there is no clear evidence in the current literature to support choosing one form of pharmacoprophylaxis over another in the medical population based on outcomes or from a cost-effectiveness standpoint. It would be reasonable to make choices based on patient preference, compliance, and ease of the panel considered that providing prophylaxis for 6 to 21 days, until full mobility is restored or until discharge from hospital, whichever comes fi rst, is a reasonable approach. CHEST 2012; 141(2)(Suppl):e195S–e226S 36
, low-dose unfractionated heparin (LDUH) bid, LDUH tid, or fondaparinux (Grade 1B) Benefi ts clearly outweigh risk and burdens or viceversa. Calidad de la evidencia media. Recomendaciones basadas en tres metaana´lisi s y revisiones sistyemáticas. Alikhan R , Cohen AT . Heparin for the prevention of venous. thromboembolism in general medical patients (excluding. stroke and myocardial infarction) . Cochrane Database Syst. Rev ;( 3 ): CD Dentali F , Douketis JD , Gianni M , Lim W , Crowther MA . Meta-analysis: anticoagulant prophylaxis to prevent symptomatic. venous thromboembolism in hospitalized medical. patients . Ann Intern Med ; 146 ( 4 ): Lloyd NS, Douketis JD, Moinuddin I, Lim W, Crowther MA. Anticoagulant prophylaxis to prevent asymptomatic deep. vein thrombosis in hospitalized medical patients: a systematic. review and meta-analysis . J Thromb Haemost ; 6 ( 3 ): The potential for less bleeding with LMWH represents a benefi t that is small, and it may be very small. From a patient preference perspective, twice daily injections are likely to be preferred and better tolerated than thrice daily injections. In summary, there is no clear evidence in the current. literature to support choosing one form of pharmacoprophylaxis. over another in the medical population. based on outcomes or from a cost-effectiveness. standpoint. It would be reasonable to make choices. based on patient preference, compliance, and ease of. the panel considered that providing prophylaxis for 6 to 21 days, until full mobility is restored or until discharge from hospital, whichever comes fi rst, is a reasonable approach. CHEST 2012; 141(2)(Suppl):e195S–e226S. 36.")
37
Remarks: In choosing the specific anticoagulant drug to be used for pharmacoprophylaxis, choices should be based on patient preference, compliance, and ease of administration (eg, daily vs bid vs tid dosing), as well as on local factors affecting acquisition costs (eg, prices of various pharmacologic agents in individual hospital formularies).
, as well as on local factors affecting acquisition costs (eg, prices of various pharmacologic agents in individual hospital formularies).")
38
Semin Thromb Hemost. 2011 Apr;37(3):267-74.
Prevention of venous thromboembolism in medical patients with thrombocytopenia or with platelet dysfunction: a review of the literature. Tufano A, al. At variance with severe thrombocytopenia (< 50,000/μL), mild/moderate thrombocytopenia (> 50,000/μL) should not interfere with VTE prevention decisions. In severe thrombocytopenia, prophylaxis should be considered on an individual basis: Low platelet number/function and clotting abnormalities are common in patients with liver cirrhosis. However, these patients have a high incidence of portal and idiopathic venous thromboses, implying that cirrhotic coagulopathy does not protect against thrombosis. Semin Thromb Hemost Apr;37(3): Epub 2011 Mar 31. Prevention of venous thromboembolism in medical patients with thrombocytopenia or with platelet dysfunction: a review of the literature. Tufano A, Guida A, Di Minno MN, Prisco D, Cerbone AM, Di Minno G. Abstract Current guidelines for venous thromboembolism (VTE) primary prophylaxis are based on randomized clinical trials that exclude subjects at a potentially high bleeding risk. Thus no specific recommendation/algorithm for pharmacological prophylaxis in patients with thrombocytopenia and/or platelet dysfunction is available. Because at least 25% of subjects admitted to medical departments exhibit these conditions, information on this subject is provided here to optimize their VTE prophylaxis. Low platelet number/function and clotting abnormalities are common in patients with liver cirrhosis. However, these patients have a high incidence of portal and idiopathic venous thromboses, implying that cirrhotic coagulopathy does not protect against thrombosis. At variance with severe thrombocytopenia (< 50,000/μL), mild/moderate thrombocytopenia (> 50,000/μL) should not interfere with VTE prevention decisions. In severe thrombocytopenia, prophylaxis should be considered on an individual basis, however. In patients with antiphospholipid antibodies and thrombocytopenia, a thrombotic tendency is usually associated rather than a bleeding risk. VTE prophylaxis in high-risk conditions is thus suggested in these patients. Except in cases with contraindications to anticoagulation, antithrombotic prophylaxis should be always considered in hospitalized cancer patients with thrombocytopenia, especially in those with hematologic malignancies and multiple VTE risk factors. Aspirin treatment is not as effective as heparins in lowering the risk of VTE. Studies in stroke suggest that thromboprophylaxis with heparins is safe in patients with ischemic stroke undergoing aspirin treatment. The need for VTE prophylaxis in patients on chronic treatment with aspirin and/or clopidogrel should be evaluated after assessing the individual risk-benefit ratio.
, mild/moderate thrombocytopenia (> 50,000/μL) should not interfere with VTE prevention decisions. In severe thrombocytopenia, prophylaxis should be considered on an individual basis: Low platelet number/function and clotting abnormalities are common in patients with liver cirrhosis. However, these patients have a high incidence of portal and idiopathic venous thromboses, implying that cirrhotic coagulopathy does not protect against thrombosis. Semin Thromb Hemost Apr;37(3): Epub 2011 Mar 31. Prevention of venous thromboembolism in medical patients with thrombocytopenia or with platelet dysfunction: a review of the literature. Tufano A, Guida A, Di Minno MN, Prisco D, Cerbone AM, Di Minno G. Abstract. Current guidelines for venous thromboembolism (VTE) primary prophylaxis are based on randomized clinical trials that exclude subjects at a potentially high bleeding risk. Thus no specific recommendation/algorithm for pharmacological prophylaxis in patients with thrombocytopenia and/or platelet dysfunction is available. Because at least 25% of subjects admitted to medical departments exhibit these conditions, information on this subject is provided here to optimize their VTE prophylaxis. Low platelet number/function and clotting abnormalities are common in patients with liver cirrhosis. However, these patients have a high incidence of portal and idiopathic venous thromboses, implying that cirrhotic coagulopathy does not protect against thrombosis. At variance with severe thrombocytopenia (< 50,000/μL), mild/moderate thrombocytopenia (> 50,000/μL) should not interfere with VTE prevention decisions. In severe thrombocytopenia, prophylaxis should be considered on an individual basis, however. In patients with antiphospholipid antibodies and thrombocytopenia, a thrombotic tendency is usually associated rather than a bleeding risk. VTE prophylaxis in high-risk conditions is thus suggested in these patients. Except in cases with contraindications to anticoagulation, antithrombotic prophylaxis should be always considered in hospitalized cancer patients with thrombocytopenia, especially in those with hematologic malignancies and multiple VTE risk factors. Aspirin treatment is not as effective as heparins in lowering the risk of VTE. Studies in stroke suggest that thromboprophylaxis with heparins is safe in patients with ischemic stroke undergoing aspirin treatment. The need for VTE prophylaxis in patients on chronic treatment with aspirin and/or clopidogrel should be evaluated after assessing the individual risk-benefit ratio.")
41
Anciana institucionalizada con ingreso hospitalario por ITU

42
Anciana institucionalizada con ingreso hospitalario por ITU
Paciente de 88 años, con deterioro cognitivo moderado por enfermedad de Alzheimer. Obesidad. Vive en una residencia. Vida cama/sillón. Dependiente para todas las actividades de la vida diaria. Incapacidad para deambular Antecedentes de TVP tras cirugía de cadera hace 2 años. Ingresa por cuadro febril y deterioro de función renal secundario a ITU, permaneciendo ingresada durante 7 días con sueroterapia y antibioterapia y enoxaparina 40 mg cc/24 hs. Alta aconsejando mantener 7 días más la TP

43
Analítica Hb 9,2 gr/dl Plaq Cr: 1,2 mg/dl . FGE 50 ml/m

44
No Si, medias elásticas Sí, AAS 500 mg al día Sí HBPM Si ribaroxaban
Tras el alta, y pasados esos 7 días, continuaría con tromboprofilaxis ? No Si, medias elásticas Sí, AAS 500 mg al día Sí HBPM Si ribaroxaban

45
Ultimas guías ACCP In chronically immobilized persons residing
at home or at a nursing home, we suggest against the routine use of thromboprophylaxis (Grade 2C) . The chronically immobile population is large and includes patients who are homebound, as well as residents of nursing homes and postacute care facilities. Despite their similarities to medical inpatients, there have been few studies and no placebo-controlled trials investigating VTE prophylaxis for chronically immobilized outpatients. Although the population at risk is clearly large, the scope of the problem and incidence of symptomatic VTE is uncertain. One study of outpatients examined the incidence of symptomatic VTE in 16,532 outpatients . 40 years of age (median age, 71 years) who were not immobile at baseline and had an acute med- ical condition reducing mobility for at least 48 h. 115 Anticoagulant prophylaxis was administered to 35% of patients. The study found a 1.2% incidence of symptomatic VTE in the 3 weeks after the onset of the acute condition. This incidence is similar to studies examining patients hospitalized with acute medical conditions, but the pattern of immobility (acute rather than chronic) does not allow extrapolation to homebound patients. Several observational studies have examined the incidence of VTE in nursing home patients, including two large studies using the Minimum Data Set, a mandatory questionnaire completed for all Medicarelicensed long-term facilities in the United States. 116,117 Liperoti and colleagues retrospectively assessed 132,018 nursing home patients across fi ve state and found a symptomatic VTE incidence of 0.91 per 100 person-years. Similarly, a retrospective study of 18,661 nursing home patients in Kansas found a VTE incidence of 1.30 per 100 person-years. 116 These studies suggest that the best estimate of the annual incidence of symptomatic VTE in nursing home patients is approximately 1%. The use of anticoagulant prophylaxis has not been examined adequately in this population to draw conclusions on whether the benefi ts outweigh the risks and costs. The incidence of VTE in postacute care facilities was examined in a prospective cohort study of 3,039 patients admitted for rehabilitation after acute medical illness or surgery. 118 Reasons for admission to the facility included medical illness (54.7%), stroke (21.1%), and surgery (31.7%). Most patients (75.1%) received anticoagulant thromboprophylaxis, which was primarily LMWH. The incidence of symptomatic VTE was 2.4% during the stay at the facility (median duration 26 days). Risk factors for VTE were cancer and prior VTE. Two cross-sectional studies examined the prevalence of asymptomatic DVT in elderly patients in postacute care facilities in France and detected asymptomatic DVT in 14.0% and 15.8% of patients, respectively. 119,120 A subsequent analysis that combined data from these two studies noted that although proximal DVT was not signifi cantly reduced among patients who received LMWH prophylaxis (5.7% vs 4.0%; P 5 .16), this difference became statistically signifi cant with the use of propensity analysis to control for potentially confounding variables (OR, 0.56; P 5 .03). 121 These studies suggest that the incidence of asymptomatic DVT in elderly patients in postacute care facilities is similar to that of hospitalized patients. However, their observational designs and lack of patient-important end points does not allow for any conclusions to be drawn on whether thrombopro The available data suggest that nursing home patients have an incidence of symptomatic VTE of 1% annually and postacute care patients have an incidence of 1.0% to 2.4% during their stay at the facility. These data offer some indirect support for prophylaxis of immobile patients in postacute or subacute care facilities, as their incidence of VTE may be similar to that of acutely ill hospitalized patients. Randomized trials are needed to determine if the benefi ts of anticoagulant thromboprophylaxis outweigh the risks in this population. CHEST 2012; 141(2)(Suppl):e195S–e226S
