Descargar la presentación
La descarga está en progreso. Por favor, espere

1
UPDATE 2006. ¿Qué hay de nuevo en el manejo de los lípidos?
Fuengirola. Enero 2006 Dr. JJ Gómez Doblas Hospital Universitario Virgen de la Victoria Málaga

2
Índice Tratamiento con estatinas ¿Intensivo o moderado?.
Riesgos del uso de estatinas. Aumentar el HDL. Resultados con fármacos. Otros usos de las estatinas. Insuficiencia cardiaca, sepsis, arritmias. Actualización guías clínicas

3
Tratamiento con estatinas ¿intensivo o moderado?.
Estudios recientes han demostrado que altas dosis de estatinas pueden ser mas efectivas que las dosis estandar en reducir la aparicion de eventos CV (PROVE IT- TIMI-22, TNT) Sin embargo otros dos estudios (A-to-Z e IDEAL) mostraron una tendencia no significativa hacia el beneficio de la estrategia intensiva para sus end-point primarios.
 Sin embargo otros dos estudios (A-to-Z e IDEAL) mostraron una tendencia no significativa hacia el beneficio de la estrategia intensiva para sus end-point primarios.")
4
Meta-Analysis of Cardiovascular Outcomes Trials
Comparing Intensive Versus Moderate Statin Therapy Christopher P. Cannon, MD, Benjamin A. Steinberg, BA, Sabina A. Murphy, MPH, Jessica L. Mega, MD, Eugene Braunwald, MD J Am Coll Cardiol 2006;48:438–45) 1 Agosto , 2006
 1 Agosto ,")
5
Diseños de los estudios incluidos
PROVE IT-TIMI-22 A to Z TNT IDEAL n 4162 4497 10001 8888 Población Post-SCA CI estable Brazos tto 40 mg Pravastatina vs 80 mg Atorvastatina Placebo ( 4 meses ) -20 mg Simvastatina vs 40 mg Simvastatina (1 mes) -80 mg Simvastatina 10 mg Atorvastatina vs 80 mg Atorvastatina 20 mg Simvastatina vs 80 mg Atorvastatina Duración 24 meses (media) 721 dias (mediana) 4,9 años (mediana) 4,8 años (mediana) End-point primario Muerte, IAM, AI hosp, revascularización > 30 días, ACV Muerte CV, IAM, reingreso por SCA, ACV Muerte coronaria, IAM, PCR resucitada, ACV Muerte coronaria, IAM, PCR resucitada
 -20 mg Simvastatina vs 40 mg Simvastatina (1 mes) -80 mg Simvastatina. 10 mg Atorvastatina vs 80 mg Atorvastatina. 20 mg Simvastatina vs 80 mg Atorvastatina. Duración. 24 meses (media) 721 dias (mediana) 4,9 años (mediana) 4,8 años (mediana) End-point primario. Muerte, IAM, AI hosp, revascularización > 30 días, ACV. Muerte CV, IAM, reingreso por SCA, ACV. Muerte coronaria, IAM, PCR resucitada, ACV. Muerte coronaria, IAM, PCR resucitada.")
6
Niveles de LDL alcanzados

7
Reducción 16 % riesgo de muerte coronaria o algún evento CV (IAM, ACV, AI o revascularización)
")
8
Mortalidad Mortalidad CV Mortalidad Total

9
Tasa de efectos adversos

10
Conclusiones El tratamiento intensivo con estatinas vs. el tratamiento estándar aporta beneficios en la prevención de eventos CV no fatales, incluyendo ACV, con una tendencia en la reducción de la mortalidad CV en pacientes con cardiopatía isquemica estable o tras SCA.

