Descargar la presentación
La descarga está en progreso. Por favor, espere

1
DE POLITICA DE ANTIBIÓTICO
DOCUMENTO DE CONSENSO DE POLITICA DE ANTIBIÓTICO EN HAD

2
1- INTRODUCCIÓN Consiste en el tratamiento de la enfermedad infecciosa en el domicilio del enfermo, tanto en lo que se refiere a la administración del antimicrobiano por vía endovenosa como a los controles clínicos y analíticos indicadores de la evolución de la enfermedad Constituye una alternativa al ingreso hospitalario para el tratamiento de enfermedades infecciosas En nuestro medio, la Hospitalización Domiciliaria (HaD) constituye el principal recurso asistencial para su aplicación y control
 constituye el principal recurso asistencial para su aplicación y control.")
3
Se inició en EEUU, en 1974 en niños con fibrosis quística e infecciones respiratorias de repetición
En España, se inició en por Antelo y Pestaña₁ también en niños con fibrosis quística e infecciones respiratorias En España, en 2005, se realizaban al menos procedimientos de este tipo al año₂ Antelo MC, Pestaña A. Terapeútica antimicrobiana intravenosa domiciliaria en niños con fibrosis quística. An Esp Pediatr. 1988; 28 Supl 31:55 27º Congreso Mundial de Medicina Interna. Granada 2004

4
2- VENTAJAS Reducción de las infecciones nosocomiales que aumentan los días de hospitalización e incrementan la morbimortalidad y el gasto Posibilidad de colonización o infección por microorganismos cada vez más resistentes en hospital Beneficio para el paciente de estar en su medio habitual Puede volver en ocasiones a su actividad laboral, social o escolar

5
3- CARACTERÍSTICAS Hay que realizar una buena selección del paciente y la patología a tratar Seleccionar el antibiótico más adecuado y la vía de administración que más se amolde a las necesidades del paciente, así como al equipo sanitario que supervise dicha acción, priorizando antibioterapia activa frente a la infección a tratar y calidad asistencial en función de los recursos humanos y técnicos posibles Conocer bien la estabilidad del antibiótico a distintas temperaturas, si se precisa perfusión contínua

6
4- INFECCIONES SUBSIDIARIAS
En la casuística de nuestro país, las infecciones más tratadas₁,₂₋₃ han sido las infecciones respiratorias, urinarias y tejidos blandos Hoy en día y con la experiencia acumulada, es posible tratar casi la totalidad de infecciones presentes, ya sea desde el inicio o en su continuidad de cuidados, en ámbito domiciliario Goenaga MA, Carrera JA, Garde C, Millet M. Antibióticos parenterales en el domicilio. Enferm Infecc Microbiol Clin. 1999; 17: Horcajada JP, García L, Benito N, Cervera C, Sala M, et al. Hospitalización a domicilio especializada en enfermedades infecciosas.Experiencia de a Enferm Infecc Microbiol Clin, 2007; 25(7): Mendoza-Ruiz de Zuazu H, et al. Antibioterapia intravenosa en domicilio. Estudio de casos. Enferm Infecc Microbiol Clin 2005; 23(7):
: Mendoza-Ruiz de Zuazu H, et al. Antibioterapia intravenosa en domicilio. Estudio de 515 casos. Enferm Infecc Microbiol Clin 2005; 23(7):")
7
Escherichia Coli Staphylococo aureus

8
Neumonía por Pseudomona
Staphylococo aureus Neumonía por Pseudomona

9
Mendoza –Ruiz de Zuazu H,et al. Antibioterapia intravenosa en domicilio. Estudio de casos. Enferm, Infecc Microbiol 2005;23 (7):
:")
10
INFECCIONES TRATADAS

11
Mendoza –Ruiz de Zuazu H,et al. Antibioterapia intravenosa en domicilio. Estudio de casos. Enferm, Infecc Microbiol 2005; 23(7):
:")
12
ANTIBIOTERAPIA UTILIZADA

13
Mendoza –Ruiz de Zuazu H,et al. Antibioterapia intravenosa en domicilio. Estudio de casos. Enferm, Infecc Microbiol 2005; 23(7):
:")
14
PROCEDENCIA 24

15
EVOLUCIÓN DESFAVORABLE FAVORABLE

16
5- ANTIBIOTICO IDEAL Perfil de seguridad
Amplio espectro Perfil de seguridad Administración en dosis única diaria, si es posible Tiempo de infusión breve Estabilidad a temperatura ambiente o en la nevera, una vez reconstituido y diluido

18
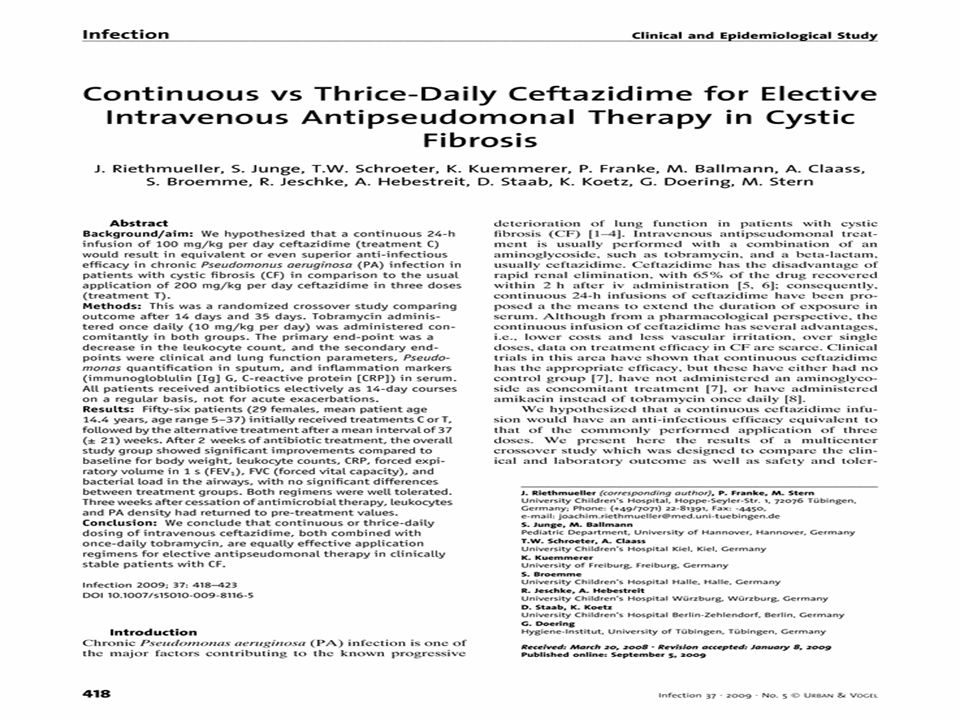
Patient receiving a continuous infusion of flucloxacillin via a computerised infusion pump and peripherally inserted central catheter

19
GRUPO DE ANTIBIOTERAPIA
Inició su andadura en 2013 Inicialmente se ha planteado realizar: revisión de antibióticos más empleados en nuestras unidades formas diversas de administración parenteral efectos secundarios frecuentes antibioterapia en dosis única y alternativas en cada h TODO CON BIBLIOGRAFIA También se ha planteado otros temas a revisar : ¿utilizamos vías centrales, las cambiamos? ,¿cada cuánto cambiamos periféricas y cómo las cuidamos ? , ¿problemáticas con nuestras farmacias ?, ¿antivirales utilizamos ? Perioricidad de controles a realizar, sellados de catéteres centrales,¿autoadministración?.....otros (control de ab en residencias)?.....
")
20
CEFALOSPORINAS CEFTRIAXONA₁ CEFEPIME₂₋₃
Se puede utilizar en perfusión contínua, con estabilidad a temperatura ambiente 25⁰ durante 24 h Recomendable, previamente bolo iv de mg ₁ CEFEPIME₂₋₃ Se puede utilizar en perfusión contínua, con estabilidad a temperatura ambiente 25⁰ durante 24 h Recomendable , previamente bolo de 2 g iv ₄