 . The chronically. immobile population is large and includes patients. who are homebound, as well as residents of nursing. homes and postacute care facilities. Despite their. similarities to medical inpatients, there have been. few studies and no placebo-controlled trials investigating. VTE prophylaxis for chronically immobilized. outpatients. Although the population at risk is clearly large, the. scope of the problem and incidence of symptomatic. VTE is uncertain. One study of outpatients examined. the incidence of symptomatic VTE in 16,532 outpatients years of age (median age, 71 years) who. were not immobile at baseline and had an acute med- ical condition reducing mobility for at least 48 h Anticoagulant prophylaxis was administered to 35% of patients. The study found a 1.2% incidence of. symptomatic VTE in the 3 weeks after the onset of. the acute condition. This incidence is similar to studies. examining patients hospitalized with acute medical. conditions, but the pattern of immobility (acute rather. than chronic) does not allow extrapolation to homebound. patients. Several observational studies have examined the. incidence of VTE in nursing home patients, including. two large studies using the Minimum Data Set, a. mandatory questionnaire completed for all Medicarelicensed. long-term facilities in the United States. 116,117. Liperoti and colleagues retrospectively assessed. 132,018 nursing home patients across fi ve state. and found a symptomatic VTE incidence of per 100 person-years. Similarly, a retrospective study. of 18,661 nursing home patients in Kansas found a. VTE incidence of 1.30 per 100 person-years. 116 These. studies suggest that the best estimate of the annual. incidence of symptomatic VTE in nursing home. patients is approximately 1%. The use of anticoagulant. prophylaxis has not been examined adequately. in this population to draw conclusions on whether. the benefi ts outweigh the risks and costs. The incidence of VTE in postacute care facilities. was examined in a prospective cohort study of. 3,039 patients admitted for rehabilitation after acute. medical illness or surgery. 118 Reasons for admission to. the facility included medical illness (54.7%), stroke. (21.1%), and surgery (31.7%). Most patients (75.1%) received anticoagulant thromboprophylaxis, which. was primarily LMWH. The incidence of symptomatic. VTE was 2.4% during the stay at the facility. (median duration 26 days). Risk factors for VTE were. cancer and prior VTE. Two cross-sectional studies examined the prevalence. of asymptomatic DVT in elderly patients in. postacute care facilities in France and detected. asymptomatic DVT in 14.0% and 15.8% of patients, respectively. 119,120 A subsequent analysis that combined. data from these two studies noted that although. proximal DVT was not signifi cantly reduced among. patients who received LMWH prophylaxis (5.7% vs 4.0%; P 5 .16), this difference became statistically. signifi cant with the use of propensity analysis to control. for potentially confounding variables (OR, 0.56; P 5 .03). 121 These studies suggest that the incidence. of asymptomatic DVT in elderly patients in postacute. care facilities is similar to that of hospitalized patients. However, their observational designs and lack of. patient-important end points does not allow for any. conclusions to be drawn on whether thrombopro. The available data suggest that nursing home. patients have an incidence of symptomatic VTE of. 1% annually and postacute care patients have an. incidence of 1.0% to 2.4% during their stay at the. facility. These data offer some indirect support for. prophylaxis of immobile patients in postacute or. subacute care facilities, as their incidence of VTE. may be similar to that of acutely ill hospitalized. patients. Randomized trials are needed to determine. if the benefi ts of anticoagulant thromboprophylaxis. outweigh the risks in this population. CHEST 2012; 141(2)(Suppl):e195S–e226S.")
46
Si optara por mantener la HBPM al alta, cuánto tiempo la mantendría ?
Hasta que volviera a su situación basal una vez finalizada la antibioterapia. Hasta completar 15 días desde el inicio de la HBPM Hasta completar 3 semanas. Indefinida.

47
The available data suggest that nursing home patients have an incidence of symptomatic VTE of 1% annually and postacute care patients have an incidence of 1.0% to 2.4% during their stay at the facility. These data offer some indirect support for prophylaxis of immobile patients in postacute or subacute care facilities, as their incidence of VTE may be similar to that of acutely ill hospitalized patients. Randomized trials are needed to determine if the benefits of anticoagulant thromboprophylaxis outweigh the risks in this population. CHEST 2012; 141(2)(Suppl):e195S–e226S
(Suppl):e195S–e226S.")
48
exclude benefi ts or harm for fatal PE (RR, 0.34;
95% CI, ) and overall mortality (RR, 1.00; 95% CI, ). The risk of major bleeding was signifi cantly increased with extended-duration enoxaparin (RR, 2.51; 95% CI, ), and there were four intracranial bleeding events (one fatal) in the extended enoxaparin group compared with none in the placebo group. In terms of absolute effects, extended-duration enoxaparin prevented six fewer symptomatic proximal DVT per 1,000 (95% CI, from three fewer to seven fewer) at a cost of fi ve more major bleeding events per 1,000 (95% CI, from one more to 14 more) ( Table 9 , Tables S10, S11). In addition to the bleeding risk, extended prophylaxis also entails the burden and cost of daily injection.
 and overall mortality (RR, 1.00; 95% CI, ). The risk of major bleeding was. signifi cantly increased with extended-duration enoxaparin. (RR, 2.51; 95% CI, ), and there were. four intracranial bleeding events (one fatal) in the. extended enoxaparin group compared with none. in the placebo group. In terms of absolute effects, extended-duration enoxaparin prevented six fewer. symptomatic proximal DVT per 1,000 (95% CI, from. three fewer to seven fewer) at a cost of fi ve more. major bleeding events per 1,000 (95% CI, from one. more to 14 more) ( Table 9 , Tables S10, S11). In addition. to the bleeding risk, extended prophylaxis also. entails the burden and cost of daily injection.")
49
Incidencia bajísima de ETEV sintomática
EXCLAIM (Extended Prophylaxis for Venous ThromboEmbolism in Acutely Ill Medical Patients With Prolonged Immobilization) study. . Beneficio solo en mujeres, > 75 años y aquellos con inmovilización completa. ( nivel 1) (no desplazaminmetos al servicio) Incidencia bajísima de ETEV sintomática Alta incidencia de hemorragias ( similar a la encontrada en ensayos de tratamiento vs placebo). BACKGROUND: Extended-duration low-molecular-weight heparin has been shown to prevent venous thromboembolism (VTE) in high-risk surgical patients. OBJECTIVE: To evaluate the efficacy and safety of extended-duration enoxaparin thromboprophylaxis in acutely ill medical patients. DESIGN: Randomized, parallel, placebo-controlled trial. Randomization was computer-generated. Allocation was centralized. Patients, caregivers, and outcome assessors were blinded to group assignment. (ClinicalTrials.gov registration number: NCT ) SETTING: 370 sites in 20 countries across North and South America, Europe, and Asia. PATIENTS: Acutely ill medical patients 40 years or older with recently reduced mobility (bed rest or sedentary without [level 1] or with [level 2] bathroom privileges). Eligibility criteria for patients with level 2 immobility were amended to include only those who had additional VTE risk factors (age >75 years, history of VTE, or active or previous cancer) after interim analyses suggested lower-than-expected VTE rates. INTERVENTION: Enoxaparin, 40 mg/d subcutaneously (2975 patients), or placebo (2988 patients), for 28 +/- 4 days after receiving open-label enoxaparin for an initial 10 +/- 4 days. MEASUREMENTS: Incidence of VTE up to day 28 and of major bleeding events up to 48 hours after the last study treatment dose. RESULTs: Extended-duration enoxaparin reduced VTE incidence compared with placebo (2.5% vs. 4%; absolute risk difference favoring enoxaparin, -1.53% [95.8% CI, -2.54% to -0.52%]). Enoxaparin increased major bleeding events (0.8% vs. 0.3%; absolute risk difference favoring placebo, 0.51% [95% CI, 0.12% to 0.89%]). The benefits of extended-duration enoxaparin seemed to be restricted to women, patients older than 75 years, and those with level 1 immobility. LIMITATION: Estimates of efficacy and safety for the overall trial population are difficult to interpret because of the change in eligibility criteria during the trial. CONCLUSION: Use of extended-duration enoxaparin reduces VTE more than it increases major bleeding events in acutely ill medical patients with level 1 immobility, those older than 75 years, and women. Thromb Thrombolysis May 8. [Epub ahead of print] Standard or extended-duration prophylaxis in medical patients? A review of the evidence. Stark JE, Smith WJ. Source Department of Pharmacy, Washington Regional Medical Center, 3215 N. North Hills Blvd, Fayetteville, AR, 72703, USA, Abstract Acutely ill medical patients are at significant risk of venous thromboembolism (VTE). Thromboprophylaxis can substantially reduce the incidence of VTE, but to be optimally effective must consist of the correct choice of agent, at an appropriate dose, and for sufficient duration. Increasing evidence suggests that VTE risk persists beyond the standard period of prophylaxis. Although there is evidence that extended-duration prophylaxis is beneficial in preventing late VTE complications in high-risk surgical patients, few data exist in medical patients. The recent EXCLAIM study demonstrated that, subsequent to a standard prophylaxis regimen of 10 ± 4 days with enoxaparin 40 mg once daily, extended-duration prophylaxis (28 ± 4 days) with enoxaparin reduced total VTE events compared with placebo: 2.5% versus 4.0%; (absolute risk difference -1.53%; 95.8% confidence interval [CI] to -0.52), with parallel increases in major bleeding rates (0.8% vs. 0.3%; absolute risk difference 0.51%; 95% CI %). The reduction in total VTE was principally driven by a decrease in symptomatic deep-vein thrombosis (absolute risk difference -0.60%; 95.8% CI to -0.19%). Favorable benefit-to-risk ratios were observed in certain high-risk patient groups: level 1 immobility, women, and age >75 years. In addition to their underlying medical condition, medical patients often have multiple risk factors, placing them at sustained risk of VTE. Extended-duration prophylaxis might be most relevant in such patients. The development of appropriate risk assessment tools could help identify medical patients at greatest risk of late VTE events who might benefit most from extended-duration prophylaxis. Ann Intern Med Jul 6; 153(1):8-18 49