11
Comentarios y limitaciones.
Nuevos datos del estudio SEARCH (80 mg Simvastatina vs 20 mg Simvastatina) aportaran poder estadístico sobre los end points de mortalidad. No existen datos de pacientes individuales, con lo que no es posible determinar si el beneficio es por el nivel de LDL alcanzado o por la dosis altas de estatinas. No existe un análisis de costo-beneficio
 aportaran poder estadístico sobre los end points de mortalidad. No existen datos de pacientes individuales, con lo que no es posible determinar si el beneficio es por el nivel de LDL alcanzado o por la dosis altas de estatinas. No existe un análisis de costo-beneficio.")
12
Effect of Very High-Intensity Statin Therapy
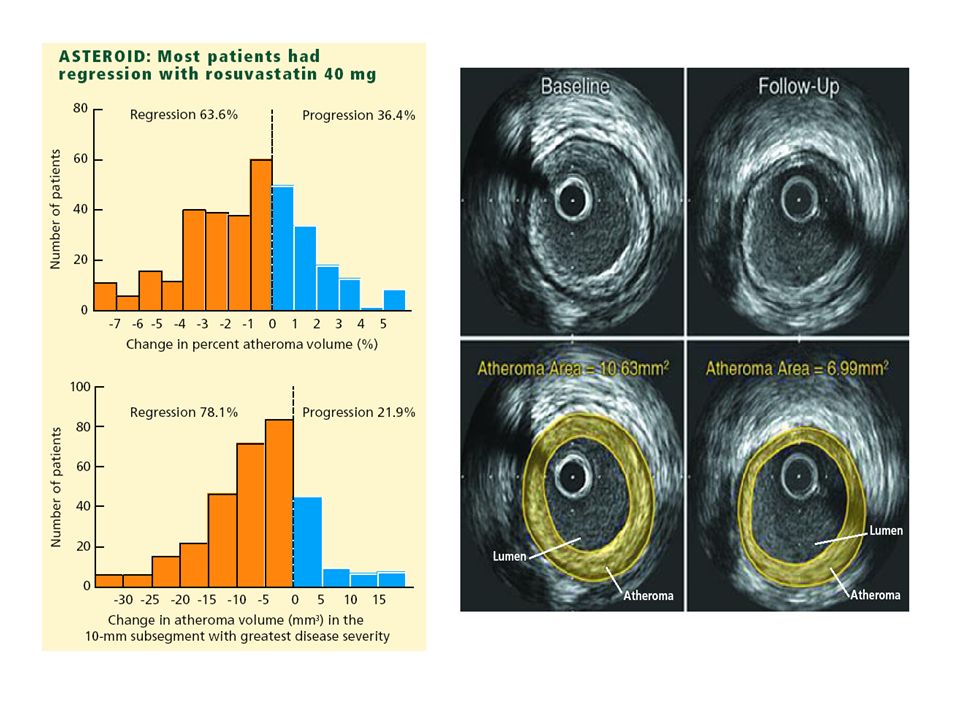
on Regression of Coronary Atherosclerosis The ASTEROID Trial S Nissen et al. Context Prior intravascular ultrasound (IVUS) trials have demonstrated slowing or halting of atherosclerosis progression with statin therapy but have not shown convincing evidence of regression using percent atheroma volume (PAV), the most rigorous IVUS measure of disease progression and regression. Objective To assess whether very intensive statin therapy could regress coronary atherosclerosis as determined by IVUS imaging. Design and Setting Prospective, open-label blinded end-points trial (A Study to Evaluate the Effect of Rosuvastatin on Intravascular Ultrasound-Derived Coronary Atheroma Burden [ASTEROID]) was performed at 53 community and tertiary care centers in the United States, Canada, Europe, and Australia. A motorized IVUS pullback was used to assess coronary atheroma burden at baseline and after 24 months of treatment. Each pair of baseline and follow-up IVUS assessments was analyzed in a blinded fashion. Patients Between November 2002 and October 2003, 507 patients had a baseline IVUS examination and received at least 1 dose of study drug. After 24 months, 349 patients had evaluable serial IVUS examinations. Intervention All patients received intensive statin therapy with rosuvastatin, 40 mg/d. Main Outcome Measures Two primary efficacy parameters were prespecified: the change in PAV and the change in nominal atheroma volume in the 10-mm subsegment with the greatest disease severity at baseline. A secondary efficacy variable, change in normalized total atheroma volume for the entire artery, was also prespecified. Results The mean (SD) baseline low-density lipoprotein cholesterol (LDL-C) level of 130.4 (34.3) mg/dL declined to 60.8 (20.0) mg/dL, a mean reduction of 53.2% (P.001). Mean (SD) high-density lipoprotein cholesterol (HDL-C) level at baseline was 43.1 (11.1) mg/dL, increasing to 49.0 (12.6) mg/dL, an increase of 14.7% (P.001). The mean SD) change in PAV for the entire vessel was -0.98% (3.15%), with a median of -0.79% 97.5% CI, -1.21% to -0.53%) (P.001 vs baseline). The mean (SD) change in atheroma volume in the most diseased 10-mm subsegment was -6.1 (10.1) mm3, with a median of -5.6 mm3 (97.5% CI, -6.8 to -4.0 mm3) (P.001 vs baseline). Change in total atheroma volume showed a 6.8% median reduction; with a mean (SD) reduction of (25.7)mm3, with a median of -12.5mm3 (95% CI, to -10.5mm3) (P.001 vs baseline). Adverse events were infrequent and similar to other statin trials. Conclusions Very high-intensity statin therapy using rosuvastatin 40 mg/d achieved an average LDL-C of 60.8 mg/dL and increased HDL-C by 14.7%, resulting in significant regression of atherosclerosis for all 3 prespecified IVUS measures of disease burden. Treatment to LDL-C levels below currently accepted guidelines, when accompanied by significant HDL-C increases, can regress atherosclerosis in coronary disease patients. Further studies are needed to determine the effect of the observed changes on clinical outcome. Trial Registration ClinicalTrials.gov Identifier: NCT JAMA. 2006;295: JAMA. 2006;295: 5 Abril , 2006
 trials have demonstrated slowing or. halting of atherosclerosis progression with statin therapy but have not shown convincing. evidence of regression using percent atheroma volume (PAV), the most rigorous. IVUS measure of disease progression and regression. Objective To assess whether very intensive statin therapy could regress coronary. atherosclerosis as determined by IVUS imaging. Design and Setting Prospective, open-label blinded end-points trial (A Study to Evaluate. the Effect of Rosuvastatin on Intravascular Ultrasound-Derived Coronary Atheroma. Burden [ASTEROID]) was performed at 53 community and tertiary care centers in the. United States, Canada, Europe, and Australia. A motorized IVUS pullback was used to. assess coronary atheroma burden at baseline and after 24 months of treatment. Each. pair of baseline and follow-up IVUS assessments was analyzed in a blinded fashion. Patients Between November 2002 and October 2003, 507 patients had a baseline. IVUS examination and received at least 1 dose of study drug. After 24 months, 349. patients had evaluable serial IVUS examinations. Intervention All patients received intensive statin therapy with rosuvastatin, 40 mg/d. Main Outcome Measures Two primary efficacy parameters were prespecified: the. change in PAV and the change in nominal atheroma volume in the 10-mm subsegment. with the greatest disease severity at baseline. A secondary efficacy variable, change in. normalized total atheroma volume for the entire artery, was also prespecified. Results The mean (SD) baseline low-density lipoprotein cholesterol (LDL-C) level of (34.3) mg/dL declined to 60.8 (20.0) mg/dL, a mean reduction of 53.2% (P.001). Mean (SD) high-density lipoprotein cholesterol (HDL-C) level at baseline was 43.1 (11.1) mg/dL, increasing to 49.0 (12.6) mg/dL, an increase of 14.7% (P.001). The mean. SD) change in PAV for the entire vessel was -0.98% (3.15%), with a median of -0.79% 97.5% CI, -1.21% to -0.53%) (P.001 vs baseline). The mean (SD) change in atheroma. volume in the most diseased 10-mm subsegment was -6.1 (10.1) mm3, with a. median of -5.6 mm3 (97.5% CI, -6.8 to -4.0 mm3) (P.001 vs baseline). Change in. total atheroma volume showed a 6.8% median reduction; with a mean (SD) reduction. of (25.7)mm3, with a median of -12.5mm3 (95% CI, to -10.5mm3) (P.001. vs baseline). Adverse events were infrequent and similar to other statin trials. Conclusions Very high-intensity statin therapy using rosuvastatin 40 mg/d achieved. an average LDL-C of 60.8 mg/dL and increased HDL-C by 14.7%, resulting in significant. regression of atherosclerosis for all 3 prespecified IVUS measures of disease burden. Treatment. to LDL-C levels below currently accepted guidelines, when accompanied by significant. HDL-C increases, can regress atherosclerosis in coronary disease patients. Further. studies are needed to determine the effect of the observed changes on clinical outcome. Trial Registration ClinicalTrials.gov Identifier: NCT JAMA. 2006;295: JAMA. 2006;295: Abril ,")
13
Diseño 349 pacientes tratados con Rosuvastatina End points. IVUS
LDL-C se redujo de 130 mg/dL a 61 mg/dL durante el estudio (reducción del 53%). HDL-C aumento de 43 mg/dL a 49 mg/dL un incremento del 15%
. HDL-C aumento de 43 mg/dL a 49 mg/dL un incremento del 15%")
15
Estudios de regresion coronaria con IVUS
Relacion entre LDL colesterol y tasa progresion. CAMELOT placebo REVERSAL pravastatin ACTIVATE placebo Median Change in Percent Atheroma Volume (%) REVERSAL atorvastatin A-Plus placebo ASTEROID provides us with further scientific evidence to support the concept that lower is likely better for LDL-C levels. Further, by showing that actual plaque regression can be achieved, the enthusiasm for lowering LDL-C to low levels (~60 mg/dL) as achieved in this trial is bound to increase. One must, however, remember that there was not a clinically meaningful endpoint in this trial, i.e., it was not an event-driven trial. Hence, it is unlikely that these results will change clinical practice or guidelines significantly other than to endorse strongly the option of lowering LDL-C to <70 mg/dL and to raise the question of whether this optional goal should become a recommended target. Nevertheless, clinically relevant information has been gained from this study: a) the maximum dose of rosuvastatin (40 mg/d) was well tolerated and had an acceptable adverse effect profile, and b) lower LDL-C values were also well tolerated without any apparent problems. The study also raises several important research questions that will likely impact our management of atherosclerotic arterial disease in a significant way in the future. Was it the LDL-C decrease, the HDL-C increase, the percent changes in these lipids, or the LDL-C/HDL-C ratio (i.e., values close to 1) that led to plaque regression? Was the effect statin specific, or would all statins have a similar effect if they achieved an LDL-C level similar to that achieved in this study? Another study, Measuring Effects on Intima–Media Thickness: an Evaluation of Rosuvastatin (METEOR), is evaluating the effect of rosuvastatin 40 mg/d on atherosclerosis as evaluated by carotid ultrasound. Asymptomatic subjects at low risk for cardiovascular disease but with atherosclerosis as evidenced by intima–media thickness will be randomized in this placebo-controlled, parallel-group study and followed for 104 weeks. Although new drugs such as squalene synthase inhibitors are being evaluated to target LDL-C lowering, the next major focus in lipid studies will be towards targeting HDL. HDL is thought to be atheroprotective, a function that has been linked to its ability to help in the process of reverse cholesterol transport. Lipid-poor nascent HDL particles accept cholesterol from peripheral cells through the interaction of apolipoprotein A-I (apo A-I), the major protein of HDL, with ATP-binding cassette protein A1. After cholesterol esterification, the HDL particle transfers the cholesteryl esters to the liver via scavenger receptor B1 or to the apo B–containing particles (in exchange for triglycerides) through the action of cholesteryl ester transfer protein (CETP). A CETP inhibitor, torcetrapib, is already being studied in clinical trials, and other strategies such as synthetic HDLs are also being tested. The statistically significant regression achieved in ASTEROID with a 53.2% reduction in LDL-C and a 14.7% increase in HDL-C holds promise that HDL-modifying therapy in concert with LDL-C–lowering therapy may achieve even greater amounts of plaque regression. Current therapies such as niacin plus statin are being examined in ongoing studies such as Atherothrombosis Drug Intervention for Metabolic Syndrome with Low HDL/High Triglycerides and Its Impact on Global Health Outcomes (AIM HIGH), and experimental therapies such as torcetrapib/atorvastatin are also being evaluated in clinical trials; the results should be available in the next few years. Further advances in lipid management over the next decade will likely impact the management of atherosclerotic cardiovascular disease in a significant way, and it may be possible to perform "noninvasive angioplasty" effectively and successfully. R2 = 0.95 p<0.001 ASTEROID rosuvastatin 50 60 70 80 90 100 110 120 Mean LDL-C (mg/dL) Nissen SE et al. JAMA 2006;295:
 REVERSAL atorvastatin. A-Plus placebo. ASTEROID provides us with further scientific evidence to support the concept that lower is likely better for LDL-C levels. Further, by showing that actual plaque regression can be achieved, the enthusiasm for lowering LDL-C to low levels (~60 mg/dL) as achieved in this trial is bound to increase. One must, however, remember that there was not a clinically meaningful endpoint in this trial, i.e., it was not an event-driven trial. Hence, it is unlikely that these results will change clinical practice or guidelines significantly other than to endorse strongly the option of lowering LDL-C to <70 mg/dL and to raise the question of whether this optional goal should become a recommended target. Nevertheless, clinically relevant information has been gained from this study: a) the maximum dose of rosuvastatin (40 mg/d) was well tolerated and had an acceptable adverse effect profile, and b) lower LDL-C values were also well tolerated without any apparent problems. The study also raises several important research questions that will likely impact our management of atherosclerotic arterial disease in a significant way in the future. Was it the LDL-C decrease, the HDL-C increase, the percent changes in these lipids, or the LDL-C/HDL-C ratio (i.e., values close to 1) that led to plaque regression Was the effect statin specific, or would all statins have a similar effect if they achieved an LDL-C level similar to that achieved in this study Another study, Measuring Effects on Intima–Media Thickness: an Evaluation of Rosuvastatin (METEOR), is evaluating the effect of rosuvastatin 40 mg/d on atherosclerosis as evaluated by carotid ultrasound. Asymptomatic subjects at low risk for cardiovascular disease but with atherosclerosis as evidenced by intima–media thickness will be randomized in this placebo-controlled, parallel-group study and followed for 104 weeks. Although new drugs such as squalene synthase inhibitors are being evaluated to target LDL-C lowering, the next major focus in lipid studies will be towards targeting HDL. HDL is thought to be atheroprotective, a function that has been linked to its ability to help in the process of reverse cholesterol transport. Lipid-poor nascent HDL particles accept cholesterol from peripheral cells through the interaction of apolipoprotein A-I (apo A-I), the major protein of HDL, with ATP-binding cassette protein A1. After cholesterol esterification, the HDL particle transfers the cholesteryl esters to the liver via scavenger receptor B1 or to the apo B–containing particles (in exchange for triglycerides) through the action of cholesteryl ester transfer protein (CETP). A CETP inhibitor, torcetrapib, is already being studied in clinical trials, and other strategies such as synthetic HDLs are also being tested. The statistically significant regression achieved in ASTEROID with a 53.2% reduction in LDL-C and a 14.7% increase in HDL-C holds promise that HDL-modifying therapy in concert with LDL-C–lowering therapy may achieve even greater amounts of plaque regression. Current therapies such as niacin plus statin are being examined in ongoing studies such as Atherothrombosis Drug Intervention for Metabolic Syndrome with Low HDL/High Triglycerides and Its Impact on Global Health Outcomes (AIM HIGH), and experimental therapies such as torcetrapib/atorvastatin are also being evaluated in clinical trials; the results should be available in the next few years. Further advances in lipid management over the next decade will likely impact the management of atherosclerotic cardiovascular disease in a significant way, and it may be possible to perform noninvasive angioplasty effectively and successfully. R2 = 0.95 p< ASTEROID rosuvastatin Mean LDL-C (mg/dL) Nissen SE et al. JAMA 2006;295:")
16
Riesgos en el uso de estatinas.
El uso de estatinas esta infrautilizado. El miedo a sus efectos adversos puede ser un factor limitante en su uso. Metanalisis previos sobre la seguridad de las estatinas se focalizaban en solo algunos efectos adversos.