21
3. CEFTACIDIMA⁻⁶⁻⁷ Se ha objetivado en varios estudios su estabilidad en perfusión contínua a temperatura ambiente 25⁰ durante 24 – 48 h TODOS ESTOS FÁRMACOS A MENOR TEMPERATURA (2⁰ - 8⁰) PUEDEN ESTAR ESTABLES MÁS TIEMPO
 PUEDEN ESTAR ESTABLES MÁS TIEMPO.")
22
Is continuous infusion ceftriaxone better than once-a-day dosingin intensive care? A randomized controlled pilot study Jason A. Roberts, et al. Is continuous infusion ceftriaxone better than once-a-day dosing in intensive care ?. A randomized controlled pilot study. Journal of Antimicrobial Chemotherapy (2007) 59: Objectives: To compare the clinical and bacteriological outcome of critically ill patients with sepsis treated by ceftriaxone administered as a once-a-day intermittent bolus dose or by 24 h continuous infusion. Patients and methods: We conducted an open-label, randomized controlled pilot study in 57 patients clinically diagnosed with sepsis (suspected/proven infection and systemic inflammatory response syndrome) in a tertiary level intensive care unit. Patients were randomized to receive 2 g of ceftriaxone administered by once-daily intermittent bolus dosing or by 24 h continuous infusion. Clinical and bacteriological outcomes were assessed by blinded clinicians. Results: Fifty-seven patients were enrolled in the study, 50 of whom fulfilled the a priori definition of treatment for 4 or more days. The infusion (n = 29) and bolus groups (n = 28) were similar in terms of demographics, although the median age of those receiving the infusion was younger. Intention-to-treat analysis found no statistically significant differences in the primary outcomes for clinical response (P = 0.17), clinical cure [infusion n = 13/29 versus bolus n = 5/28; adjusted odds ratio (AOR) = 3.74; 95% confidence interval (95% CI) = 1.11–12.57; P = 0.06], bacteriological response (P = 0.41) and bacteriological cure (infusion n = 18/29 versus bolus 14/28; AOR = 1.64; 95% CI = 0.57–4.70; P = 0.52). However, logistic regression in patients that complied with the a priori definitions who received ceftriaxone by continuous infusion (AOR = 22.8; 95% CI = 2.24–232.3; P = 0.008) or patients with a low Acute Physiology and Chronic Health Evaluation (APACHE) II score (AOR = 0.70; 95% CI = 0.54–0.91; P = 0.008) were associated with an improved clinical outcome when age and Sepsis Organ Failure Assessment (SOFA) score at time of study entry were controlled for. Conclusions: This pilot study suggests clinical and bacteriological advantages of continuous infusion of ceftriaxone over bolus administration in critically ill patients in patients requiring 4 or more days of treatment. This sets the scene for a large multicentre double-blind randomized controlled trial to confirm these findings.
 59: Objectives: To compare the clinical and bacteriological outcome of critically ill patients with sepsis treated by ceftriaxone administered as a once-a-day intermittent bolus dose or by 24 h continuous infusion. Patients and methods: We conducted an open-label, randomized controlled pilot study in 57 patients clinically diagnosed with sepsis (suspected/proven infection and systemic inflammatory response syndrome) in a tertiary level intensive care unit. Patients were randomized to receive 2 g of ceftriaxone administered by once-daily intermittent bolus dosing or by 24 h continuous infusion. Clinical and bacteriological outcomes were assessed by blinded clinicians. Results: Fifty-seven patients were enrolled in the study, 50 of whom fulfilled the a priori definition of treatment for 4 or more days. The infusion (n = 29) and bolus groups (n = 28) were similar in terms of demographics, although the median age of those receiving the infusion was younger. Intention-to-treat analysis found no statistically significant differences in the primary outcomes for clinical response (P = 0.17), clinical cure [infusion n = 13/29 versus bolus n = 5/28; adjusted odds ratio (AOR) = 3.74; 95% confidence interval (95% CI) = 1.11–12.57; P = 0.06], bacteriological response (P = 0.41) and bacteriological cure (infusion n = 18/29 versus bolus 14/28; AOR = 1.64; 95% CI = 0.57–4.70; P = 0.52). However, logistic regression in patients that complied with the a priori definitions who received. ceftriaxone by continuous infusion (AOR = 22.8; 95% CI = 2.24–232.3; P = 0.008) or patients with a low Acute Physiology and Chronic Health Evaluation (APACHE) II score (AOR = 0.70; 95% CI = 0.54–0.91; P = 0.008) were associated with an improved clinical outcome when age and Sepsis Organ Failure Assessment (SOFA) score at time of study entry were controlled for. Conclusions: This pilot study suggests clinical and bacteriological advantages of continuous infusion of ceftriaxone over bolus administration in critically ill patients in patients requiring 4 or more days of treatment. This sets the scene for a large multicentre double-blind randomized controlled trial to confirm these findings.")
23
ANTIMICROBIAL AGENTS AND CHEMOTHERAPY, June 2003, p. 1991–1994 Vol
ANTIMICROBIAL AGENTS AND CHEMOTHERAPY, June 2003, p. 1991–1994 Vol. 47, No. 6 Stability and Antibacterial Activity of Cefepime during Continuous Infusion Pa°l F. Sprauten,1,2 Paul M. Beringer,2* Stan G. Louie,2 Timothy W. Synold,3 and Mark A. Gill2 University of Oslo, Oslo, Norway,1 and University of Southern California, Los Angeles,2 and City of Hope, Duarte,3 California The stability of cefepime during simulated continuous infusion was determined with a motorized portable infusion pump worn over a period of 24 to 36 h. Susceptibility testing on cefepime solutions over time indicates that the degradation products do not exhibit antibacterial activity. Cefepime stability at 24 h following continuous infusion was 94.3% ± 1%, wich supports the use of continuous infusion