 study. . Beneficio solo en mujeres, > 75 años y aquellos con inmovilización completa. ( nivel 1) (no desplazaminmetos al servicio) Incidencia bajísima de ETEV sintomática. Alta incidencia de hemorragias ( similar a la encontrada en ensayos de tratamiento vs placebo). BACKGROUND: Extended-duration low-molecular-weight heparin has been shown to prevent venous thromboembolism (VTE) in high-risk surgical patients. OBJECTIVE: To evaluate the efficacy and safety of extended-duration enoxaparin thromboprophylaxis in acutely ill medical patients. DESIGN: Randomized, parallel, placebo-controlled trial. Randomization was computer-generated. Allocation was centralized. Patients, caregivers, and outcome assessors were blinded to group assignment. (ClinicalTrials.gov registration number: NCT ) SETTING: 370 sites in 20 countries across North and South America, Europe, and Asia. PATIENTS: Acutely ill medical patients 40 years or older with recently reduced mobility (bed rest or sedentary without [level 1] or with [level 2] bathroom privileges). Eligibility criteria for patients with level 2 immobility were amended to include only those who had additional VTE risk factors (age >75 years, history of VTE, or active or previous cancer) after interim analyses suggested lower-than-expected VTE rates. INTERVENTION: Enoxaparin, 40 mg/d subcutaneously (2975 patients), or placebo (2988 patients), for 28 +/- 4 days after receiving open-label enoxaparin for an initial 10 +/- 4 days. MEASUREMENTS: Incidence of VTE up to day 28 and of major bleeding events up to 48 hours after the last study treatment dose. RESULTs: Extended-duration enoxaparin reduced VTE incidence compared with placebo (2.5% vs. 4%; absolute risk difference favoring enoxaparin, -1.53% [95.8% CI, -2.54% to -0.52%]). Enoxaparin increased major bleeding events (0.8% vs. 0.3%; absolute risk difference favoring placebo, 0.51% [95% CI, 0.12% to 0.89%]). The benefits of extended-duration enoxaparin seemed to be restricted to women, patients older than 75 years, and those with level 1 immobility. LIMITATION: Estimates of efficacy and safety for the overall trial population are difficult to interpret because of the change in eligibility criteria during the trial. CONCLUSION: Use of extended-duration enoxaparin reduces VTE more than it increases major bleeding events in acutely ill medical patients with level 1 immobility, those older than 75 years, and women. Thromb Thrombolysis May 8. [Epub ahead of print] Standard or extended-duration prophylaxis in medical patients A review of the evidence. Stark JE, Smith WJ. Source. Department of Pharmacy, Washington Regional Medical Center, 3215 N. North Hills Blvd, Fayetteville, AR, 72703, USA, Abstract. Acutely ill medical patients are at significant risk of venous thromboembolism (VTE). Thromboprophylaxis can substantially reduce the incidence of VTE, but to be optimally effective must consist of the correct choice of agent, at an appropriate dose, and for sufficient duration. Increasing evidence suggests that VTE risk persists beyond the standard period of prophylaxis. Although there is evidence that extended-duration prophylaxis is beneficial in preventing late VTE complications in high-risk surgical patients, few data exist in medical patients. The recent EXCLAIM study demonstrated that, subsequent to a standard prophylaxis regimen of 10 ± 4 days with enoxaparin 40 mg once daily, extended-duration prophylaxis (28 ± 4 days) with enoxaparin reduced total VTE events compared with placebo: 2.5% versus 4.0%; (absolute risk difference -1.53%; 95.8% confidence interval [CI] to -0.52), with parallel increases in major bleeding rates (0.8% vs. 0.3%; absolute risk difference 0.51%; 95% CI %). The reduction in total VTE was principally driven by a decrease in symptomatic deep-vein thrombosis (absolute risk difference -0.60%; 95.8% CI to -0.19%). Favorable benefit-to-risk ratios were observed in certain high-risk patient groups: level 1 immobility, women, and age >75 years. In addition to their underlying medical condition, medical patients often have multiple risk factors, placing them at sustained risk of VTE. Extended-duration prophylaxis might be most relevant in such patients. The development of appropriate risk assessment tools could help identify medical patients at greatest risk of late VTE events who might benefit most from extended-duration prophylaxis. Ann Intern Med Jul 6; 153(1):")
50
Turpie AG, et all EXCLAIM Investigators. BACKGROUND AND PURPOSE:
Stroke Jan;44(1): Venous thromboembolism risk in ischemic stroke patients receiving extended-duration enoxaparin prophylaxis: results from the EXCLAIM study. Turpie AG, et all EXCLAIM Investigators. BACKGROUND AND PURPOSE: The optimal duration of venous thromboembolism prophylaxis in acute stroke patients is unknown. This subanalysis of the Extended Prophylaxis for Venous ThromboEmbolism in Acutely Ill Medical Patients With Prolonged Immobilization (EXCLAIM) study investigated extended-duration thromboprophylaxis with enoxaparin, compared with placebo following standard-duration enoxaparin, in ischemic stroke patients. METHODS: Acutely ill medical patients with recently reduced mobility received open-label enoxaparin 40 mg for 10±4 days, and they were then randomized to double-blind enoxaparin 40 mg daily or placebo for further 28±4 days. Venous thromboembolism incidence (symptomatic/asymptomatic deep-vein thrombosis, symptomatic/fatal pulmonary embolism) up to day 28 after randomization and major bleeding rates up to 48 h after the last dose of study treatment were reported. RESULTS: In total, 389 of 5963 (6.5%) randomized patients had ischemic stroke: 198 received extended-duration prophylaxis and 191 placebo. Extended-duration prophylaxis reduced venous thromboembolism incidence versus placebo (2.4% versus 8.0%; absolute risk difference, -5.6%; 95% CI, -10.5% to -0.7%), but it was associated with an increase in major bleeding (1.5% versus 0% in enoxaparin and placebo groups; absolute risk difference, +1.5%; 95% CI, -0.2% to 3.2%). CONCLUSIONS: Extended-duration thromboprophylaxis with enoxaparin was associated with reduced venous thromboembolism risk and increased major bleeding in the subgroup of patients with ischemic stroke in the EXCLAIM study. Stroke Jan;44(1): doi: /STROKEAHA Epub 2012 Nov 1. Venous thromboembolism risk in ischemic stroke patients receiving extended-duration enoxaparin prophylaxis: results from the EXCLAIM study. Turpie AG, Hull RD, Schellong SM, Tapson VF, Monreal M, Samama MM, Chen M, Yusen RD; EXCLAIM Investigators. Source Department of Medicine, McMaster University, Hamilton Health Sciences-General Hospital, 237 Barton Street East, Hamilton, Ontario L8L 2X2, Canada. Abstract BACKGROUND AND PURPOSE: The optimal duration of venous thromboembolism prophylaxis in acute stroke patients is unknown. This subanalysis of the Extended Prophylaxis for Venous ThromboEmbolism in Acutely Ill Medical Patients With Prolonged Immobilization (EXCLAIM) study investigated extended-duration thromboprophylaxis with enoxaparin, compared with placebo following standard-duration enoxaparin, in ischemic stroke patients. METHODS: Acutely ill medical patients with recently reduced mobility received open-label enoxaparin 40 mg for 10±4 days, and they were then randomized to double-blind enoxaparin 40 mg daily or placebo for further 28±4 days. Venous thromboembolism incidence (symptomatic/asymptomatic deep-vein thrombosis, symptomatic/fatal pulmonary embolism) up to day 28 after randomization and major bleeding rates up to 48 h after the last dose of study treatment were reported. RESULTS: In total, 389 of 5963 (6.5%) randomized patients had ischemic stroke: 198 received extended-duration prophylaxis and 191 placebo. Extended-duration prophylaxis reduced venous thromboembolism incidence versus placebo (2.4% versus 8.0%; absolute risk difference, -5.6%; 95% CI, -10.5% to -0.7%), but it was associated with an increase in major bleeding (1.5% versus 0% in enoxaparin and placebo groups; absolute risk difference, +1.5%; 95% CI, -0.2% to 3.2%). CONCLUSIONS: Extended-duration thromboprophylaxis with enoxaparin was associated with reduced venous thromboembolism risk and increased major bleeding in the subgroup of patients with ischemic stroke in the EXCLAIM study.
: Venous thromboembolism risk in ischemic stroke patients receiving extended-duration enoxaparin prophylaxis: results from the EXCLAIM study. Turpie AG, et all EXCLAIM Investigators. BACKGROUND AND PURPOSE: The optimal duration of venous thromboembolism prophylaxis in acute stroke patients is unknown. This subanalysis of the Extended Prophylaxis for Venous ThromboEmbolism in Acutely Ill Medical Patients With Prolonged Immobilization (EXCLAIM) study investigated extended-duration thromboprophylaxis with enoxaparin, compared with placebo following standard-duration enoxaparin, in ischemic stroke patients. METHODS: Acutely ill medical patients with recently reduced mobility received open-label enoxaparin 40 mg for 10±4 days, and they were then randomized to double-blind enoxaparin 40 mg daily or placebo for further 28±4 days. Venous thromboembolism incidence (symptomatic/asymptomatic deep-vein thrombosis, symptomatic/fatal pulmonary embolism) up to day 28 after randomization and major bleeding rates up to 48 h after the last dose of study treatment were reported. RESULTS: In total, 389 of 5963 (6.5%) randomized patients had ischemic stroke: 198 received extended-duration prophylaxis and 191 placebo. Extended-duration prophylaxis reduced venous thromboembolism incidence versus placebo (2.4% versus 8.0%; absolute risk difference, -5.6%; 95% CI, -10.5% to -0.7%), but it was associated with an increase in major bleeding (1.5% versus 0% in enoxaparin and placebo groups; absolute risk difference, +1.5%; 95% CI, -0.2% to 3.2%). CONCLUSIONS: Extended-duration thromboprophylaxis with enoxaparin was associated with reduced venous thromboembolism risk and increased major bleeding in the subgroup of patients with ischemic stroke in the EXCLAIM study. Stroke Jan;44(1): doi: /STROKEAHA Epub 2012 Nov 1. Venous thromboembolism risk in ischemic stroke patients receiving extended-duration enoxaparin prophylaxis: results from the EXCLAIM study. Turpie AG, Hull RD, Schellong SM, Tapson VF, Monreal M, Samama MM, Chen M, Yusen RD; EXCLAIM Investigators. Source. Department of Medicine, McMaster University, Hamilton Health Sciences-General Hospital, 237 Barton Street East, Hamilton, Ontario L8L 2X2, Canada. Abstract. BACKGROUND AND PURPOSE: The optimal duration of venous thromboembolism prophylaxis in acute stroke patients is unknown. This subanalysis of the Extended Prophylaxis for Venous ThromboEmbolism in Acutely Ill Medical Patients With Prolonged Immobilization (EXCLAIM) study investigated extended-duration thromboprophylaxis with enoxaparin, compared with placebo following standard-duration enoxaparin, in ischemic stroke patients. METHODS: Acutely ill medical patients with recently reduced mobility received open-label enoxaparin 40 mg for 10±4 days, and they were then randomized to double-blind enoxaparin 40 mg daily or placebo for further 28±4 days. Venous thromboembolism incidence (symptomatic/asymptomatic deep-vein thrombosis, symptomatic/fatal pulmonary embolism) up to day 28 after randomization and major bleeding rates up to 48 h after the last dose of study treatment were reported. RESULTS: In total, 389 of 5963 (6.5%) randomized patients had ischemic stroke: 198 received extended-duration prophylaxis and 191 placebo. Extended-duration prophylaxis reduced venous thromboembolism incidence versus placebo (2.4% versus 8.0%; absolute risk difference, -5.6%; 95% CI, -10.5% to -0.7%), but it was associated with an increase in major bleeding (1.5% versus 0% in enoxaparin and placebo groups; absolute risk difference, +1.5%; 95% CI, -0.2% to 3.2%). CONCLUSIONS: Extended-duration thromboprophylaxis with enoxaparin was associated with reduced venous thromboembolism risk and increased major bleeding in the subgroup of patients with ischemic stroke in the EXCLAIM study.")