17
Risks Associated With Statin Therapy:
A Systematic Overview of Randomized Clinical Trials Amir Kashani, Christopher O. Phillips, JoAnne M. Foody, Yongfei Wang, Sandeep Mangalmurti, Dennis T. Ko and Harlan M. Krumholz Circulation 2006;114; Online 11 Diciembre 2006

18
74102 pacientes en 35 estudios con un rango de seguimiento de 1-65 meses

19
RD : Diferencia de riesgo por 1000 pacientes.
Mialgias . Mas mialgias con atorvastatina. Elevación de transaminasas. Todas las estatinas

20
Comparación con cerivastatina
Figure 2. Risk difference of FDAapproved statins vs cerivastatin. The significant increased risk of CK elevation and rhabdomyolysis with cerivastatin compared with currently FDA-approved statins is shown. However, cerivastatin was not associated with an increased risk of myalgias. This may result in the elimination of warning signs (ie, musculoskeletal symptoms) before the development of more serious adverse events. IRD indicates incidence risk difference. Probability value is for statin vs placebo.
 before the development. of more serious adverse events. IRD indicates incidence risk difference. Probability value is for statin vs placebo.")
21
Conclusiones El uso de estatinas se asocia a un ligero riesgo de elevación de transaminasas, pero no de mialgias, elevación de CK, rabdomiolisis o abandono de tratamiento frente al uso de placebo. Son necesarios mas estudios poblaciones para conocer si estos resultados son similares en la practica clínica diaria, particularmente ancianos, comorbilidad importante o uso de altas dosis de estatinas .

22
Limitaciones Escasa validez externa: Sesgo en la selección de pacientes de ensayos clínicos (jóvenes y escasa comorbilidad) Problemas de diseños. > 95 % estudios dosis bajas de estatinas Escaso poder para efectos adversos infrecuentes. No aporta información sobre el uso concomitante de fibratos y estatinas. Seguimiento < 3 meses en 5,9 % de los pacientes.

23
Pacientes dislipémicos y objetivos terapéuticos: Estudio HISPALIPID
Ref 11 pg420 abstract Determinar la prevalencia de dislipemia en los pacientes que acuden a consultas médicas ambulatorias en el Sistema Sanitario Español (SSE), así como el manejo terapéutico y el uso de hipolipemiantes de esta población MÉTODOS Estudio epidemiológico transversal, en el que participaron 1689 médicos (79% Atención Primaria y 21% Atención Especializada: Cardiólogos, Internistas ó Endocrinólogos ) Se obtuvieron datos de 8256 pacientes diagnosticados de dislipemia (24,3% de la población total vista en consultas, n =33913) Diapositiva 12: PACIENTES DISLIPÉMICOS Y OBJETIVOS TERAPÉUTICOS: ESTUDIO HISPALIPID Muy recientemente se han publicado los resultados del estudio Hispalipid cuyo objetivo fue estudiar la prevalencia de la dislipemia en los pacientes atendidos en el Sistema Sanitario Español (SSE) y evaluar el grado de control de esta población.11 Se realizó un estudio transversal a nivel nacional, en el que participaron 1689 médicos (79% Atención Primaria y 21% Atención Especializada: Cardiólogos, Internistas o Endocrinólogos). Se obtuvieron datos de 8256 pacientes que estaban diagnosticados de dislipemia (24,3% de la población total vista en consultas, n=33913). La edad media de los pacientes dislipémicos fue 62,4+12 años y el 52,4% era mujeres. El 73% de los pacientes estaban en tratamiento farmacológico hipolipemiante (91% con estatinas). De los pacientes con alto riesgo cardiovascular, tan sólo el 15,1% estaba controlado, frente al 29,6% de los de riesgo medio y el 58,5% de bajo riesgo.11 Ref 11 pg421c2p4L1-4 pg421c2p3L1-5 pg422c1p3L1-2 y c2p1 L2-3 Banegas et al. The gap between dyslipidemia control perceived by physicians and objective control patterns in Spain. Atherosclerosis 2006(188):
, así como el manejo terapéutico y el uso de hipolipemiantes de esta población. MÉTODOS. Estudio epidemiológico transversal, en el que participaron 1689 médicos. (79% Atención Primaria y 21% Atención Especializada: Cardiólogos, Internistas ó Endocrinólogos ) Se obtuvieron datos de 8256 pacientes diagnosticados de. dislipemia (24,3% de la población total vista en consultas, n =33913) Diapositiva 12: PACIENTES DISLIPÉMICOS Y OBJETIVOS TERAPÉUTICOS: ESTUDIO HISPALIPID. Muy recientemente se han publicado los resultados del estudio Hispalipid cuyo objetivo fue estudiar la prevalencia de la dislipemia en los pacientes atendidos en el Sistema Sanitario Español (SSE) y evaluar el grado de control de esta población.11. Se realizó un estudio transversal a nivel nacional, en el que participaron 1689 médicos (79% Atención Primaria y 21% Atención Especializada: Cardiólogos, Internistas o Endocrinólogos). Se obtuvieron datos de 8256 pacientes que estaban diagnosticados de dislipemia (24,3% de la población total vista en consultas, n=33913). La edad media de los pacientes dislipémicos fue 62,4+12 años y el 52,4% era mujeres. El 73% de los pacientes estaban en tratamiento farmacológico hipolipemiante (91% con estatinas). De los pacientes con alto riesgo cardiovascular, tan sólo el 15,1% estaba controlado, frente al 29,6% de los de riesgo medio y el 58,5% de bajo riesgo.11. Ref 11 pg421c2p4L1-4. pg421c2p3L1-5. pg422c1p3L1-2 y c2p1. L2-3. Banegas et al. The gap between dyslipidemia control perceived by physicians and objective control patterns in Spain. Atherosclerosis 2006(188):")
24
Control Dislipemia en Consultas (NCEP-ATPIII)
Estudio HISPALIPID: Control de la dislipemia en los distintos Grupos de Riesgo Control Dislipemia en Consultas (NCEP-ATPIII) 58,5% Ref 11 pg423 Tabla 1 50% (p<0,001) 29,6% R Bajo n=1804 % Control R Moderado n=1407 25% 15,1% R Alto n=2372 Diapositiva 13: ESTUDIO HISPALIPID: CONTROL DE LA DISLIPEMIA EN GLOBAL Y EN EL GRUPO DE ALTO RIESGO Una vez analizado los datos según los distintos grupos de riesgo, se puede destacar que aunque el grado de tratamiento farmacológico de la dislipemia en las consultas españolas es elevado, el control según directrices del ATP III es bajo (sólo uno de cada tres de forma global y uno de cada seis en prevención secundaria). Por tanto, existe un amplio margen de mejora en el control de la dislipemia, siendo necesario investigar sus determinantes.11 Otro dato obtenido fue que no hubo diferencias significativas en el control objetivo entre Atención Primaria y Especialistas (33,2% vs 31,3%, p<0,05).11 Ref 11Pg 422 c2p2L6-12 0% R Bajo R. Moderado R. Alto El control objetivo de la dislipemia en España es bajo en los pacientes de factores de riesgo más elevado Banegas et al. The gap between dyslipidemia control perceived by physicians and objective control patterns in Spain. Atherosclerosis 2006(188):
 58,5% Ref 11 pg423. Tabla 1. 50% (p<0,001) 29,6% R Bajo n=1804. % Control. R Moderado n= % 15,1% R Alto n=2372. Diapositiva 13: ESTUDIO HISPALIPID: CONTROL DE LA DISLIPEMIA EN GLOBAL Y EN EL GRUPO DE ALTO RIESGO. Una vez analizado los datos según los distintos grupos de riesgo, se puede destacar que aunque el grado de tratamiento farmacológico de la dislipemia en las consultas españolas es elevado, el control según directrices del ATP III es bajo (sólo uno de cada tres de forma global y uno de cada seis en prevención secundaria). Por tanto, existe un amplio margen de mejora en el control de la dislipemia, siendo necesario investigar sus determinantes.11. Otro dato obtenido fue que no hubo diferencias significativas en el control objetivo entre Atención Primaria y Especialistas (33,2% vs 31,3%, p<0,05).11. Ref 11Pg 422 c2p2L % R Bajo. R. Moderado. R. Alto. El control objetivo de la dislipemia en España es bajo en los pacientes de factores de riesgo más elevado. Banegas et al. The gap between dyslipidemia control perceived by physicians and objective control patterns in Spain. Atherosclerosis 2006(188):")
25
Estudio HISPALIPID: Control objetivo y subjetivo de la dislipemia en los pacientes de Alto Riesgo
Ref 11 pg 423 tabla 1 50% 41,6% 40% 30% 15,1% 20% N=2372 Diapositiva 14: ESTUDIO HISPALIPID: CONTROL DE LA DISLIPEMIA EN GLOBAL Y EN EL GRUPO DE ALTO RIESGO De esta diapositiva se puede comentar que globalmente, los médicos consideraron que el 41,6% de los pacientes con enfermedad coronaria o riesgo equivalente (N=2372) mostraba un control adecuado de la dislipemia (control subjetivo), mientras que siguiendo las recomendaciones del NCEP ATP III, solo el 15,1% de estos pacientes dislipémicos de alto riesgo estaba bien controlado (control objetivo).11 En definitiva los médicos sobreestimaron el control de los dislipémicos de alto riesgo (según ATP-III): control objetivo 15% vs control subjetivo 41%. Estos datos son consistentes con los de estudios previos, como veremos más adelante. 10% Ref 11 pg 423 tabla 1 0% Control subjetivo Control objetivo* * Según NCEP-ATPIII Los médicos sobreestimaron el control de los dislipémicos de alto riesgo (según ATP-III): control objetivo: 15% vs. control subjetivo: 41% Banegas et al. The gap between dyslipidemia control perceived by physicians and objective control patterns in Spain. Atherosclerosis 2006(188):
 mostraba un control adecuado de la dislipemia (control subjetivo), mientras que siguiendo las recomendaciones del NCEP ATP III, solo el 15,1% de estos pacientes dislipémicos de alto riesgo estaba bien controlado (control objetivo).11. En definitiva los médicos sobreestimaron el control de los dislipémicos de alto riesgo (según ATP-III): control objetivo 15% vs control subjetivo 41%. Estos datos son consistentes con los de estudios previos, como veremos más adelante. 10% Ref 11 pg 423 tabla 1. 0% Control subjetivo. Control objetivo* * Según NCEP-ATPIII. Los médicos sobreestimaron el control de los dislipémicos de alto riesgo (según ATP-III): control objetivo: 15% vs. control subjetivo: 41% Banegas et al. The gap between dyslipidemia control perceived by physicians and objective control patterns in Spain. Atherosclerosis 2006(188):")
26
Aumentar el HDL. Resultados iniciales con fármacos
Mechanism of reverse cholesterol transport (RCT). First step in RCT is efflux of phospholipid and free cholesterol from cell membrane to lipid-poor apoA-I, which acts as initial cholesterol acceptor, mediated by ATP binding cassette (ABC) A-1. This leads to formation of nascent HDL (pre-ß HDL). Transferred free cholesterol is then esterified by lecithin:cholesterol acyltransferase (LCAT) into cholesteryl esters (CE) that move into core of HDL particle, converting nascent HDL into spherical plasma HDL. CETP then modulates transfer of CE to VLDL and LDL in exchange for triglyceride. CE is delivered to liver for biliary excretion in 2 ways. CE in HDL particle is taken up selectively by scavenger receptor (SRB-1), whereas that in apoB particles is taken up by LDL receptor (LDL-R). During RCT, group of lipases, including hepatic lipase (HL), lipoprotein lipase (LPL), and endothelial lipase (EL) participate in modifying size and density of HDL molecule. Thus, RCT is complex process in which CETP is only one factor. Figure and text adapted with permission from the excellent clinical review of RCT by Rader.60 Consequently, other less clinically developed methods of altering RCT could prove to be more effective than CETP inhibition. Strategies currently under intense investigation include upregulation of ABC A-1 and SRB-I receptor.For more information about the following terms, which are not mentioned in the text of the present article, see von Eckardstein et al,27 Borggreve et al,28 Ma et al,29 and Cilingiroglu and Ballantyne.30 ABC A-1: adenosine triphosphate binding cassette, the initiator of cholesterol efflux from the cell membrane. SR-BI: scavenger receptor class B-1, the receptor responsible for uptake of cholesterol ester from the HDL particle when it arrives in the liver. LCAT: lecithin cholesterol acyl transferase; the enzyme responsible for esterifying cholesterol after it is carried from the cell membrane. HL: hepatic lipase, which hydrolyzes HDL triglyceride and phospholipids remodeling larger HDL particles to smaller HDL particles. The smaller HDL particles are at greater risk of renal catabolism. EL: endothelial lipase, which like HL remodels HDL to smaller particles. LPL: lipoprotein lipase, which contributes to HDL formation by generating phospholipids on apoB-containing lipoproteins that are then transferred to HDL. Secretory phospholipase A2: a lipase that remodels HDL to smaller particles. Duffy, D., Rader, D. J.. Emerging Therapies Targeting High-Density Lipoprotein Metabolism and Reverse Cholesterol Transport. Circulation :
. First step in RCT is efflux of phospholipid and free cholesterol from cell membrane to lipid-poor apoA-I, which acts as initial cholesterol acceptor, mediated by ATP binding cassette (ABC) A-1. This leads to formation of nascent HDL (pre-ß HDL). Transferred free cholesterol is then esterified by lecithin:cholesterol acyltransferase (LCAT) into cholesteryl esters (CE) that move into core of HDL particle, converting nascent HDL into spherical plasma HDL. CETP then modulates transfer of CE to VLDL and LDL in exchange for triglyceride. CE is delivered to liver for biliary excretion in 2 ways. CE in HDL particle is taken up selectively by scavenger receptor (SRB-1), whereas that in apoB particles is taken up by LDL receptor (LDL-R). During RCT, group of lipases, including hepatic lipase (HL), lipoprotein lipase (LPL), and endothelial lipase (EL) participate in modifying size and density of HDL molecule. Thus, RCT is complex process in which CETP is only one factor. Figure and text adapted with permission from the excellent clinical review of RCT by Rader.60 Consequently, other less clinically developed methods of altering RCT could prove to be more effective than CETP inhibition. Strategies currently under intense investigation include upregulation of ABC A-1 and SRB-I receptor.For more information about the following terms, which are not mentioned in the text of the present article, see von Eckardstein et al,27 Borggreve et al,28 Ma et al,29 and Cilingiroglu and Ballantyne.30 ABC A-1: adenosine triphosphate binding cassette, the initiator of cholesterol efflux from the cell membrane. SR-BI: scavenger receptor class B-1, the receptor responsible for uptake of cholesterol ester from the HDL particle when it arrives in the liver. LCAT: lecithin cholesterol acyl transferase; the enzyme responsible for esterifying cholesterol after it is carried from the cell membrane. HL: hepatic lipase, which hydrolyzes HDL triglyceride and phospholipids remodeling larger HDL particles to smaller HDL particles. The smaller HDL particles are at greater risk of renal catabolism. EL: endothelial lipase, which like HL remodels HDL to smaller particles. LPL: lipoprotein lipase, which contributes to HDL formation by generating phospholipids on apoB-containing lipoproteins that are then transferred to HDL. Secretory phospholipase A2: a lipase that remodels HDL to smaller particles. Duffy, D., Rader, D. J.. Emerging Therapies Targeting High-Density Lipoprotein Metabolism and Reverse Cholesterol Transport. Circulation :")
27
Effect of ACAT Inhibition on the Progression of Coronary Atherosclerosis (ACTIVATE trial)
Steven E. Nissen, M.D., E. Murat Tuzcu, M.D., H. Bryan Brewer, M.D., Ilke Sipahi, M.D., Stephen J. Nicholls, M.B., B.S., Ph.D., Peter Ganz, M.D., Paul Schoenhagen, M.D., David D. Waters, M.D., Carl J. Pepine, M.D., Tim D. Crowe, B.S., Michael H. Davidson, M.D., John E. Deanfield, M.D., Lisa M. Wisniewski, R.N., James J. Hanyok, Pharm.D. and Laurent M. Kassalow, M.S. N Engl J Med Volume 354;12: March 23, 2006

