Descargar la presentación
La descarga está en progreso. Por favor, espere

1
Dr Díaz Vargas Trauma Abdomen UCR

2
Trauma de Abdomen CERRADO PENETRANTE

3
OBJETIVOS Enfoque diagnóstico adecuado
Ubicación dentro de un todo en el paciente politraumatizado Conocer el abordaje diagnóstico Conocimiento básico de abordaje terapéutico

4
EXPLORACION FISICA INSPECCION

5
EXPLORACION FISICA PALPACION TRAUMA CERRADO TRAUMA PENETRANTE
(PALPACION PERCUCION) TRAUMA PENETRANTE (EXPLORACION DIGITAL)
 TRAUMA PENETRANTE. (EXPLORACION DIGITAL)")
6
EXPLORACION FISICA AUSCULTACION

7
METODOS DIAGNOSTICOS LAVADO PERITONEAL ULTRASONIDO TAC LAPAROSCOPIA
ARTERIOGRAFIA RESONANCIA MAGNETICA

8
LAVADO PERITONEAL Desventajas Ventajas Sobre sensible
Introduce aire y líquido a cavidad Limita manejo conservador Poco específico Invasivo Ventajas Barato Anestesia local Muy sensible

9
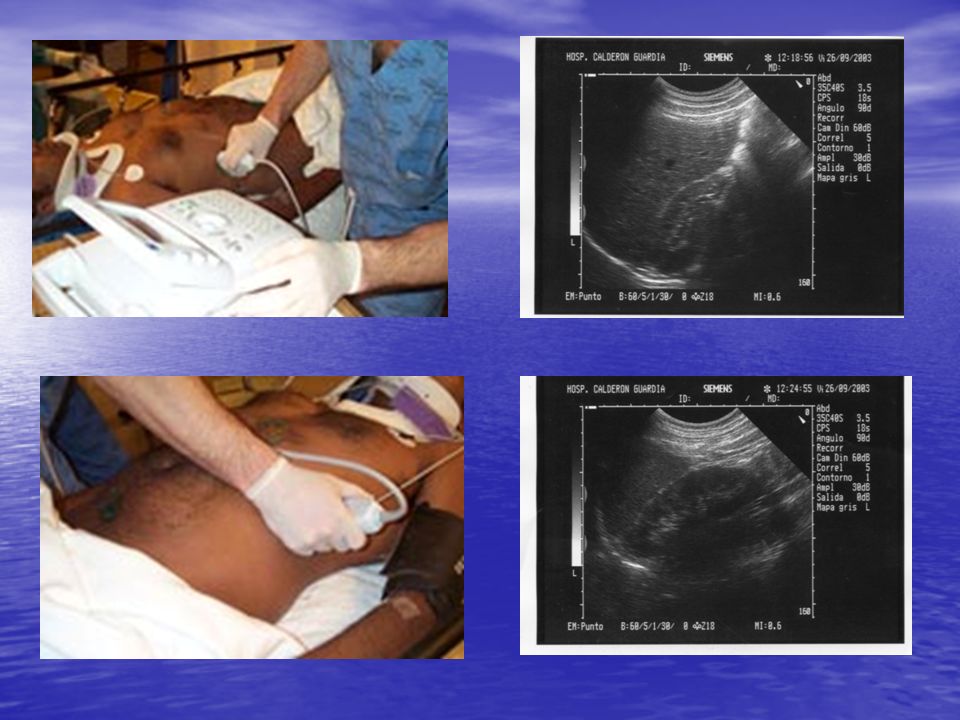
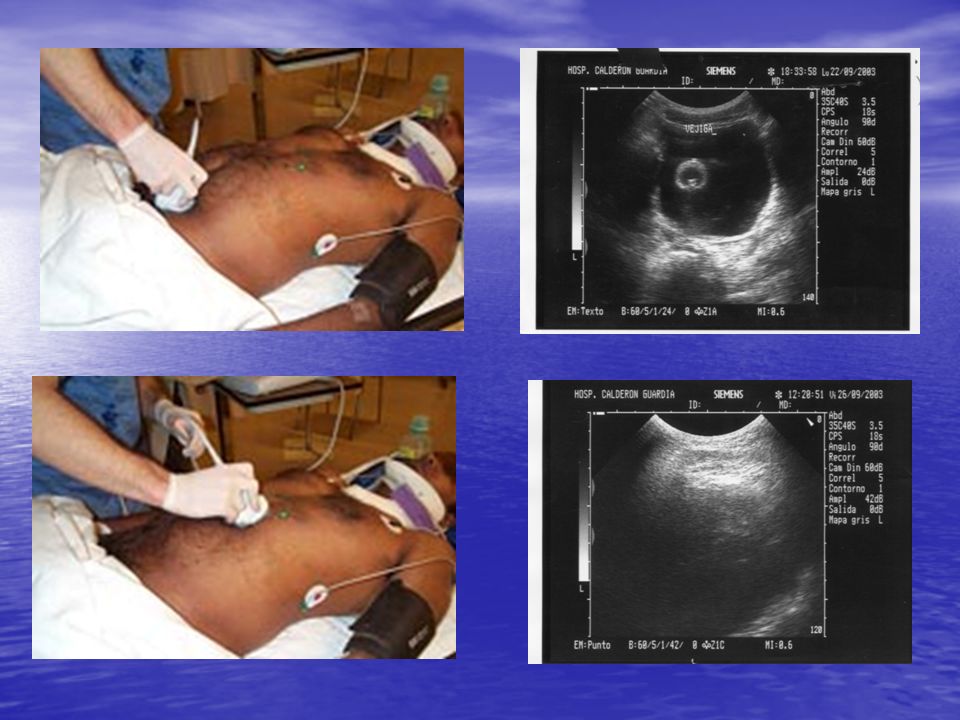
FAST F OCUS A SSESMENT (A BDOMINAL) S ONOGRAPHY IN T RAUMA
 S ONOGRAPHY IN T RAUMA")
12
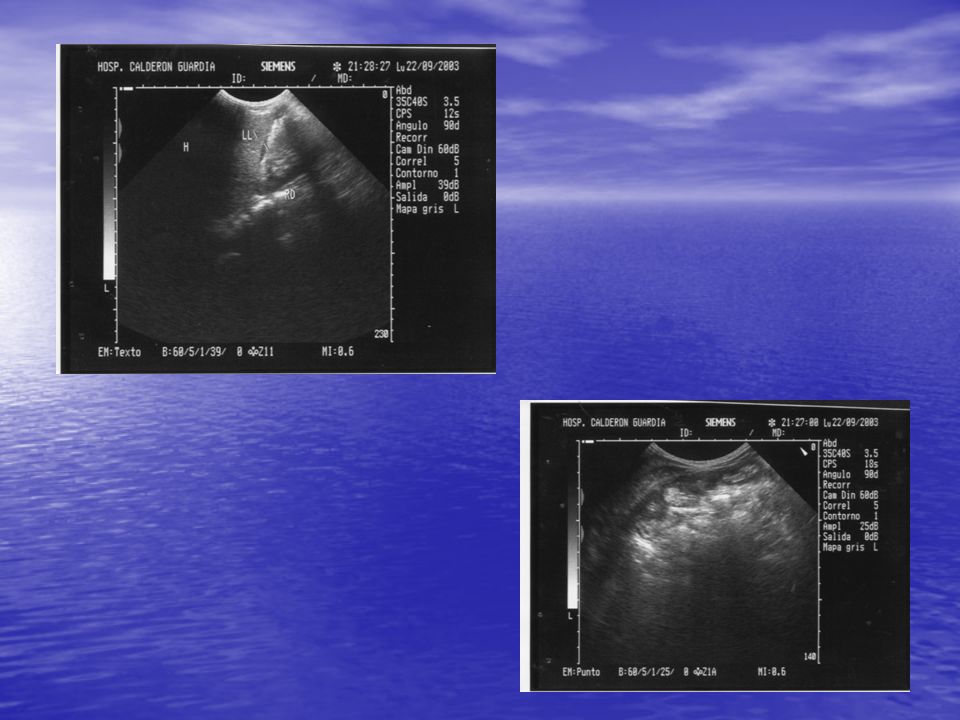
Ultrasonido FAST SANGRE HIGADO RIÑON LIQUIDO LIBRE