51
Bajo riesgo de sangrado

52
medical patients (section 2.9) is based on indirect
Our summary of ASA to prevent VTE in hospitalized evidence from the PEP (Pulmonary Embolism Prevention) trial, a multicenter trial of ASA 160 mg daily vs placebo for 35 days in hip fracture surgery or elective hip or knee arthroplasty patients 58 for the outcomes mortality, symptomatic DVT, and bleeding; and the PEP trial meta-analysis of 53 randomized trials (nine trials conducted in medical patients, as discussed above) of antiplatelet therapy to prevent VTE for the outcome PE. Use of ASA/antiplatelet drugs, compared with placebo, had little or no effect on mortality (RR, 0.97; 95% CI, ) and was associated with a reduced risk of PE (RR, 0.47; 95% CI, ), a reduced risk of DVT (RR, 0.71; 95% CI, ), and an increased risk of nonsurgical site-related bleeding events (RR, 1.42; 95% CI, ). The quality of the evidence was rated down for indirectness based on relative effects derived primarily from surgical patients (only 555 of the 26,890 patients included in PEP trial report metaanalysis were high-risk medical patients, and all PEP trials participants were orthopedic surgery patients). The panel judged that based on the low quality of available evidence pertaining to use of ASA to prevent VTE in hospitalized medical patients, no recommendation could be made. There have been no studies of antiplatelet therapy compared with antithrombotic therapy to prevent VTE in acutely ill medical patients. 2.10 Screening for DVT in Hospitalized Medical Patients Ultrasound screening in medical patients has not been systematically studied. Indirect evidence from hospitalized orthopedic patients 59 and spinal cord injury patients 60 suggests that routine screening is not of benefi t to reduce symptomatic VTE events. For example, in a population of patients who had joint arthroplasty and were receiving warfarin prophylaxis, screening compression ultrasonography with subsequent treatment of identifi ed asymptomatic DVT did not reduce the rate of subsequent symptomatic VTE. 59 In a population with a low prevalence of DVT, such as medical patients, even with a highly-specifi c test such as ultrasound, one would anticipate a substantial number of false-positive results. Moreover, even without considering false-positive results, routine ultrasound screening would be associated with appreciable cost and inconvenience without evidence of benefi t. 2.10 Screening for DVT in Hospitalized Medical Patients 2.11 Gaps in Care Low rates of adherence to recommended thromboprophylaxis regimens have been documented worldwide. 31,61-64 In the last few years, research efforts have focused on evaluating strategies to improve uptake of evidence-based VTE prophylaxis regimens in hospitalized patients, including medical patients. Results
 trial, a multicenter trial of ASA 160 mg. daily vs placebo for 35 days in hip fracture surgery or. elective hip or knee arthroplasty patients 58 for the. outcomes mortality, symptomatic DVT, and bleeding; and the PEP trial meta-analysis of 53 randomized. trials (nine trials conducted in medical patients, as. discussed above) of antiplatelet therapy to prevent. VTE for the outcome PE. Use of ASA/antiplatelet. drugs, compared with placebo, had little or no effect. on mortality (RR, 0.97; 95% CI, ) and. was associated with a reduced risk of PE (RR, 0.47; 95% CI, ), a reduced risk of DVT (RR, 0.71; 95% CI, ), and an increased risk of nonsurgical. site-related bleeding events (RR, 1.42; 95% CI, ). The quality of the evidence was rated down for. indirectness based on relative effects derived primarily. from surgical patients (only 555 of the. 26,890 patients included in PEP trial report metaanalysis. were high-risk medical patients, and all PEP. trials participants were orthopedic surgery patients). The panel judged that based on the low quality of. available evidence pertaining to use of ASA to prevent. VTE in hospitalized medical patients, no recommendation. could be made. There have been no. studies of antiplatelet therapy compared with antithrombotic. therapy to prevent VTE in acutely ill. medical patients Screening for DVT in Hospitalized Medical Patients. Ultrasound screening in medical patients has not. been systematically studied. Indirect evidence from. hospitalized orthopedic patients 59 and spinal cord. injury patients 60 suggests that routine screening is not. of benefi t to reduce symptomatic VTE events. For. example, in a population of patients who had joint. arthroplasty and were receiving warfarin prophylaxis, screening compression ultrasonography with subsequent. treatment of identifi ed asymptomatic DVT. did not reduce the rate of subsequent symptomatic. VTE. 59 In a population with a low prevalence of DVT, such as medical patients, even with a highly-specifi c. test such as ultrasound, one would anticipate a substantial. number of false-positive results. Moreover, even without considering false-positive results, routine. ultrasound screening would be associated with. appreciable cost and inconvenience without evidence. of benefi t Screening for DVT. in Hospitalized Medical Patients Gaps in Care. Low rates of adherence to recommended thromboprophylaxis. regimens have been documented worldwide. 31,61-64 In the last few years, research efforts have. focused on evaluating strategies to improve uptake of. evidence-based VTE prophylaxis regimens in hospitalized. patients, including medical patients. Results.")
53
N Engl J Med Nov 22;367(21): Low-dose aspirin for preventing recurrent venous thromboembolism. Brighton TA, Eikelboom JW, Mann K, Mister R, Gallus A, Ockelford P, Gibbs H, Hague W, Xavier D, Diaz R, Kirby A, Simes J; ASPIRE Investigators. The following toggler user interface control may not be accessible. Tab to the next button to revert the control to an accessible version. Department of Haematology, South Eastern Area Laboratory Services (SEALS), Prince of Wales Hospital, Sydney, Australia. Abstract BACKGROUND: Patients who have had a first episode of unprovoked venous thromboembolism have a high risk of recurrence after anticoagulants are discontinued. Aspirin may be effective in preventing a recurrence of venous thromboembolism. METHODS: We randomly assigned 822 patients who had completed initial anticoagulant therapy after a first episode of unprovoked venous thromboembolism to receive aspirin, at a dose of 100 mg daily, or placebo for up to 4 years. The primary outcome was a recurrence of venous thromboembolism. RESULTS: During a median follow-up period of 37.2 months, venous thromboembolism recurred in 73 of 411 patients assigned to placebo and in 57 of 411 assigned to aspirin (a rate of 6.5% per year vs. 4.8% per year; hazard ratio with aspirin, 0.74; 95% confidence interval [CI], 0.52 to 1.05; P=0.09). Aspirin reduced the rate of the two prespecified secondary composite outcomes: the rate of venous thromboembolism, myocardial infarction, stroke, or cardiovascular death was reduced by 34% (a rate of 8.0% per year with placebo vs. 5.2% per year with aspirin; hazard ratio with aspirin, 0.66; 95% CI, 0.48 to 0.92; P=0.01), and the rate of venous thromboembolism, myocardial infarction, stroke, major bleeding, or death from any cause was reduced by 33% (hazard ratio, 0.67; 95% CI, 0.49 to 0.91; P=0.01). There was no significant between-group difference in the rates of major or clinically relevant nonmajor bleeding episodes (rate of 0.6% per year with placebo vs. 1.1% per year with aspirin, P=0.22) or serious adverse events. CONCLUSIONS: In this study, aspirin, as compared with placebo, did not significantly reduce the rate of recurrence of venous thromboembolism but resulted in a significant reduction in the rate of major vascular events, with improved net clinical benefit. These results substantiate earlier evidence of a therapeutic benefit of aspirin when it is given to patients after initial anticoagulant therapy for a first episode of unprovoked venous thromboembolism N Engl J Med Nov 22;367(21): doi: /NEJMoa Epub 2012 Nov 4. Low-dose aspirin for preventing recurrent venous thromboembolism. Brighton TA, Eikelboom JW, Mann K, Mister R, Gallus A, Ockelford P, Gibbs H, Hague W, Xavier D, Diaz R, Kirby A, Simes J; ASPIRE Investigators. The following toggler user interface control may not be accessible. Tab to the next button to revert the control to an accessible version. Destroy user interface controlCollaborators (147) Brighton T, Eikelboom J, Hague W, Kirby A, Mister R, Simes J, Gallus A, Ockelford P, Baker R, Gibbs H, Coughlin P, Xavier D, Diaz R, Agnelli G, Gibbs H, Karplus T, Fletcher J, van Rij A, Rogers A, Hayward C, Young G, Crispin P, Slade J, Ward C, Tadayon N, Koutts J, Fisher L, Brighton T, McCardie K, Bianchi A, Trinh J, Joseph J, Plenge P, Chong B, Davidson S, Waites J, Cahill P, Tiley C, Lacey M, Jackson D, Boys J, Seldon M, Gambrill M, Nandurkar H, Worland H, Salem H, Gollogly C, Campbell P, Marshall I, Hamilton K, Goss C, Salem H, Poulton L, Jackson M, de Man T, Gan E, Cummins A, Leyden M, Sturtz C, Kubler P, Sansome X, McCann A, Downey C, Carroll P, Duroux M, Hamwood S, Styles G, Buckmaster N, Schmidt T, Colquhoun D, Jardim A, Gallus A, Osmond J, Jeffries W, Trezona B, McRae S, King D, Baker R, Courtley K, Kimber R, Oliver L, MacDonald A, Shepherd J, Ockelford P, Hulton M, Royle G, Haycock L, Simpson D, Yap K, Baker B, McQuilkin H, Carter J, Body J, Heng LL, Tan M, Tay JC, Zou J, Pandharpurkar HK, G R, Stephen E, Benjamin A, Desai SC, Singh R, Suresh KR, R GK, Natarajan S, Goel D, Gupta R, Mishra BS, Sidhu G, Sidhu RS, Parakh R, Sharma R, Joshi S, Mahajan M, Grover T, Sharma K, Patel P, Kothurkar A, Ranade P, Fedele JL, Cristófaro AC, Gelersztein E, Gelersztein M, Sánchez AS, Bowen LC, Durán RO, Cámpora F, Ferro HH, Casais MV, Mister R, Kirby A, Mann K, Van Holst Pellekaan C, Chinchen S, Lucas A, Hague W, Simes J, Xavier D, Pais P, Sigamani A, Mathur N, M A, B DK, Diaz R, Chacon C, Rucci R. Source Department of Haematology, South Eastern Area Laboratory Services (SEALS), Prince of Wales Hospital, Sydney, Australia. Abstract BACKGROUND: Patients who have had a first episode of unprovoked venous thromboembolism have a high risk of recurrence after anticoagulants are discontinued. Aspirin may be effective in preventing a recurrence of venous thromboembolism. METHODS: We randomly assigned 822 patients who had completed initial anticoagulant therapy after a first episode of unprovoked venous thromboembolism to receive aspirin, at a dose of 100 mg daily, or placebo for up to 4 years. The primary outcome was a recurrence of venous thromboembolism. RESULTS: During a median follow-up period of 37.2 months, venous thromboembolism recurred in 73 of 411 patients assigned to placebo and in 57 of 411 assigned to aspirin (a rate of 6.5% per year vs. 4.8% per year; hazard ratio with aspirin, 0.74; 95% confidence interval [CI], 0.52 to 1.05; P=0.09). Aspirin reduced the rate of the two prespecified secondary composite outcomes: the rate of venous thromboembolism, myocardial infarction, stroke, or cardiovascular death was reduced by 34% (a rate of 8.0% per year with placebo vs. 5.2% per year with aspirin; hazard ratio with aspirin, 0.66; 95% CI, 0.48 to 0.92; P=0.01), and the rate of venous thromboembolism, myocardial infarction, stroke, major bleeding, or death from any cause was reduced by 33% (hazard ratio, 0.67; 95% CI, 0.49 to 0.91; P=0.01). There was no significant between-group difference in the rates of major or clinically relevant nonmajor bleeding episodes (rate of 0.6% per year with placebo vs. 1.1% per year with aspirin, P=0.22) or serious adverse events. CONCLUSIONS: In this study, aspirin, as compared with placebo, did not significantly reduce the rate of recurrence of venous thromboembolism but resulted in a significant reduction in the rate of major vascular events, with improved net clinical benefit. These results substantiate earlier evidence of a therapeutic benefit of aspirin when it is given to patients after initial anticoagulant therapy for a first episode of unprovoked venous thromboembolism