28
Existen dos formas de esta enzima:
Localizacion y funcion de la enzima Acyl-Coenzyme A:Cholesterol Acyltransferase (ACAT) ACAT (Acyl-CoA:Cholesterol Acetyl Transferase) es responsable de la esterificacion del colesterol en los tejidos. Existen dos formas de esta enzima: ACAT 1 esterifica colesterol libre en macrofagos. ACAT 2 actua sobre el colesterol libre en celulas intestinales y hepatocitos. Approaches that target arterial plaque through the use of acyl–coenzyme A:cholesterol acyltransferase (ACAT) inhibitors have been investigated experimentally for two decades. ACAT inhibitors interfere with intracellular cholesterol transport within plaque macrophages and may delay the formation of foam cells while activating reverse cholesterol transport.1 There are at least two forms of this intracellular enzyme. ACAT2 esterifies the free cholesterol that will form the core of lipoproteins assembled in hepatocytes and intestinal epithelium, ACAT1 esterifies free cholesterol so that it can be stored as cholesteryl ester droplets in macrophages.2 Inhibition of ACAT2 may reduce plasma cholesterol levels, whereas inhibition of ACAT1 may reduce the cholesterol burden in plaque macrophages. Nissen, S. et al. N Engl J Med 2006;354:
 ACAT (Acyl-CoA:Cholesterol Acetyl Transferase) es responsable de la esterificacion del colesterol en los tejidos. Existen dos formas de esta enzima: ACAT 1 esterifica colesterol libre en macrofagos. ACAT 2 actua sobre el colesterol libre en celulas intestinales y hepatocitos. Approaches that target arterial plaque through the use of acyl–coenzyme A:cholesterol acyltransferase (ACAT) inhibitors have been investigated experimentally for two decades. ACAT inhibitors interfere with intracellular cholesterol transport within plaque macrophages and may delay the formation of foam cells while activating reverse cholesterol transport.1. There are at least two forms of this intracellular enzyme. ACAT2 esterifies the free cholesterol that will form the core of lipoproteins assembled in hepatocytes and intestinal epithelium, ACAT1 esterifies free cholesterol so that it can be stored as cholesteryl ester droplets in macrophages.2. Inhibition of ACAT2 may reduce plasma cholesterol levels, whereas inhibition of ACAT1 may reduce the cholesterol burden in plaque macrophages. Nissen, S. et al. N Engl J Med 2006;354:")
29
ACTIVATE Trial 408 pacientes con evidencia angiografica de enfermedad coronaria recibieron tratamiento habitual (incluyendo estatinas) y randomizados a placebo o pactimibe. Pactimibe es un inhibidor no selectivo de la ACAT El % de los pacientes recibieron tratamiento con estatinas, y su LDL medio al final del estudio fue de 90 mg/dl. El end-point primario del estudio fue la modificación en el % del volumen de ateroma por IVUS. Nissen, S. et al. N Engl J Med 2006;354:
 y randomizados a placebo o pactimibe. Pactimibe es un inhibidor no selectivo de la ACAT. El % de los pacientes recibieron tratamiento con estatinas, y su LDL medio al final del estudio fue de 90 mg/dl. El end-point primario del estudio fue la modificación en el % del volumen de ateroma por IVUS. Nissen, S. et al. N Engl J Med 2006;354:")
30
Medidas por IVUS basalmente y tras fin del estudio
Nissen, S. et al. N Engl J Med 2006;354:

31
Efectos adversos Nissen, S. et al. N Engl J Med 2006;354:

32
Tiempo hasta el primer evento cardiovascular.
Nissen, S. et al. N Engl J Med 2006;354:

33
Conclusion En pacientes con enfermedad coronaria, el tratamiento con inhibidores ACAT bloqueo la regresion de la placa apreciada en el grupo placebo. No se aprecio un aumento de eventos cardiovasculares.