13
ULTRASONIDO FAST Ventajas: Desventajas: Rápido Barato Versátil
Sensible Más específico que l.p. Puede ser repetido con frecuencia Puede ser realizado por no radiólogos Desventajas: Operador dependiente No es específico

15
…sin palabras

16
TAC

18
TAC DESVENTAJAS: Consume tiempo VENTAJAS: Sensible Precio Específico
Dificultad de controlar mientras se realiza el estudio Limitación técnica del equipo VENTAJAS: Sensible Específico Permite manejo sin cirugía en pacientes estables Valora retroperitoneo

20
LAPAROSCOPÍA VENTAJAS DESVENTAJAS
Requiere anestesia general y equipo especializado Consume tiempo Eventual peligro de lesiones diafragmáticas Dificil de valorar intestino VENTAJAS Alta sensibilidad Permite terapéutica en algunos casos

21
ALGUNAS ´¨NOVEDADES¨¨... POR EL MOMENTO
METODOS DIAGNOSTICOS CONTROL DE DAÑO S.COMPARTIMENTAL ABDOMINAL ABDOMEN ABIERTO BED SIDE LAPAROTOMY MANEJO NO QUIRURGICO

22
CONTROL DE DAÑO

23
CONTROL DE DAÑO

24
CONTROL DE DAÑO ACIDOSIS HIPOTENSION HIPOTERMIA TRIADA DE LA MUERTE

25
TRIADA DE LA MUERTE HIPOTERMIA COAGULOPATÍA ARRITMIA - PARO CARDIACO

26
CONTROL DE DAÑO I- EN SALA DE OPERACIONES II- EN UCI O RECUPERACIÓN
HEMOSTASIA CONTROL DE CONTAMINACION I- EN SALA DE OPERACIONES CUAGULACION RESTITUCIÓN DE LÍQUIDOS II- EN UCI O RECUPERACIÓN CALENTAMIENTO DEL PACIENTE TX. ACIDOSIS III-EN SALA DE OPERACIONES