24
Pilot study of continuous infusion cefepime in adult patients with cystic fibrosis
Emily E. Han, et al. Journal of Antimicrobial Chemotherapy (2006) March, CF patients were prospectively randomized to receive either II or CI cefepime once the study was approved by the local Institutional Review Board. Dosing regimens were as follows: cefepime (Elan Pharmaceuticals, San Diego, CA, USA) 50 mg/kg over 30 min every 8 h (maximum 6 g/day) in the II group; a loading dose of 15 mg/kg over 30 min, followed by a CI of 100 mg/kg/24 h (maximum 6 g/day) via a portable infusion pump (Microject 30, Sorensen Medical, West Jordan,UT, USA) in the CI group. Tobramycin was initiated in all patient
 March, CF patients were prospectively randomized to receive either II or CI cefepime once the study was approved by the local Institutional Review Board. Dosing regimens were as follows: cefepime (Elan Pharmaceuticals, San Diego, CA, USA) 50 mg/kg over 30 min every 8 h (maximum 6 g/day) in the II group; a loading dose of 15 mg/kg over 30 min, followed by a CI of 100 mg/kg/24 h (maximum 6 g/day) via a portable infusion pump (Microject 30, Sorensen Medical, West Jordan,UT, USA) in the CI group. Tobramycin was initiated in all patient.")
26
PIPERACILINA-TAZOBACTAM
Presenta estabilidad en perfusión contínua durante 24 h a temperatura ambiente (25⁰) Presenta estabilidad durante 48 h en frío (2⁰- 8⁰) Valorar dosis de carga de 2 g iv, antes de iniciar perfusión 1- Chonghua Li and et al. Population pharmacokinetics and pharmacodynamics of piperacillin/tazobactam in patients with complicated intra-adominal infection. Journal of Antimicrobial Chemotherapy 2005, 56: 2- Kim A and et al. Optimal dosing of piperacillin-tazobactam for the treatment of Pseudomonas aeruginosa infections: prolonged or continuous infusion?.Pharmacotherapy Nov; 27 (11): 3- Lorente L and et al. Clinical cure of ventilator-associated pneumonia treated with piperacillin/tazobactam administered by continuous or intermittent infusion. Int J Antimicrob Agents May; 33 (5): 464-8
 Presenta estabilidad durante 48 h en frío (2⁰- 8⁰) Valorar dosis de carga de 2 g iv, antes de iniciar perfusión. 1- Chonghua Li and et al. Population pharmacokinetics and pharmacodynamics of piperacillin/tazobactam in patients with complicated intra-adominal infection. Journal of Antimicrobial Chemotherapy 2005, 56: Kim A and et al. Optimal dosing of piperacillin-tazobactam for the treatment of Pseudomonas aeruginosa infections: prolonged or continuous infusion .Pharmacotherapy 2007 Nov; 27 (11): Lorente L and et al. Clinical cure of ventilator-associated pneumonia treated with piperacillin/tazobactam administered by continuous or intermittent infusion. Int J Antimicrob Agents 2009 May; 33 (5):")
27
Clin Infect Dis. 2013 Jan 56 (2): 272-82
Clinical Outcomes With Extended or Continuous Versus Short-term Intravenous Infusion of Carbapenems and Piperacillin/Tazobactam: A Systematic Review and Meta-analysis Ellie J. C. Goldstein, Section Editor Matthew E. Falagas1,2,4, Giannoula S. Tansarli1, Kazuro Ikawa3, and Konstantinos Z. Vardakas1,2 1Alfa Institute of Biomedical Sciences (AIBS) 2Department of Internal Medicine-Infectious Diseases, Mitera Hospital, Hygeia Group, Athens, Greece 3Department of Clinical Pharmacotherapy, Hiroshima University, Japan 4Tufts University School of Medicine, Boston, Massachusetts Abstract We sought to study whether the better pharmacokinetic and pharmacodynamic (PK/PD) properties of carbapenems and piperacillin/tazobactam, when the duration of infusion is longer, were associated with lower mortality. PubMed and Scopus were searched for studies reporting on patients treated with extended (≥3 hours) or continuous (24 hours) versus short-term duration (20–60 minutes) infusions of carbapenems or piperacillin/tazobactam. Fourteen studies were included (1229 patients). Mortality was lower among patients receiving extended or continuous infusion of carbapenems or piperacillin/tazobactam compared to those receiving short-term (risk ratio [RR], 0.59; 95% confidence interval [CI], .41–.83). Patients with pneumonia who received extended or continuous infusion had lower mortality than those receiving short-term infusion (RR, 0.50; 95% CI, 0.26–0.96). Data for other specific infections were not available. The available evidence from mainly nonrandomized studies suggests that extended or continuous infusion of carbapenems or piperacillin/tazobactam was associated with lower mortality. Well-designed randomized controlled trials are warranted to confirm these findings before such approaches become widely used.
 2Department of Internal Medicine-Infectious Diseases, Mitera Hospital, Hygeia Group, Athens, Greece. 3Department of Clinical Pharmacotherapy, Hiroshima University, Japan. 4Tufts University School of Medicine, Boston, Massachusetts. Abstract. We sought to study whether the better pharmacokinetic and pharmacodynamic (PK/PD) properties of carbapenems and piperacillin/tazobactam, when the duration of infusion is longer, were associated with lower mortality. PubMed and Scopus were searched for studies reporting on patients treated with extended (≥3 hours) or continuous (24 hours) versus short-term duration (20–60 minutes) infusions of carbapenems or piperacillin/tazobactam. Fourteen studies were included (1229 patients). Mortality was lower among patients receiving extended or continuous infusion of carbapenems or piperacillin/tazobactam compared to those receiving short-term (risk ratio [RR], 0.59; 95% confidence interval [CI], .41–.83). Patients with pneumonia who received extended or continuous infusion had lower mortality than those receiving short-term infusion (RR, 0.50; 95% CI, 0.26–0.96). Data for other specific infections were not available. The available evidence from mainly nonrandomized studies suggests that extended or continuous infusion of carbapenems or piperacillin/tazobactam was associated with lower mortality. Well-designed randomized controlled trials are warranted to confirm these findings before such approaches become widely used.")
28
Optimal Dosing of Piperacillin-Tazobactam for the Treatment of Pseudomonas aeruginosa Infections: Prolonged or Continuous Infusion? Aryun Kim Pharm.D.1, Christina A. Sutherland B.S.1, Joseph L. Kuti Pharm.D.1, Dr. David P. Nicolau Pharm.D., FCCP2,* Pharmacotherapy: The Journal of Human Pharmacology and Drug Therapy Volume 27, Issue 11, pages 1490–1497, November 2007 Study Objective. To compare conventional intermittent dosing regimens of piperacillin-tazobactam with prolonged and continuous infusions to determine the optimal dosing scheme against a local Pseudomonas aeruginosa population. Design. Pharmacodynamic Monte Carlo simulation model. Data Source. Microbiologic data from 470 consecutive nonduplicate P. aeruginosa isolates collected from a single institution over 6 months in 2006. Patients. Five thousand simulated surgical patients and patients with neutropenia. Measurements and Main Results. We simulated serum concentration-time profiles at steady state for several piperacillin-tazobactam dosing regimens, including intermittent, prolonged, and continuous infusions. The probability of achieving 50% free time above the MIC against 470 P. aeruginosa isolates was calculated. The cumulative fractions of response for the intermittent-infusion regimens were 74.7% (3.375 g every 6 hrs), 79.9% (4.5 g every 6 hrs), and 85.6% (3.375 g every 4 hrs). For prolonged-infusion regimens, the cumulative fractions of response were 83.3% (3.375 g every 8 hrs, 4-hr infusion), 87.1% (4.5 g every 8 hrs, 4-hr infusion), and 89.6% (4.5 g every 6 hrs, 3-hr infusion). For continuous-infusion regimens, the cumulative fractions of response were 82.3% ( g), 86.5% (13.5 g), 89.2% (18 g), 90.0% (20.25 g), and 90.6% (22.5 g). Conclusion. Both prolonged- and continuous-infusion strategies improved the pharmacodynamics of piperacillin-tazobactam over those of traditional 30-minute intermittent-infusion regimens. Prolonged- and continuous-infusion regimens that contained the same daily doses of piperacillin had similar likelihoods of bactericidal exposure. Thus, the selection of dosing strategy depends on the availability of intravenous access versus the convenience of once-daily administration.
, 79.9% (4.5 g every 6 hrs), and 85.6% (3.375 g every 4 hrs). For prolonged-infusion regimens, the cumulative fractions of response were 83.3% (3.375 g every 8 hrs, 4-hr infusion), 87.1% (4.5 g every 8 hrs, 4-hr infusion), and 89.6% (4.5 g every 6 hrs, 3-hr infusion). For continuous-infusion regimens, the cumulative fractions of response were 82.3% ( g), 86.5% (13.5 g), 89.2% (18 g), 90.0% (20.25 g), and 90.6% (22.5 g). Conclusion. Both prolonged- and continuous-infusion strategies improved the pharmacodynamics of piperacillin-tazobactam over those of traditional 30-minute intermittent-infusion regimens. Prolonged- and continuous-infusion regimens that contained the same daily doses of piperacillin had similar likelihoods of bactericidal exposure. Thus, the selection of dosing strategy depends on the availability of intravenous access versus the convenience of once-daily administration.")
29