34
Efecto no intencionado de la inhibicion de la Acyl-Coenzyme A:Cholesterol Acyltransferase (ACAT)
In Panel A, the arterial macrophage transports incoming lipoprotein cholesterol as part of a cycle of interconversion of free cholesterol and cholesteryl ester controlled by ACAT and cholesteryl ester hydrolase (CEH). Liberated free cholesterol can be exported to high-density lipoprotein (HDL). Excess cholesteryl ester is stored in lipid droplets. In Panel B, the inhibition of ACAT (red X) increases free cholesterol levels and reduces the levels of cholesteryl ester, thus activating efflux and limiting storage. In Panel C, the continued inhibition of ACAT increases free cholesterol levels and limits the efflux of free cholesterol, thus inducing cytotoxic effects. the HDL pathway are more complex than we originally thought; the excess free cholesterol produced by blocking ACAT is not readily available for export and may accumulate in the macrophage above the toxic threshold (Fig. 1). This could be the consequence of the compartmentalization of free cholesterol to sites disconnected from the efflux machinery, dysfunction of the efflux machinery caused by stiffening of the plasma membrane, or the presence of relatively low levels of extracellular cholesterol acceptors in the atheroma. For cholesterol to exit the cell, an acceptor must be present on the other side of the membrane. Apolipoprotein A-I, the HDL protein, is a physiologic cholesterol acceptor. Limited access of plasma-derived apolipoprotein A-I to the growing atheroma may result in inefficient elimination of cellular cholesterol, even when conditions are ripe for export. Fazio S and Linton M. N Engl J Med 2006;354:
. Liberated free cholesterol can be exported to high-density lipoprotein (HDL). Excess cholesteryl ester is stored in lipid droplets. In Panel B, the inhibition of ACAT (red X) increases free cholesterol levels and reduces the levels of cholesteryl ester, thus activating efflux and limiting storage. In Panel C, the continued inhibition of ACAT increases free cholesterol levels and limits the efflux of free cholesterol, thus inducing cytotoxic effects. the HDL pathway are more complex than we originally. thought; the excess free cholesterol produced. by blocking ACAT is not readily available. for export and may accumulate in the macrophage. above the toxic threshold (Fig. 1). This could be. the consequence of the compartmentalization of. free cholesterol to sites disconnected from the. efflux machinery, dysfunction of the efflux machinery. caused by stiffening of the plasma membrane, or the presence of relatively low levels of. extracellular cholesterol acceptors in the atheroma. For cholesterol to exit the cell, an acceptor. must be present on the other side of the membrane. Apolipoprotein A-I, the HDL protein, is a. physiologic cholesterol acceptor. Limited access. of plasma-derived apolipoprotein A-I to the growing. atheroma may result in inefficient elimination. of cellular cholesterol, even when conditions. are ripe for export. Fazio S and Linton M. N Engl J Med 2006;354:")
35
Otras estrategias para aumentar HDL
Schematic Model of Reverse Cholesterol Transport Mediated by High-Density Lipoprotein (HDL), Resulting in an Increase in the Plasma HDL Level. Triglycerides and cholesterol are transported by chylomicrons and remnant lipoproteins from the intestine and by very-low-density lipoproteins (VLDL) and low-density lipoproteins (LDL) from the liver (white arrows). Apolipoprotein A-I (apoA-I) is synthesized by the liver and, after interaction with hepatic ATP-binding cassette transporter 1 (ABCA1), is secreted into plasma as lipid-poor apolipoprotein A-I (yellow arrow). In reverse cholesterol transport, newly synthesized lipid-poor apolipoprotein A-I interacts with ABCA1, removing excess cellular cholesterol and forming pre- -HDL (green arrow). Pre- -HDL is converted into mature -HDL by lecithin–cholesterol acyltransferase (LCAT, black arrow). HDL cholesterol is returned to the liver through two pathways: selective uptake of cholesterol by the hepatic scavenger receptor, class B, type I (SR-BI, blue arrow), or the transfer of cholesteryl ester by cholesteryl ester transfer protein (CETP) to VLDL–LDL, with uptake by the liver through the LDL receptor (red arrows). Short-term HDL therapy to increase the HDL level and potentially provide protection against cardiovascular events can be achieved with the infusion of complexes consisting of apolipoprotein A-I Milano and phospholipids. Long-term increases in the HDL level and reductions in the LDL level result from the partial inhibition of CETP. FC denotes free cholesterol, PL phospholipids, LRP LDL-related protein, and LPL lipoprotein lipase.
, Resulting in an Increase in the Plasma HDL Level. Triglycerides and cholesterol are transported by chylomicrons and remnant lipoproteins from the intestine and by very-low-density lipoproteins (VLDL) and low-density lipoproteins (LDL) from the liver (white arrows). Apolipoprotein A-I (apoA-I) is synthesized by the liver and, after interaction with hepatic ATP-binding cassette transporter 1 (ABCA1), is secreted into plasma as lipid-poor apolipoprotein A-I (yellow arrow). In reverse cholesterol transport, newly synthesized lipid-poor apolipoprotein A-I interacts with ABCA1, removing excess cellular cholesterol and forming pre- -HDL (green arrow). Pre- -HDL is converted into mature -HDL by lecithin–cholesterol acyltransferase (LCAT, black arrow). HDL cholesterol is returned to the liver through two pathways: selective uptake of cholesterol by the hepatic scavenger receptor, class B, type I (SR-BI, blue arrow), or the transfer of cholesteryl ester by cholesteryl ester transfer protein (CETP) to VLDL–LDL, with uptake by the liver through the LDL receptor (red arrows). Short-term HDL therapy to increase the HDL level and potentially provide protection against cardiovascular events can be achieved with the infusion of complexes consisting of apolipoprotein A-I Milano and phospholipids. Long-term increases in the HDL level and reductions in the LDL level result from the partial inhibition of CETP. FC denotes free cholesterol, PL phospholipids, LRP LDL-related protein, and LPL lipoprotein lipase.")
36
ILLUMINATE Trial Este estudio randomizo 15,000 pacientes a la combinación de torcetrapib y atorvastatina frente a atorvastatina solo. El estudio fue suspendido por apreciarse 82 muertes en el brazo de torcetrapib/atorvastatina frente a 51 en el grupo de monoterapia con atorvastatina. Se había previamente comunicado un aumento de TA en pacientes randomizados a torcetrapib , aunque se desconoce aun si el efecto sobre la TA es el mecanismo del aumento de las muertes en el grupo con torcetrapib.

37
Otros estudios. Otras cuestiones
MEGA Trial. Estatinas e Insuficiencia Cardiaca. Estatinas y sepsis. Estatinas y arritmias. Estudio Vytal