29
100% Sugrue M, D'Amours SK, Joshipura M Damage control surgery and the abdomen. Injury (England), Jul 2004, 35(7) p642-8 Rotondo MF, Bard MR Damage control surgery for thoracic injuries. Injury (England), Jul 2004, 35(7) p649-54 Rosenfeld JV Damage control neurosurgery. Injury (England), Jul 2004, 35(7) p655-60 Kossmann T, Trease L, Freedman I, et al. Damage control surgery for spine trauma. Injury (England), Jul 2004, 35(7) p661-70 Henzan E [Damage control in vascular trauma] Nippon Geka Gakkai Zasshi (Japan), Jul 2002, 103(7) p521-3
, Jul 2004, 35(7) p Rotondo MF, Bard MR Damage control surgery for thoracic injuries. Injury (England), Jul 2004, 35(7) p Rosenfeld JV Damage control neurosurgery. Injury (England), Jul 2004, 35(7) p Kossmann T, Trease L, Freedman I, et al. Damage control surgery for spine trauma. Injury (England), Jul 2004, 35(7) p Henzan E [Damage control in vascular trauma] Nippon Geka Gakkai Zasshi (Japan), Jul 2002, 103(7) p")
31
v

33
Damage control surgery for thoracic injuries.
Injury 2004 Jul;35(7):649-54 (ISSN: ) Rotondo MF; Bard MR School of Medicine, East Carolina University, 600 Moye Blvd. Greenville, NC , USA. Damage control of thoracic injuries begins frequently with an emergency department thoracotomy via an anterolateral incision. Bleeding and air leaks are quickly temporised. As opposed to abdominal damage control where most injuries can be temporised, most thoracic injuries require initial definitive repair. Thus, the goal of thoracic damage control is to perform the least definitive repair using the fastest and easiest techniques to shorten the operative time as much as possible. There are some injuries that can be temporised and require re-operation once physiologic normality has been achieved
: (ISSN: ) Rotondo MF; Bard MR School of Medicine, East Carolina University, 600 Moye Blvd. Greenville, NC , USA. Damage control of thoracic injuries begins frequently with an emergency department thoracotomy via an anterolateral incision. Bleeding and air leaks are quickly temporised. As opposed to abdominal damage control where most injuries can be temporised, most thoracic injuries require initial definitive repair. Thus, the goal of thoracic damage control is to perform the least definitive repair using the fastest and easiest techniques to shorten the operative time as much as possible. There are some injuries that can be temporised and require re-operation once physiologic normality has been achieved.")
34
-SINDROME COMPARTIMENTAL ABDOMINAL -HIPERTENSION ABDOMINAL

35
Síndrome Compartmental Abdominal
TERCER ESPACIO EMPAQUE ILEO PARALÍTICO P INTRACRANEAL DIFICULTAD EN EL CIERRE O2 CO2 AUMENTO DE PRESION INTRA ABDOMINAL AUMENTO P. TORACICA DISMINUCIÓN RETORNO VENOSO ISQUEMIA ESPLACNICA ACIDOSIS DISMINUCIÓN GASTO CARDIACO DISMINUYE PRESIÓN DE PERFUSIÓN INSUFICIENCIA RENAL

37
S. COMPARTIMENTAL ABDOMINAL
Clínicamente se caracteriza por: Distensión abdominal Incremento de la presión de inspiración en la vía aérea Aumento de la presión venosa central (PVC) Hipercarbia Hipoxia Oliguria
 Hipercarbia. Hipoxia. Oliguria.")
38
GRADOS DE HIPERTENSIÓN INTRAABDOMINAL.
Presión vesical en cm de agua I 10-15 II 15-25 III 25-35 IV > 35

39
Return to Main Page

40
CAUSAS S. COMPARTIMENTAL ABDOMINAL ·. Espontánea ·
CAUSAS S. COMPARTIMENTAL ABDOMINAL · Espontánea · Peritonitis y absceso intraabdominal · Íleo, obstrucción intestinal · Aneurisma aórtico roto · Neumopritoneo a tensión · Pancreatitis aguda · Trombosis venosa mesentérica · Postoperatoria · Dilatación gástrica aguda · Hemorragia intraperitoneal · Postraumática · Sangrado intraperitoneal/retroperitoneal · Edema visceral posrresucitación · Iatrogénica · Procedimientos laparoscópicos · Vestidos antichoque · Empaquetamiento abdominal · Reducción masiva de hernia parietal o diafragmática · Cierre abdominal a tensión · Crónica · Ascitis · Tumor abdominal de gran tamaño · Diálisis peritoneal ambulatoria · Embarazo

41
S. COMPARTIMENTAL ABDOMINAL
DESCOMPRESION EXPANSIÓN DE VASOS ABDOMINO PELVICOS HIPOVOLEMIA RELATIVA ARRESTO CARDIACO RADICALES LIBRES NETABOLISMO AEROBIO ION H ION K SIND. REPERFUSION HIPOXIA