, Prince of Wales Hospital, Sydney, Australia. Abstract. BACKGROUND: Patients who have had a first episode of unprovoked venous thromboembolism have a high risk of recurrence after anticoagulants are discontinued. Aspirin may be effective in preventing a recurrence of venous thromboembolism. METHODS: We randomly assigned 822 patients who had completed initial anticoagulant therapy after a first episode of unprovoked venous thromboembolism to receive aspirin, at a dose of 100 mg daily, or placebo for up to 4 years. The primary outcome was a recurrence of venous thromboembolism. RESULTS: During a median follow-up period of 37.2 months, venous thromboembolism recurred in 73 of 411 patients assigned to placebo and in 57 of 411 assigned to aspirin (a rate of 6.5% per year vs. 4.8% per year; hazard ratio with aspirin, 0.74; 95% confidence interval [CI], 0.52 to 1.05; P=0.09). Aspirin reduced the rate of the two prespecified secondary composite outcomes: the rate of venous thromboembolism, myocardial infarction, stroke, or cardiovascular death was reduced by 34% (a rate of 8.0% per year with placebo vs. 5.2% per year with aspirin; hazard ratio with aspirin, 0.66; 95% CI, 0.48 to 0.92; P=0.01), and the rate of venous thromboembolism, myocardial infarction, stroke, major bleeding, or death from any cause was reduced by 33% (hazard ratio, 0.67; 95% CI, 0.49 to 0.91; P=0.01). There was no significant between-group difference in the rates of major or clinically relevant nonmajor bleeding episodes (rate of 0.6% per year with placebo vs. 1.1% per year with aspirin, P=0.22) or serious adverse events. CONCLUSIONS: In this study, aspirin, as compared with placebo, did not significantly reduce the rate of recurrence of venous thromboembolism but resulted in a significant reduction in the rate of major vascular events, with improved net clinical benefit. These results substantiate earlier evidence of a therapeutic benefit of aspirin when it is given to patients after initial anticoagulant therapy for a first episode of unprovoked venous thromboembolism. N Engl J Med Nov 22;367(21): doi: /NEJMoa Epub 2012 Nov 4. Low-dose aspirin for preventing recurrent venous thromboembolism. Brighton TA, Eikelboom JW, Mann K, Mister R, Gallus A, Ockelford P, Gibbs H, Hague W, Xavier D, Diaz R, Kirby A, Simes J; ASPIRE Investigators. The following toggler user interface control may not be accessible. Tab to the next button to revert the control to an accessible version. Destroy user interface controlCollaborators (147) Brighton T, Eikelboom J, Hague W, Kirby A, Mister R, Simes J, Gallus A, Ockelford P, Baker R, Gibbs H, Coughlin P, Xavier D, Diaz R, Agnelli G, Gibbs H, Karplus T, Fletcher J, van Rij A, Rogers A, Hayward C, Young G, Crispin P, Slade J, Ward C, Tadayon N, Koutts J, Fisher L, Brighton T, McCardie K, Bianchi A, Trinh J, Joseph J, Plenge P, Chong B, Davidson S, Waites J, Cahill P, Tiley C, Lacey M, Jackson D, Boys J, Seldon M, Gambrill M, Nandurkar H, Worland H, Salem H, Gollogly C, Campbell P, Marshall I, Hamilton K, Goss C, Salem H, Poulton L, Jackson M, de Man T, Gan E, Cummins A, Leyden M, Sturtz C, Kubler P, Sansome X, McCann A, Downey C, Carroll P, Duroux M, Hamwood S, Styles G, Buckmaster N, Schmidt T, Colquhoun D, Jardim A, Gallus A, Osmond J, Jeffries W, Trezona B, McRae S, King D, Baker R, Courtley K, Kimber R, Oliver L, MacDonald A, Shepherd J, Ockelford P, Hulton M, Royle G, Haycock L, Simpson D, Yap K, Baker B, McQuilkin H, Carter J, Body J, Heng LL, Tan M, Tay JC, Zou J, Pandharpurkar HK, G R, Stephen E, Benjamin A, Desai SC, Singh R, Suresh KR, R GK, Natarajan S, Goel D, Gupta R, Mishra BS, Sidhu G, Sidhu RS, Parakh R, Sharma R, Joshi S, Mahajan M, Grover T, Sharma K, Patel P, Kothurkar A, Ranade P, Fedele JL, Cristófaro AC, Gelersztein E, Gelersztein M, Sánchez AS, Bowen LC, Durán RO, Cámpora F, Ferro HH, Casais MV, Mister R, Kirby A, Mann K, Van Holst Pellekaan C, Chinchen S, Lucas A, Hague W, Simes J, Xavier D, Pais P, Sigamani A, Mathur N, M A, B DK, Diaz R, Chacon C, Rucci R. Source. Department of Haematology, South Eastern Area Laboratory Services (SEALS), Prince of Wales Hospital, Sydney, Australia. Abstract. BACKGROUND: Patients who have had a first episode of unprovoked venous thromboembolism have a high risk of recurrence after anticoagulants are discontinued. Aspirin may be effective in preventing a recurrence of venous thromboembolism. METHODS: We randomly assigned 822 patients who had completed initial anticoagulant therapy after a first episode of unprovoked venous thromboembolism to receive aspirin, at a dose of 100 mg daily, or placebo for up to 4 years. The primary outcome was a recurrence of venous thromboembolism. RESULTS: During a median follow-up period of 37.2 months, venous thromboembolism recurred in 73 of 411 patients assigned to placebo and in 57 of 411 assigned to aspirin (a rate of 6.5% per year vs. 4.8% per year; hazard ratio with aspirin, 0.74; 95% confidence interval [CI], 0.52 to 1.05; P=0.09). Aspirin reduced the rate of the two prespecified secondary composite outcomes: the rate of venous thromboembolism, myocardial infarction, stroke, or cardiovascular death was reduced by 34% (a rate of 8.0% per year with placebo vs. 5.2% per year with aspirin; hazard ratio with aspirin, 0.66; 95% CI, 0.48 to 0.92; P=0.01), and the rate of venous thromboembolism, myocardial infarction, stroke, major bleeding, or death from any cause was reduced by 33% (hazard ratio, 0.67; 95% CI, 0.49 to 0.91; P=0.01). There was no significant between-group difference in the rates of major or clinically relevant nonmajor bleeding episodes (rate of 0.6% per year with placebo vs. 1.1% per year with aspirin, P=0.22) or serious adverse events. CONCLUSIONS: In this study, aspirin, as compared with placebo, did not significantly reduce the rate of recurrence of venous thromboembolism but resulted in a significant reduction in the rate of major vascular events, with improved net clinical benefit. These results substantiate earlier evidence of a therapeutic benefit of aspirin when it is given to patients after initial anticoagulant therapy for a first episode of unprovoked venous thromboembolism.")
54
N Engl J Med. 2012 May 24;366(21):1959-67. doi: 10.1056/NEJMoa1114238.
Aspirin for preventing the recurrence of venous thromboembolism. Becattini C, Agnelli G, Schenone A, Eichinger S, Bucherini E, Silingardi M, Bianchi M, Moia M, Ageno W, Vandelli MR, Grandone E, Prandoni P; WARFASA Investigators. Division of Internal and Cardiovascular Medicine and Stroke Unit, Department of Internal Medicine, University of Perugia, Perugia, Italy. Erratum in N Engl J Med Oct 18;367(16):1573. Abstract BACKGROUND: About 20% of patients with unprovoked venous thromboembolism have a recurrence within 2 years after the withdrawal of oral anticoagulant therapy. Extending anticoagulation prevents recurrences but is associated with increased bleeding. The benefit of aspirin for the prevention of recurrent venous thromboembolism is unknown. METHODS: In this multicenter, investigator-initiated, double-blind study, patients with first-ever unprovoked venous thromboembolism who had completed 6 to 18 months of oral anticoagulant treatment were randomly assigned to aspirin, 100 mg daily, or placebo for 2 years, with the option of extending the study treatment. The primary efficacy outcome was recurrence of venous thromboembolism, and major bleeding was the primary safety outcome. RESULTS: Venous thromboembolism recurred in 28 of the 205 patients who received aspirin and in 43 of the 197 patients who received placebo (6.6% vs. 11.2% per year; hazard ratio, 0.58; 95% confidence interval [CI], 0.36 to 0.93) (median study period, 24.6 months). During a median treatment period of 23.9 months, 23 patients taking aspirin and 39 taking placebo had a recurrence (5.9% vs. 11.0% per year; hazard ratio, 0.55; 95% CI, 0.33 to 0.92). One patient in each treatment group had a major bleeding episode. Adverse events were similar in the two groups. CONCLUSIONS: Aspirin reduced the risk of recurrence when given to patients with unprovoked venous thromboembolism who had discontinued anticoagulant treatment, with no apparent increase in the risk of major bleeding. (Funded by the University of Perugia and others; WARFASA N Engl J Med May 24;366(21): doi: /NEJMoa Aspirin for preventing the recurrence of venous thromboembolism. Becattini C, Agnelli G, Schenone A, Eichinger S, Bucherini E, Silingardi M, Bianchi M, Moia M, Ageno W, Vandelli MR, Grandone E, Prandoni P; WARFASA Investigators. The following toggler user interface control may not be accessible. Tab to the next button to revert the control to an accessible version. Destroy user interface controlCollaborators (56) Agnelli G, Becattini C, Prandoni P, Becattini C, Agnelli G, Prandoni P, Ageno W, Cimminiello C, Eichinger S, Duranti M, Radicchia S, Guercini F, Vedovati MC, Tormene D, Perlati M, Barbar S, Poggio R, Leischer L, Bucherini E, Galimberti D, Leone MF, Beretta A, Carugati A, Braham S, Romualdi E, Tiscia G, Colaizzo D, Grilli M, Siragusa S, Salvi R, Miccio M, Ria L, Zanatta N, Poli D, Camporese G, Verlato F, Salvi A, Nitti C, Santi R, Cimminiello C, Scannapieco G, Barillari G, Pasca S, De Gaudenzi E, Cappelli R, Di Minno G, Tufano A, Frausini G, Bova C, Pogliani E, Signorelli SS, Testa S, Alatri A, Mancuso G, Grifoni S, Lodigiani C. Source Division of Internal and Cardiovascular Medicine and Stroke Unit, Department of Internal Medicine, University of Perugia, Perugia, Italy. Erratum in N Engl J Med Oct 18;367(16):1573. Abstract BACKGROUND: About 20% of patients with unprovoked venous thromboembolism have a recurrence within 2 years after the withdrawal of oral anticoagulant therapy. Extending anticoagulation prevents recurrences but is associated with increased bleeding. The benefit of aspirin for the prevention of recurrent venous thromboembolism is unknown. METHODS: In this multicenter, investigator-initiated, double-blind study, patients with first-ever unprovoked venous thromboembolism who had completed 6 to 18 months of oral anticoagulant treatment were randomly assigned to aspirin, 100 mg daily, or placebo for 2 years, with the option of extending the study treatment. The primary efficacy outcome was recurrence of venous thromboembolism, and major bleeding was the primary safety