38
MEGA trial. Estudio japonés prospectivo, randomizado, ciego, en pacientes con hipercolesterolemia (CT 5·69–6·98 mmol/L) sin historia de CI o ACV asignado a dieta o dieta mas Pravastatina 10-20mg Endpoint primario fue la aparición de enfermedad coronaria Reducción 33 % la incidencia de cardiopatía isquémica Diferencias en la respuesta según razas¿¿ Summary Background Evidence-based treatment for hypercholesterolaemia in Japan has been hindered by the lack of direct evidence in this population. Our aim was to assess whether evidence for treatment with statins derived from western populations can be extrapolated to the Japanese population. Methods In this prospective, randomised, open-labelled, blinded study, patients with hypercholesterolaemia (total cholesterol 5·69–6·98 mmol/L) and no history of coronary heart disease or stroke were randomly assigned diet or diet plus 10–20 mg pravastatin daily. The primary endpoint was the . rst occurrence of coronary heart disease. Statistical analyses were done by intention to treat. This trial is registered at ClinicalTrials.gov, number NCT Findings 3966 patients were randomly assigned to the diet group and 3866 to the diet plus pravastatin group. Mean follow-up was 5·3 years. At the end of study, 471 and 522 patients had withdrawn, died, or been lost to follow-up in the diet and diet plus pravastatin groups, respectively. Mean total cholesterol was reduced by 2·1% (from 6·27 mmol/L to 6·13 mmol/L) and 11·5% (from 6·27 mmol/L to 5·55 mmol/L) and mean LDL cholesterol by 3·2% (from 4·05 mmol/L to 3·90 mmol/L) and 18·0% (from 4·05 mmol/L to 3·31 mmol/L) in the diet and the diet plus pravastatin groups, respectively. Coronary heart disease was signi. cantly lower in the diet plus pravastatin group than in the diet alone group (66 events vs 101 events; HR 0·67, 95% CI 0·49–0·91; p=0·01). There was no di. erence in the incidence of malignant neoplasms or other serious adverse events between the two groups. Interpretation Treatment with a low dose of pravastatin reduces the risk of coronary heart disease in Japan by much the same amount as higher doses have shown in Europe and the USA. People from China, Japan, and Korea should be prescribed lower starting doses of statins than Caucasians, a researcher recommends, after noting that East Asians frequently have heightened responses to therapeutic drugs. "Typically, Asians achieve similar benefits [to] Westerners at lower statin doses," states James Liao, from Brigham and Women's Hospital in Cambridge, Massachusetts, USA. "In a comparison of atorvastatin and simvastatin in dyslipidemic patients at six Asian centers, just 10 mg of simvastatin and 10 mg of atorvastatin over 8 weeks resulted in average low-density lipoprotein cholesterol reductions of 35% and 43%, respectively." Furthermore, the Management of Elevated Cholesterol in the Primary Prevention of Adult Japanese (MEGA) study of 7800 Japanese patients with hypercholesterolemia but no cardiovascular disease (CVD) revealed a 33% reduction in the risk of coronary heart disease when low dose mg pravastatin was added to dietary intervention. Variants in gene structure can influence a drug's pharmacokinetic or pharmacodynamic properties, says Liao. Of the pharmacokinetic phases of absorption, distribution, metabolism, and excretion, the clinician notes that metabolism is most subject to interpatient and interethnic variability. Differences between East Asians and Caucasians are particularly noteworthy in the metabolic activity of cytochrome (CY)P450 2D6 and the CYP450 2C subfamily, and allelic frequencies of CYP450 3A also differ between Asians and Whites. Variations in the activity of the transmembrane drug efflux pump P-glycoprotein and polymorphisms in genes encoding organic anion transporting polypeptides may also have effects. "The proved efficacy of statins in reducing risk for CVD in Asians, along with their proved safety in Asian populations, amply justifies their use in Asians and subjects of Asian descent," he stresses in the American Journal of Cardiology. However, he adds: "It may be advisable… to initiate therapy with the older as well as the newer statins at low doses in Asian and Asian-American patients." Lancet 2006; 368: 1155–63
 sin historia de CI o ACV asignado a dieta o dieta mas Pravastatina 10-20mg. Endpoint primario fue la aparición de enfermedad coronaria. Reducción 33 % la incidencia de cardiopatía isquémica. Diferencias en la respuesta según razas¿¿ Summary. Background Evidence-based treatment for hypercholesterolaemia in Japan has been hindered by the lack of direct. evidence in this population. Our aim was to assess whether evidence for treatment with statins derived from. western populations can be extrapolated to the Japanese population. Methods In this prospective, randomised, open-labelled, blinded study, patients with hypercholesterolaemia (total. cholesterol 5·69–6·98 mmol/L) and no history of coronary heart disease or stroke were randomly assigned diet or. diet plus 10–20 mg pravastatin daily. The primary endpoint was the . rst occurrence of coronary heart disease. Statistical analyses were done by intention to treat. This trial is registered at ClinicalTrials.gov, number. NCT Findings 3966 patients were randomly assigned to the diet group and 3866 to the diet plus pravastatin group. Mean follow-up was 5·3 years. At the end of study, 471 and 522 patients had withdrawn, died, or been lost to. follow-up in the diet and diet plus pravastatin groups, respectively. Mean total cholesterol was reduced by 2·1% (from 6·27 mmol/L to 6·13 mmol/L) and 11·5% (from 6·27 mmol/L to 5·55 mmol/L) and mean LDL cholesterol. by 3·2% (from 4·05 mmol/L to 3·90 mmol/L) and 18·0% (from 4·05 mmol/L to 3·31 mmol/L) in the diet and. the diet plus pravastatin groups, respectively. Coronary heart disease was signi. cantly lower in the diet plus. pravastatin group than in the diet alone group (66 events vs 101 events; HR 0·67, 95% CI 0·49–0·91; p=0·01). There was no di. erence in the incidence of malignant neoplasms or other serious adverse events between the. two groups. Interpretation Treatment with a low dose of pravastatin reduces the risk of coronary heart disease in Japan by much. the same amount as higher doses have shown in Europe and the USA. People from China, Japan, and Korea should be prescribed lower starting doses of statins than Caucasians, a researcher recommends, after noting that East Asians frequently have heightened responses to therapeutic drugs. Typically, Asians achieve similar benefits [to] Westerners at lower statin doses, states James Liao, from Brigham and Women s Hospital in Cambridge, Massachusetts, USA. In a comparison of atorvastatin and simvastatin in dyslipidemic patients at six Asian centers, just 10 mg of simvastatin and 10 mg of atorvastatin over 8 weeks resulted in average low-density lipoprotein cholesterol reductions of 35% and 43%, respectively. Furthermore, the Management of Elevated Cholesterol in the Primary Prevention of Adult Japanese (MEGA) study of 7800 Japanese patients with hypercholesterolemia but no cardiovascular disease (CVD) revealed a 33% reduction in the risk of coronary heart disease when low dose mg pravastatin was added to dietary intervention. Variants in gene structure can influence a drug s pharmacokinetic or pharmacodynamic properties, says Liao. Of the pharmacokinetic phases of absorption, distribution, metabolism, and excretion, the clinician notes that metabolism is most subject to interpatient and interethnic variability. Differences between East Asians and Caucasians are particularly noteworthy in the metabolic activity of cytochrome (CY)P450 2D6 and the CYP450 2C subfamily, and allelic frequencies of CYP450 3A also differ between Asians and Whites. Variations in the activity of the transmembrane drug efflux pump P-glycoprotein and polymorphisms in genes encoding organic anion transporting polypeptides may also have effects. The proved efficacy of statins in reducing risk for CVD in Asians, along with their proved safety in Asian populations, amply justifies their use in Asians and subjects of Asian descent, he stresses in the American Journal of Cardiology. However, he adds: It may be advisable… to initiate therapy with the older as well as the newer statins at low doses in Asian and Asian-American patients. Lancet 2006; 368: 1155–63.")
39
Estudio Vytal Estudio de eficacia y seguridad de Ezetimibe/Simvastatina vs Atorvastatina. Randomizado, doble ciego, 1229 pac. End-points. % cambio LDL y % pac con LDL< 70 OBJECTIVE: To compare the efficacy and safety of the recommended usual starting and next highest doses of ezetimibe/ simvastatin and atorvastatin in patients with type 2 diabetes mellitus and hypercholesterolemia. PATIENTS AND METHODS: This double-blind, multicenter study (June 22 to December 7, 2005) consisted of adult patients randomized to the recommended usual starting (ezetimibe/simvastatin, 10/20 mg/d, vs atorvastatin, 10 or 20 mg/d) or next highest (ezetimibe/simvastatin, 10/40 mg/d, vs atorvastatin, 40 mg/d) doses. Efficacy end points included percent changes from baseline in low-density lipoprotein cholesterol (LDL-C) levels (primary) and proportion of patients attaining LDL-C levels less than 70 mg/dL (secondary). RESULTS: A total of 1229 patients participated in the study. Significantly greater mean reductions were found in LDL-C levels with ezetimibe/simvastatin, 10/20 mg/d (–53.6%; 95% confidence interval [CI], –55.4% to –51.8%), than with atorvastatin, 10 mg/d (–38.3%; 95% CI, –40.1% to –36.5%; P<.001))or 20 mg/d (–44.6%; 95% CI, –46.4% to –42.8%; P<.001), and with ezetimibe/simvastatin, 10/40 mg/d (–57.6%; 95% CI, –59.4% to –55.8%), vs atorvastatin, 40 mg/d (–50.9%; 95% CI, –52.7% to –49.1%; P<.001). Ezetimibe/simvastatin was also superior to atorvastatin in attainment of LDL-C levels less than 70 mg/dL ( P<.001 for all dose comparisons). Significantly better improvements with ezetimibe/simvastatin than with atorvastatin ( P≤.001) were observed for total cholesterol, high-density lipoprotein cholesterol, and non–high-density lipoprotein cholesterol. Ezetimibe/ simvastatin, 10/20 mg/d, reduced high-sensitivity C-reactive protein and triglyceride levels significantly more than atorvastatin, 10 mg/d ( P=.02), with comparable reductions at other doses. Incidences of clinical adverse events, including serious drug-related and prespecified gastrointestinal-, gallbladder-, and hepatitis-related allergic reactions or rash events, and laboratory adverse events, including repeated elevation of hepatic transaminases or creatine kinase levels, were similar for both treatments. CONCLUSION: Ezetimibe/simvastatin provided additional lipidmodifying benefits over atorvastatin monotherapy at the recommended usual starting and next highest doses in patients with type 2 diabetes. Both treatments were generally well tolerated. Mayo Clin Proc. 2006;81(12): Mayo Clin Proc. 2006;81(12):