42
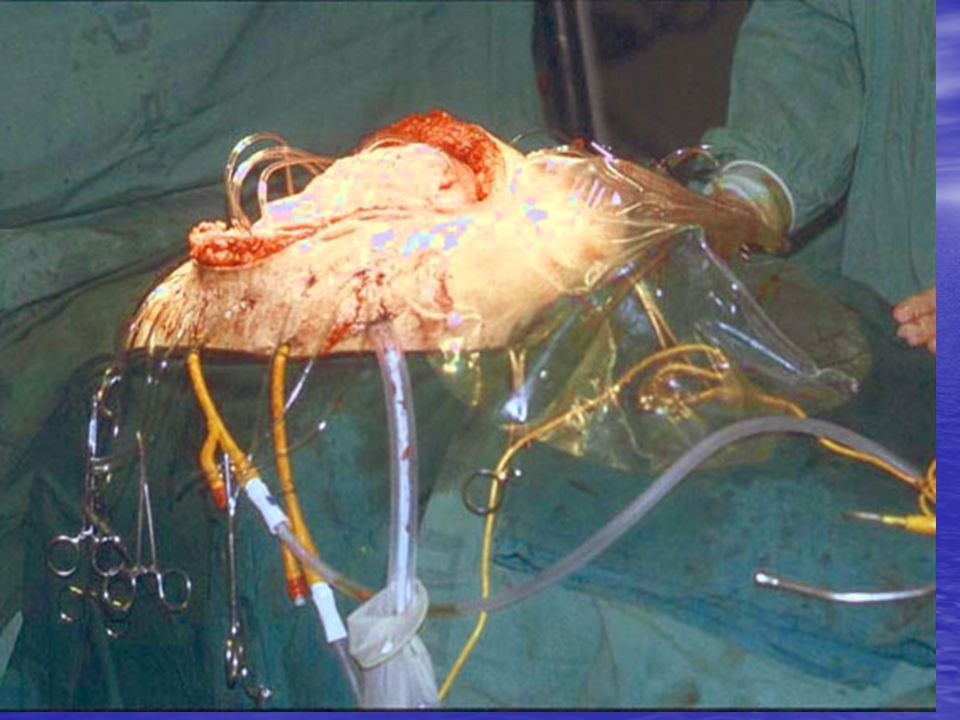
Laparostomy

44
Bedside Laparotomy for Trauma: Are There Risks? Posted 06/01/2004
Jose J. Diaz, Jr.; Adele Mauer; Addison K. May; Richard Miller; Jeffery S. Guy; John A. Morris, Jr. Abstract and Introduction Abstract Background: Critically ill trauma patients are often too unstable for safe transfer to the operating room. Damage control laparotomy patients frequently require early reoperation and have a reported mortality of 50-60%. As a result, many of these patients must undergo laparotomy in the intensive care unit. We hypothesized that patients undergoing bedside laparotomy (BSL) and managed with the abdomen left open would have an unacceptably high mortality or intraabdominal complications. Methods: We performed a retrospective chart review of our Trauma Registry. Of the 11,096 consecutive trauma admissions from March 1, 1996 to May 20, 2000, 75 patients underwent 95 BSL. Patients were stratified according to injury severity score (ISS), base deficit (BD), lactic acid (LA), total transfusion (TRBC) requirements, indication for BSL, mechanism of injury, infectious complications (intraabdominal abscess (IAA), fistula), and length of hospital stay. Results: Seventy-five patients underwent 95 BSL. Mean ISS was 50.6 ± 18.9, mean BD was (± 5), and the mean LA was 5 ± 5 for the study group. The TRBC for the group was 43.7 ± 42.6 units. Indications for the 95 BSL were (1) abdominal compartment syndrome (n = 47, 49.5%); (2) suspected intraabdominal infection (n = 18, 19.0%); (3) washout/pack removal (n = 14, 14.7%); (4) washout with fascial closure (n = 12, 12.6%); and (5) other (n = 4, 4.2%). Twentynine of 75 patients (39.2%; ISS 52.3 ± 18.8) died within 72 h of operation. Of the 46 remaining patients, an additional eight died 72 h or more after operation, for a late mortality rate of 17.4% and a total mortality rate of 49%. None of these deaths were attributable to either the operation or to postoperative IAA or fistula formation; all late deaths were secondary to multiple organ failure. Intraabdominal abscesses developed in three of 46 patients (6.5%), each of whom had a TRBC of > 100 units (mean, 160 units). Five of 46 patients (10.9%) developed enterocutaneous fistulae. None of these eight patients died. Thirtyeight of 75 patients (50.7%) survived to discharge, with a mean ISS of 40 (± 11.9). Conclusions: Despite the high acuity of the population undergoing BSL, 50.7% of patients survived. Moreover, during BSL, IAA and fistula formation occurred at low rates. Introduction In the early 1990s, reports of damage control laparotomy for abdominal trauma began to appear in the medical literature.[1,2] Damage control laparotomy patients present in extremis, frequently require early reoperation, and have a reported 50-60% mortality rate.[3,4] Concurrently, advances in critical care management of the severely injured trauma patient are allowing many patients who would previously have died to survive the initial injury. As such, trauma centers are caring for an increasing number of critically ill patients who are often too unstable for safe transfer to the operating room. This often manifests as ventilatory requirements that are too high for either bagmask ventilation or a transport ventilator, or a sudden change in the patient's pathophysiology such that the brief time needed for transportation and preparation of the operating room would be nonsurvivable. As a result, many of these patients require bedside laparotomy (BSL) in the intensive care unit (ICU) accepting the known limitations of inadequate lighting, lack of a sterile environment, absence of trained operating room personnel, and limited surgical instruments. An adjunct to damage control in the management of the trauma patient, a protocol for BSL should be prepared before an emergent need for bedside surgery.[5] With the recognition of the abdominal compartment syndrome, bedside surgical decompression has become more common as a lifesaving procedure.[6] As a result, the occurrence of trauma patients managed with an open abdomen has become commonplace. We hypothesized that patients undergoing BSL and managed with an open abdomen would have an unacceptably high mortality rate or incidence of intraabdominal complications.