Clinical Outcomes With Extended or Continuous Versus Short-term Intravenous Infusion of Carbapenems and Piperacillin/Tazobactam: A Systematic Review and Meta-analysis Matthew E. Falagas, Giannoula S. Tansarli, Kazuro Ikawa and Konstantinos Z. Vardakas. Clin Infect Dis (2013) 56 (2): We sought to study whether the better pharmacokinetic and pharmacodynamic (PK/PD) properties of carbapenems and piperacillin/tazobactam, when the duration of infusion is longer, were associated with lower mortality. PubMed and Scopus were searched for studies reporting on patients treated with extended (≥3 hours) or continuous (24 hours) versus short-term duration (20–60 minutes) infusions of carbapenems or piperacillin/tazobactam. Fourteen studies were included (1229 patients). Mortality was lower among patients receiving extended or continuous infusion of carbapenems or piperacillin/tazobactam compared to those receiving short-term (risk ratio [RR], 0.59; 95% confidence interval [CI], .41–.83). Patients with pneumonia who received extended or continuous infusion had lower mortality than those receiving short-term infusion (RR, 0.50; 95% CI, 0.26–0.96). Data for other specific infections were not available. The available evidence from mainly nonrandomized studies suggests that extended or continuous infusion of carbapenems or piperacillin/tazobactam was associated with lower mortality. Well-designed randomized controlled trials are warranted to confirm these findings before such approaches become widely used.
 56 (2): We sought to study whether the better pharmacokinetic and pharmacodynamic (PK/PD) properties of carbapenems and piperacillin/tazobactam, when the duration of infusion is longer, were associated with lower mortality. PubMed and Scopus were searched for studies reporting on patients treated with extended (≥3 hours) or continuous (24 hours) versus short-term duration (20–60 minutes) infusions of carbapenems or piperacillin/tazobactam. Fourteen studies were included (1229 patients). Mortality was lower among patients receiving extended or continuous infusion of carbapenems or piperacillin/tazobactam compared to those receiving short-term (risk ratio [RR], 0.59; 95% confidence interval [CI], .41–.83). Patients with pneumonia who received extended or continuous infusion had lower mortality than those receiving short-term infusion (RR, 0.50; 95% CI, 0.26–0.96). Data for other specific infections were not available. The available evidence from mainly nonrandomized studies suggests that extended or continuous infusion of carbapenems or piperacillin/tazobactam was associated with lower mortality. Well-designed randomized controlled trials are warranted to confirm these findings before such approaches become widely used.")
30
ANTIMICROBIAL AGENTS AND CHEMOTHERAPY, Aug. 2002, p. 2327–2332
Comparative Stability Studies of Antipseudomonal -Lactams for Potential Administration through Portable Elastomeric Pumps (Home Therapy for Cystic Fibrosis Patients) and Motor-Operated Syringes (Intensive Care Units) Eric Viaene,* Hugues Chanteux, He´le`ne Servais, Marie-Paule Mingeot-Leclercq, and Paul M. Tulkens Unite´ de Pharmacologie Cellulaire et Mole´culaire, Universite´ Catholique de Louvain, B-1200 Brussels, Belgium The stability of antipseudomonal -lactams in concentrated solutions was examined in view of their potential administration by continuous infusion with external pumps (for intensive care patients) or with portable pumps carried under clothing (for cystic fibrosis patients). Aztreonam (100 g/liter), piperacillin (128 g/liter, with tazobactam), and azlocillin (128 g/liter) remained 90% stable for up to more than 24 h at 37°C (mezlocillin [128 g/liter] was stable at 25°C but not at 37°C). Ceftazidime (120 g/liter), cefpirome (32 g/liter), and cefepime (50 g/liter) remained 90% stable for up to 24, 23.7, and 20.5 h at 25°C but only for 8, 7.25, and 13 h at 37°C, respectively. The control of temperature therefore appears to be critical for all three cephalosporins that cannot be recommended for use in portable pumps carried under clothes for prolonged periods for reasons of stability. Cefpirome and cefepime solutions developed an important color change (from light yellow to dark red) upon exposure when stored at 30°C or higher. Degradation of ceftazidime was accompanied by the liberation of pyridine which, at 37°C, was in excess of what is allowed by the U.S. Pharmacopeia, i.e., 1.1 mg/liter, after 8 and 12 h for drug concentrations of 12 and 8.3%, respectively. Imipenem and meropenem are too unstable (10% degradation at 25°C after 3.5 and 5.15 h, respectively) to be recommended for use by continuous infusion. Faropenem, examined in comparison with imipenem and meropenem, proved as stable as aztreonam or piperacillin. ANTIMICROBIAL AGENTS AND CHEMOTHERAPY, Aug. 2002, p. 2327–2332
 and Motor-Operated Syringes (Intensive Care Units) Eric Viaene,* Hugues Chanteux, He´le`ne Servais, Marie-Paule Mingeot-Leclercq, and Paul M. Tulkens. Unite´ de Pharmacologie Cellulaire et Mole´culaire, Universite´ Catholique de Louvain, B-1200 Brussels, Belgium. The stability of antipseudomonal -lactams in concentrated solutions was examined in view of their potential administration by continuous infusion with external pumps (for intensive care patients) or with portable pumps carried under clothing (for cystic fibrosis patients). Aztreonam (100 g/liter), piperacillin (128 g/liter, with tazobactam), and azlocillin (128 g/liter) remained 90% stable for up to more than 24 h at 37°C (mezlocillin [128 g/liter] was stable at 25°C but not at 37°C). Ceftazidime (120 g/liter), cefpirome (32 g/liter), and cefepime (50 g/liter) remained 90% stable for up to 24, 23.7, and 20.5 h at 25°C but only for 8, 7.25, and 13 h at 37°C, respectively. The control of temperature therefore appears to be critical for all three cephalosporins that cannot be recommended for use in portable pumps carried under clothes for prolonged periods for reasons of stability. Cefpirome and cefepime solutions developed an important color change (from light yellow to dark red) upon exposure when stored at 30°C or higher. Degradation of ceftazidime was accompanied by the liberation of pyridine which, at 37°C, was in excess of what is allowed by the U.S. Pharmacopeia, i.e., 1.1 mg/liter, after 8 and 12 h for drug concentrations of 12 and 8.3%, respectively. Imipenem and meropenem are too unstable (10% degradation at 25°C after 3.5 and 5.15 h, respectively) to be recommended for use by continuous infusion. Faropenem, examined in comparison with imipenem and meropenem, proved as stable as aztreonam or piperacillin. ANTIMICROBIAL AGENTS AND CHEMOTHERAPY, Aug. 2002, p. 2327–2332.")
31
Artículo original: Does prolonged β-lactam infusions improve clinical outcomes compared to intermittent infusions? A meta-analysis and systematic review of randomized, controlled trials. Tamma PD, Putcha N, Suh YD, Van Arendonk KJ, Rinke ML. BMC Infect Dis 2011; 11: 181. Introducción: El parámetro farmacocinético que mejor predice la efectividad de los betalactámicos es el tiempo en que la concentración plasmática del antibiótico supera la concentración mínima inhibitoria. Mantener dicho parámetro en valores óptimos durante la mayor parte del intervalo de administración es difícil, sobre todo para microorganismos con CMI elevadas. Desde hace años se evalúa la perfusión continua como alternativa a la administración intermitente, con resultados contradictorios. Resumen: Este metaanálisis recoge 14 ensayos clínicos sobre perfusión continua (ritmo constante en 24 horas) y/o también infusión prolongada intermitente (administración de cada dosis en 3 a 7 horas). No se exige que el betalactámico administrado en el grupo de estudio sea el mismo que el del brazo control, sólo se requiere que tengan un espectro similar. Esto podría haber sido limitante, teniendo en cuenta que no necesariamente tienen similares características farmacocinéticas y farmacodinámicas como por ejemplo el efecto post-antibiótico; sin embargo, en la práctica sólo en uno de los estudios hubo diferencia (doripenem frente a imipenem). No hubo diferencias significativas en el desenlace principal (mortalidad hospitalaria). Sólo un estudio evidenció reducción de mortalidad con la perfusión continua, pero es de interés que es el único en que todos los pacientes estaban críticos e infectados por bacilos Gram negativos resistentes. Tampoco hubo diferencias en la curación clínica o la incidencia de efectos adversos. Los betalactámicos son muy heterogéneos en propiedades farmacocinéticas y farmacodinámicas, teniendo por ejemplo un efecto post-antibiótico muy dispar que posibilita que con algunos de ellos, los carbapenémicos, el plantear la perfusión continua probablemente no tiene interés. Los autores hacen un análisis de subgrupos de cada familia para explorar esta circunstancia pero tampoco encuentran diferencias.
 y/o también infusión prolongada intermitente (administración de cada dosis en 3 a 7 horas). No se exige que el betalactámico administrado en el grupo de estudio sea el mismo que el del brazo control, sólo se requiere que tengan un espectro similar. Esto podría haber sido limitante, teniendo en cuenta que no necesariamente tienen similares características farmacocinéticas y farmacodinámicas como por ejemplo el efecto post-antibiótico; sin embargo, en la práctica sólo en uno de los estudios hubo diferencia (doripenem frente a imipenem). No hubo diferencias significativas en el desenlace principal (mortalidad hospitalaria). Sólo un estudio evidenció reducción de mortalidad con la perfusión continua, pero es de interés que es el único en que todos los pacientes estaban críticos e infectados por bacilos Gram negativos resistentes. Tampoco hubo diferencias en la curación clínica o la incidencia de efectos adversos. Los betalactámicos son muy heterogéneos en propiedades farmacocinéticas y farmacodinámicas, teniendo por ejemplo un efecto post-antibiótico muy dispar que posibilita que con algunos de ellos, los carbapenémicos, el plantear la perfusión continua probablemente no tiene interés. Los autores hacen un análisis de subgrupos de cada familia para explorar esta circunstancia pero tampoco encuentran diferencias.")
32
MEROPENEM Se puede administrar en perfusión contínua
Estabilidad una vez diluido, de 24 h, a temperatura de 2⁰ - 8⁰ A temperatura ambiente, 25⁰, tiene una estabilidad de 8 h, una vez diluido Se puede diluir en salino o glucosado 5 % Recomendable, administrar dosis de carga de 500 – mg ₁₋₂ 1 - Jason A Roberts and et al. Meropenem dosing in critically ill patients with sepsis and without renal dysfunction: intermittent bolus versus continuous administration? Monte Carlo dosing simulations and subcutaneous tissue distribution. Journal of Antimicrobial Chemotherapy (2009) 64, 2 - Leonardo Lorente and et al. Meropenem by Continuous Versus Intermittent Infusion in Ventilator – Associated Pneumonia due to Gram-Negative Bacilli. The Annals of Pharmacotherapy (2006) 40:
 64, Leonardo Lorente and et al. Meropenem by Continuous Versus Intermittent Infusion in Ventilator – Associated Pneumonia due to Gram-Negative Bacilli. The Annals of Pharmacotherapy (2006) 40:")
33
Clinical and microbiological efficacy of continuous versus intermittent application of meropenem in critically ill patients: a randomized open-label controlled trial Ivan Chytra1*, Martin Stepan1, Jan Benes1, Petr Pelnar1, Alexandra Zidkova1, Tamara Bergerova2, Richard Pradl1 and Eduard Kasal1 1 Department of Anesthesiology and Intensive Care Medicine, Charles University in Prague, Faculty of Medicine in Plzen, University Hospital Plzen, alej Svobody 80, , Czech Republic 2 Department of Microbiology, Charles University in Prague, Faculty of Medicine in Plzen, University Hospital Plzen, alej Svobody 80, , Czech Republic Critical Care 2012, 16:R113 Published: 28 June 2012 Introduction Meropenem bactericidal activity depends on the time when the free drug concentrations remain above the minimum inhibitory concentration of pathogens. The goal of this study was to compare clinical and bacteriological efficacy of continuous meropenem infusion versus bolus administration in critically ill patients with severe infection, and to evaluate the safety of both dosing regimens. Methods Patients admitted to the interdisciplinary Intensive Care Unit (ICU) who suffered from severe infections and received meropenem were randomized either in the Infusion group (n = 120) or in the Bolus group (n = 120). Patients in the Infusion group received a loading dose of 2 g of meropenem followed by a continuous infusion of 4 g of meropenem over 24 hours. Patients in the Bolus group were given 2 g of meropenem over 30 minutes every 8 hours. Clinical and microbiological outcome, safety, meropenem-related length of ICU and hospital stay, meropenem-related length of mechanical ventilation, duration of meropenem treatment, total dose of meropenem, and ICU and in-hospital mortality were assessed. Results Clinical cure at the end of meropenem therapy was comparable between both groups (83.0% patients in the Infusion vs. 75.0% patients in the Bolus group; P = 0.180). Microbiological success rate was higher in the Infusion group as opposed to the Bolus group (90.6% vs. 78.4%; P = 0.020). Multivariate logistic regression identified continuous administration of meropenem as an independent predictor of microbiological success (OR = 2.977; 95% CI = to 8.443; P = 0.040). Meropenem-related ICU stay was shorter in the Infusion group compared to the Bolus group (10 (7 to 14) days vs. 12 (7 to 19) days; P = 0.044) as well as shorter duration of meropenem therapy (7 (6 to 8) days vs. 8 (7 to 10) days; P = 0.035) and lower total dose of meropenem (24 (21 to 32) grams vs. 48 (42 to 60) grams; P < ). No severe adverse events related to meropenem administration in either group were observed. Conclusions Continuous infusion of meropenem is safe and, in comparison with higher intermittent dosage, provides equal clinical outcome, generates superior bacteriological efficacy and offers encouraging alternative of antimicrobial therapy in critically ill patients.
 who suffered from severe infections and received meropenem were randomized either in the Infusion group (n = 120) or in the Bolus group (n = 120). Patients in the Infusion group received a loading dose of 2 g of meropenem followed by a continuous infusion of 4 g of meropenem over 24 hours. Patients in the Bolus group were given 2 g of meropenem over 30 minutes every 8 hours. Clinical and microbiological outcome, safety, meropenem-related length of ICU and hospital stay, meropenem-related length of mechanical ventilation, duration of meropenem treatment, total dose of meropenem, and ICU and in-hospital mortality were assessed. Results Clinical cure at the end of meropenem therapy was comparable between both groups (83.0% patients in the Infusion vs. 75.0% patients in the Bolus group; P = 0.180). Microbiological success rate was higher in the Infusion group as opposed to the Bolus group (90.6% vs. 78.4%; P = 0.020). Multivariate logistic regression identified continuous administration of meropenem as an independent predictor of microbiological success (OR = 2.977; 95% CI = to 8.443; P = 0.040). Meropenem-related ICU stay was shorter in the Infusion group compared to the Bolus group (10 (7 to 14) days vs. 12 (7 to 19) days; P = 0.044) as well as shorter duration of meropenem therapy (7 (6 to 8) days vs. 8 (7 to 10) days; P = 0.035) and lower total dose of meropenem (24 (21 to 32) grams vs. 48 (42 to 60) grams; P < ). No severe adverse events related to meropenem administration in either group were observed. Conclusions. Continuous infusion of meropenem is safe and, in comparison with higher intermittent dosage, provides equal clinical outcome, generates superior bacteriological efficacy and offers encouraging alternative of antimicrobial therapy in critically ill patients.")
34
Meropenem dosing in critically ill patients with sepsis and without renal dysfunction: intermittent bolus versus continuous administration? Monte Carlo dosing simulations and subcutaneous tissue distribution Jason A Roberts and et al. Meropenem dosing in critically ill patients with sepsis and without renal dysfunction: intermittent bolus versus continuous administration? Monte Carlo dosing simulations and subcutaneous tissue distribution. Journal of Antimicrobial Chemotherapy (2009) 64, Objectives: To compare the plasma and subcutaneous tissue concentration–time profiles of meropenem administered by intermittent bolus dosing or continuous infusion to critically ill patients with sepsis and without renal dysfunction, and to use population pharmacokinetic modelling and Monte Carlo simulations to assess the cumulative fraction of response (CFR) against Gram-negative pathogens likely to be encountered in critical care units. Patients and methods: We randomized 10 patients with sepsis to receive meropenem by intermittent bolus administration (n=5; 1 g 8 hourly) or an equal dose administered by continuous infusion (n=5). Serial subcutaneous tissue concentrations were determined using microdialysis and compared with plasma data for first-dose and steady-state pharmacokinetics. Population pharmacokinetic modelling of plasma data and Monte Carlo simulations were then undertaken with NONMEMw. Results: It was found that continuous infusion maintains higher median trough concentrations, in both plasma (intermittent bolus 0 versus infusion 7 mg/L) and subcutaneous tissue (0 versus 4 mg/L). All simulated intermittent bolus, extended and continuous infusion dosing achieved 100% of pharmacodynamic targets against most Gram-negative pathogens. Superior obtainment of pharmacodynamic targets was achieved using administration by extended or continuous infusion against less susceptible Pseudomonas aeruginosa and Acinetobacter species. Conclusions: This is the first study to compare the relative concentration–time data of bolus and continuous administration of meropenem at the subcutaneous tissue and plasma levels. We found that the administration of meropenem by continuous infusion maintains higher concentrations in subcutaneous tissue and plasma than by intermittent bolus dosing. Administration by extended or continuous infusion will achieve superior CFR against less-susceptible organisms in patients without renal dysfunction.
 64, Objectives: To compare the plasma and subcutaneous tissue concentration–time profiles of meropenem administered by intermittent bolus dosing or continuous infusion to critically ill patients with sepsis and without renal dysfunction, and to use population pharmacokinetic modelling and Monte Carlo simulations to assess the cumulative fraction of response (CFR) against Gram-negative pathogens likely to be encountered in critical care units. Patients and methods: We randomized 10 patients with sepsis to receive meropenem by intermittent bolus administration (n=5; 1 g 8 hourly) or an equal dose administered by continuous infusion (n=5). Serial subcutaneous tissue concentrations were determined using microdialysis and compared with plasma data for first-dose and steady-state pharmacokinetics. Population pharmacokinetic modelling of plasma data and Monte Carlo simulations were then undertaken with NONMEMw. Results: It was found that continuous infusion maintains higher median trough concentrations, in both plasma (intermittent bolus 0 versus infusion 7 mg/L) and subcutaneous tissue (0 versus 4 mg/L). All simulated intermittent bolus, extended and continuous infusion dosing achieved 100% of pharmacodynamic. targets against most Gram-negative pathogens. Superior obtainment of pharmacodynamic. targets was achieved using administration by extended or continuous infusion against less susceptible Pseudomonas aeruginosa and Acinetobacter species. Conclusions: This is the first study to compare the relative concentration–time data of bolus and continuous administration of meropenem at the subcutaneous tissue and plasma levels. We found that the administration of meropenem by continuous infusion maintains higher concentrations in subcutaneous tissue and plasma than by intermittent bolus dosing. Administration by extended or continuous infusion will achieve superior CFR against less-susceptible organisms in patients without renal dysfunction.")
35
J Antimicrob Chemother 2010
Stability of meropenem and doripenem solutions for administration by continuous infusion Karine Berthoin1, Cecile S. Le Duff2, Jacqueline MarchandBrynaert2,StephaneCarryn1,3 and Paul M. Tulkens1*