 consisted of adult patients randomized. to the recommended usual starting (ezetimibe/simvastatin, 10/20 mg/d, vs atorvastatin, 10 or 20 mg/d) or next highest. (ezetimibe/simvastatin, 10/40 mg/d, vs atorvastatin, 40 mg/d) doses. Efficacy end points included percent changes from baseline. in low-density lipoprotein cholesterol (LDL-C) levels (primary) and. proportion of patients attaining LDL-C levels less than 70 mg/dL. (secondary). RESULTS: A total of 1229 patients participated in the study. Significantly greater mean reductions were found in LDL-C levels. with ezetimibe/simvastatin, 10/20 mg/d (–53.6%; 95% confidence. interval [CI], –55.4% to –51.8%), than with atorvastatin, 10. mg/d (–38.3%; 95% CI, –40.1% to –36.5%; P<.001))or 20 mg/d. (–44.6%; 95% CI, –46.4% to –42.8%; P<.001), and with. ezetimibe/simvastatin, 10/40 mg/d (–57.6%; 95% CI, –59.4% to –55.8%), vs atorvastatin, 40 mg/d (–50.9%; 95% CI, –52.7% to –49.1%; P<.001). Ezetimibe/simvastatin was also superior to. atorvastatin in attainment of LDL-C levels less than 70 mg/dL. ( P<.001 for all dose comparisons). Significantly better improvements. with ezetimibe/simvastatin than with atorvastatin ( P≤.001) were observed for total cholesterol, high-density lipoprotein cholesterol, and non–high-density lipoprotein cholesterol. Ezetimibe/ simvastatin, 10/20 mg/d, reduced high-sensitivity C-reactive protein. and triglyceride levels significantly more than atorvastatin, 10. mg/d ( P=.02), with comparable reductions at other doses. Incidences. of clinical adverse events, including serious drug-related. and prespecified gastrointestinal-, gallbladder-, and hepatitis-related. allergic reactions or rash events, and laboratory adverse. events, including repeated elevation of hepatic transaminases or. creatine kinase levels, were similar for both treatments. CONCLUSION: Ezetimibe/simvastatin provided additional lipidmodifying. benefits over atorvastatin monotherapy at the recommended. usual starting and next highest doses in patients with. type 2 diabetes. Both treatments were generally well tolerated. Mayo Clin Proc. 2006;81(12): Mayo Clin Proc. 2006;81(12):")
40
Estatinas y sepsis. Análisis de cohorte de población >65 a hospitalizados por SCA, ACV o revascularizacion Incidencia de sepsis fue menor en pacientes con tto con estatinas (HR 0.81) Summary Background Atherosclerosis and sepsis share several pathophysiological similarities, including immune dysregulation, increased thrombogenesis, and systemic in.ammation. The relation between statins and risk of sepsis in patients with atherosclerosis is unknown. Methods We did a population-based cohort analysis through linked administrative databases in Ontario, Canada, with accrual from 1997 to We identi.ed patients older than 65 years who had been hospitalised for an acute coronary syndrome, ischaemic stroke, or revascularisation, who survived for at least 3 months after discharge. (33%) were prescribed a statin within 90 days of discharge, (67%) were not. Propensity-based matching, which accounted for each individual’s likelihood of receiving a statin, yielded a cohort of patients, of whom half (34 584) received a statin and half (34 584) did not. Findings Incidence of sepsis was lower in patients receiving statins than in controls (71·2 vs 88·0 events per person-years; hazard ratio [HR] 0·81; 95% CI 0·72–0·91). Adjustment for demographic characteristics, sepsis risk factors, comorbidities, and health-care use gave similar results (HR 0·81; 95% CI 0·72–0·90). The protective association between statins and sepsis persisted in high-risk subgroups, including patients with diabetes mellitus, chronic renal failure, or a history of infections. Signi.cant reductions in severe sepsis (HR 0·83; 95% CI 0·70–0·97) and fatal sepsis (0·75; 0·61–0·93) were also observed. No bene.t was noted with non-statin lipid-lowering agents (0·95; 0·75–1·22). Implications Use of statins in patients with atherosclerosis is associated with a reduced risk of subsequent sepsis. Randomised trials of statins for prevention of sepsis are warranted. Lancet 2006; 367: 413–18
 Summary. Background Atherosclerosis and sepsis share several pathophysiological similarities, including immune. dysregulation, increased thrombogenesis, and systemic in.ammation. The relation between statins and risk of. sepsis in patients with atherosclerosis is unknown. Methods We did a population-based cohort analysis through linked administrative databases in Ontario, Canada, with accrual from 1997 to We identi.ed patients older than 65 years who had been hospitalised for an. acute coronary syndrome, ischaemic stroke, or revascularisation, who survived for at least 3 months after discharge (33%) were prescribed a statin within 90 days of discharge, (67%) were not. Propensity-based. matching, which accounted for each individual’s likelihood of receiving a statin, yielded a cohort of patients, of whom half (34 584) received a statin and half (34 584) did not. Findings Incidence of sepsis was lower in patients receiving statins than in controls (71·2 vs 88·0 events per person-years; hazard ratio [HR] 0·81; 95% CI 0·72–0·91). Adjustment for demographic characteristics, sepsis risk. factors, comorbidities, and health-care use gave similar results (HR 0·81; 95% CI 0·72–0·90). The protective. association between statins and sepsis persisted in high-risk subgroups, including patients with diabetes mellitus, chronic renal failure, or a history of infections. Signi.cant reductions in severe sepsis (HR 0·83; 95% CI 0·70–0·97) and fatal sepsis (0·75; 0·61–0·93) were also observed. No bene.t was noted with non-statin lipid-lowering agents. (0·95; 0·75–1·22). Implications. Use of statins in patients with atherosclerosis is associated with a reduced risk of subsequent sepsis. Randomised. trials of statins for prevention of sepsis are warranted. Lancet 2006; 367: 413–18.")
41
Estatinas y arritmias. Subestudio estudio DEFINITE (DAI en miocardiopatia dilatada no isquemica) El uso de estatinas se asocio a una reducción del 78 % en mortalidad. OBJECTIVES We sought to evaluate whether statins were associated with a survival benefit and significant attenuation in life-threatening arrhythmias in patients with nonischemic dilated cardiomyopathy. BACKGROUND Statins are associated with a reduction in appropriate implantable cardioverter-defibrillator (ICD) therapy in patients with coronary artery disease and improved clinical status in nonischemic dilated cardiomyopathy. METHODS The effect of statin use on time to death or resuscitated cardiac arrest and time to arrhythmic sudden death was evaluated in 458 patients enrolled in the DEFINITE (DEFIbrillators in Non-Ischemic cardiomyopathy Treatment Evaluation) study. The effect of statin use on time to first appropriate shock was analyzed only in the 229 patients who were randomized to ICD therapy. RESULTS The unadjusted hazard ratio (HR) for death among patients on versus those not on statin therapy was 0.22 (95% confidence interval [CI] 0.09 to 0.55; p ). When controlled for statin effects, ICD therapy was associated with improved survival (HR 0.61; 95% CI 0.38 to 0.99; p 0.04). There was one arrhythmic sudden death in the 110 patients receiving statin therapy (0.9%) versus 18 of 348 patients not receiving statins (5.2%; p 0.04). The unadjusted HR for arrhythmic sudden death among patients on versus those not on statin therapy was 0.16 (95% CI to 1.21; p 0.08). The HR for appropriate shocks among patients on versus those not on statin therapy was 0.78 (95% CI 0.34 to 1.82) after adjustment for baseline differences in the two groups. CONCLUSIONS Statin use in the DEFINITE study was associated with a 78% reduction in mortality. This reduction was caused, in part, by a reduction in arrhythmic sudden death. These findings should be confirmed in a prospective, randomized clinical trial. (J Am Coll Cardiol 2006; 48:1228 –33) © 2006 by the American College of Cardiology Foundation J Am Coll Cardiol 2006; 48:1228 –33
 therapy in patients with coronary artery disease and improved clinical status in. nonischemic dilated cardiomyopathy. METHODS The effect of statin use on time to death or resuscitated cardiac arrest and time to arrhythmic. sudden death was evaluated in 458 patients enrolled in the DEFINITE (DEFIbrillators in. Non-Ischemic cardiomyopathy Treatment Evaluation) study. The effect of statin use on time. to first appropriate shock was analyzed only in the 229 patients who were randomized to ICD. therapy. RESULTS The unadjusted hazard ratio (HR) for death among patients on versus those not on statin. therapy was 0.22 (95% confidence interval [CI] 0.09 to 0.55; p 0.001). When controlled. for statin effects, ICD therapy was associated with improved survival (HR 0.61; 95% CI to 0.99; p 0.04). There was one arrhythmic sudden death in the 110 patients receiving. statin therapy (0.9%) versus 18 of 348 patients not receiving statins (5.2%; p 0.04). The. unadjusted HR for arrhythmic sudden death among patients on versus those not on statin. therapy was 0.16 (95% CI to 1.21; p 0.08). The HR for appropriate shocks among. patients on versus those not on statin therapy was 0.78 (95% CI 0.34 to 1.82) after adjustment. for baseline differences in the two groups. CONCLUSIONS Statin use in the DEFINITE study was associated with a 78% reduction in mortality. This. reduction was caused, in part, by a reduction in arrhythmic sudden death. These findings. should be confirmed in a prospective, randomized clinical trial. (J Am Coll Cardiol 2006; 48:1228 –33) © 2006 by the American College of Cardiology Foundation. J Am Coll Cardiol 2006; 48:1228 –33.")
42
Estatinas y arritmias. Estudio Armyda-3
El uso de estatinas se asocio a una reducción de la incidencia de FA en pacientes post CCV con bomba. Reducción de riesgo de FA del 61 % y de la estancia media. Atrial fibrillation after cardiac surgery is a relatively common complication that may increase morbidity, length of hospital stay, and cost of care. ARMYDA-3 (Atorvastatin for Reduction of MYocardial Dysrhythmia After cardiac surgery) is the first randomized, controlled trial demonstrating that treatment with atorvastatin significantly reduces the incidence of new-onset postoperative atrial fibrillation and shortens length of stay in patients undergoing cardiac surgery with cardiopulmonary bypass. Administration of atorvastatin 40 mg/d starting 7 days before surgery reduced the risk of postoperative atrial fibrillation by 61% and reduced length of stay by 0.6 days. Whether the mechanism of benefit is due to an antiinflammatory effect is not known. These findings support the administration of atorvastatin to reduce atrial fibrillation in patients undergoing elective cardiac operations. Circulation. 2006;114:
 is the first randomized, controlled trial demonstrating that treatment with atorvastatin significantly reduces the incidence of new-onset postoperative atrial fibrillation and shortens length of stay in patients undergoing cardiac surgery with cardiopulmonary bypass. Administration of atorvastatin 40 mg/d starting 7 days before surgery reduced the risk of postoperative atrial fibrillation by 61% and reduced length of stay by 0.6 days. Whether the mechanism of benefit is due. to an antiinflammatory effect is not known. These findings support the administration of atorvastatin to reduce atrial fibrillation in patients undergoing elective cardiac operations. Circulation. 2006;114:")
43
Estatinas y arritmias. Subestudio MADIT-2
El uso de estatinas se asocio a una reducción del riesgo de muerte cardiaca y con una reducción de episodios de FV/TV Efecto antiarritmico de las estatinas?? OBJECTIVES We evaluated whether statins have anti-arrhythmic effects by exploring the association of statin use with appropriate implantable cardioverter-defibrillator (ICD) therapy for ventricular tachycardia/ventricular fibrillation (VT/VF) in the Multicenter Automatic Defibrillator Implantation Trial (MADIT)-II. BACKGROUND A few studies have suggested that lipid-lowering drugs may have anti-arrhythmic effects in patients with coronary artery disease. METHODS Patients receiving an ICD (n 654; U.S. centers only) in the MADIT-II study were categorized by the percentage of days each patient received statins during follow-up (90% to 100%, n 386; 11% to 89%, n 116; and 0% to 10%, n 152). The Kaplan-Meier method with significance testing by the log-rank statistic and time-dependent proportional hazards regression analysis were used to evaluate the effect of statin use on the probability of ICD therapy for the combined end point VT/VF or cardiac death and for the end point VT/VF. RESULTS The cumulative rate of ICD therapy for VT/VF or cardiac death, whichever occurred first, was significantly reduced in those with 90% statin usage compared to those with lower statin usage (p 0.01). The time-dependent statin:no statin therapy hazard ratio was 0.65 (p 0.01) for the end point of VT/VF or cardiac death and 0.72 (p ) for VT/VF after adjusting for relevant covariates. CONCLUSIONS Statin use in patients with an ICD was associated with a reduction in the risk of cardiac death or VT/VF, whichever occurred first, and was associated with a reduction in VT/VF episodes. These findings suggest that statins have anti-arrhythmic properties. (J Am Coll Cardiol 2006;47:769 –73) © 2006 by the American College of Cardiology Foundation . J Am Coll Cardiol ;47:769 –73
 therapy for ventricular. tachycardia/ventricular fibrillation (VT/VF) in the Multicenter Automatic Defibrillator. Implantation Trial (MADIT)-II. BACKGROUND A few studies have suggested that lipid-lowering drugs may have anti-arrhythmic effects in. patients with coronary artery disease. METHODS Patients receiving an ICD (n 654; U.S. centers only) in the MADIT-II study were. categorized by the percentage of days each patient received statins during follow-up (90% to. 100%, n 386; 11% to 89%, n 116; and 0% to 10%, n 152). The Kaplan-Meier method. with significance testing by the log-rank statistic and time-dependent proportional hazards. regression analysis were used to evaluate the effect of statin use on the probability of ICD. therapy for the combined end point VT/VF or cardiac death and for the end point VT/VF. RESULTS The cumulative rate of ICD therapy for VT/VF or cardiac death, whichever occurred first, was significantly reduced in those with 90% statin usage compared to those with lower. statin usage (p 0.01). The time-dependent statin:no statin therapy hazard ratio was (p 0.01) for the end point of VT/VF or cardiac death and 0.72 (p 0.046) for VT/VF after. adjusting for relevant covariates. CONCLUSIONS Statin use in patients with an ICD was associated with a reduction in the risk of cardiac death. or VT/VF, whichever occurred first, and was associated with a reduction in VT/VF episodes. These findings suggest that statins have anti-arrhythmic properties. (J Am Coll Cardiol. 2006;47:769 –73) © 2006 by the American College of Cardiology Foundation. . J Am Coll Cardiol 2006;47:769 –73.")
44
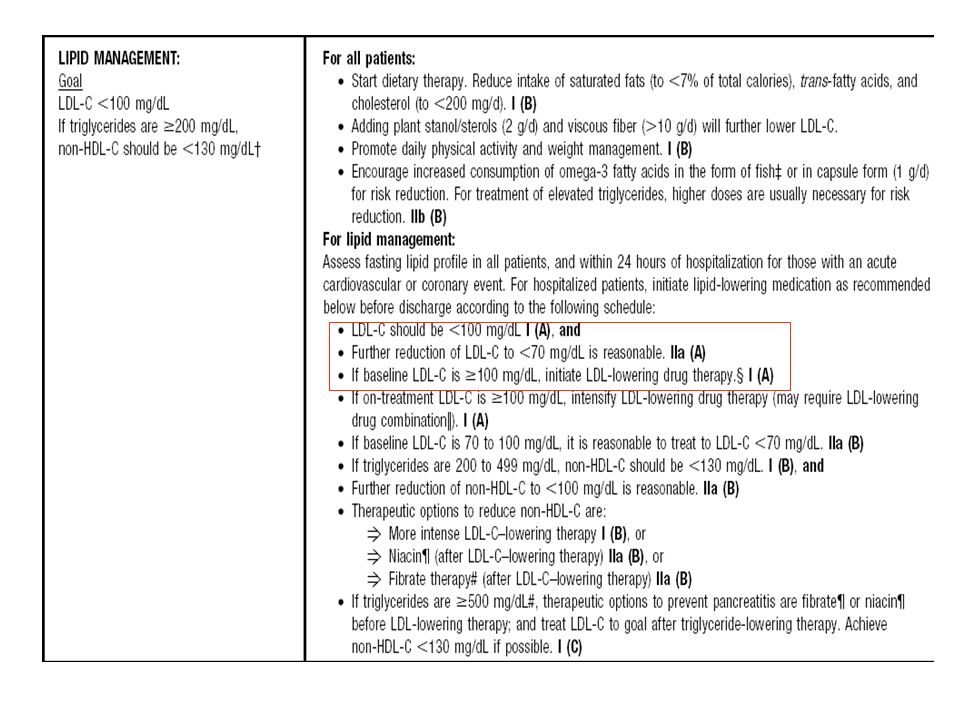
Ref 27 Guías AHA/ACC Report Abstract Diapositiva 26 En el mes de mayo de 2006, se ha publicado una actualización de las recientes guías de consenso en Prevención Secundaria de la Asociación americana del Corazón y el Colegio Americano de Aardiología (AHA/ACC). Desde la publicación del anterior consenso distintas publicaciones han empujado a la actualización de dichas guías clasificando a las recomendaciones en función de los resultados basados en la evidencia como explicaremos en siguiente diapositiva27. Como principal idea destaca el objetivo de c-LDL<100mg/dl para todos los pacientes con enfermedad coronaria y otras manifestaciones ateroscleróticas, pero además incluye como medida razonable un objetivo de c-LDL <70mg/dl para el mencionado grupo de pacientes. Sin embargo no se modifican las recomendaciones establecidas por el ATPIII para los pacientes sin enfermedad aterosclerótica. 27 Ref 27 Página 2363 C1 P1-2 y C2 P1 L17-21 cont Ref 27 Pg2365 C2P1 L2-4 Circulation Mayo 16, 2006 Smith Sidney, et al. AHA/ACC Guidelines for Secondary Prevention for Patients With Coronary and Other Atherosclerotic Vascular Disease: 2006 Update. Circulation 2006; 113:
. Desde la publicación del anterior consenso distintas publicaciones han empujado a la actualización de dichas guías clasificando a las recomendaciones en función de los resultados basados en la evidencia como explicaremos en siguiente diapositiva27. Como principal idea destaca el objetivo de c-LDL<100mg/dl para todos los pacientes con enfermedad coronaria y otras manifestaciones ateroscleróticas, pero además incluye como medida razonable un objetivo de c-LDL <70mg/dl para el mencionado grupo de pacientes. Sin embargo no se modifican las recomendaciones establecidas por el ATPIII para los pacientes sin enfermedad aterosclerótica. 27. Ref 27 Página C1 P1-2 y C2 P1 L17-21 cont. Ref 27 Pg2365 C2P1 L2-4. Circulation Mayo 16, Smith Sidney, et al. AHA/ACC Guidelines for Secondary Prevention for Patients With Coronary and Other Atherosclerotic Vascular Disease: 2006 Update. Circulation 2006; 113:")
46
Actualización de las Guías AHA/ACC II
Ref 27 GUIAS AHA/ACC pg 2364 Tabla 1 C 2, P3 apto lipid management Objetivo c-LDL en Prevención Secundaria para pacientes con enfermedad coronaria: c-LDL<100mg/dl Recomendación Clase I y Nivel Evidencia “A” c-LDL<70mg/dl Objetivo Razonable: Clase IIa y N.E. “A” Si c-LDL>100mg/dl Iniciar terapia hipolipemiante: Clase I y N.E. “A” Diapositiva 27 En esta diapositiva se recogen las recomendaciones para el manejo lipídico en prevención secundaria para pacientes con enfermedad coronaria, de acuerdo a dos clasificaciones: Recomendaciones Clase I, II, IIa, IIb y III, donde la I es la que tiene mayor peso en cuanto al beneficio, utilidad y eficacia del tratamiento basado tanto en evidencias como en consenso general de expertos. La clase II, es la recomendación donde hay conflictos de evidencia y/o divergencias de opinión acerca de la utilidad/eficacia de un procedimiento o tratamiento. A partir de la clase II van perdiendo fuerza el establecimiento de un tratamiento, aún así la IIa es la que cuenta con el peso de la evidencia y opinión a favor de la utilidad y eficacia, en la IIb dicha evidencia y opinión está menos establecida y por último la III que cuenta con evidencia y consenso referente a la falta de utilidad y eficacia del tratamiento/procedimiento24 Nivel de Evidencia (N.E.): A, B y C; donde el nivel A representa a las recomendaciones a partir de resultados obtenidos a través de los estudios de mayor fiabilidad científica, que son los datos de múltiples ensayos clínicos aleatorizados o metaanálisis. Y el C es elaborado únicamente a partir de opiniones de expertos entre otros.27 De acuerdo a las clasificaciones comentadas anteriormente, la Guía de la AHA/ACC establece las siguientes recomendaciones: Objetivo de C-LDL<100mg/dl, como recomendación Clase I y nivel de evidencia A C-LDL<70mg/dl, como objetivo razonable: recomendación Clase IIa y nivel de evidencia A Si C-LDL>100mg/dl, iniciar terapia hipolipemiante: recomendación Clase I y nivel de evidencia A Si c-LDL continúa siendo >100mg/dl aún con tratamiento, la intensificación del tratamiento es recomendación Clase I y Nivel de Evidencia A y puede requerir terapia de combinación. En este sentido la combinación de estatinas a dosis estándar + Ezetimiba es la primera opción recomendada. 27 Ref 27 Página 2366 Tabla 2 Si con tratamiento el c-LDL >100mg/dl, intensificar la terapia (puede requerir combinación). Clase I y N.E. “A” N.E.= nivel de evidencia Smith Sidney, et al. AHA/ACC Guidelines for Secondary Prevention for Patients With Coronary and Other Atherosclerotic Vascular Disease: 2006 Update. Circulation 2006; 113:
: A, B y C; donde el nivel A representa a las recomendaciones a partir de resultados obtenidos a través de los estudios de mayor fiabilidad científica, que son los datos de múltiples ensayos clínicos aleatorizados o metaanálisis. Y el C es elaborado únicamente a partir de opiniones de expertos entre otros.27. De acuerdo a las clasificaciones comentadas anteriormente, la Guía de la AHA/ACC establece las siguientes recomendaciones: Objetivo de C-LDL<100mg/dl, como recomendación Clase I y nivel de evidencia A. C-LDL<70mg/dl, como objetivo razonable: recomendación Clase IIa y nivel de evidencia A. Si C-LDL>100mg/dl, iniciar terapia hipolipemiante: recomendación Clase I y nivel de evidencia A. Si c-LDL continúa siendo >100mg/dl aún con tratamiento, la intensificación del tratamiento es recomendación Clase I y Nivel de Evidencia A y puede requerir terapia de combinación. En este sentido la combinación de estatinas a dosis estándar + Ezetimiba es la primera opción recomendada. 27. Ref 27 Página Tabla 2. Si con tratamiento el c-LDL >100mg/dl, intensificar la terapia (puede requerir combinación). Clase I y N.E. A N.E.= nivel de evidencia. Smith Sidney, et al. AHA/ACC Guidelines for Secondary Prevention for Patients With Coronary and Other Atherosclerotic Vascular Disease: 2006 Update. Circulation 2006; 113:")
Presentaciones similares










en Ateroesclerosis. Seguridad y Eficacia Presentado en el.>")