 and managed with the abdomen left open would have an unacceptably high mortality or intraabdominal complications. Methods: We performed a retrospective chart review of our Trauma Registry. Of the 11,096 consecutive trauma admissions from March 1, 1996 to May 20, 2000, 75 patients underwent 95 BSL. Patients were stratified according to injury severity score (ISS), base deficit (BD), lactic acid (LA), total transfusion (TRBC) requirements, indication for BSL, mechanism of injury, infectious complications (intraabdominal abscess (IAA), fistula), and length of hospital stay. Results: Seventy-five patients underwent 95 BSL. Mean ISS was 50.6 ± 18.9, mean BD was (± 5), and the mean LA was 5 ± 5 for the study group. The TRBC for the group was 43.7 ± 42.6 units. Indications for the 95 BSL were (1) abdominal compartment syndrome (n = 47, 49.5%); (2) suspected intraabdominal infection (n = 18, 19.0%); (3) washout/pack removal (n = 14, 14.7%); (4) washout with fascial closure (n = 12, 12.6%); and (5) other (n = 4, 4.2%). Twentynine of 75 patients (39.2%; ISS 52.3 ± 18.8) died within 72 h of operation. Of the 46 remaining patients, an additional eight died 72 h or more after operation, for a late mortality rate of 17.4% and a total mortality rate of 49%. None of these deaths were attributable to either the operation or to postoperative IAA or fistula formation; all late deaths were secondary to multiple organ failure. Intraabdominal abscesses developed in three of 46 patients (6.5%), each of whom had a TRBC of > 100 units (mean, 160 units). Five of 46 patients (10.9%) developed enterocutaneous fistulae. None of these eight patients died. Thirtyeight of 75 patients (50.7%) survived to discharge, with a mean ISS of 40 (± 11.9). Conclusions: Despite the high acuity of the population undergoing BSL, 50.7% of patients survived. Moreover, during BSL, IAA and fistula formation occurred at low rates. Introduction. In the early 1990s, reports of damage control laparotomy for abdominal trauma began to appear in the medical literature.[1,2] Damage control laparotomy patients present in extremis, frequently require early reoperation, and have a reported 50-60% mortality rate.[3,4] Concurrently, advances in critical care management of the severely injured trauma patient are allowing many patients who would previously have died to survive the initial injury. As such, trauma centers are caring for an increasing number of critically ill patients who are often too unstable for safe transfer to the operating room. This often manifests as ventilatory requirements that are too high for either bagmask ventilation or a transport ventilator, or a sudden change in the patient s pathophysiology such that the brief time needed for transportation and preparation of the operating room would be nonsurvivable. As a result, many of these patients require bedside laparotomy (BSL) in the intensive care unit (ICU) accepting the known limitations of inadequate lighting, lack of a sterile environment, absence of trained operating room personnel, and limited surgical instruments. An adjunct to damage control in the management of the trauma patient, a protocol for BSL should be prepared before an emergent need for bedside surgery.[5] With the recognition of the abdominal compartment syndrome, bedside surgical decompression has become more common as a lifesaving procedure.[6] As a result, the occurrence of trauma patients managed with an open abdomen has become commonplace. We hypothesized that patients undergoing BSL and managed with an open abdomen would have an unacceptably high mortality rate or incidence of intraabdominal complications.")
45
MANEJO NO QUIRÚRGICO

46
Manejo Conservador Laparotomías Innecesarias Renz 1995 Wigelt 1988
27.1% negativas laparotomías incluyendo penetrantes y no penetrantes Wigelt 1988 1.2% lesiones Iatrogénicas 16 publicaciones colectivamente 20.6% por Penetrante 20% por no penetrantes

47
Trauma Abdominal Cerrado
Lesiones que pueden ser seguidas conservadoramente Hígado Bazo Fracturas pélvicas Hematomas retroperitoneales Excépto: Hematomas pancreaticoduodenales