36
Am J Health Syst Pharm 2004 aug 15;61(16):1682-5
Stability of meropenem in polyvinyl chloride bags and an elastomeric infusion device DL Smith, SM Bauer and DP Nicolau PURPOSE: The stability of meropenem in i.v. solutions stored in polyvinyl chloride (PVC) bags and an elastomeric infusion device at concentrations commonly used in home care was studied. METHODS: Vials of meropenem were reconstituted with sterile water for injection and mixed with 0.9% sodium chloride injection (NS) to yield concentrations of 4, 10, and 20 mg/mL. Six replicate solutions were prepared in PVC containers and six in the Homepump ECLIPSE elastomeric infusion device. All solutions were stored at an average temperature of 5 degrees C and sampled immediately after preparation and at intervals up to 120 hours (five days); the 4-mg/mL solution was also sampled at 144 and 168 hours (seven days). Samples were assayed for meropenem concentration by stability-indicating high-performance liquid chromatography. RESULTS: All solutions of meropenem retained over 90% of the initial drug concentration at five days. The 4-mg/mL solutions retained over 93% of the initial concentration at seven days. The rate of meropenem decay did not differ significantly between PVC and elastomeric infusion containers for the 4- and 20-mg/mL solutions; however, there was a difference for the 10-mg/mL solutions. CONCLUSION: Meropenem 4 mg/mL in NS was stable for at least seven days in PVC bags and elastomeric infusion containers when stored at 5 degrees C, and meropenem 10 and 20 mg/mL in NS was stable for at least five days in both containers at 5 degrees C.
 bags and an elastomeric infusion device at concentrations commonly used in home care was studied. METHODS: Vials of meropenem were reconstituted with sterile water for injection and mixed with 0.9% sodium chloride injection (NS) to yield concentrations of 4, 10, and 20 mg/mL. Six replicate solutions were prepared in PVC containers and six in the Homepump ECLIPSE elastomeric infusion device. All solutions were stored at an average temperature of 5 degrees C and sampled immediately after preparation and at intervals up to 120 hours (five days); the 4-mg/mL solution was also sampled at 144 and 168 hours (seven days). Samples were assayed for meropenem concentration by stability-indicating high-performance liquid chromatography. RESULTS: All solutions of meropenem retained over 90% of the initial drug concentration at five days. The 4-mg/mL solutions retained over 93% of the initial concentration at seven days. The rate of meropenem decay did not differ significantly between PVC and elastomeric infusion containers for the 4- and 20-mg/mL solutions; however, there was a difference for the 10-mg/mL solutions. CONCLUSION: Meropenem 4 mg/mL in NS was stable for at least seven days in PVC bags and elastomeric infusion containers when stored at 5 degrees C, and meropenem 10 and 20 mg/mL in NS was stable for at least five days in both containers at 5 degrees C.")
37
Continuous Infusion of Beta-Lactam Antibiotics in Severe Sepsis: A Multicenter Double-Blind, Randomized Controlled Trial Joel M. Dulhunty1, Jason A. Roberts1, Joshua S. Davis2, Steven A. R. Webb3, Rinaldo Bellomo4, Charles Gomersall5, Charudatt Shirwadkar6, Glenn M. Eastwood4, John Myburgh7, David L. Paterson8, and Jeffrey Lipman1 1Department of Intensive Care Medicine, Royal Brisbane and Women's Hospital, and Burns, Trauma and Critical Care Research Centre, University of Queensland, Brisbane 2Menzies School of Health Research, Charles Darwin University and Royal Darwin Hospital 3Royal Perth Hospital, and School of Medicine and Pharmacology, University of Western Australia, Perth 4Department of Intensive Care, Austin Hospital, Melbourne, Australia 5Prince of Wales Hospital and Chinese University of Hong Kong, Hong Kong 6Blacktown Hospital 7Critical Care and Trauma Division, George Institute for Global Health, Sydney 8Infectious Diseases Unit, Royal Brisbane and Women's Hospital, and University of Queensland Centre for Clinical Research, Brisbane, Australia Background. Beta-lactam antibiotics are a commonly used treatment for severe sepsis, with intermittent bolus dosing standard therapy, despite a strong theoretical rationale for continuous administration. The aim of this trial was to determine the clinical and pharmacokinetic differences between continuous and intermittent dosing in patients with severe sepsis. Methods. This was a prospective, double-blind, randomized controlled trial of continuous infusion versus intermittent bolus dosing of piperacillin-tazobactam, meropenem, and ticarcillin-clavulanate conducted in 5 intensive care units across Australia and Hong Kong. The primary pharmacokinetic outcome on treatment analysis was plasma antibiotic concentration above the minimum inhibitory concentration (MIC) on days 3 and 4. The assessed clinical outcomes were clinical response 7–14 days after study drug cessation, ICU-free days at day 28 and hospital survival. Results. Sixty patients were enrolled with 30 patients each allocated to the intervention and control groups. Plasma antibiotic concentrations exceeded the MIC in 82% of patients (18 of 22) in the continuous arm versus 29% (6 of 21) in the intermittent arm (P = .001). Clinical cure was higher in the continuous group (70% vs 43%; P = .037), but ICU-free days (19.5 vs 17 days; P = .14) did not significantly differ between groups. Survival to hospital discharge was 90% in the continuous group versus 80% in the intermittent group (P = .47). Conclusions. Continuous administration of beta-lactam antibiotics achieved higher plasma antibiotic concentrations than intermittent administration with improvement in clinical cure. This study provides a strong rationale for further multicenter trials with sufficient power to identify differences in patient-centered endpoints. Clin Infect Dis 2013; 56 (2):
 on days 3 and 4. The assessed clinical outcomes were clinical response 7–14 days after study drug cessation, ICU-free days at day 28 and hospital survival. Results. Sixty patients were enrolled with 30 patients each allocated to the intervention and control groups. Plasma antibiotic concentrations exceeded the MIC in 82% of patients (18 of 22) in the continuous arm versus 29% (6 of 21) in the intermittent arm (P = .001). Clinical cure was higher in the continuous group (70% vs 43%; P = .037), but ICU-free days (19.5 vs 17 days; P = .14) did not significantly differ between groups. Survival to hospital discharge was 90% in the continuous group versus 80% in the intermittent group (P = .47). Conclusions. Continuous administration of beta-lactam antibiotics achieved higher plasma antibiotic concentrations than intermittent administration with improvement in clinical cure. This study provides a strong rationale for further multicenter trials with sufficient power to identify differences in patient-centered endpoints. Clin Infect Dis 2013; 56 (2):")
38
VANCOMICINA Se puede administrar en perfusión contínua₁₋₂₋₃
Estabilidad de 24 h a temperatura ambiente, una vez diluido Se puede utilizar tanto salino como glucosado 5 % para la dilución Concentración máxima de 5 mg/ml 1 - Payne Cj and et al. Vancomycin Continuous Infusion as Prophylaxis for Vascular Surgery. Ther Drug Monit , Oct 5 2- Ingram PR and et al. Nephrotoxicity of continuous versus intermittent infusion of vancomycin in outpatient parenteral antimicrobial therapy. Int J antimicrob Agents Sep 9 3 - Vuagnat A and et al. High dose vancomycin for osteomyelitis : continuous vs intermittent infusion. J Clin Pharm Ther Aug; 29 (4): 351-7
:")
39
Publicado en Med Intensiva. 2005;29:83-7. - vol.29 núm 02
Vancomicina en perfusión continua, una nueva pauta posológica en las Unidades de Cuidados Intensivos Alonso-Fernandez, MA; Estébanez-Montiel, MB; Rico-Cepeda, MP; Catalan-Gonzalez, M; Montejo-Gonzalez, JC Publicado en Med Intensiva. 2005;29: vol.29 núm 02 Objetivo. Valorar la eficacia clínica y la incidencia de efectos adversos con la nueva pauta posológica de vancomicina en perfusión continua. Diseño. Estudio prospectivo, descriptivo durante 17 semanas, desde el 1 de septiembre hasta el 31 de diciembre de Ámbito. Unidad de Cuidados Intensivos (UCI) Polivalente del Hospital Universitario Doce de Octubre de Madrid. Pacientes. Se incluyeron todos los pacientes ingresados en la UCI mayores de 18 años de edad, con sospecha clínica o diagnóstico de infección por cocos grampositivos que fueron tratados con vancomicina en perfusión continua. Durante el período de estudio fueron ingresados 110 pacientes, de los cuales 18 fueron incluidos. Intervención. Se pautó una dosis inicial de carga de 15 mg/kg de peso administrada en 60 minutos, seguida de dosis de mantenimiento de 30 mg/kg de peso cada 12 horas en perfusión continua. Variables de interés principales. Monitorización de los niveles séricos de vancomicina cada 48 horas y de la función renal mediante la determinación de creatinina sérica diaria y el cálculo de aclaramiento de creatinina basal previa al inicio de la perfusión de vancomicina y semanalmente. Resultados. Fueron incluidos en el estudio 18 pacientes de los cuales 14 fueron mujeres. La edad media fue de 61,9 años. El APACHE II medio al ingreso fue de 16,7. Los motivos de ingreso más frecuentes fueron: shock séptico de distintas etiologías, 7 enfermos; insuficiencia respiratoria en 6. El antibiótico se pautó de forma empírica en 4 pacientes. El microorganismo más frecuentemente aislado en los cultivos microbiológicos fue el Staphylococcus epidermidis, 7. La dosis media de vancomicina administrada fue de 25,8 mg/kg/día. Los niveles plasmáticos medios de vancomicina fueron 18,15 µg/ml. La duración media del tratamiento fue de 13,8 días. Se asociaron antibióticos ß-lactámicos en todos los pacientes y aminoglucósidos en 11. En 2 pacientes se suspendió el tratamiento por deterioro de la función renal. Once pacientes presentaron mejoría, en 4 hubo fracaso terapéutico y 3 fallecieron. Conclusiones. La administración de vancomicina en perfusión continua se asocia a una eficacia clínica ligeramente mayor y menores efectos adversos que los descritos con la administración de dosis múltiples. Asimismo supone mayor comodidad de administración, disminución de las cargas de trabajo de enfermería y menor manipulación de los catéteres intravasculares.
 Polivalente del Hospital Universitario Doce de Octubre de Madrid. Pacientes. Se incluyeron todos los pacientes ingresados en la UCI mayores de 18 años de edad, con sospecha clínica o diagnóstico de infección por cocos grampositivos que fueron tratados con vancomicina en perfusión continua. Durante el período de estudio fueron ingresados 110 pacientes, de los cuales 18 fueron incluidos. Intervención. Se pautó una dosis inicial de carga de 15 mg/kg de peso administrada en 60 minutos, seguida de dosis de mantenimiento de 30 mg/kg de peso cada 12 horas en perfusión continua. Variables de interés principales. Monitorización de los niveles séricos de vancomicina cada 48 horas y de la función renal mediante la determinación de creatinina sérica diaria y el cálculo de aclaramiento de creatinina basal previa al inicio de la perfusión de vancomicina y semanalmente. Resultados. Fueron incluidos en el estudio 18 pacientes de los cuales 14 fueron mujeres. La edad media fue de 61,9 años. El APACHE II medio al ingreso fue de 16,7. Los motivos de ingreso más frecuentes fueron: shock séptico de distintas etiologías, 7 enfermos; insuficiencia respiratoria en 6. El antibiótico se pautó de forma empírica en 4 pacientes. El microorganismo más frecuentemente aislado en los cultivos microbiológicos fue el Staphylococcus epidermidis, 7. La dosis media de vancomicina administrada fue de 25,8 mg/kg/día. Los niveles plasmáticos medios de vancomicina fueron 18,15 µg/ml. La duración media del tratamiento fue de 13,8 días. Se asociaron antibióticos ß-lactámicos en todos los pacientes y aminoglucósidos en 11. En 2 pacientes se suspendió el tratamiento por deterioro de la función renal. Once pacientes presentaron mejoría, en 4 hubo fracaso terapéutico y 3 fallecieron. Conclusiones. La administración de vancomicina en perfusión continua se asocia a una eficacia clínica ligeramente mayor y menores efectos adversos que los descritos con la administración de dosis múltiples. Asimismo supone mayor comodidad de administración, disminución de las cargas de trabajo de enfermería y menor manipulación de los catéteres intravasculares.")
40
BIBLIOGRAFÍA Jason A. Roberts, et al. Is continuous infusion ceftriaxone better than once-a-day dosing in intensive care ?. A randomized controlled pilot study. Journal of Antimicrobial Chemotherapy (2007) 59: Pal F. Sprauten, et al. Stability and Antibacterial Activity of Cefepime during Continuous Infusion. Antimicrobial Agents and Chemotherapy. June 2003, Emily E. Han, et al. Pilot study of continuous infusion cefepime in adult patientes with cystic fibrosis. Journal of Antimicrobial Chemotherapy (2006) March, E. Bernard, et al. Is there a rationales for the continuous infusion of cefepime ?. A multidisciplinary approach. Clin Microbiol Infect 2003; 9: C. R. frei and D. S. Burgess. Continuous infusion β-lactams for intensive care unit pulmonary infections. Clin Microbiol Infect 2005; 11: Fadoua Laghzaoui, et al. Ceftacidima en infusión contínua en el tratamiento de infecciones por Pseudomona aeruginosa en una Unidad de Hospitalización a Domicilio. Enferm Infecc Microbiol Clin 2007; 25 (1): 71-72 Riethmueller J, et al. Continuous vs Thrice-Daily Ceftacidime for Elective Intravenous Antipseudomonal Therapy in Cystic Fibrosis. Infection 2009, Sep 5
 59: Pal F. Sprauten, et al. Stability and Antibacterial Activity of Cefepime during Continuous Infusion. Antimicrobial Agents and Chemotherapy. June 2003, Emily E. Han, et al. Pilot study of continuous infusion cefepime in adult patientes with cystic fibrosis. Journal of Antimicrobial Chemotherapy (2006) March, E. Bernard, et al. Is there a rationales for the continuous infusion of cefepime . A multidisciplinary approach. Clin Microbiol Infect 2003; 9: C. R. frei and D. S. Burgess. Continuous infusion β-lactams for intensive care unit pulmonary infections. Clin Microbiol Infect 2005; 11: Fadoua Laghzaoui, et al. Ceftacidima en infusión contínua en el tratamiento de infecciones por Pseudomona aeruginosa en una Unidad de Hospitalización a Domicilio. Enferm Infecc Microbiol Clin 2007; 25 (1): Riethmueller J, et al. Continuous vs Thrice-Daily Ceftacidime for Elective Intravenous Antipseudomonal Therapy in Cystic Fibrosis. Infection 2009, Sep 5.")
41
Brief Report: Practicability and safety of amphotericin B deoxycholate as continuous infusion in neutropenic patients with hematological malignancies Authors: Axel Schulenburg a; Wolfgang Sperr b; Werner Rabitsch a; Paul Kn bl b; Florian Thalhammer c Published in: Leukemia and Lymphoma, Volume 46, Issue 8 August 2005 , pages