outcome. RESULTS: Venous thromboembolism recurred in 28 of the 205 patients who received aspirin and in 43 of the 197 patients who received placebo (6.6% vs. 11.2% per year; hazard ratio, 0.58; 95% confidence interval [CI], 0.36 to 0.93) (median study period, 24.6 months). During a median treatment period of 23.9 months, 23 patients taking aspirin and 39 taking placebo had a recurrence (5.9% vs. 11.0% per year; hazard ratio, 0.55; 95% CI, 0.33 to 0.92). One patient in each treatment group had a major bleeding episode. Adverse events were similar in the two groups. CONCLUSIONS: Aspirin reduced the risk of recurrence when given to patients with unprovoked venous thromboembolism who had discontinued anticoagulant treatment, with no apparent increase in the risk of major bleeding. (Funded by the University of Perugia and others; WARFASA To the Editor: In their report on the Aspirin to Prevent Recurrent Venous Thromboembolism (ASPIRE) trial, Brighton et al. (Nov. 22 issue)1 describe a nonsignificant decrease in the rate of recurrent venous thromboembolism and a significant reduction in the rate of major vascular events in patients receiving low-dose aspirin, as compared with those receiving placebo. These findings are similar to those of Becattini et al. (May 24 issue)2 in their report on the Aspirin for the Prevention of Recurrent Venous Thromboembolism (the Warfarin and Aspirin [WARFASA])2 study. However, the biologic effects of aspirin could in part be sex-dependent. Women seem to have a higher baseline level of platelet reactivity than men,3 but the effect of low-dose aspirin on arachidonic acid–induced aggregation is greater in women.3 In addition, women have been found to have higher circulating levels of acetylsalicylic acid, because of its slower clearance.4 Possible sex differences were further suggested by a meta-analysis showing that the use of aspirin was associated with a reduced rate of myocardial infarction with no effect on stroke among men and a reduced rate of stroke with no effect on myocardial infarction among women.5 Data from the ASPIRE and WARFASA trials, and particularly pooled data with hazard ratios, regarding the effect of aspirin on venous and arterial cardiovascular events according to sex would be useful clinical information. Viktor Čulić, M.D., Ph.D. University Hospital Center Split, Split, Croatia No potential conflict of interest relevant to this letter was reported. 5 References 1 Brighton TA, Eikelboom JW, Mann K, et al. Low-dose aspirin for preventing recurrent venous thromboembolism. N Engl J Med 2012;367: Full Text | Medline 2 Becattini C, Agnelli G, Schenone A, et al. Aspirin for preventing the recurrence of venous thromboembolism. N Engl J Med 2012;366: [Erratum, N Engl J Med 2012;367:1573.] Free Full Text | Web of Science | Medline 3 Becker DM, Segal J, Vaidya D, et al. Sex differences in platelet reactivity and response to low-dose aspirin therapy. JAMA 2006;295: CrossRef | Medline 4 Jochmann N, Stangl K, Garbe E, Baumann G, Stangl V. Female-specific aspects in the pharmacotherapy of chronic cardiovascular diseases. Eur Heart J 2005;26: CrossRef | Medline 5 Berger JS, Roncaglioni MC, Avanzini F, Pangrazzi I, Tognoni G, Brown DL. Aspirin for the primary prevention of cardiovascular events in women and men: a sex-specific meta-analysis of randomized controlled trials. JAMA 2006;295: [Erratum, JAMA 2006;295:2002.] CrossRef | Medline Brighton et al. report that aspirin, as compared with placebo, did not significantly reduce the rate of venous thromboembolism in patients who had completed initial anticoagulant therapy. A secondary analysis of the Justification for the Use of Statins in Primary Prevention: an Intervention Trial Evaluating Rosuvastatin (JUPITER)1 showed that treatment with rosuvastatin was associated with a reduction of 43% in the risk of venous thromboembolism, as compared with placebo (hazard ratio for rosuvastatin, 0.57; P=0.007). The efficacy of statins in preventing venous thromboembolism has been supported in some studies2 but not in others.3 A recent study verified that statin use was associated with a reduced risk of venous thromboembolism (hazard ratio, 0.29; P<0.001).4 This study also showed that dual antiplatelet therapy with aspirin and clopidogrel decreased the occurrence of venous thromboembolism (hazard ratio, 0.19; P<0.001). The combined use of statins and antiplatelet therapy further reduced the occurrence of venous thromboembolism (hazard ratio, 0.16; P<0.001).4 It would be interesting to know whether Brighton et al. recorded statin use in their population and whether their results would be affected after adjustment for statin use. Kosmas I. Paraskevas, M.D. 24 Alexander Papagou St., Athens, Greece No potential conflict of interest relevant to this letter was reported Glynn RJ, Danielson E, Fonseca FA, et al. A randomized trial of rosuvastatin in the prevention of venous thromboembolism. N Engl J Med 2009;360: Free Full Text | Web of Science | Medline Squizzato A, Galli M, Romualdi E, et al. Statins, fibrates, and venous thromboembolism: a meta-analysis. Eur Heart J 2010;31: CrossRef | Medline Rahimi K, Bhala N, Kamphuisen P, et al. Effect of statins on venous thromboembolic events: a meta-analysis of published and unpublished evidence from randomised controlled trials. PLoS Med 2012;9:e e CrossRef | Medline Khemasuwan D, Chae YK, Gupta S, et al. Dose-related effect of statins in venous thrombosis risk reduction. Am J Med 2011;124: CrossRef | Medline Čulić highlights potential differences between men and women with respect to the platelet inhibitory effects and clinical efficacy of aspirin. Our results indicated that the 447 men in our study, as compared with the 375 women, were almost twice as likely to have recurrent venous thromboembolism (8.6% vs. 4.5%). However, the use of aspirin was associated with a similar reduction in relative risk in men and women (P=0.58 for interaction) (see Fig. 3 in the Supplementary Appendix, available with the full text of our article at NEJM.org). Consequently, larger absolute treatment benefits may be expected in men. The reason for higher recurrence rates in men than in women is uncertain. Our planned prospective meta-analysis of the results with respect to individual patients in the ASPIRE and WARFASA trials may provide further insights into the influence of sex on recurrence risk. Paraskevas questions whether statin use may have affected the results of our study. On the basis of many randomized trials, statins clearly reduce the rate of arterial events, but their effects on venous thrombotic events are less certain.1 In our study, 61 patients recorded statin use at enrollment, including 34 of 411 patients (8.3%) who were assigned to receive placebo and 27 of 411 patients (6.6%) who were assigned to receive low-dose aspirin. An analysis of the effect of aspirin on venous thromboembolism after adjustment for initial statin use showed results similar to those in the intention-to-treat analysis (hazard ratio, 0.74; 95% confidence interval, 0.53 to 1.05). Finally, in response to the statement by Paraskevas that our study “showed that aspirin did not reduce the rate of venous thromboembolism”: we reiterate that our study was not powered to show an effect on this outcome. However, when our results are considered in combination with the findings of the WARFASA trial, they are consistent with a reduction of about one third in the rate of recurrent venous thromboembolism after a first episode of venous thromboembolism. Timothy A. Brighton, M.B., B.S. Prince of Wales Hospital, Sydney, NSW, Australia John W. Eikelboom, M.B., B.S. McMaster University, Hamilton, ON, Canada John Simes, M.D. National Health and Medical Research Council Clinical Trials Centre, Sydney, NSW, Australia
:1573. Abstract. BACKGROUND: About 20% of patients with unprovoked venous thromboembolism have a recurrence within 2 years after the withdrawal of oral anticoagulant therapy. Extending anticoagulation prevents recurrences but is associated with increased bleeding. The benefit of aspirin for the prevention of recurrent venous thromboembolism is unknown. METHODS: In this multicenter, investigator-initiated, double-blind study, patients with first-ever unprovoked venous thromboembolism who had completed 6 to 18 months of oral anticoagulant treatment were randomly assigned to aspirin, 100 mg daily, or placebo for 2 years, with the option of extending the study treatment. The primary efficacy outcome was recurrence of venous thromboembolism, and major bleeding was the primary safety outcome. RESULTS: Venous thromboembolism recurred in 28 of the 205 patients who received aspirin and in 43 of the 197 patients who received placebo (6.6% vs. 11.2% per year; hazard ratio, 0.58; 95% confidence interval [CI], 0.36 to 0.93) (median study period, 24.6 months). During a median treatment period of 23.9 months, 23 patients taking aspirin and 39 taking placebo had a recurrence (5.9% vs. 11.0% per year; hazard ratio, 0.55; 95% CI, 0.33 to 0.92). One patient in each treatment group had a major bleeding episode. Adverse events were similar in the two groups. CONCLUSIONS: Aspirin reduced the risk of recurrence when given to patients with unprovoked venous thromboembolism who had discontinued anticoagulant treatment, with no apparent increase in the risk of major bleeding. (Funded by the University of Perugia and others; WARFASA. N Engl J Med May 24;366(21): doi: /NEJMoa Aspirin for preventing the recurrence of venous thromboembolism. Becattini C, Agnelli G, Schenone A, Eichinger S, Bucherini E, Silingardi M, Bianchi M, Moia M, Ageno W, Vandelli MR, Grandone E, Prandoni P; WARFASA Investigators. The following toggler user interface control may not be accessible. Tab to the next button to revert the control to an accessible version. Destroy user interface controlCollaborators (56) Agnelli G, Becattini C, Prandoni P, Becattini C, Agnelli G, Prandoni P, Ageno W, Cimminiello C, Eichinger S, Duranti M, Radicchia S, Guercini F, Vedovati MC, Tormene D, Perlati M, Barbar S, Poggio R, Leischer L, Bucherini E, Galimberti D, Leone MF, Beretta A, Carugati A, Braham S, Romualdi E, Tiscia G, Colaizzo D, Grilli M, Siragusa S, Salvi R, Miccio M, Ria L, Zanatta N, Poli D, Camporese G, Verlato F, Salvi A, Nitti C, Santi R, Cimminiello C, Scannapieco G, Barillari G, Pasca S, De Gaudenzi E, Cappelli R, Di Minno G, Tufano A, Frausini G, Bova C, Pogliani E, Signorelli SS, Testa S, Alatri A, Mancuso G, Grifoni S, Lodigiani C. Source. Division of Internal and Cardiovascular Medicine and Stroke Unit, Department of Internal Medicine, University of Perugia, Perugia, Italy. Erratum in. N Engl J Med Oct 18;367(16):1573. Abstract. BACKGROUND: About 20% of patients with unprovoked venous thromboembolism have a recurrence within 2 years after the withdrawal of oral anticoagulant therapy. Extending anticoagulation prevents recurrences but is associated with increased bleeding. The benefit of aspirin for the prevention of recurrent venous thromboembolism is unknown. METHODS: In this multicenter, investigator-initiated, double-blind study, patients with first-ever unprovoked venous thromboembolism who had completed 6 to 18 months of oral