49
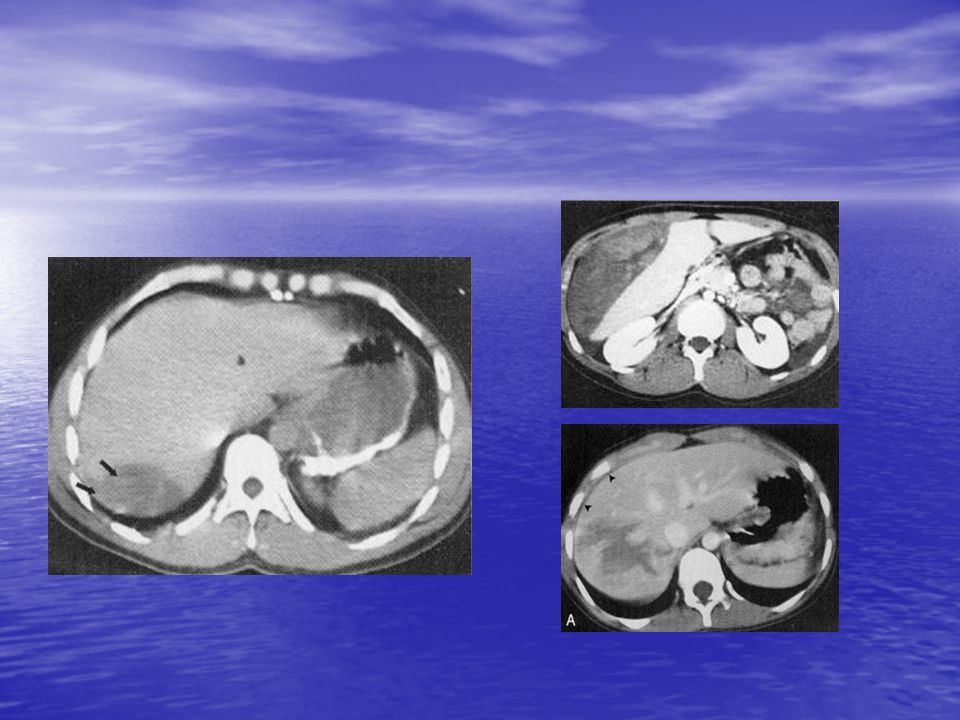
Lesiones Hepáticas Complejas
495 lesiones hepáticas 94% de éxito con tratamiento conservador Pachter HL, Hofstetter SR. The current status of nonoperative management of adult blunt hepatic injuries. Am J Surg 1995;169:442–454.

50
Lesiones Hepáticas Complejas
Promedio de transfusiones 1.9 unidades 6.2% de complicaciones 2.8% relacionadas con la hemorrágia 13 días de promedio de internación Pachter HL, Hofstetter SR. The current status of nonoperative management of adult blunt hepatic injuries. Am J Surg 1995;169:442–454.

51
Lesiones Hepáticas Complejas
404 casos de lesiones cerradas hepatica estudio multiinstitucional 98.5% de éxito evitando una intervención quirúrgica 5% de complicaciones Pachter HL, Knudson MM, Esrig B, et al. Status of nonoperative management of blunt hepatic injuries in 1995: a multicenter experience with 404 patients. J Trauma 1996;40:31–38

52
Lesiones Hepáticas Complejas
Complicaciones (3.5%) continuaron sangrando, solo 3 pacientes requirieron ser intervenidos para controlar la hemorragia (0.7%) 1.5% formación de bilomas. Pachter HL, Knudson MM, Esrig B, et al. Status of nonoperative management of blunt hepatic injuries in 1995: a multicenter experience with 404 patients. J Trauma 1996;40:31–38
 continuaron sangrando, solo 3 pacientes requirieron ser intervenidos para controlar la hemorragia (0.7%) 1.5% formación de bilomas. Pachter HL, Knudson MM, Esrig B, et al. Status of nonoperative management of blunt. hepatic injuries in 1995: a multicenter experience with 404 patients. J Trauma 1996;40:31–38.")
53
Manejo Conservador La otra cara de la moneda
Lesiones no identificadas 3.4% La morbilidad es aceptable Para tener éxito en manejo no operatorio se necesita Tecnología Encimología Olfatología Dr ludi