42
FARMACOS UTILIZABLES EN PERFUSION CONTINUA ADIESTRAMIENTO CUIDADORES
Meropenem (debe ser en frío, a temperatura entre 2 y 8 grados) Piperacilina-tazobactam (estable a temperatura ambiente cercana a 24 grados) Ceftriaxona Cefepime Cloxacilina Penicilina G Aztreonam Clindamicina Anfotericina B Linezolid Aciclovir Ganciclovir AUTOADMINISTRACION O ADIESTRAMIENTO CUIDADORES
 Piperacilina-tazobactam (estable a temperatura ambiente cercana a 24 grados) Ceftriaxona. Cefepime. Cloxacilina. Penicilina G. Aztreonam. Clindamicina. Anfotericina B. Linezolid. Aciclovir. Ganciclovir. AUTOADMINISTRACION. O. ADIESTRAMIENTO CUIDADORES.")
43
Enferm Infecc Microbiol Clin 2007;25(7):429-36
Hospitalización a domicilio especializada en enfermedades infecciosas. Experiencia de 1995 a 2002 Juan Pablo Horcajada, Laura García, Natividad Benito, Carlos Cervera, Marta Sala, Angels Olivera, Alex Soriano, Marga Robau, José M. Gatell y José M. Miró Servicio de Enfermedades Infecciosas. Hospital Clínic–IDIBAPS. Universidad de Barcelona. IDIBAPS: Institut d’Investigacions Biomèdiques August Pi i Sunyer. España. Los casos de autoadministración se aplicaron en 2 tipos de pacientes. El primer grupo consistió en pacientes que requirieron un antimicrobiano administrado dos veces al día. Una dosis se administró por la enfermera y la otra, por lo general la de la noche, fue autoadministrada. El segundo grupo consistió en pacientes que durante el curso de un tratamiento parenteral prolongado se desplazaron de la ciudad, optando por la autoadministración en períodos breves de tiempo (máximo una semana). El paciente debía estar en sus plenas facultades, ser autónomo y aceptar de forma expresa esta técnica. En todos los casos, el paciente fue instruido y entrenado en la técnica antes de aceptar la autoadministración.
. El paciente debía estar en sus plenas facultades, ser autónomo y aceptar de forma expresa esta técnica. En todos los casos, el paciente fue instruido y entrenado en la técnica antes de aceptar la autoadministración.")
44
Los antibacterianos utilizados fueron: a) ceftriaxona,teicoplanina, vancomicina,gentamicina, amikacina y levofloxacino administrados una vez al día mediante perfusión por gravedad; b) cloxacilina, ampicilina y piperacilina-tazobactam mediante el empleo de bomba electrónica portátil de perfusión intermitente en 46 episodios, y c) cefepima y carbapenemes dos o tres veces al día con la colaboración del paciente o de su familia (autoadministración) en 56 episodios. Esta modalidad de administración también se utilizó para el tratamiento con ganciclovir (28 episodios), glicopéptidos (15 episodios), ceftriaxona(12episodios),piperacilina-tazobactam (4 episodios) y otros (13 episodios) El total de episodios en los que se empleóautoadministración fue de 128, lo que supuso cerca de un 8% de los tratamientos parenterales en domicilio (128 frente a 1.591episodios totales de administración de tratamientos parenterales) La autoadministración se asoció a un mayor riesgo de complicaciones (24% frente a 12%; OR: 2,3; IC 95%: 1,5-3,6; p < 0,001) y de sepsis de catéter (4% frente a 0; OR: 12,9; IC 95%: 10,9-15,3; p < 0,001).
 La autoadministración se asoció a un mayor riesgo de complicaciones (24% frente a 12%; OR: 2,3; IC 95%: 1,5-3,6; p < 0,001) y de sepsis de catéter (4% frente a 0; OR: 12,9; IC 95%: 10,9-15,3; p < 0,001).")
45
Journal of Antimicrobial Chemotherapy
Comment on: Outpatient parenteral antibiotic therapy (OPAT): is it safe for selected patients to self-administer at home? A retrospective analysis of a large cohort over 13 years P. R. Ingram1,2, Z. Sulaiman3, A. Chua1 and D. A. Fisher1,2* ¹Department of Medicine, National University Hospital, 5 Lower Kent Ridge Road, Singapore, Singapore; ²Department of Medicine, Yong Loo Lin School of Medicine, National University of Singapore, 5 Lower Kent Ridge Road, Singapore, Singapore; ³National University Hospital,5 Lower Kent Ridge Road, Singapore, Singapore
: is it safe for selected patients to self-administer at home A retrospective analysis of a large cohort over 13 years. P. R. Ingram1,2, Z. Sulaiman3, A. Chua1 and D. A. Fisher1,2* ¹Department of Medicine, National University Hospital, 5. Lower Kent Ridge Road, Singapore, Singapore; ²Department of Medicine, Yong Loo Lin School of Medicine, National University of Singapore, 5 Lower Kent Ridge Road, Singapore, Singapore; ³National University Hospital,5 Lower Kent Ridge Road, Singapore, Singapore.")
46
hospital in the home (HITH)
Australia “outpatient antibiotic therapy” United States La aplicación de los criterios de inclusión por parte de los miembros del equipo es una medida importante para llevar a cabo esta modalidad asistencial sin detrimento de la seguridad y calidad de vida del paciente.