anticoagulant treatment were randomly assigned to aspirin, 100 mg daily, or placebo for 2 years, with the option of extending the study treatment. The primary efficacy outcome was recurrence of venous thromboembolism, and major bleeding was the primary safety outcome. RESULTS: Venous thromboembolism recurred in 28 of the 205 patients who received aspirin and in 43 of the 197 patients who received placebo (6.6% vs. 11.2% per year; hazard ratio, 0.58; 95% confidence interval [CI], 0.36 to 0.93) (median study period, 24.6 months). During a median treatment period of 23.9 months, 23 patients taking aspirin and 39 taking placebo had a recurrence (5.9% vs. 11.0% per year; hazard ratio, 0.55; 95% CI, 0.33 to 0.92). One patient in each treatment group had a major bleeding episode. Adverse events were similar in the two groups. CONCLUSIONS: Aspirin reduced the risk of recurrence when given to patients with unprovoked venous thromboembolism who had discontinued anticoagulant treatment, with no apparent increase in the risk of major bleeding. (Funded by the University of Perugia and others; WARFASA. To the Editor: In their report on the Aspirin to Prevent Recurrent Venous Thromboembolism (ASPIRE) trial, Brighton et al. (Nov. 22 issue)1 describe a nonsignificant decrease in the rate of recurrent venous thromboembolism and a significant reduction in the rate of major vascular events in patients receiving low-dose aspirin, as compared with those receiving placebo. These findings are similar to those of Becattini et al. (May 24 issue)2 in their report on the Aspirin for the Prevention of Recurrent Venous Thromboembolism (the Warfarin and Aspirin [WARFASA])2 study. However, the biologic effects of aspirin could in part be sex-dependent. Women seem to have a higher baseline level of platelet reactivity than men,3 but the effect of low-dose aspirin on arachidonic acid–induced aggregation is greater in women.3 In addition, women have been found to have higher circulating levels of acetylsalicylic acid, because of its slower clearance.4 Possible sex differences were further suggested by a meta-analysis showing that the use of aspirin was associated with a reduced rate of myocardial infarction with no effect on stroke among men and a reduced rate of stroke with no effect on myocardial infarction among women.5 Data from the ASPIRE and WARFASA trials, and particularly pooled data with hazard ratios, regarding the effect of aspirin on venous and arterial cardiovascular events according to sex would be useful clinical information. Viktor Čulić, M.D., Ph.D. University Hospital Center Split, Split, Croatia No potential conflict of interest relevant to this letter was reported. 5 References 1. Brighton TA, Eikelboom JW, Mann K, et al. Low-dose aspirin for preventing recurrent venous thromboembolism. N Engl J Med 2012;367: Full Text | Medline. 2. Becattini C, Agnelli G, Schenone A, et al. Aspirin for preventing the recurrence of venous thromboembolism. N Engl J Med 2012;366: [Erratum, N Engl J Med 2012;367:1573.] Free Full Text | Web of Science | Medline. 3. Becker DM, Segal J, Vaidya D, et al. Sex differences in platelet reactivity and response to low-dose aspirin therapy. JAMA 2006;295: CrossRef | Medline. 4. Jochmann N, Stangl K, Garbe E, Baumann G, Stangl V. Female-specific aspects in the pharmacotherapy of chronic cardiovascular diseases. Eur Heart J 2005;26: CrossRef | Medline. 5. Berger JS, Roncaglioni MC, Avanzini F, Pangrazzi I, Tognoni G, Brown DL. Aspirin for the primary prevention of cardiovascular events in women and men: a sex-specific meta-analysis of randomized controlled trials. JAMA 2006;295: [Erratum, JAMA 2006;295:2002.] CrossRef | Medline. Brighton et al. report that aspirin, as compared with placebo, did not significantly reduce the rate of venous thromboembolism in patients who had completed initial anticoagulant therapy. A secondary analysis of the Justification for the Use of Statins in Primary Prevention: an Intervention Trial Evaluating Rosuvastatin (JUPITER)1 showed that treatment with rosuvastatin was associated with a reduction of 43% in the risk of venous thromboembolism, as compared with placebo (hazard ratio for rosuvastatin, 0.57; P=0.007). The efficacy of statins in preventing venous thromboembolism has been supported in some studies2 but not in others.3. A recent study verified that statin use was associated with a reduced risk of venous thromboembolism (hazard ratio, 0.29; P<0.001).4 This study also showed that dual antiplatelet therapy with aspirin and clopidogrel decreased the occurrence of venous thromboembolism (hazard ratio, 0.19; P<0.001). The combined use of statins and antiplatelet therapy further reduced the occurrence of venous thromboembolism (hazard ratio, 0.16; P<0.001).4 It would be interesting to know whether Brighton et al. recorded statin use in their population and whether their results would be affected after adjustment for statin use. Kosmas I. Paraskevas, M.D. 24 Alexander Papagou St., Athens, Greece No potential conflict of interest relevant to this letter was reported. Glynn RJ, Danielson E, Fonseca FA, et al. A randomized trial of rosuvastatin in the prevention of venous thromboembolism. N Engl J Med 2009;360: Free Full Text | Web of Science | Medline. Squizzato A, Galli M, Romualdi E, et al. Statins, fibrates, and venous thromboembolism: a meta-analysis. Eur Heart J 2010;31: CrossRef | Medline. Rahimi K, Bhala N, Kamphuisen P, et al. Effect of statins on venous thromboembolic events: a meta-analysis of published and unpublished evidence from randomised controlled trials. PLoS Med 2012;9:e e CrossRef | Medline. Khemasuwan D, Chae YK, Gupta S, et al. Dose-related effect of statins in venous thrombosis risk reduction. Am J Med 2011;124: CrossRef | Medline. Čulić highlights potential differences between men and women with respect to the platelet inhibitory effects and clinical efficacy of aspirin. Our results indicated that the 447 men in our study, as compared with the 375 women, were almost twice as likely to have recurrent venous thromboembolism (8.6% vs. 4.5%). However, the use of aspirin was associated with a similar reduction in relative risk in men and women (P=0.58 for interaction) (see Fig. 3 in the Supplementary Appendix, available with the full text of our article at NEJM.org). Consequently, larger absolute treatment benefits may be expected in men. The reason for higher recurrence rates in men than in women is uncertain. Our planned prospective meta-analysis of the results with respect to individual patients in the ASPIRE and WARFASA trials may provide further insights into the influence of sex on recurrence risk. Paraskevas questions whether statin use may have affected the results of our study. On the basis of many randomized trials, statins clearly reduce the rate of arterial events, but their effects on venous thrombotic events are less certain.1 In our study, 61 patients recorded statin use at enrollment, including 34 of 411 patients (8.3%) who were assigned to receive placebo and 27 of 411 patients (6.6%) who were assigned to receive low-dose aspirin. An analysis of the effect of aspirin on venous thromboembolism after adjustment for initial statin use showed results similar to those in the intention-to-treat analysis (hazard ratio, 0.74; 95% confidence interval, 0.53 to 1.05). Finally, in response to the statement by Paraskevas that our study showed that aspirin did not reduce the rate of venous thromboembolism : we reiterate that our study was not powered to show an effect on this outcome. However, when our results are considered in combination with the findings of the WARFASA trial, they are consistent with a reduction of about one third in the rate of recurrent venous thromboembolism after a first episode of venous thromboembolism. Timothy A. Brighton, M.B., B.S. Prince of Wales Hospital, Sydney, NSW, Australia John W. Eikelboom, M.B., B.S. McMaster University, Hamilton, ON, Canada. John Simes, M.D. National Health and Medical Research Council Clinical Trials Centre, Sydney, NSW, Australia.")
56
NACO vs HBPM Drugs. 2012 Sep 10;72(13):1755-64.
Prevention of venous thromboembolism with new oral anticoagulants versus standard pharmacological treatment in acute medically ill patients: a systematic review and meta-analysis.Albertsen IE, Larsen TB, Rasmussen LH, Overvad TF, Lip GY. NTRODUCTION: Venous thromboembolism (VTE) is a common and potentially avoidable cause of morbidity and mortality in patients hospitalized for acute medical illness. OBJECTIVE: Our objective was to conduct a systematic review of studies that assessed the efficacy and safety of new oral anticoagulant (OAC) drugs versus standard pharmacological drugs and/or placebo in prevention of VTE in acute medically ill patients. RESULTS: Compared with subjects treated with enoxaparin followed by placebo, the RR of the primary outcome during the prolonged treatment period was 0.79 (95% CI 0.66, 0.94), the RR for the primary outcome during the first short-term treatment period was 1.03 (95% CI 0.81, 1.31). For major bleeding during the prolonged treatment period, the RR was 2.69 (95% CI 1.65, 4.39) for patients treated with an FXa inhibitor compared with enoxaparin/placebo. For major bleeding during the shorter treatment period, the RR was 2.01 (95% CI 1.10, 3.65) in favour of enoxaparin. CONCLUSION: In acute medically ill patients, prolonged thromboprophylaxis with an oral FXa inhibitor is more protective than regular short-term treatment with enoxaparin. However, treatment with FXa inhibitors is significantly associated with major bleeding, both in long- and short-term treatment compared with enoxaparin
 is a common and potentially avoidable cause of morbidity and mortality in patients hospitalized for acute medical illness. OBJECTIVE: Our objective was to conduct a systematic review of studies that assessed the efficacy and safety of new oral anticoagulant (OAC) drugs versus standard pharmacological drugs and/or placebo in prevention of VTE in acute medically ill patients. RESULTS: Compared with subjects treated with enoxaparin followed by placebo, the RR of the primary outcome during the prolonged treatment period was 0.79 (95% CI 0.66, 0.94), the RR for the primary outcome during the first short-term treatment period was 1.03 (95% CI 0.81, 1.31). For major bleeding during the prolonged treatment period, the RR was 2.69 (95% CI 1.65, 4.39) for patients treated with an FXa inhibitor compared with enoxaparin/placebo. For major bleeding during the shorter treatment period, the RR was 2.01 (95% CI 1.10, 3.65) in favour of enoxaparin. CONCLUSION: In acute medically ill patients, prolonged thromboprophylaxis with an oral FXa inhibitor is more protective than regular short-term treatment with enoxaparin. However, treatment with FXa inhibitors is significantly associated with major bleeding, both in long- and short-term treatment compared with enoxaparin.")
57
Ultimas guías ACCP Conclusions
Decisions regarding prophylaxis in nonsurgical patients should be made after consideration of risk factors for both thrombosis and bleeding, clinical context, and patients’ values and preferences. CHEST 2012; 141(2)(Suppl):e195S–e226S
(Suppl):e195S–e226S.")