55
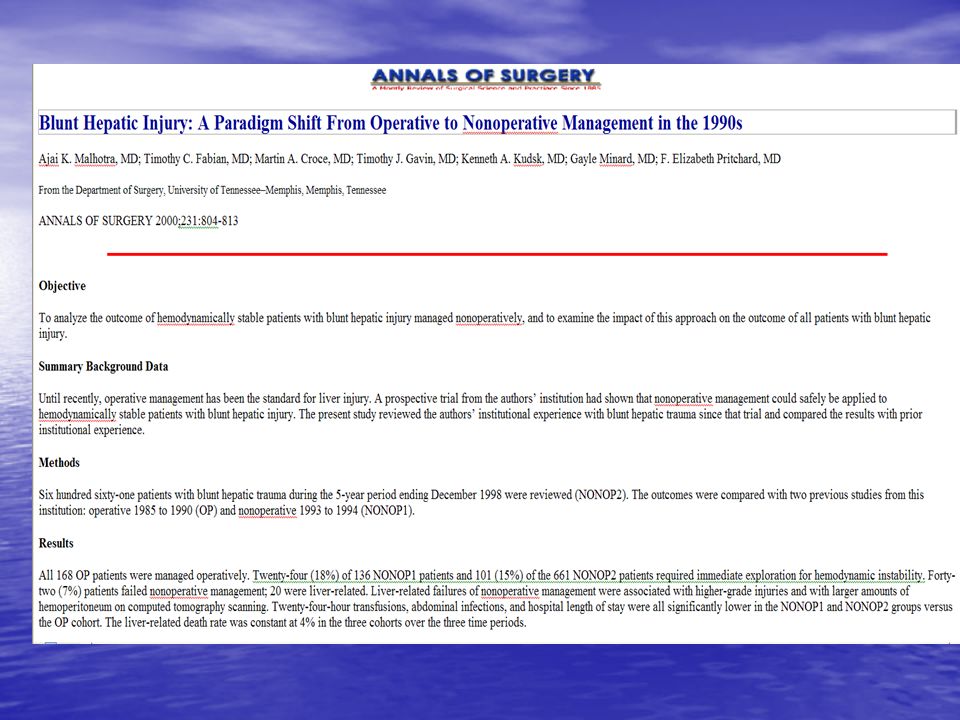
FABIAN

57
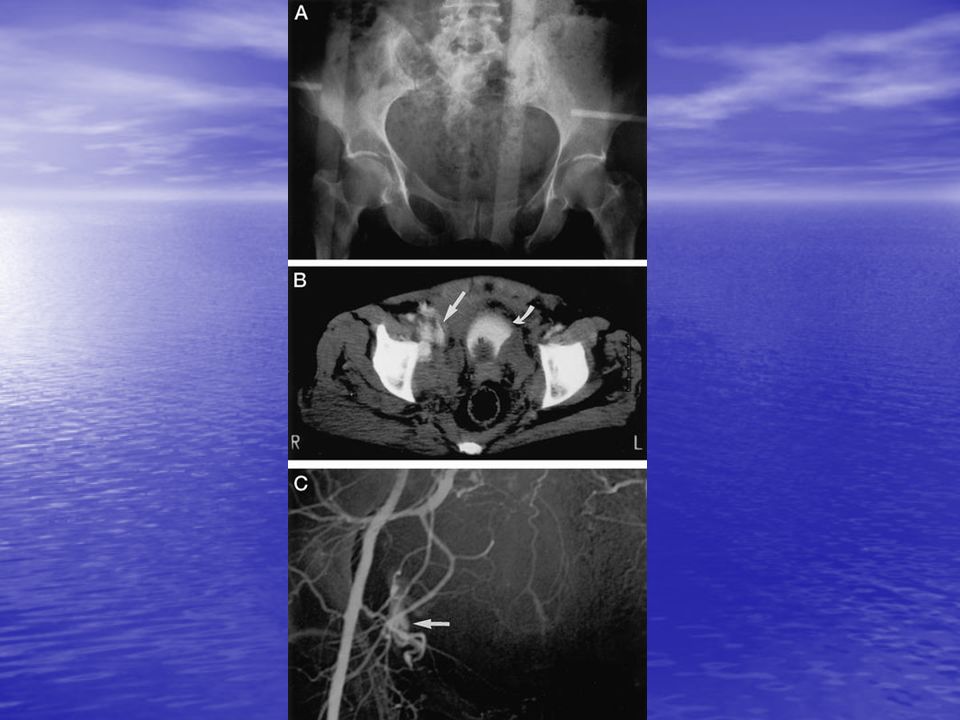
Lesiones de pelvis

58
A B C

59
Clasificasion APC anterior-posterior compresion
Type I: Isolated pubic diastasis and/or pubic ramus disruption < 2.5 cm Type II: Anterior ramus fractures and/or diastasis >2.5 cm with widened SI joint (s). Totationally unstable Type III: Disruption of symphysis or significant Separation of anterior vertical ramus fractures. Disruption of anterior/posterior ligamets of SI Joint.Totationally and vertically unstable LC (Lateral Compression) Type I: Horizontal fractures of pubic rami. Impaction injury/fracture of sacrum Type II: Horizontal fractures of pubic tam with ligamentous or Bony disruption of SI joint Type III: Horizontal fractures of pubic rami with contralateral Ramus and SI joint disruption (APC type injury) VS (vertical shear) Complete bony and ligamentous disruption of hemipelvis with Vertical displacement
. Totationally unstable. Type III: Disruption of symphysis or significant Separation of. anterior vertical ramus fractures. Disruption of anterior/posterior. ligamets of SI Joint.Totationally and vertically unstable. LC (Lateral Compression) Type I: Horizontal fractures of pubic rami. Impaction. injury/fracture of sacrum. Type II: Horizontal fractures of pubic tam with ligamentous or. Bony disruption of SI joint. Type III: Horizontal fractures of pubic rami with contralateral. Ramus and SI joint disruption (APC type injury) VS (vertical shear) Complete bony and ligamentous disruption of hemipelvis with. Vertical displacement.")
60
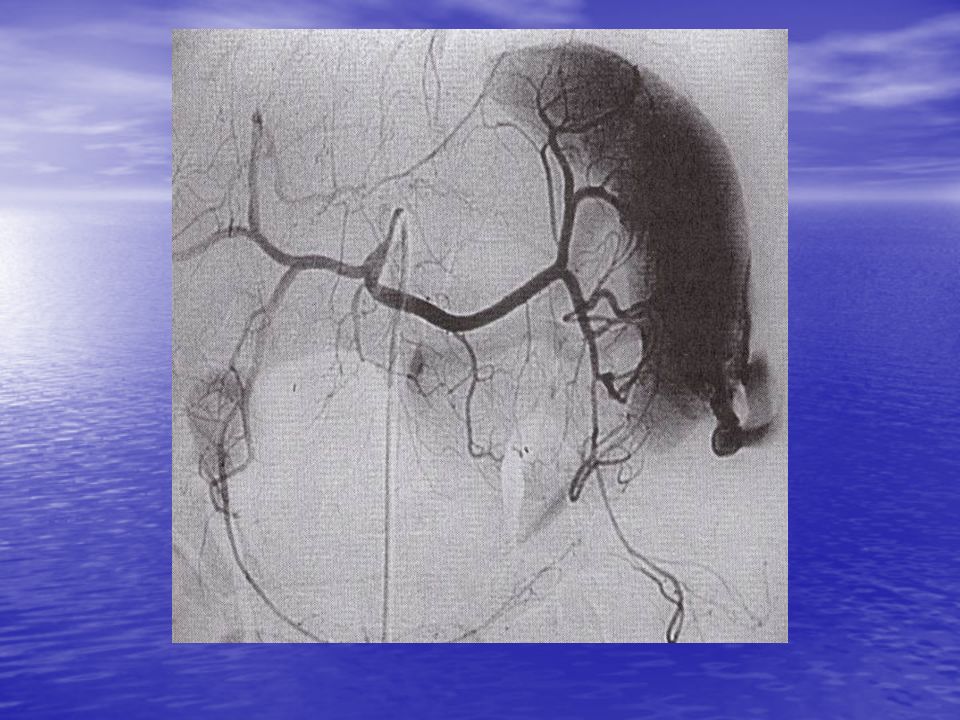
Fracturas Pélvicas y Embolización
Pacientes estables: Mortalidad 3% - 8% Pacientes inestables: Mortalidad 42% - 50% Muertes durantes las primeras 24 horas