47
Analítica y Bioquímica completa semanal, excepto en fármacos nefrotóxicos que debe ser cada días Realizar niveles valle en los fármacos nefrotóxicos Vigilar CK con la Daptomicina Vigilar Hemoglobina y Plaquetas a partir de 2 semanas con Linezolid

48
Subcutaneous administration of cefepime.
J Pain Symptom Manage Aug;30(2):170-4. Subcutaneous administration of cefepime. Walker P, Neuhauser MN, Tam VH, Willey JS, Palmer JL, Bruera E, Prince RA. Source Department of Palliative Care and Rehabilitation Medicine, The University of Texas M. D. Anderson Cancer Center, Houston, Texas 77030, USA. Abstract Management of symptomatic infections can aid in palliation. We investigated the pharmacokinetics and tolerability of cefepime given as a subcutaneous infusion. This novel route of administration is proposed as an alternative to intravenous and intramuscular administration for patients treated outside an institutional setting, such as home hospice. Ten healthy adult volunteers received a single dose of 1g cefepime infused subcutaneously over 30 minutes. Serial serum samples (0.5, 1, 1.5, 2, 4, 6, 9, and 12 hours) were obtained after the end of infusion, and cefepime concentrations were determined by high performance liquid chromatography (HPLC). All serum concentration profiles were modeled by a population pharmacokinetic analysis using the Non-Parametric Adaptive Grid (NPAG) program. Acceptability of administration was evaluated using subjective sensation grading, observation of the subcutaneous site, and a final global evaluation. The mean (median) Cmax, beta-t1/2, AUC0-oo and total clearance were found to be 36.1 (30.9) mg/L, 2.34 (2.56) hours, (125.3) h*mg/L, and 7.42 (7.98) L/h, respectively. All infusions were completed without difficulty or discomfort. No drug side effects occurred. The global acceptability was "strongly agreeable" with all the subjects. Subcutaneous infusion of cefepime appeared to result in a pharmacokinetic profile similar to that of an intramuscular injection. Our evaluations showed excellent tolerability and acceptability. These favorable results warrant further clinical evaluation.
: Subcutaneous administration of cefepime. Walker P, Neuhauser MN, Tam VH, Willey JS, Palmer JL, Bruera E, Prince RA. Source. Department of Palliative Care and Rehabilitation Medicine, The University of Texas M. D. Anderson Cancer Center, Houston, Texas 77030, USA. Abstract. Management of symptomatic infections can aid in palliation. We investigated the pharmacokinetics and tolerability of cefepime given as a subcutaneous infusion. This novel route of administration is proposed as an alternative to intravenous and intramuscular administration for patients treated outside an institutional setting, such as home hospice. Ten healthy adult volunteers received a single dose of 1g cefepime infused subcutaneously over 30 minutes. Serial serum samples (0.5, 1, 1.5, 2, 4, 6, 9, and 12 hours) were obtained after the end of infusion, and cefepime concentrations were determined by high performance liquid chromatography (HPLC). All serum concentration profiles were modeled by a population pharmacokinetic analysis using the Non-Parametric Adaptive Grid (NPAG) program. Acceptability of administration was evaluated using subjective sensation grading, observation of the subcutaneous site, and a final global evaluation. The mean (median) Cmax, beta-t1/2, AUC0-oo and total clearance were found to be 36.1 (30.9) mg/L, 2.34 (2.56) hours, (125.3) h*mg/L, and 7.42 (7.98) L/h, respectively. All infusions were completed without difficulty or discomfort. No drug side effects occurred. The global acceptability was strongly agreeable with all the subjects. Subcutaneous infusion of cefepime appeared to result in a pharmacokinetic profile similar to that of an intramuscular injection. Our evaluations showed excellent tolerability and acceptability. These favorable results warrant further clinical evaluation.")
49
La administración de fármacos por vía s.c. es útil cuando hay
Conclusión La administración de fármacos por vía s.c. es útil cuando hay una incapacidad o no se consideran convenientes las vías oral, i.v. o intramuscular. Esta situación es frecuente en pacientes oncológicos en fase terminal y en ancianos afectados de enfermedades crónicas o degenerativas evolucionadas. Sólo se han evaluado parámetros farmacocinéticos (sobre todo en voluntarios sanos y menos en enfermos) de 5 antibióticos administrados por vía s.c.: ceftriaxona, cefepima, ampicilina, tobramicina y teicoplanina, que son la mayoría de ellos de uso hospitalario, a excepción de ampicilina y tobramicina. Los resultados de los diferentes estudios que compararon la administración de antibióticos por vía s.c. con la vía i.v. fueron similares. No se han identificado estudios que hayan evaluado la eficacia clínica ni la seguridad del tratamiento antibiótico por vía s.c. en pacientes con enfermedades infecciosas tributarios de cuidados paliativos. Aunque se podría asumir que la similitud de las concentraciones plasmáticas del antibiótico por ambas vías de administración indica eficacia similar, no hay suficientes datos de eficacia clínica ni de seguridad para recomendar su uso en la práctica clínica. En España, ninguno de los antibióticos disponibles en el mercado está aprobado para su administración por vía s.c., mientras que en Francia está aprobada la administración de ceftriaxona por esta vía. En ocasiones, en la práctica clínica puede requerirse la utilización de antibióticos por vía s.c., es decir, off-label (uso no contemplado en la ficha técnica). Para ello, se debe realizar una solicitud de uso compasivo del antibiótico seleccionado a la Agencia Española de Medicamentos y Productos Sanitarios. Antibióticos por vía subcutánea en pacientes que precisan cuidados paliativos Aina Soler Mieras a, Sebastià Santaeugenia González b y Eva Montané Esteva,c a Servicio de Farmacología Clínica. bUnidad de Geriatría. Hospital Universitari Germans Trias i Pujol. Badalona. Barcelona. c Departamento de Farmacología, Terapéutica y Toxicología. Universitat Autònoma de Barcelona. Barcelona. España. Med Clin (Barc) 2007, Jul 129 (6): Conclusión La administración de fármacos por vía s.c. es útil cuando hay una incapacidad o no se consideran convenientes las vías oral, i.v. o intramuscular. Esta situación es frecuente en pacientes oncológicos en fase terminal y en ancianos afectados de enfermedades crónicas o degenerativas evolucionadas. Sólo se han evaluado parámetros farmacocinéticos (sobretodo en voluntarios sanos y menos en enfermos) de 5 antibióticos administrados por vía s.c.: ceftriaxona, cefepima,ampicilina, tobramicina y teicoplanina, que son la mayoría de ellos de uso hospitalario, a excepción de ampicilina y tobramicina.Los resultados de los diferentes estudios que compararon la administración de antibióticos por vía s.c. con la vía i.v. fueron similares. No se han identificado estudios que hayan evaluado la eficacia clínica ni la seguridad del tratamiento antibiótico por vía s.c. en pacientes con enfermedades infecciosas tributarios de cuidados paliativos. Aunque se podría asumir que la similitud de las concentraciones plasmáticas del antibiótico por ambas vías de administración indica eficacia similar, no hay suficientes datos de eficacia clínica ni de seguridad para recomendar su uso en la práctica clínica.En España, ninguno de los antibióticos disponibles en el mercado está aprobado para su administración por vía s.c., mientras que en Francia está aprobada la administración de ceftriaxona por esta vía. En ocasiones, en la práctica clínica puede requerirse la utilización de antibióticos por vía s.c., es decir, off-label (uso no contemplado en la ficha técnica). Para ello, se debe realizar una solicitud de uso compasivo del antibiótico seleccionado a la Agencia Española de Medicamentos y Productos Sanitarios.
 de 5 antibióticos. administrados por vía s.c.: ceftriaxona, cefepima, ampicilina, tobramicina y teicoplanina, que son la mayoría de. ellos de uso hospitalario, a excepción de ampicilina y tobramicina. Los resultados de los diferentes estudios que compararon. la administración de antibióticos por vía s.c. con la. vía i.v. fueron similares. No se han identificado estudios que. hayan evaluado la eficacia clínica ni la seguridad del tratamiento. antibiótico por vía s.c. en pacientes con enfermedades. infecciosas tributarios de cuidados paliativos. Aunque se. podría asumir que la similitud de las concentraciones plasmáticas. del antibiótico por ambas vías de administración indica. eficacia similar, no hay suficientes datos de eficacia clínica. ni de seguridad para recomendar su uso en la práctica clínica. En España, ninguno de los antibióticos disponibles en el. mercado está aprobado para su administración por vía s.c., mientras que en Francia está aprobada la administración de. ceftriaxona por esta vía. En ocasiones, en la práctica clínica. puede requerirse la utilización de antibióticos por vía s.c., es. decir, off-label (uso no contemplado en la ficha técnica). Para ello, se debe realizar una solicitud de uso compasivo. del antibiótico seleccionado a la Agencia Española de Medicamentos. y Productos Sanitarios. Antibióticos por vía subcutánea en pacientes que precisan cuidados paliativos. Aina Soler Mieras a, Sebastià Santaeugenia González b y Eva Montané Esteva,c. a Servicio de Farmacología Clínica. bUnidad de Geriatría. Hospital Universitari Germans Trias i Pujol. Badalona. Barcelona. c Departamento de Farmacología, Terapéutica y Toxicología. Universitat Autònoma de Barcelona. Barcelona. España. Med Clin (Barc) 2007, Jul 129 (6): Conclusión. La administración de fármacos por vía s.c. es útil cuando hay una incapacidad o no se consideran convenientes las vías oral, i.v. o intramuscular. Esta situación es frecuente en pacientes oncológicos en fase terminal y en ancianos afectados de enfermedades crónicas o degenerativas evolucionadas. Sólo se han evaluado parámetros farmacocinéticos (sobretodo en voluntarios sanos y menos en enfermos) de 5 antibióticos administrados por vía s.c.: ceftriaxona, cefepima,ampicilina, tobramicina y teicoplanina, que son la mayoría de ellos de uso hospitalario, a excepción de ampicilina y tobramicina.Los resultados de los diferentes estudios que compararon la administración de antibióticos por vía s.c. con la vía i.v. fueron similares. No se han identificado estudios que hayan evaluado la eficacia clínica ni la seguridad del tratamiento antibiótico por vía s.c. en pacientes con enfermedades infecciosas tributarios de cuidados paliativos. Aunque se podría asumir que la similitud de las concentraciones plasmáticas del antibiótico por ambas vías de administración indica eficacia similar, no hay suficientes datos de eficacia clínica ni de seguridad para recomendar su uso en la práctica clínica.En España, ninguno de los antibióticos disponibles en el mercado está aprobado para su administración por vía s.c., mientras que en Francia está aprobada la administración de ceftriaxona por esta vía. En ocasiones, en la práctica clínica puede requerirse la utilización de antibióticos por vía s.c., es decir, off-label (uso no contemplado en la ficha técnica). Para ello, se debe realizar una solicitud de uso compasivo del antibiótico seleccionado a la Agencia Española de Medicamentos. y Productos Sanitarios.")
50
GRACIAS

Presentaciones similares


 European Transfer Credit System (ECTS) Methodology in.>")




.>")