Presentaciones similares
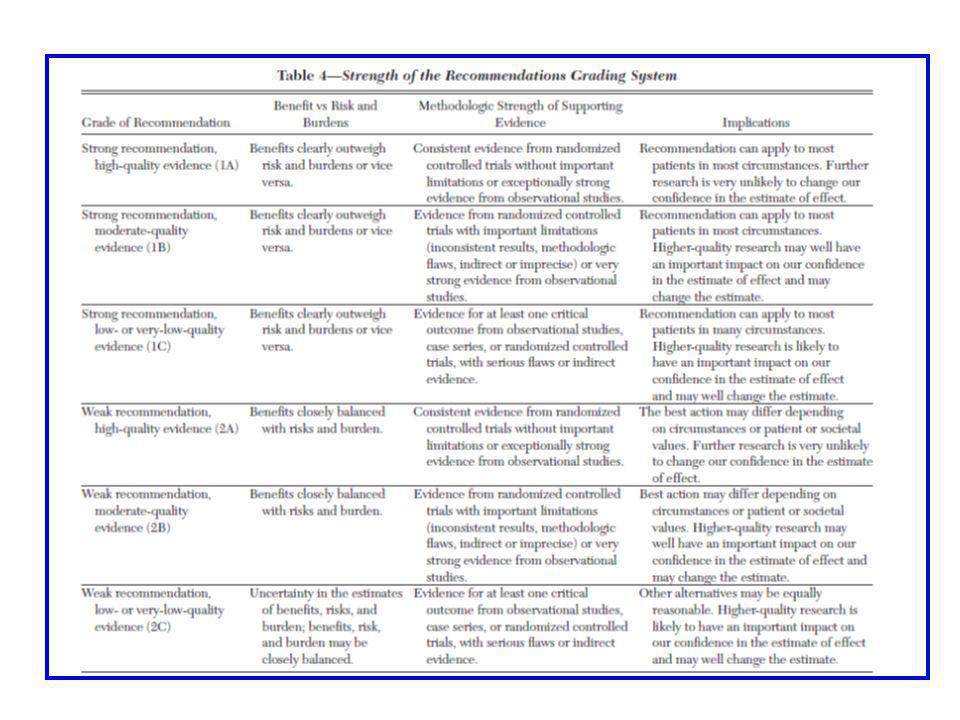
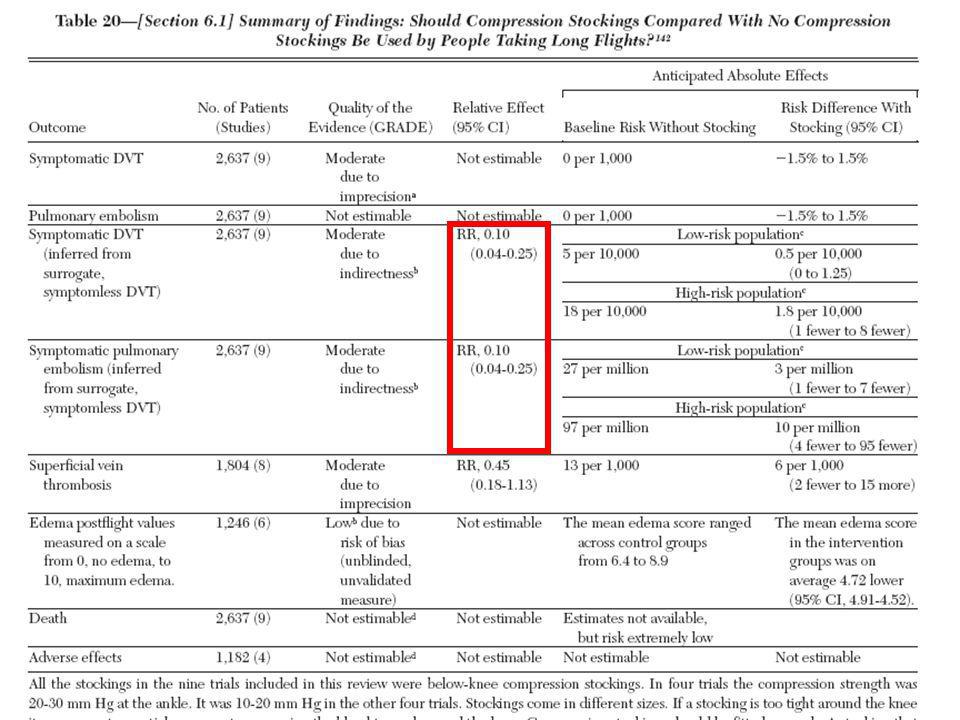

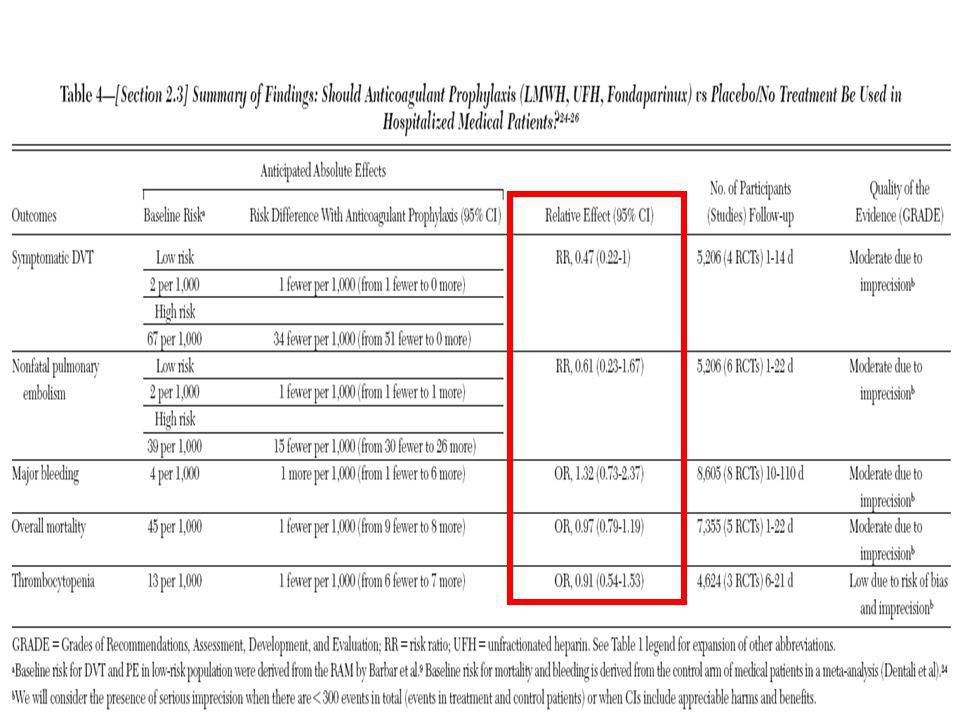
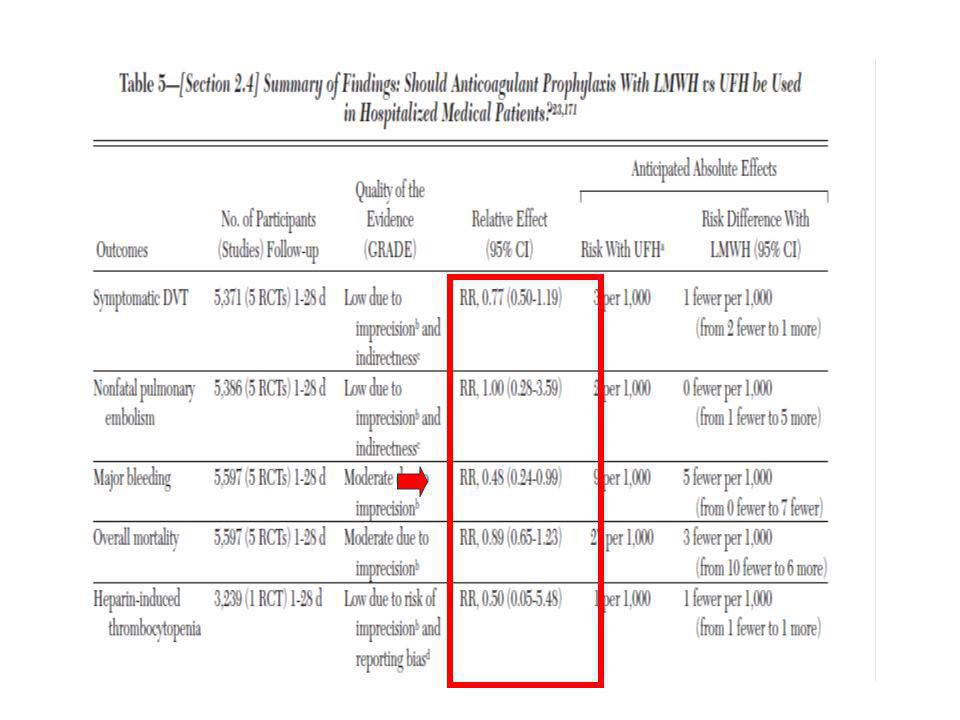
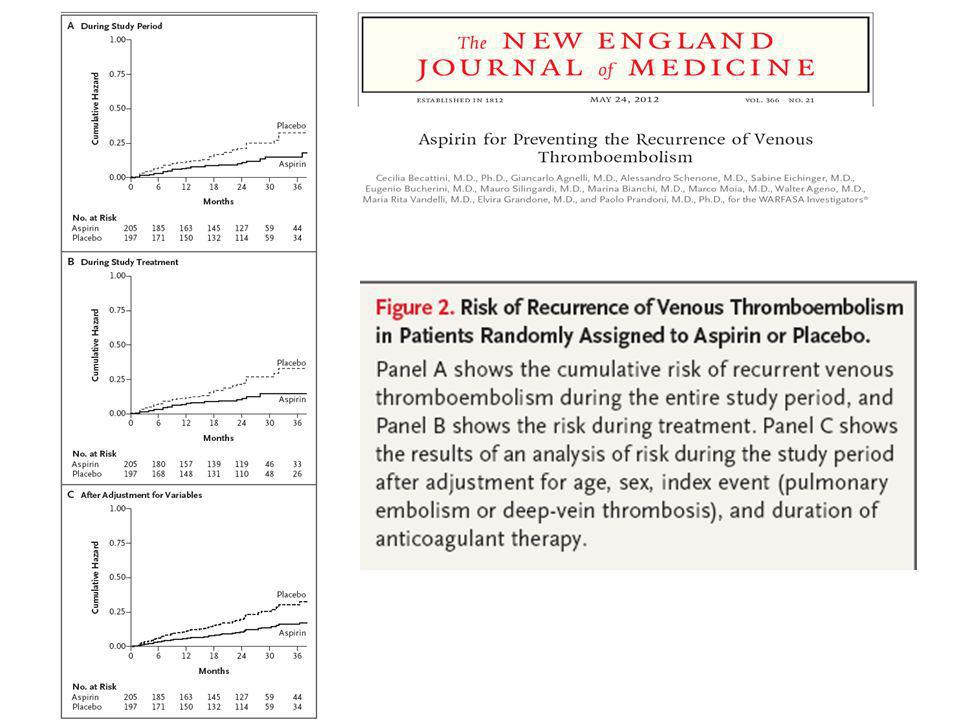
 European Transfer Credit System (ECTS) Methodology in.>")



.>")



 Usted tiene – You have (Formal) El tiene – He has Ella.>")






. It features two verb changes that we will see very soon.>")