61
EAST Guidelines Qué pacientes deberían tener una agiografía y posible embolización??? Pacientes con fracturas pélvicas con signos de un sangrado activo después que se ha descartado otra fuente de sangrado Pacientes con fracturas pélvicas mayores que durante la laparotomía exploradora no se pudo controlar el sangrado Pacientes con evidencia de extravasación arterial de contraste en la pelvis durante una TAC

62
Entendiendo la fisiología
La pelvis es una gran cavidad Control del sangrado Venoso por taponamiento va a necesitar grandes volumenes de sangrado… Con grandes consumos de Sangre entera Factores de Coagulacion Arterial probablemente no va a parar De los huesos fracturados

63
Embolización Problemas Alto porcentaje de negativos 20% +-
Alta mortalidad debido a lesiones concomitantes Todavía no bien estudiado los efectos a largo plaso de las embolizaciones bilaterales Impotencia????

65
BIBLIOGRAFIA Meyer AA: Abdominal Compartment Syndrome: A new problem or a newly recognised old problem? 85TH Clinical congress of the American College of Surgeons. Oct 10-15, San Francisco. California. Summary conference index. Medscape 1999 Ivatury RR, Porter JM, Simon RJ, et al: Intra-abdominal hypertension after life-threatening penetrating abdominal trauma: prophilaxis, incidence, and clinical relevance to gastric mucosal pH and abdominal compartment syndrome. J Trauma 1998 Jun; 44 (6): Bloomfield, G., Saggi, B., Blocher, C, & Sugerman, H. (1999). Physiologic effects of externally applied continuous negative abdominal pressure for intra-abdominal hypertension. Journal of Trauma: Injury, Infection and Critical Care. Jun; 46(6): Diebel, L., Dulchavsky & S., Brown, W. (1997). Splanchnic ischemia and bacterial translocation in the abdominal compartment syndrome Offner, P. & Burch, J. (1998). Abdominal compartment syndrome, part 1: presentation and workup: cardiopulmonary and renal findings are among the most prominent signs. Journal of Critical Illness. Oct; 13(10): Offner, P. & Burch, J. (1998). Abdominal compartment syndrome, part 2: management guidelines: which patients will require abdominal decompression? Journal of Critical Illness. Oct 13(10):
: Bloomfield, G., Saggi, B., Blocher, C, & Sugerman, H. (1999). Physiologic effects of externally applied continuous negative abdominal pressure for intra-abdominal hypertension. Journal of Trauma: Injury, Infection and Critical Care. Jun; 46(6): Diebel, L., Dulchavsky & S., Brown, W. (1997). Splanchnic ischemia and bacterial translocation in the abdominal compartment syndrome. Offner, P. & Burch, J. (1998). Abdominal compartment syndrome, part 1: presentation and workup: cardiopulmonary and renal findings are among the most prominent signs. Journal of Critical Illness. Oct; 13(10): Offner, P. & Burch, J. (1998). Abdominal compartment syndrome, part 2: management guidelines: which patients will require abdominal decompression Journal of Critical Illness. Oct 13(10):")
66
MUCHAS GRACIAS Quiero vivir la vida aventurera
de los errantes pájaros marinos... MUCHAS GRACIAS

Presentaciones similares







 European Transfer Credit System (ECTS) Methodology in.>")



.>")









 Noviembre de 2004.>")



